International Development Fund: non-communicable disease programme
This report responds to a commission by the Scottish Government to design a new international development health programme providing support to the governments of Malawi, Rwanda and Zambia with a focus on non-communicable diseases (NCDs).
Strategic Case
Why is Scottish Government support required?
1. Scotland and the SG have a long history of providing health development support to SSA in particular, to Malawi, Rwanda, and Zambia. SG are currently reviewing their 2023 development strategy which will guide investments in international health programming. SG have identified non-communicable diseases as a potential area for collaboration across the three countries.
2. Current SG health development programmes have built upon the 2008 small grants funds, and focus on a wide range of interventions, from support to a dental school, to individual support to NGOs to deliver school meals, community ear and hearing care and to improve maternal and child health.[10]
3. Scotland has longstanding expertise in delivering NCD programmes domestically, whether integration of routine diagnosis and management of NCDs into primary care systems, to setting up of comprehensive surveillance and monitoring systems for those living with diabetes mellitus, to early implementation of tobacco control legislation, to exploring the need for and use of alcohol and sugar taxation as part of public health policy. Scotland is therefore well placed to share learning beyond its borders.[11]
4. This report provides the background and context for investing in the NCD space in Malawi, Rwanda and Zambia. The definition of NCDs varies globally, however, for the purpose of this report NCDs refers to those identified in the Brazzaville Declaration including cardiovascular diseases, diabetes, cancers, chronic respiratory diseases, haemoglobinopathies (in particular sickle cell disease), mental disorders, violence and injuries, and oral and eye diseases.[12]
Why should the international community support efforts to tackle NCDs in SSA?
5. The case for investing in NCDs in SSA is compelling. Globally non-communicable diseases (NCDs) are the leading cause of death and disability, killing around 41 million people each year. This accounts for around 71% of all global deaths.[13]
“This is a time bomb for Zambia, as they [external partners] are not supporting NCDs health systems.” Zambian Academic
6. The WHO predicts that by 2030 NCDs will be the primary cause of death across SSA with around 3.8 million premature deaths (51% of all premature mortality). It is anticipated that the total number of deaths from NCDs, injuries and mental health conditions will at least triple (16.6 million deaths) by 2063 and will account for 89% of the total.[14]
7. In SSA it is estimated that the proportion of deaths from NCDs varies between 27% to 88% depending on the country.[15] The total share of deaths caused by NCDs has increased from 24.2% in 2000 to 37.1% in 2019 with over 2.1 million people dying prematurely (<70 years of age) across the region. In terms of disability, NCDs cost the region over 225 million disability adjusted life years (DALYs) in 2019 compared with 90.6 million in 1990. Injuries resulted in an additional 0.6 million premature deaths and 41 million DALYs.[16]
“You can find all the ARV medications but not the NCD medications. People with HIV are dying from stroke and other things. A lot of people are dying prematurely, HIV positive and negative, from NCDs.” Zambian Academic
8. The region is facing a rapid demographic and epidemiological transition that includes a shift in health profile from one that was previously dominated by communicable disease to one with an increasing predominance of NCDs. This is further supported by age standardised DALY rates which show that DALYs lost from NCDs (21,757 DALY’s per 100,000 population) are now almost equivalent to those lost communicable diseases, maternal and neonatal causes (26,491 DALY’s per 100,000 population) (Figure 1).[17] Indeed, many countries are already struggling to tackle this ‘double burden’ with consequent impacts on the ability of health systems to respond and allocate resource to NCDs due to competing demands.
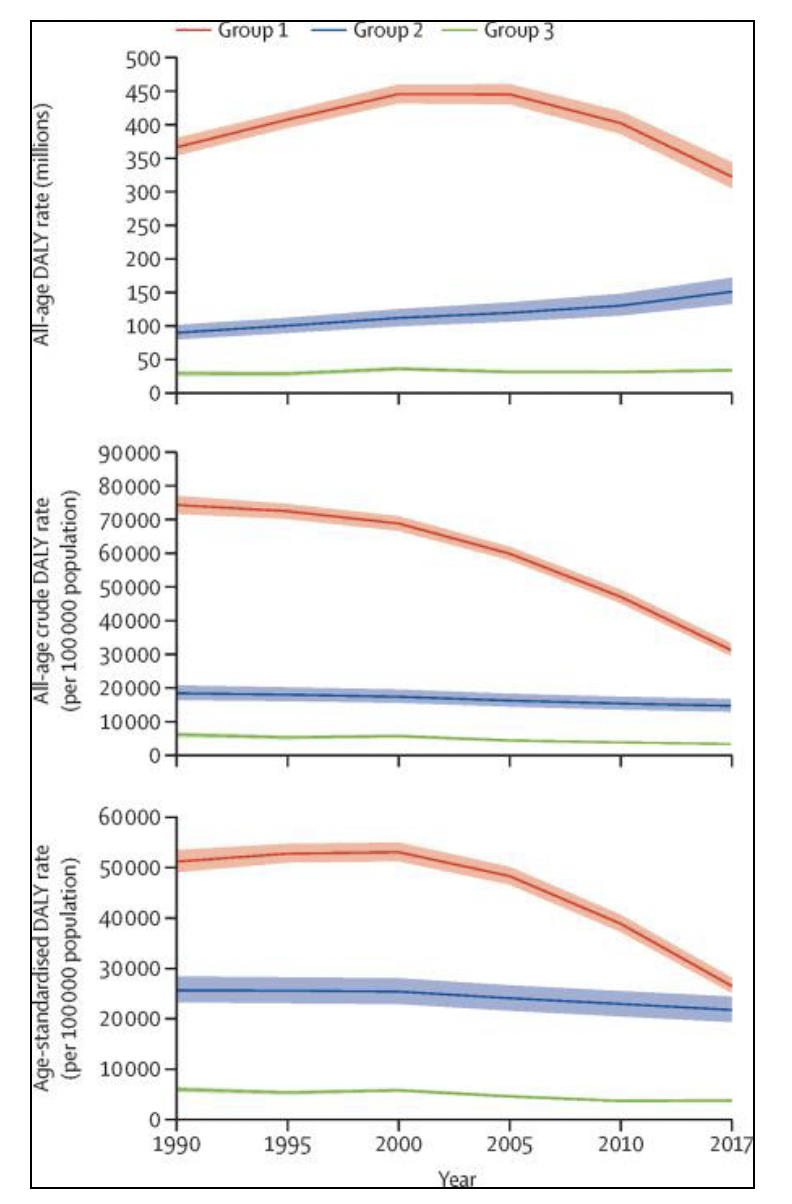
Source: Gouda, H.N. et al (2019) Burden of non-communicable diseases in sub-Saharan Africa, 1990-2017: results of the burden of disease study 2017. The Lancet Global Health. Volume 7, Issue 10, E1375-E1387. Reproduced under CC BY license.
