Community sentencing options for people with substance use problems: review findings summary
Summary findings from review of community sentencing options for people with substance use problems.
Annex 2: Applying the evidence to current practice in Scotland
Annex 2 reports findings from the review of data on Scottish practice and assesses the extent to which current approaches reflect or foster the elements of good practice identified in Annex 1.
It addresses:
- The role and aims of sentencing, and the place of DTTOs and CPOs within it
- Eligibility, targeting and assessment of people for treatment-based orders, and the extent to which this appears to reflect good practice, and whether further consideration or enquiry may be warranted in order to better align with the evidence
- How treatment-based orders are delivered and supervised in practice, and the extent to which this appears to reflect good practice, and whether further consideration or enquiry may be warranted in order to better align with the evidence
- The characteristics of people in the Scottish justice system who use drugs
1. The role and aims of sentencing in Scotland
The role of sentencing is complex. Most scholars agree that any working approach to sentencing must hybridise retributive and utilitarian approaches to sentencing – that is, that they must find a balance between responses driven by the person's past criminal actions and punishing them for those actions, and those driven by decreasing future harm by reducing the person's likelihood of reoffending or deterring others from committing crimes.
In Scotland, this balance is sought through the Scottish Sentencing Council's (2018) Sentencing Guideline: Principles and Purposes of Sentencing, which apply to all sentencing decisions in Scotland. This guideline states that a sentence should be the one best suited to "achieve the purposes of sentencing that are appropriate to the particular case" – suggesting that different cases may warrant prioritisation of different purposes. The purposes they specify are:
- Protection of the public via preventative measures and deterrence
- Punishment
- Rehabilitation of offenders, to reduce their risk of reoffending and allow them to change and move past offending
- Giving an opportunity to make amends, acknowledging the harm caused to both victims and communities
- Expressing disapproval of the behaviour and reflecting society's concern about it.
The guidance also states that in achieving the appropriate purpose of a particular sentence, the efficient use of public resources may be taken into account.
2. Sentencing and substance use
However, the role of a person's substance use in judicial decision-making further complicates things. Sinclair-House et al (2020) note that in both the liability and sentencing stage, sentencing guidelines consistently characterise intoxication as aggravating and mental illness as mitigating.[7] Where an offender presents with a substance use disorder, potentially involving elements of both mental illness and intoxication (or, at least, historic intoxication), sentencing guidance is lacking. In their survey of sentencers in England and Wales, they found that sentencers gave significantly lighter prison sentences to people described as having a particular neuropsychiatric profile due to disease, than if an identical neuropsychiatric profile was due to heroin dependency. Moreover, they found that belief in the person's choice to acquire the dependency was a key component of this effect, and that evidence of dependency was more likely to evoke punishment considerations than rehabilitation.
While the above research took place in the English and Welsh system, the Scottish Sentencing Council's (2021) Sentencing Guideline: The Sentencing Process raises a similar dilemma. In this Guideline:
- The offence being committed "whilst under the influence of alcohol or drugs which were consumed voluntarily" is listed as a possible aggravating factor
- The person having a "mental illness or disability, especially when linked to the commission of the offence" is listed as a possible mitigating factor
- Having "demonstrated a willingness to address their personal problems and to change their offending behaviour, including addressing any drug, alcohol or mental health issues" is listed as a possible mitigating factor
- Sentencers are advised "Cases may have both aggravating and mitigating factors. Whether any factor has an aggravating or mitigating effect will depend on all of the circumstances of the case."
This guidance gives individual sentencers discretion to interpret:
- How important each factor is in relation to one another
- The meaning of substances being "consumed voluntarily", especially in the context of dependency
- The extent to which substance use constitutes a "mental illness or disability" in its own right, and the extent to which this affects the commission of offences
- The extent to which mental illness may cause a substance use problem, or a substance use problem may mask an underlying mental illness
- How a person may "demonstrate a willingness to address their personal problems", how far that willingness must extend, and how much the sentencer must share some belief in their likelihood of success.
Additionally, a further implicit goal for sentencing has guided changes in sentencing frameworks in Scotland over recent decades: the Scottish Government's policy priority of shifting the balance between use of custody and justice in the community , has led to changes including:
- the legislative presumption against short sentences (of three months or less) in 2010,
- the advent of Community Payback Orders from 2011,
- the creation of Community Justice Scotland and local Community Justice Partnerships from 2017, and
- the extension of the presumption against short sentences to 12 months or less in 2019 – although it should be noted that sentences under 12 months have still been imposed each year since.
While judicial decision making is driven by the specific circumstances of each case, rather than population level considerations such as reducing the number of people in prison, these policies and laws shape the context in which sentencers decide which available sentence will best serve their intended purposes in each case.
Despite the measures listed above, it is worth noting that Audit Scotland concluded in 2021 that the aims of reducing imprisonment and increasing community sentences have not yet been achieved, with Scotland's incarceration rate still amongst the highest in Western Europe.
Studies exploring judicial decision making are very rare in Scotland. However, the Scottish Sentencing Council recently published an Issues Paper on judicial perspectives of community based disposals (2021). While not specific to people with substance related problems, it is informative to note that this report found that:
- Some sentencers perceive a need for greater consistency in provision of community-based programmes and services
- One of the greatest challenges to judicial confidence in community-based disposals concerns limitations of resources to support their management and delivery
- Judicial awareness of available services in each area could be improved
- Sentencers have noted that breach proceedings have the potential to take significant periods of time, and some would desire earlier reporting of breaches to the court
- Sentencers generally desire greater flexibility to impose what they see as an appropriate sentence for each specific case
- Some sentencers see Covid-19 pandemic related disruptions as having negatively impacted the efficacy of community disposals, and in some instances this has affected sentencing practice.
