The Scottish Health Survey 2022 – volume 1: main report
This report presents results for the Scottish Health Survey 2022, providing information on the health and factors relating to health of people living in Scotland.
1 Mental Health and Wellbeing
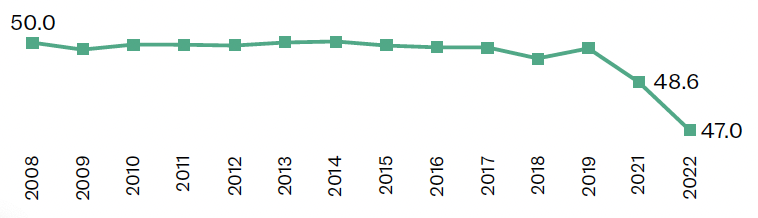
Average levels of mental wellbeing (measured by mean WEMWBS scores[21]) decreased between 2021 and 2022 and were outside of the range previously observed between 2008 and 2019 (49.4-50.0)[21].
In 2022, older adults reported higher WEMWBS scores compared to younger adults.
- 16-24: 46.5
- 25-34: 46.0
- 35-44: 46.4
- 45-54: 45.5
- 55-64: 47.1
- 65-74: 49.8
- 75+: 49.3
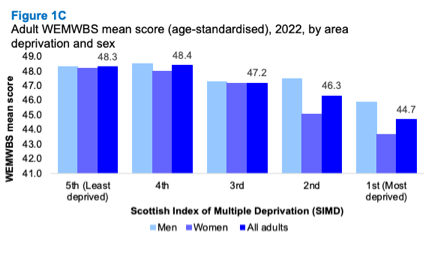
In 2022, WEMWBS scores decreased as levels of deprivation increased.
- Least deprived: 48.3
- 4th: 48.4
- 3rd: 47.2
- 2nd: 46.3
- Most deprived: 44.7
In 2022, 27% of adults had a GHQ-12[22] score of 4 or more (indicative of a possible psychiatric disorder), an increase from 2021 and higher than previous scores in the time series (14%-19% between 2003 and 2019).
- 2021: 22%
- 2022: 27%
In 2022, GHQ-12 scores of 4 or more were significantly higher for women than for men.
- Women: 31%
- Men: 22%
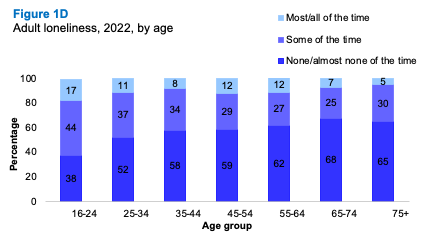
The proportion of adults feeling lonely ‘most’ or ‘all of the time’ increased between 2021 and 2022.
- 2021: 8%
- 2022: 11%
Overall, older adults were less likely to report feeling lonely ‘most’ or ‘all of the time’ compared with younger adults.
- 16-24: 17%
- 25-34: 11%
- 35-44: 8%
- 45-54: 12%
- 55-64: 12%
- 65-74: 7%
- 75+: 5%
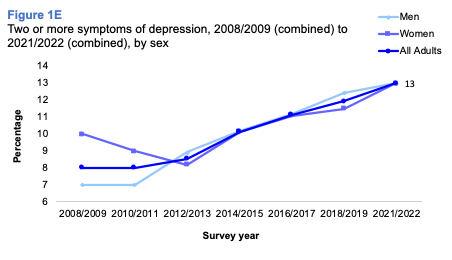
There has been a gradual but overall significant increase in the proportion of adults reporting two or more symptoms of depression, rising from:
- 2008/09: 8%
- 2010/11: 8%
- 2012/13: 9%
- 2014/15: 10%
- 2016/17: 11%
- 2018/19: 12%
- 2021/22: 13%
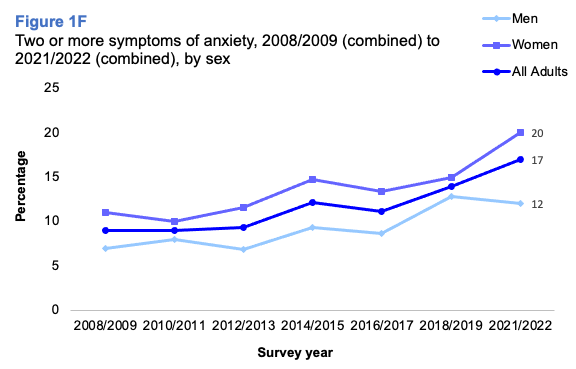
The proportion of adults that reported having two or more symptoms of anxiety was 17% in 2021/2022. This had increased from 9% between 2008/2009 and 2012/2013, and 11 - 14% between 2014/2015 and 2018/2019.