9. NCD risk factor surveillance suggests that most adults in SSA are exposed to at least one risk factor whether tobacco consumption, harmful alcohol use, unhealthy diet, physical inactivity, obesity or high blood pressure and there is growing concern that the burden of disease will continue to increase with increasing rates of smoking and poor dietary practices with ensuing pressure on health systems (Figure 2).[19]
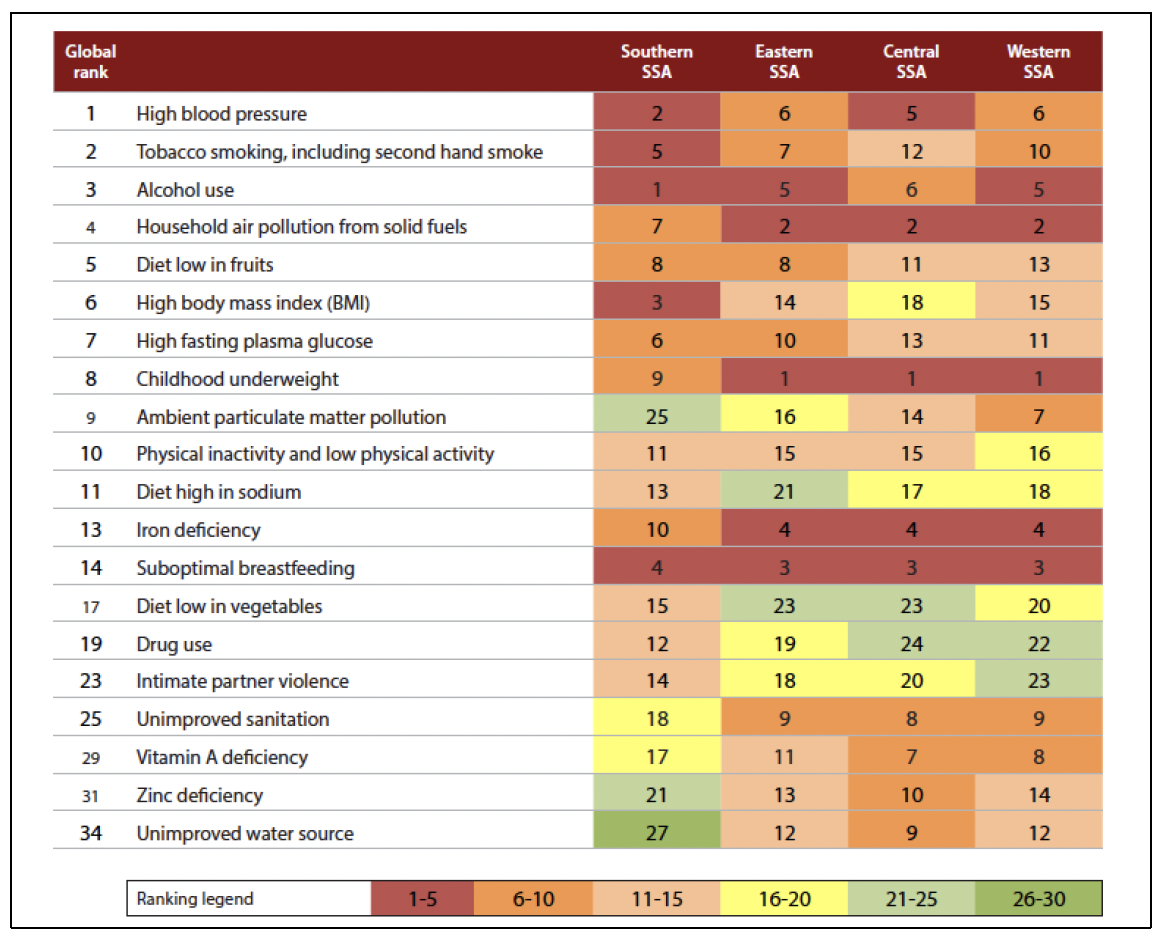
Source: Marquez, P.V.; Farrington, J.L. (2013) The challenge of non-communicable diseases and road traffic injuries in Sub-Saharan Africa: an overview. Washington, D.C.: World Bank Group.
10. Cardiovascular diseases (predominantly strokes driven by hypertension) were the main cause of disease burden from NCDs in SSA in 2017 contributing around 15.1% of the total NCD disease burden, as shown in Figure 3. This was followed by neoplasms and mental health related issues which accounted for around 11.2% and 9.0% of the disease burden respectively. In terms of neoplasms, cervical and breast cancer are the leading causes of disease burden in 2017, with cervical cancer closely linked to HIV.[20] Diabetes also causes a great deal of morbidity, with an increase in DALYs of 126.4% between 1990 and 2017. Late diagnosis exacerbates the impact of these conditions on the region.[21] However, in contrast to assumptions on NCDs being an issue of aging, NCDs in SSA are prevalent across the full life course particularly for the poorest and most vulnerable.
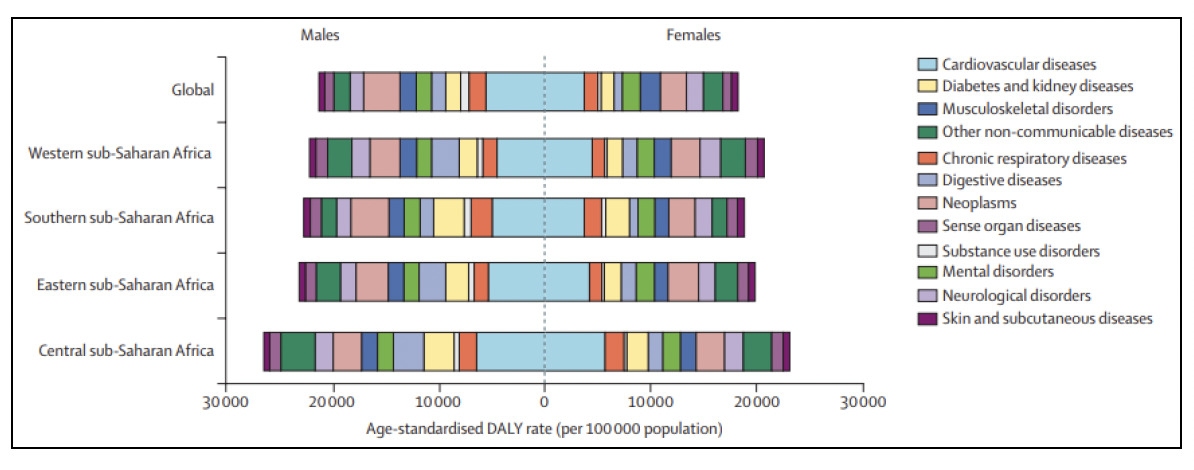
Source: Gouda, H.N. et al (2019) Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: results from the Global Burden of Disease Study 2017. The Lancet Global Health. Volume 7, Issue 10, E1375-E1387. Reproduced under CC BY license.