- 2008/09: 9%
- 2010/11: 9%
- 2012/13: 9%
- 2014/15: 12%
- 2016/17: 11%
- 2018/19: 14%
- 2021/22: 17%
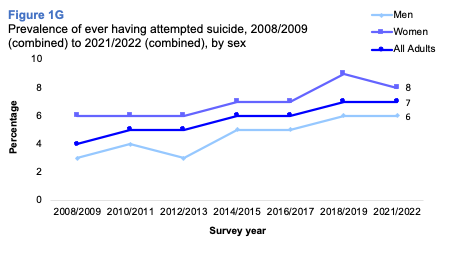
The proportion of adults reporting that they had ever attempted suicide has risen from 4% in 2008/2009 to 7% in 2018/2019 combined and 2021/2022 combined.
- 2008/09: 4%
- 2010/11: 5%
- 2012/13: 5%
- 2014/15: 6%
- 2016/17: 6%
- 2018/19: 7%
- 2021/22: 7%
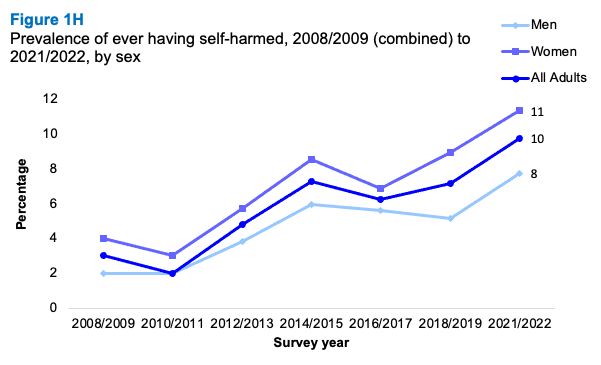
The proportion of adults reporting that they have ever self-harmed increased from 2-3% in 2008/2009 to 10% in 2021/2022.
- 2008/09: 3%
- 2010/11: 2%
- 2012/13: 5%
- 2014/15: 7%
- 2016/17: 6%
- 2018/19: 7%
- 2021/22: 10%
The prevalence of adults reporting two or more symptoms of depression tended to decrease with age, although not linearly. Lowest levels were recorded among those aged 75 and over, and highest among those aged 16-34 or 55-64.
- 16-24: 16%
- 25-34: 16%
- 35-44: 12%
- 45-54: 14%
- 55-64: 16%
- 65-74: 9%
- 75+: 7%
Prevalence of two or more symptoms of anxiety was highest among those aged 16-34 (25 - 26%) and lowest was among those aged 65-74 (7%). Differences by sex were greatest amongst the 16-24 age group, at 13% of men and 33% of women.
- Men 16-24: 13%
- Women 16-24: 33%
In 2021/2022, age was a significant factor in whether someone had ever attempted suicide. The highest prevalence was among those aged 16-34 and those aged 55-64.
- 16-24: 10%
- 25-34: 11%
- 35-44: 5%
- 45-54: 7%
- 55-64: 10%
- 65-74: 4%
- 75+: <1%
In 2022, 30% of children lived with a parent with a GHQ12 score of 4 or above (indicative of a possible psychiatric disorder).
- 2022: 30%
Erin Deakin
1.1 Introduction
Mental health is defined by the World Health Organisation as a state of well-being in which every individual realises their own potential, can cope with the stresses of life, can work productively, and is able to make a contribution to their community[21]. Positive mental health helps individuals to connect with others, cope with stress, emotions and decision making, make healthy choices and to thrive. Therefore, eradicating any stigma associated with seeking help and ensuring the promotion of mental wellbeing for all, not just those experiencing difficulties, have been identified as key areas of focus for mental health reform[22]. Mental disorders often co-exist with physical illnesses[23] and are impacted by the same inequalities that have been observed for physical health. Those with severe mental disorders have a life expectancy 15-20 years shorter than the general population[24].
Around one in three people are estimated to be affected by mental health problems in Scotland in any one year[25], with levels of loneliness, anxiety and economic concerns having increased during the COVID-19 pandemic[26]. It is also evidenced that mental ill health in adolescence increases the risk of subsequent mental ill health later in life[27], with impacts of COVID-19 pandemic reported to include a deterioration in mental wellbeing and increased loneliness among children and young people[28]. Globally, around 5% of adults are estimated to experience depression and it is more prevalent among women than men[29]. Around 703,000 people die due to suicide every year globally and rates remain consistently higher for men than for women[30].
Poor mental health, including mental disorder, has a considerable impact on individuals, their families and society in general[31] and is clearly associated with both poverty and social exclusion[32]. Loneliness is a significant public health problem[33] which can contribute to the onset and continuation of poor mental health[34]. Some population groups at increased risk include those with poor mental and/or physical health, those living in poverty, those with disabilities, those from LGBTI or minority ethnic communities and carers. The risk of loneliness is also greater for those with mental health problems than for those with physical health problems and particularly high for those who experience anxiety, depression or stress[35],[36].
1.1.1 Policy background
The impact of the COVID-19 pandemic was felt widely at both societal and individual levels, impacting on mental health in both the short and longer term. The Mental Health – Scotland’s Transition and Recovery Plan[37] sets out the mental health needs resulting from the pandemic and how the Scottish Government is addressing these.
The plan’s commitments focus on areas or groups of people whose mental health was most likely to be affected, focusing on promoting positive mental health at the population level, signposting to help and support, rapid and accessible support for those in distress and treatment for those living with mental illness.
The Scottish Government’s Mental Health Strategy 2017-2027 sets out a number of actions in place or planned to improve areas including prevention and early intervention, access to treatment and physical wellbeing for those experiencing mental health issues. The Strategy is thus to focus on promoting positive mental health and preventative services, with the same level of commitment as with physical health[38].
In June 2023, the Scottish Government published Scotland's Mental Health and Wellbeing: Strategy[39], which had been informed by public consultation. It builds on the Transition and Recovery Plan and sets out priorities for the coming years.
1.1.2 Reporting on mental wellbeing in the Scottish Health Survey
This chapter updates trends in mental wellbeing for adults using the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS). Trends in mental health are also updated for adults including the General Health Questionnaire 12 (GHQ-12) and CIS-R anxiety and depression scores, as well as data on attempted suicide, self-harm, loneliness and children living with a parent with a possible psychiatric disorder. Figures are also reported by age, sex and area deprivation.
The Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS) data for children, reported in both 2019 and 2021, has not been presented in this report. This is because it requires several years of data and will be presented once data has been collected for both 2022 and 2023.
The area deprivation data are presented in Scottish Index of Multiple Deprivation (SIMD) quintiles. To ensure that the comparisons presented are not confounded by the different age profiles of the quintiles, the data have been age-standardised. For a detailed description of both SIMD and age-standardisation as well as definitions of other terminology used in this chapter and for further details on the data collection methods for mental health and wellbeing and loneliness, please refer to Chapter 2, of the Scottish Health Survey 2022 volume 2 technical report.
Supplementary tables on mental wellbeing are also published on the Scottish Government website: Scottish Health Survey.
1.2 Mental Health & Wellbeing
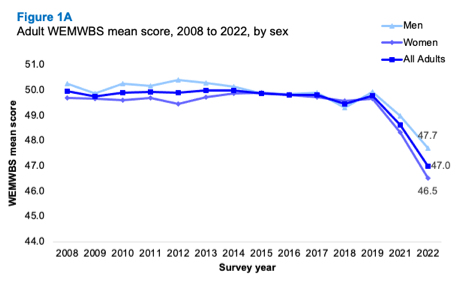
1.2.1 Adult WEMWBS mean score, 2008 to 2022, by sex
In 2022, the mean WEMWBS score for all adults was 47.0, a decrease from the mean of 48.6 recorded in 2021 and outside the range observed prior to 2021 (49.4– 50.0).
Across the time series, men have generally recorded higher mean WEMWBS scores, although the differences have not always been significant. In 2022, no significant difference was recorded between men (47.7) and women (46.5). However, scores for both men and women have decreased since 2019, with the 2022 scores representing significant decreases from those recorded for 2021 (49.0 and 48.3 respectively).
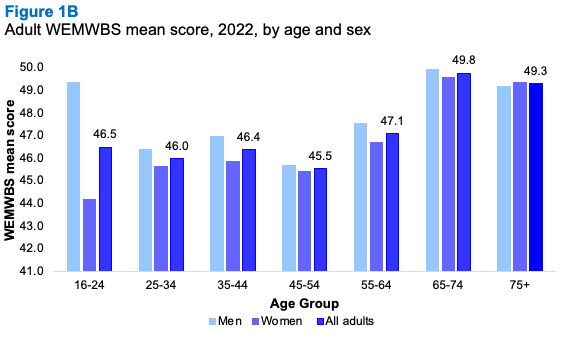
1.2.2 Adult WEMWBS mean score, 2022, by age and sex
Consistent with previous survey years, higher mental wellbeing scores were reported in older adults compared to younger adults. In 2022, adults aged 65-74 reported a mean WEMWBS score of 49.8 and those aged 75 or older, a mean score of 49.3. In comparison, the mean scores for those aged 16-64 were in the range 45.5-47.1.