11. Palliative care is an essential component of NCD care. In 2014, the World Health Assembly adopted a resolution to integrate palliative care into national health policies. Despite this, only 50% of countries have integrated palliative care into their NCD policy. During KIIs palliative care was often not brought up spontaneously by participants as a NCD area of focus, upon direct questioning all participants strongly emphasised the importance of this neglected area. Access to essential medications is essential to the delivery of quality palliative care services but is challenged by lack of availability to opiates and other commodities. Only 13% of LICs report general availability of oral morphine.[22]
How are NCDs linked to poverty?
12. In 2020 a Lancet commission found that one third of the disease burden in the poorest billion globally are a consequence of NCDs. They state that ‘the world’s poorest billion are being systematically deprived of life saving and life changing interventions’ for NCDs. With more than 90% of the poorest billion living in rural areas of LMICs in SSA and South Asia, aged under 55 years of age and at risk of developing NCDs at younger ages, it is clear that NCDs are inextricably linked to poverty and are therefore of relevance to development financing and programming in SSA.[23]
“85% of Malawians live in rural areas – they think NCDs are a disease of people who live in the city” Individual, Ministry of Health, Malawi
13. T he poorest living in SSA are disproportionately affected by NCDs throughout their life course. This is contributed to by hunger, exposure to toxic environments, infectious diseases and lack of health care. In under-fives the burden is driven by congenital anomalies and sickle cell disorders with 80-90% of children with sickle cell dying before they turn five years of age. Those who survive are at increased risk of both communicable and NCDs. In 2017, mental health issues contributed a large burden in people aged 14-39 years of age (see Figure 4). Morbidity and mortality from cancer and cardiovascular disease is also higher in these groups.
“There is an unfinished MDG agenda. Donors still focus on that.” Donor agency
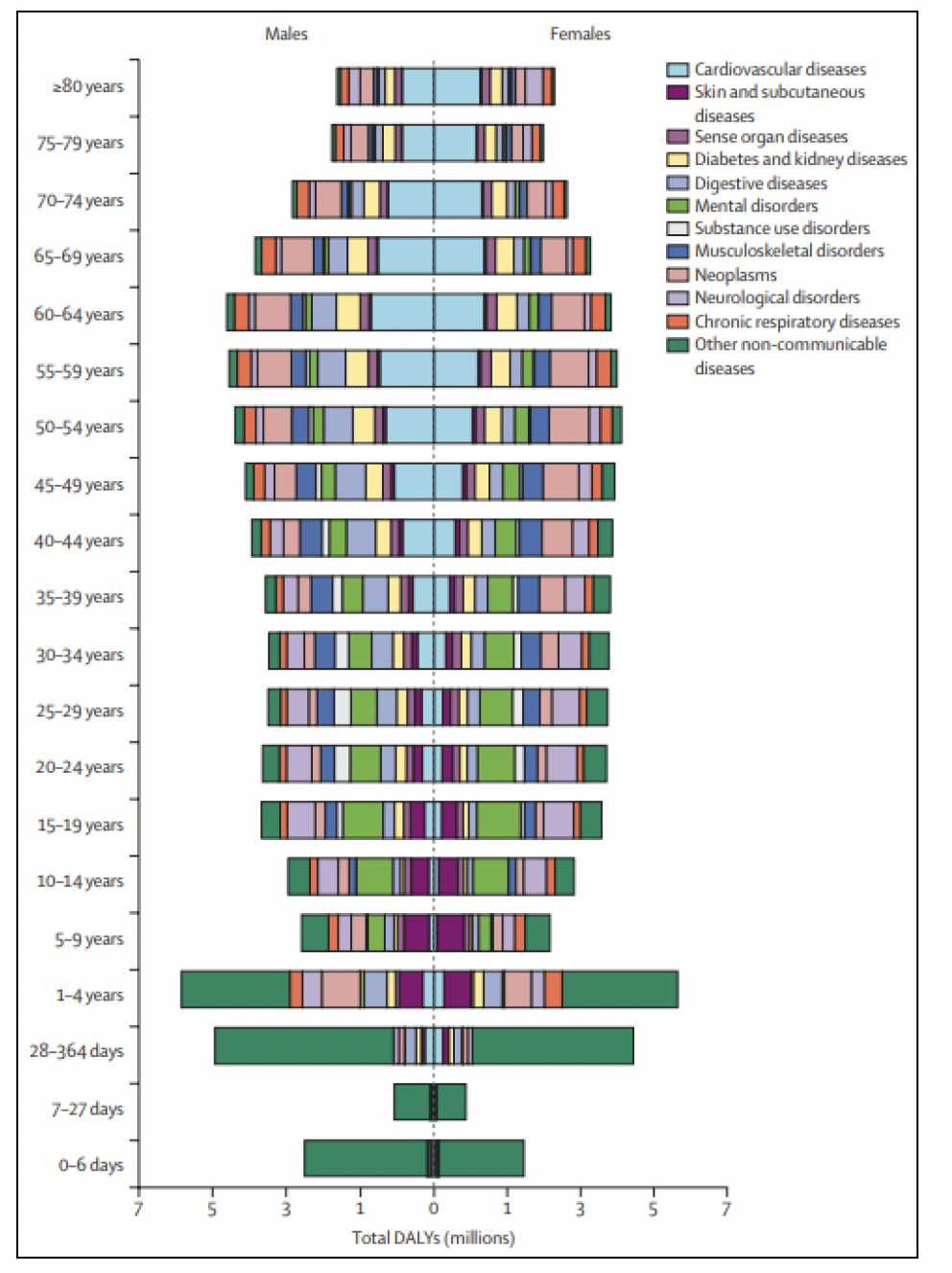
Source: Gouda, H.N. et al (2019) Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: results from the Global Burden of Disease Study 2017. The Lancet Global Health. Volume 7, Issue 10, E1375-E1387. Reproduced under CC BY license.