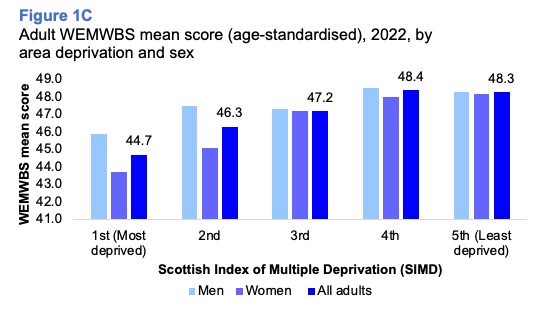
1.2.3 Adult WEMWBS mean score (age-standardised), 2022, by area deprivation and sex
Age-standardised adult WEMWBS mean scores continued to show significant variation by area deprivation in 2022. WEMWBS mean scores decreased as deprivation increased, from mean scores of 48.3 and 48.4 in the two least deprived quintiles, to a mean score of 44.7 in the most deprived areas.
No significant differences were recorded by SIMD between men and women in 2022.
1.2.4 GHQ-12 score, 2003 to 2022, by sex
A GHQ-12 score of four or more is indicative of a possible psychiatric disorder. In 2022, the proportion of adults with a GHQ-12 score of 4 or more was 27%, a significant increase on the proportion recorded in 2021 (22%) and on the proportions recorded in previous years which ranged from 14%-19%.
In 2022, the proportion of adults with a GHQ-12 score of zero was the lowest in the time series (45%) and a significant decrease compared with 2021 (52%). Across the timeseries, the proportion of adults with a score between one and three has remained in the range 21%-28%, with the 2022 proportion (28%) at the upper end of this range.
As in previous years, the proportion of adults with a GHQ-12 score of four or more was significantly higher for women (31%) compared to men (23%) in 2022, with these proportions the largest recorded for both men and women. Table 1.4
1.2.5 Adult loneliness, 2022, by age and sex
In 2022, 11% of adults reported having felt lonely ‘most’ or ‘all of the time’ in the week prior to being interviewed. Additionally, 32% of adults reported having felt lonely ‘some of the time’. The proportion of adults reporting feeling lonely ‘almost none of the time’ or ‘not at all’ was 58%.
Overall, older adults were less likely to report feeling lonely ‘most’ or ‘all of the time’ (7% of those aged 65-7 and 5% of those aged 75 or older) compared with younger adults (17% of those aged 16-24).
No significant variation was recorded in 2022 by sex in the proportions who reported being lonely ‘all/most of the time’. However, women were more likely than men to report feeling lonely ‘some of the time’ (35%, compared with 28% of men).
1.2.6 CIS-R anxiety and depression scores, attempted suicide and self-harm, 2008/2009 combined to 2021/2022 combined, by sex
To increase the sample size available, the analysis of anxiety and depression scores, attempted suicide and self-harm, by sex, made use of sets of two-years of combined data from 2008/2009 to 2021/2022, excluding 2020 due to a lack of comparable data.
Depression
Across the time series, there has been a gradual but overall significant increase in the proportion of adults reporting two or more symptoms of depression, rising from 8% in 2010/2011 to 13% in 2021/2022.
Among men, the proportion that reported two or more symptoms of depression has risen from 7% in 2010/2011 combined to 13% in 2021/2022 combined.
The prevalence of two or more symptoms of depression has varied among women over the time series, although this has been more consistent in recent years (in the range 10% - 13% since 2014/2015) with the 2021/2022 proportion at the upper end of this range.
Anxiety
The proportion of adults that reported having two or more symptoms of anxiety has increased overall throughout the time series, with the highest percentage (17%) being reported in 2021/2022. In comparison to earlier years, 9% recorded two or more symptoms of anxiety between 2008/2009 and 2012/2013, while 11-14% reported two or more symptoms between 2014/2015 and 2018/2019.
Among men, the prevalence of reporting two or more symptoms of anxiety has generally increased over the time series, from 7% in 2008/2009 to 13% in 2018/2019 and 12% in 2021/2022.