14. Across the poorest billion, 800,000 deaths from NCDs are in those aged under 40 years, more than HIV, tuberculosis and maternal deaths combined and result in 20 more years healthy life loss than those in high income countries. They account for over one third (35%) the DALYs in its population. Some of this can be accounted for by earlier age of presentation in those living in extreme poverty coupled with lower access to quality health services, but late diagnosis, lower treatment adherence and poorer quality care all play a role, as well as exposure to infectious diseases and undernutrition (Figure 5). Years of life lost due to NCDs is higher in those living in extreme poverty compared with others.[24]
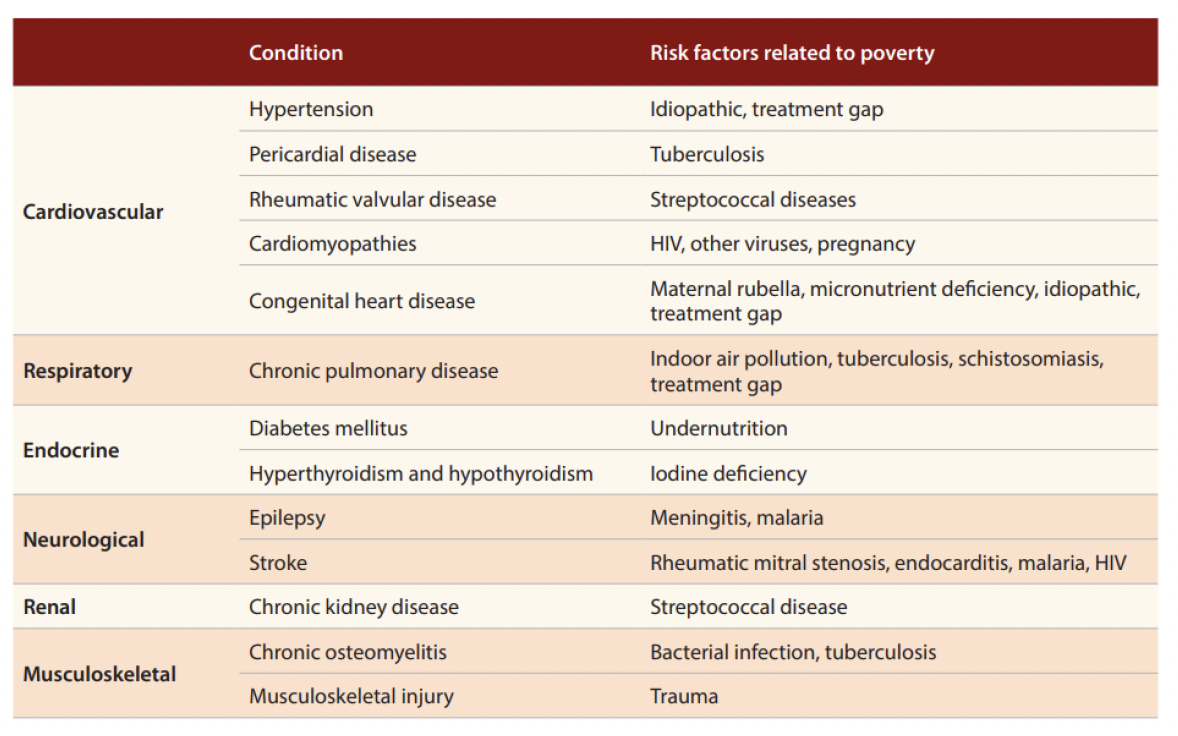
Source: Marquez, P. V., Farrington, J. L. (2013) The Challenge of Non-Communicable Diseases and Road Traffic Injuries in Sub-Saharan Africa. An Overview. Washington, DC.: The World Bank. Reproduced under CC BY license.
15. Management of NCDs often focuses on measures that relate to behaviour change and prevention rather than on unblocking barriers to access for the poorest (Figure 6). It is estimated that half (49%) the total NCD burden in the poorest is avoidable, with the potential to avert 2.4 million deaths and 93.8 million DALYs. However, almost half (47%) the NCD burden among the poorest billion is due to conditions not yet addressed by global NCD frameworks which tend to focus on prevention around five disease categories (cardiovascular, cancer, chronic respiratory disease, diabetes, and mental health and substance abuse). There is a general sense amongst KIIs that issues such as smoking are not currently the main driver of NCDs in the three partner countries, which is in contrast to the Global North. That said, it was also highlighted that this may change in the coming years. The commission argues by focusing on more traditional models of NCD care we are neglecting the needs of the poorest.[25]
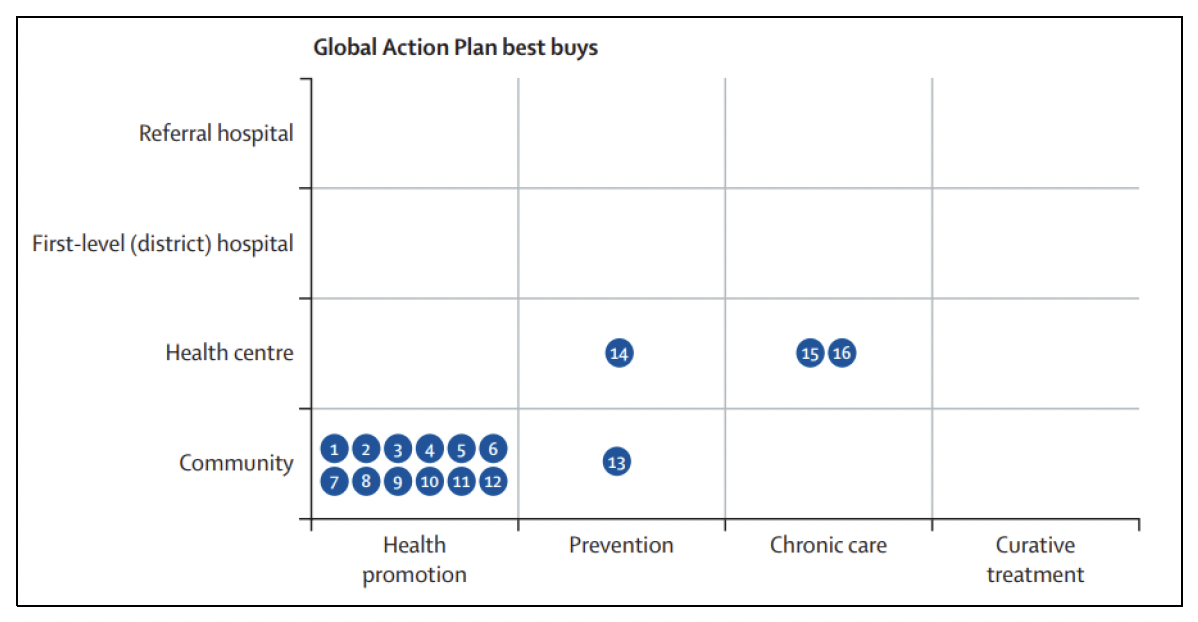
Source: Bukhman G. et al (2020) Lancet NCDI Poverty Commission Study Group. The Lancet NCDI Poverty Commission: bridging a gap in universal health coverage for the poorest billion. Lancet. 3;396(10256):991-1044. Permission to reproduce content secured via RightsLink.
What is the policy context for tackling NCDs?
16. There is global recognition of the challenge of NCDs. In 2013, WHO Member States ratified the Global Action Plan (GAP) on NCDs which sets out a roadmap, policy options and nine voluntary targets to be achieved by 2025 (subsequently extended to 2030). The aim is to reduce premature mortality from cardiovascular diseases, cancer, diabetes, or chronic respiratory diseases by 25%.[27]
17. In 2015 the United Nations Sustainable Development Goals (SDGs) included a target to reduce the probability of premature death from the four main NCDs in adults aged between 30-70 years by 30% by the year 2030.[28]
18. In 2017, a list of options of cost-effective interventions or ‘WHO Best Buys’ were produced for NCDs (Figure 6). These target four of the primary risk factors (tobacco, harmful use of alcohol, unhealthy diet and physical inactivity) associated with the four main NCD disease areas (cardiovascular disease, diabetes, cancer and chronic respiratory disease).
“Most countries NCDs are poorly funded and Ministry of Health’s human resource are weak.” UNO NCD focal point
19. In 2020 WHO launched the Global NCD Compact 2020-2030 bringing together Heads of State and Governments to encourage Member States to adopt best practice policies on the prevention and control of NCDs. It will aim to deliver the Implementation Roadmap 2023-2030 of the GAP as endorsed by WHO Member States in 2022, by implementing the best-buys and WHO NCDs technical packages. These include: PEN: package on non-communicable disease interventions;[29] HEARTS: technical package for cardiovascular disease management in primary health care: risk-based CVD management;[30] MPOWER: measures intended to assist in the country-level implementation of effective interventions to reduce the demand for tobacco, contained in the WHO Framework convention of tobacco control;[31] SAFER: to deliver health and development gains caused by the harmful use of alcohol;[32] SHAKE: technical package for salt reduction;[33] ACTIVE: technical package for increasing physical activity and also including reorientation of PHC and strengthening of health systems.[34][35] Due to the recent nature of these packages, no reviews have yet been carried out.
“There has been lots of regional and global commitments but despite all this, one thing stands out. Only two countries in the region are on track to meet the SDG 3.4 targets – South Africa and eSwatini, 45 countries are not… Malawi is a poster country for PEN plus, as is Rwanda. So, we have a model of what works from these two countries and the strategy was adopted by member states this year.” UNO NCD focal point
20. In 2020, a mid-term review of the GAP report showed that since inception, the number of countries with a policy, strategy, or action plan on NCDs had almost doubled. Half of member states however still lacked an NCD policy.[36]
21. At regional level the WHO AFRO set out recommendations in support of member states to implement the WHO Package of Essential NCD Interventions for primary health care in low-resource settings (PEN). This set out interventions that could be delivered at primary care level and through referrals to secondary care.[37]
22. Member states adopted PEN Plus in August 2022 at the Regional Committee for WHO AFRO setting out a regional strategy to address severe NCDs at first referral level health facilities. PEN Plus builds upon PEN to expand and strengthen the capacity of primary care facilities to detect and care for those living with chronic and severe NCDs at district hospitals with a focus on type 1 diabetes mellitus, advanced rheumatic heart disease and sickle cell disease, which are normally only treated in tertiary referral centres.[38] It is hoped that by focusing efforts on building diagnostic and complex disease management capacity at district hospital level, with routine follow up at health centre level that scale up of PEN will also be increased through supervision and mentoring for health centre staff.
“A good starting place, and one of the great advances we have made in the 15 years, is that there is now very clear and well evidenced interventions, actions, and policies that countries can turn to for guidance. 15 years ago, it wasn’t clear what would work, or any examples of previous interventions, however, now we can answer all those questions.” Vice President, NCD INGO
23. In 2022, African Centre for Disease Control and Prevention (Africa CDC) published the Africa CDC NCDs, injuries prevention and control and mental health promotions strategy 2022-2026 as a catalyst, seeking to bring together policies to support Member States in their strategic actions and implementation of activities. This is an African led strategy, with a view to complement other strategies already in place. The associated implementation plans are pending.[39]
What is the international funding landscape for NCDs?
24. NCDs are the largest unmet need in term of health financing in LMICs and receive very little external development finance. External financial support to countries in SSA still tends to focus on the unfinished agenda of the Millennium Development Goals (MDGs) and communicable disease control. This has increased following the ongoing pandemic of SARS Co-V virus which has increased attention on Global Health Security. The 2020 mid-term review of the GAP for NCDs showed that since 2001 only 1-2% of total Development Assistance for Health (DAH) has been targeted towards NCDs. This plateaued in 2013 at around $800 million per year. Figure 7 shows that lack of health development assistance to NCDs is a longstanding issue, despite the high number of DALYs attributed.[40]
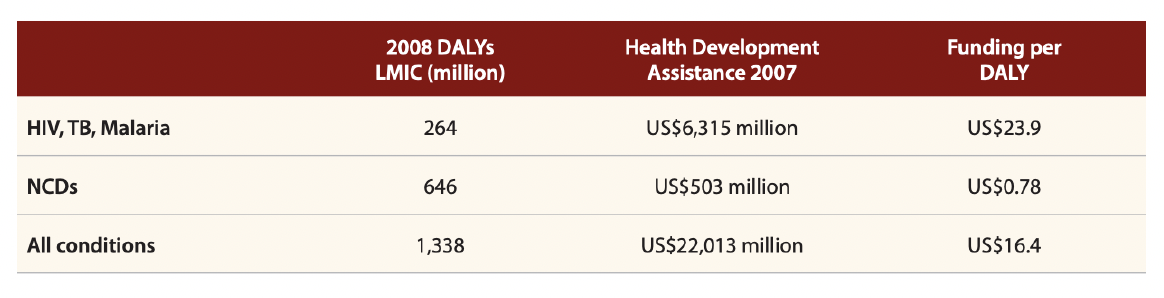
Source: Africa CDC (2022) Africa CDC non-communicable diseases, injuries prevention and control and mental health promotion strategy (2022-2026). Open access.
25. Globally between 2015 and 2017, $35.9 billion was spent on communicable disease control compared to $12.2 for NCDs. Of this 95% was generated domestically for NCDs, compared to 49% for communicable disease.[41] In terms of equity in 2011 only US$74m in external financing for NCDs went to the poorest countries accounting for 14% of all global development assistance for NCDs in 2011. This increased to US$83m by 2016 or 10% of global development assistance for NCDs and 0.3% of DAH in 2016.[42] Funding for NCD research and palliative care lags behind that of other NCD areas.[43]
Why should the Scottish Government invest in NCDs in Malawi, Rwanda and Zambia?