Across the time series there has also been an overall increase in the prevalence of women reporting two or more symptoms of anxiety, rising from 10 - 11% in 2008/2009 and 2010/2011 to its highest proportion of 20% in 2021/2022.
Over the time series (2008/2009 to 2021/2022), consistently higher proportions of women recorded two or more symptoms of anxiety, with the difference varying from two to eight percentage points higher than the proportions among men. The difference by sex in 2021/2022 was the highest across the time series (eight percentage points).
Attempted suicide
Across the time series, the proportion of adults reporting that they had ever attempted suicide has risen from 4% in 2008/2009 to 7% in 2018/2019 and 2021/2022.
Women have been consistently more likely to report ever having attempted suicide compared with men over the time series (two to three percentage points difference) although there was no significant difference between men and women in 2021/2022.
Self-harm
The proportion of adults reporting that they have ever self-harmed has generally increased across the time series. In 2021/2022, 10% of adults reported having self-harmed, the highest proportion recorded in the series to date. Equivalent levels in 2008/2009 and 2010/2011 ranged from 2-3%. It should be noted that in 2012/2013 the mode of data collection changed from nurse administered to self-completion questionnaire.
Similar patterns of overall increase were recorded by sex with the prevalence of self-harm for both men and women the highest in the time series in 2021/2022 at 8% and 11% respectively. When comparing sexes across the years, women have been more likely than men to report ever having self-harmed, however there was no statistically significant difference recorded in 2021/2022.
1.2.7 CIS-R anxiety and depression scores, attempted suicide and self-harm, 2021/2022 combined, by age and sex
Overall, the prevalence of adults reporting two or more symptoms of depression tended to decrease with age, although a linear decrease was not recorded. In 2021/2022, the lowest levels were recorded among those aged 75 and over (7%), while the highest prevalence was among young people aged 16-34 (16%) and those between the ages of 55 and 64 (16%).
Prevalence of two or more symptoms of anxiety displayed similar patterns, with a general decrease being observed with age in 2021/2022. Those aged 16-34 (25 - 26%) recorded the highest proportion with two or more anxiety symptoms while the lowest was among those aged 65 and over (7%). When comparing sexes, women were significantly more likely to report two or more symptoms of anxiety compared to men for several age groups. The largest variation was recorded among those aged 16-24, where 13% of men and 33% of women in this age group reported having experienced two or more symptoms of anxiety.
In 2021/2022, age was a significant factor in whether someone had ever attempted suicide. While a general decrease in prevalence as age increased was observed, this was again not a linear pattern. The highest prevalence was among those aged 16-34 (10 - 11%) and those aged 55-64 (10%) with the lowest recorded among those aged 75 and over who were the least likely to report having done so (<1%). A similar pattern by age was observed for both men and women.
Age was also significant with regards to the proportion of adults who reported ever having self-harmed, with a general decrease in prevalence as age increased. In 2021/2022, 29% of those aged 16-24 and 19% of those aged 25-34 reported having self-harmed, compared with <1% of those aged 75 and over. Table 1.7
1.2.8 Children living with a parent with GHQ12 score of 4+, 2022, by age and sex
In 2022, 30% of children lived with a parent with a GHQ12 score of 4 or above (indicative of a possible psychiatric disorder). No significant variations were recorded by age, with this proportion in the range 27-33% or by sex (32% among boys compared with 28% among girls).
There were some significant variations between sexes for certain age groups. Boys aged 0-3 were more likely to be living with a parent who has a GHQ12 score of four or above (30%) compared to girls the same age (23%). Boys aged 12–15 were also more likely to be living with a parent who has a score of four or above (40%) compared to girls (27%). Table 1.8
Table List
Table 1.1 Adult WEMWBS mean score, 2008 to 2022, by sex
Table 1.2 Adult WEMWBS mean score, 2022, by age and sex
Table 1.3 Adult WEMWBS mean score (age-standardised), 2022, by area deprivation and sex
Table 1.4 GHQ-12 score, 2003 to 2022, by sex
Table 1.5 Adult loneliness, 2022, by age and sex
Table 1.6 CIS-R anxiety and depression scores, attempted suicide and self-harm, 2008/2009 combined to 2021/2022 combined, by sex
Table 1.7 CIS-R anxiety and depression scores, attempted suicide and self-harm, 2021/2022 combined, by age and sex
Table 1.8 Children living with a parent with GHQ12 score of 4+, 2022, by age and sex