26. A summary of core demographic features of each country and basic health indicators is shown in Appendices 2-4 in the country snapshots. All three countries are currently classified as low-income countries (LICs) but each has a vision or plan for reaching LMIC or middle-income status (MIC).[44] Malawi and Rwanda are primarily rural with under one fifth of the population living in urban centres, whilst Zambia has undergone more rapid urbanisation with under half the population in rural areas. All have significant proportions of the population living in poverty (Malawi 50.7%, Rwanda 38.3% and Zambia 54.5%).[45]
27. Each of the three countries are relatively politically stable presently. Zambia has just experienced a change in government following a period of turbulence, including reforms to the MoH. These changes have been welcomed by international partners following several corruption challenges, mainly with regards to medicines procurement over recent years. In 2013, Malawi experienced corruption related issues in the health sector colloquially known as ‘Cash Gate’ which led donors to move away from Sector Wide Approaches and budget support. Rwanda has seen relative stability following the 1994 genocide under the leadership of President Kagame.[46]
28. In 2001, African Union Member States pledged to allocated 15% of their annual budget to improve the health sector, called the Abuja Target.[47] Malawi, Rwanda and Zambia have not met the Abuja target, with 1.8%, 9.9% and 8.0% allocated to the health budget from the total government expenditure respectively.[48]
29. All three countries receive substantial amounts of external health financing from Government donors, the UN and other partners with donors contributing to 74% of the health budget in Malawi, 56.8% in Rwanda, and 50% in Zambia (see Appendices 2-4 and 9-11).[49] Malawi is the only country that presently has a functioning donor pooled fund supported by the UK, Germany, and Norway, entitled the Health Services Joint Fund (HSJF).[50] In Zambia, corruption led to the dismantling of a Sector Wide Approach for health. According to anecdotal evidence from a KII, this, plus classification of the country as a LMIC in 2011, led donors to move support away from the health sector. Zambia has recently once again been classified as an LIC.
30. Each of the three countries have well-formed health sector strategies or plans which Malawi and Zambia are currently updating.[51] NCDs are a priority for each country and indeed each have developed an NCD plan or strategy, although Zambia’s, which was developed during the pandemic if SARS Co-V, requires further finalisation.[52]
31. NCDs place a significant burden of disease on the health of those living in Malawi, Rwanda and Zambia, causing 40%, 50% and 35% of mortality in 2019 respectively.[53] Malawi and Zambia have high HIV burdens, and there is strong and growing evidence of the link between HIV, its management and NCDs with comorbidity increasing in importance e.g. antiretrovirals (ARVs) linked to increased CVD risk, diabetes associated with increased risk of TB and pneumonia, and one third of cancer cases associated with infectious diseases.[54] The most common causes of death from NCDs across the three countries are cardiovascular disease, in particular stroke, followed by cancers, especially breast and cervical, digestive disorders and diabetes (Figures 8 and 9),[55] with incidence increasing with age, and late presentation being more common. Injuries place a substantial burden on the health sector with poor enforcement of speed and seatbelt legislation where this is available.[56] Each of the three countries is experiencing a demographic transition, as described in paragraph 8, meaning that without accelerated action the proportion of people at risk of living with and dying from NCDs is set to increase over the coming 20 years. Poverty remains a significant challenge, with consequent implications for the patterns of NCDs seen beyond the main four NCDs and mental health. Despite this, in 2019, eight per cent of government expenditure for health went towards NCDs (around US$2 per capita) in Malawi, 11% in Zambia (US$7 per capita). Two and three per cent of the health budget went towards management of injuries in Malawi and Zambia respectively.[57]
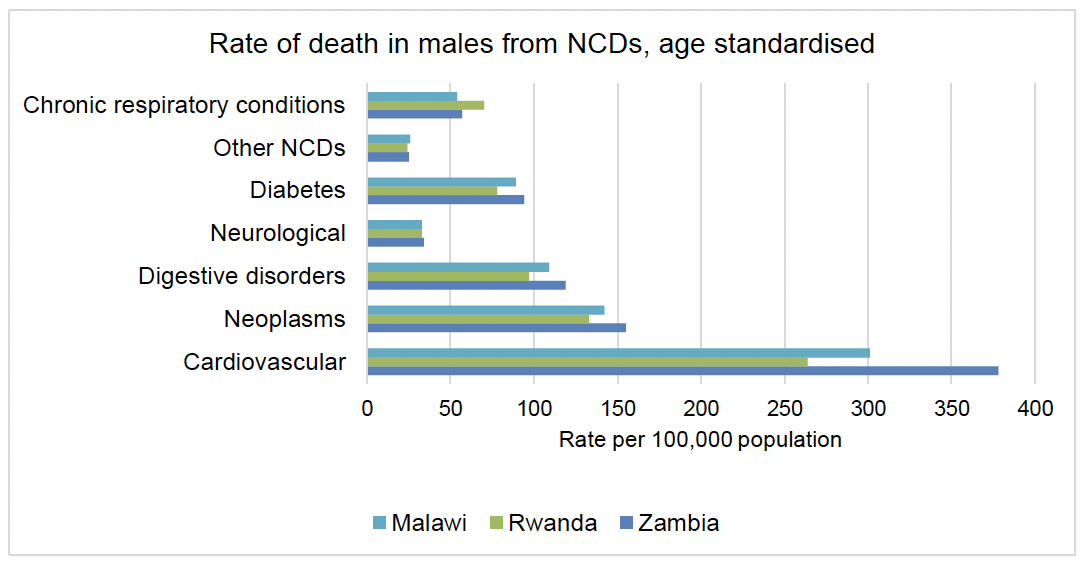
Source: Adapted from data from World Bank Data on Malawi, Zambia and Rwanda [accessed on 23/12/2022].
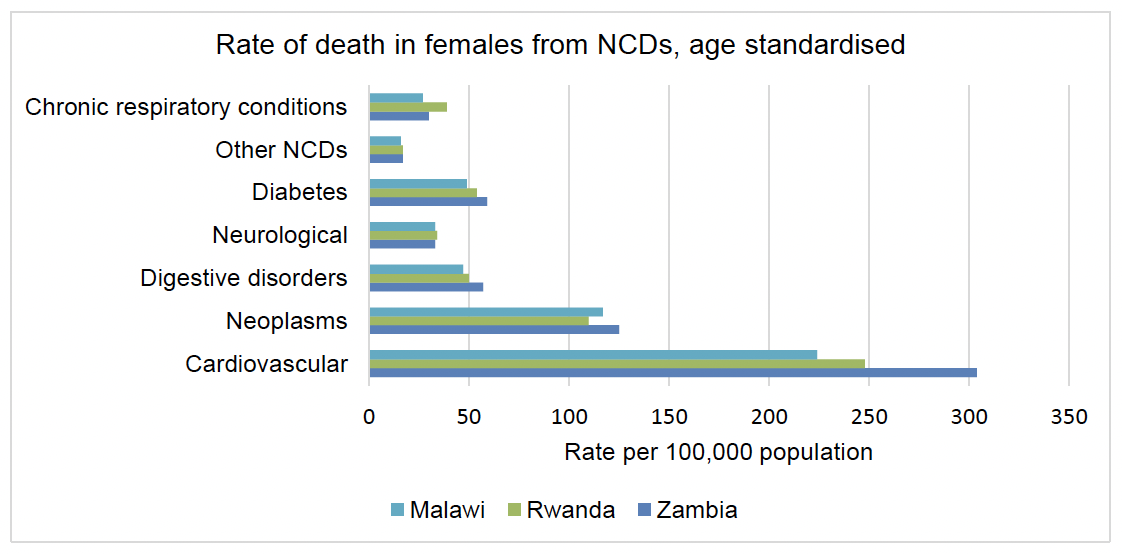
Source: Adapted from data from World Bank Data on Malawi, Zambia and Rwanda [accessed on 29/12/2022].
“For management of NCDs, PEN Plus is going to be a priority.” Individual working within the MoH, Zambia
32. All three countries are making progress against the GAP targets (see Appendices 5-7), predominantly with regard to policy making and some large-scale public health interventions. Progress on improving data collection, developing guidelines and treatment interventions has however lagged.[58] Rwanda and Malawi have prioritised a selection of NCDs including common and at times less severe diseases, such as asthma, hypertensive heart disease and epilepsy, alongside less common, more severe conditions such as type 1 diabetes, advanced rheumatic heart disease and sickle cell disease.[59] At present, a large proportion of care for NCDs is carried out at tertiary level,[60] however, all three countries have committed to decentralising patient care for NCDs and to use the PEN and PEN Plus models to address these priorities.[61]
“Rwanda probably the most advanced with NCDs in Africa. They have a really good government and lots of support from funders. Malawi is probably second.” INGO worker
33. In terms of roll out of PEN and PEN Plus Rwanda and Malawi have both made significant progress (Figure 10). Rwanda has rolled out PEN across much of the country and is now working to scale up PEN Plus. In Malawi 40 facilities across all districts now offer PEN and international support is helping scale up of PEN Plus. In Zambia, whilst there is a commitment to roll out PEN, implementation of this has been slow, with only one district in the Copperbelt receiving the pilot training. Efforts are currently underway to set up two training sites for PEN Plus, led by a national implementing partner and partnership between a US and Zambian University (anecdotal evidence from KII).[62] As noted earlier, it is hoped that the current focus on PEN Plus will have indirect benefits for the scale up of PEN through provision of training and mentoring for the ongoing routine management of those diagnosed with complex NCDs at health centre level as part of PEN PLUS.[63]
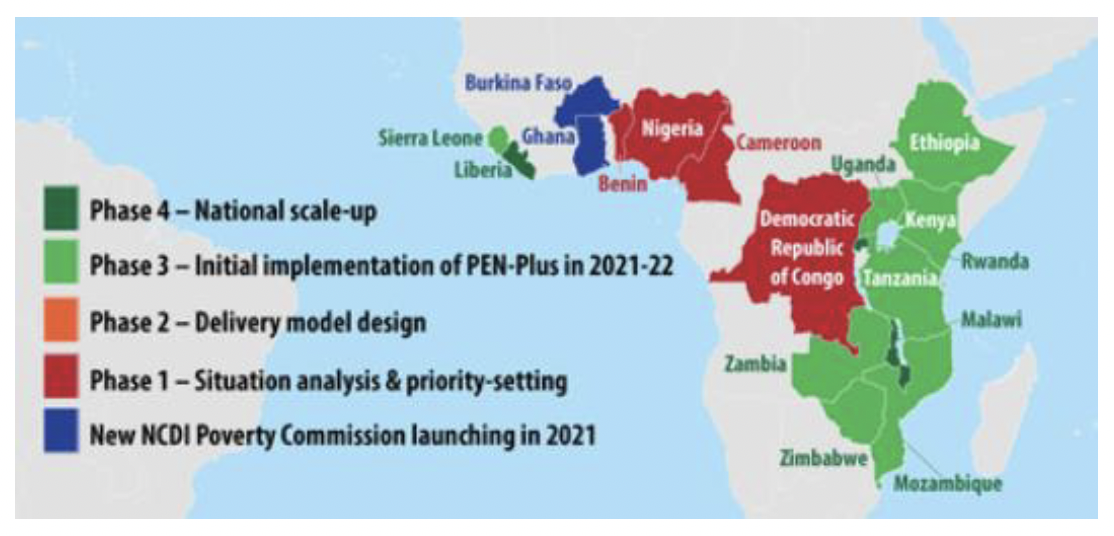
Source: NCDI Poverty Network, 2022. Reproduced with permission.
“There is a Zambian tradition that people do not complain about something which is not painful. Anything serious must cause pain or disfigurement.” Zambian academic
34. Despite the progress made, coverage remains poor, particularly in Malawi and Zambia. Lack of access to diagnostics and long-term supply of medications, including blood pressure monitors and glucose strips act as a barrier to management (Table 1). It was noted by a KI that screening for NCDs only happens as part of antenatal care, or when travelling for a job. Separately another KI noted that checks for NCDs, such as blood pressure monitoring, only happen on demand, and there are many missed opportunities to screen people for NCDs, in part due to lack of awareness of providers. Whilst diagnosis and initial treatment is technically covered by national health insurance schemes, out of pocket (OOP) payments are common, also limiting the ability of the poorest to access care.[64] This coupled with lack of training and poor patient data collection and follow up have challenged role out of PEN and PEN Plus,[65] although efforts have been made to integrate data collection for NCDs into the national systems in Malawi. Human resources for health are sparce across all three countries, requiring task shifting and cross specialism, with Malawi having one of the lower ratio of doctors to population in the world.[66]
“OOP expenditure for chronic disease can be so high. We need to think how can we bring the treatment closer to the patients and how can we target these high risk groups.” Individual working for the MoH Malawi
| Availability of equipment and medications for trained staff to treat prioritised conditions | ||||
|---|---|---|---|---|
| Condition | Hospitals with availability of | Health centres with availability of | ||
| Equipment and medications | Trained staff | Equipment and medications | Trained staff | |
| Type 2 diabetes | 63% | 29% | 12% | 5% |
| Cardiovascular disease | 17% | 34% | 1% | 10% |
| Chronic respiratory disease | 4% | 23% | 2% | 8% |
| Rheumatic heart disease | 34% | 1% | ||
| Type 1 diabetes | 42% | 2% | ||
Source: Republic of Malawi (2021) Malawi PEN Plus Operation Plan. Reproduced with permission.
35. International support for NCDs in the three countries is limited (see Appendices 9-11). Stakeholder mapping shows external stakeholder priorities for development assistance for health. Many partners interested in NCDs are outside traditional government donor partners, often supporting disease specific areas or piloting of approaches. Whilst many donors are supportive of efforts to attain Universal Health Care (UHC), there is a risk that unless explicit attention is given to NCDs within this agenda, targets will not be met.
36. Support for palliative care was noted to be even more limited than for diagnosis and management of NCDs as a whole. Each of the three countries have central cancer referral centres that in addition to diagnosis and some treatment of common cancers, also provide some palliative care to those terminal from cancer related diagnoses, however, availability of opiates and other palliative care medicines remain a challenge. According to interviews, support for palliative care at decentralised levels is scant, including for those terminal from NCDs such as end stage renal failure, or respiratory failure from chronic heart disease. Previously palliative care was provided at community level for HIV, with funding from PEPFAR providing support until the early 2000s. With the scale up of treatments for HIV and improved survival funding was redirected towards treatment and palliative care support ceased. KIIs from each of the three countries recalled the strength of these programmes with specific requests from Rwanda to SG to support set up of community models to deliver palliative care.
37. In addition to donors providing development finance, there are a range of civil society or patient advocacy groups, with varying degrees of success. The NCD Alliance works internationally to raise awareness of NCDs through work with its federation associations. These are functional to varying extents in the three countries, with the most organised in Rwanda and Malawi. In Zambia, lack of funding led to cessation of activities by the NCD Alliance lead in country, but recently efforts have been made to reawaken the group.
What is the link between NCDs and gender?
38. This section considers how gender interacts with NCDs across SSA, focusing on differences in burden of disease, risk and access to care. The section also shows how the report considered gender in terms of those interviewed in order to avoid bias.
39. Whilst commonly assumed that NCDs predominantly affect men, the situation is more nuanced and two of every three deaths in women are a consequence of a NCD.[67] Figure 3 (see p.16) shows how gender affects morbidity from NCDs at global, and regional level across SSA. It demonstrates that at an aggregate level the burden of NCDs is higher in men than women and that this is largely driven by cardiovascular disease, the most common cause of morbidity and mortality. When you look beyond aggregate data differences start to be seen for example in SSA women experience a greater burden of disease from neoplasms (cervical and breast cancer) with more than 65% of all cancer cases in 2017 in SSA affecting women.[68]
40. Further differences become apparent when we analyse age and sex disaggregated data as per Figure 4 (see p.18). Here again the role of cardiovascular disease in driving disease burden across both sexes in adults over 40 years of age can be seen particularly in men. Mental health disorders are important at younger age groups, and neoplasms account for a higher proportion of disease, particularly for women from the age of 35 onwards.[69] Digestive disorders appear to have a greater impact in men, as can be seen in Figure 8 and 9.[70] Chronic respiratory diseases cause the third largest burden of disease across SSA and affected over 70 million people in 2017, more than half of those affected were women.[71] A recent systematic review found that women with chronic obstructive pulmonary disease were younger, smoked less, had a lower body mass index, and were more likely to be of lower socioeconomic status than their male counterparts which shows the importance of nuance when exploring the gender dynamics of NCDs in SSA.[72] The data show a similar pattern when we explore the burden from NCDs for the three partner countries.
41. Although behavioural risk factors affect both sexes, it is commonly reported that women can be exposed to risk factors disproportionally due to lower levels of education and lower exercise levels due to gender and social norms, especially those who are from lower socio-economic status. Across the three partner countries, more men (20%) than women (8%) smoke and men are more likely to drink alcohol (see Appendices 2-4).[73] In Malawi, the proportion of women that are overweight (27.4%) is much higher when compared with men (9.4%).[74] This disparity is noted when considering proportion of the population not meeting the WHO recommendations for physical activity for health, with twice as many women than men not engaging in sufficient physical activity (men 0.9%: women 1.8%). This was mirrored in Zambia with 10% of the population not engaging in sufficient physical activity, with the gender disparity greatest when considering vigorous activity, with 45.5% of women reporting no vigorous activity at all, compared to 23.9% of men.[75] Salt intake, which is an important risk factor for cardiovascular disease, was higher in men than women in Zambia however consumption of vegetables was similar across both sexes.[76] They are also more likely to be exposed to indoor air pollution which also has a disproportionate impact on children and those living in rural areas.[77]
42. Biological risk factors for cardiovascular disease or chronic kidney disease include hypertension, high glucose levels and high cholesterol. In Malawi, screening for hypertension was substantially higher in women with 81.7% of men never being screened for blood pressure, compared to 49.9% of women. A similar picture was seen in Zambia, where two thirds of men had never been screened, compared to one third of women, and in Rwanda where more than twice as many women as men had ever had their blood pressure measured, with 29.9% of women screened compared to 11.8% of men. Correspondingly, in Malawi, more women than men had been diagnosed with hypertension in the last 12 months but in Rwanda, men were found to be more likely to have hypertension, and for this to come on at a younger age.[78] In Zambia, there were marked differences in the proportion of men and women on treatment in those diagnosed with 23% of women with diagnosed hypertension on treatment compared to 9% of men. This was also the case when you look at control of hypertension with 11.4% of women well controlled compared to 2.5% of men.[79] 99.8% of respondents to the Malawi STEPS survey had never been tested for cholesterol, but of those tested women had a higher mean cholesterol level than men. Blood glucose was similarly found to be marginally higher in women than men. In Rwanda, women were found to be slightly more likely to have high cholesterol, but there was found to be no difference between men and women when glucose level or evidence of kidney disease were reviewed.[80]
43. It is well documented that women face barriers to accessing care for example, prioritization of other family members for healthcare, high travel times and costs to access clinics, limited financial decision making and stigma related to gender specific illnesses, such as cervical and breast cancer.[81] Despite these documented barriers to accessing care, both anecdotally from the KIIs, and from reviewing the three STEPS surveys from the partner countries women appear to access NCD screening and treatment more effectively, for example, with more women on effective treatment for hypertension.[82] Two small studies, from Zimbabwe and Uganda both show women are more likely to approach traditional healers than men for their diabetic care and that women were engaged in their follow up care. One of the studies also showed that women are more likely to approach free government facilities whereas men would attend private for-profit clinics.[83] Within mental health, one study in Rwanda showed poor health seeking behaviours in men were more pronounced than in women.[84] There is however very little data for health seeking behaviour for NCDs in SSA.
44. Whilst conducting this study, the consultants were mindful to ensure data, opinions and expertise were gained from both sexes. Of the 48 KIs that were interviewed, 29 were female. They included women in government positions, working within donor agencies and as directors, vice-presidents and programme leads in international and national NGOs.
Contact
Email: socialresearch@gov.scot