These findings appear consistent with Garrett et al's (2019) work on judicial decision-making in the US. They report: "our findings support the "treatment resource hypothesis" as one explanation for variation among courts and judges in the extent to which alternative sentences are offered to low risk offenders… providing these resources will be crucial in reducing mass incarceration." The authors found that all measures of treatment resources were strongly related to the frequency with which judges gave out non-custodial alternative sentences. Similarly, Monahan et al (2018) also found that most judges in their Virginia, USA study supported the principle of alternative, treatment based sentencing, but felt alternatives to custody in their jurisdiction were "inadequate at best".
The Issues Paper mentioned above followed an earlier report published by the Sentencing Council (2019) on a discussion event amongst members of the judiciary and representatives of various health, social care and justice stakeholders regarding sentencing people with mental welfare issues. It noted that:
- Participants perceived systemic challenges in information sharing, which, if overcome, could increase the amount of information available to the courts at sentencing.
- In some cases a defence solicitor may be the first person in a position to consider whether the person has a mental health difficulty that should be brought to the attention of the court. This may have an impact on what assessments the court orders, and consequently which sentencing options are available.
- Sentencers expressed a desire for more detailed information from community justice social workers about interventions and programmes available, for example more on what is involved, how long they take, and waiting times, so that they could have more confidence that a community sentence would be effectively implemented.
- Long waits for psychiatric, psychological or Mental Health Officer reports seem to be more likely to delay sentencing than waits for Criminal Justice Social Work Reports. Participants "noted that many offenders may have a cluster of issues – for example a personality disorder, substance use issues, and adverse childhood experiences – and that additional resources might be required to investigate and obtain information in relation to each."
- In relation to which issues or conditions might constitute a "mental disorder" for the purposes of sentencing, "some attendees noted that the inclusion of 'substance use disorder (drugs/alcohol)' would risk bringing a very large number of offenders within the scope of any such guideline, and that it may be preferable not to include this." The reasons behind this view are not enumerated in the report.
- Participants felt that "the level of resources and support available to offenders through Drug Treatment and Testing Orders, together with the multidisciplinary approach of such orders, is not generally available to offenders with mental welfare difficulties."
For sentencing people with mental welfare issues, "a package of measures similar to those available under drug treatment and testing orders was favoured, adopting the same multi-disciplinary approach, and providing the same type of care and support. The Structured Deferred Sentence court was suggested as a model of the type of monitoring and support that the court – with the appropriate level of support from the local authority and social work – could seek to provide in appropriate cases. Again, the provision of the necessary resources for such an approach was recognised as being outwith the Council's remit."
3. Sentencing options and details of orders
Sentencing options
Currently in Scotland, courts have a range of sentencing options they can impose for offending behaviour, including a prison sentence at the most restrictive end, and a spectrum of community orders with various degrees of restriction or requirement on the person's movements or behaviour. The range of sentencing options available in a given case may depend on a number of factors, including the offence being prosecuted and the level of court in which the case is being heard.
Some features of the current landscape include:
- A legislative presumption against prison sentences of less than 12 months.[8]
- No person under the age of 21 may be sent to prison. The only custodial disposal available (whether by way of sentence or otherwise) in the case of persons other than children who are not less than 16 but under 21 is detention under section 207(2) of the Criminal Procedure (Scotland) Act 1995.
The introduction of Community Payback Orders from 2011, and the subsequent creation of Community Justice Scotland and local Community Justice Partnerships from 2017.
- Efforts to develop more opportunities for people to be diverted from the harms of the justice system at earlier stages, including:
- the Recorded Police Warning system, which provides police officers with a means of dealing with certain less serious offending behaviour.[9]
- diversion from prosecution, where an accused person is referred to local authority justice social work (or a partner agency) for support, treatment or other action as a means of addressing the underlying causes of the alleged offending and preventing further offending.
However, despite these measures, Audit Scotland concluded in 2021 that the aims of reducing imprisonment and increasing community sentences have not yet been achieved, with Scotland's incarceration rate still amongst the highest in Western Europe.
Geographically, courts and the community sentences they impose operate within slightly different administrative bureaucracies. The court system has six Sheriffdoms, which break down into 39 district Sheriff Courts, and each person will appear in the court for the area where the offence was committed. However, community sentences are served in the area where the person lives, and are primarily delivered by justice social work teams who are typically employed by local authorities (of which there are 32), and work with Community Justice Partnerships (of which there are 30), regional NHS Boards (of which there are 14) and local Alcohol and Drug Partnerships (of which there are 31). This is a complex bureaucratic landscape, and, notably, one that means sentencers may have different disposals or interventions available to them in each case, depending on where the person being sentenced lives.
The two main community orders options specifically aimed at people with substance use problems are a Drug Treatment and Testing Order (DTTO) or a Community Payback Order (CPO) with a drug treatment requirement. For both orders, the person must confirm that they are willing to comply with the relevant requirements before the order is made – although it is important to note that a prison sentence is a possible alternative, so the voluntariness of such consent may be contested.
The two orders have slightly different legal definitions – a CPO is a sentence of the court, while a DTTO is an order instead of a sentence. This creates a technical distinction in the person's status, with CPO recipients being convicted and sentenced, while DTTO recipients are convicted with no sentence passed. However, the orders function in broadly the same way. For both orders if the person fails to comply the court may vary or revoke the order, or impose any sentence competent for the original offence, but should take account of the time spent on the previous order. Both orders are also listed in Section 5D(2) of the Rehabilitation of Offenders Act 1974, and consequently have the same disclosure periods in respect of the person's criminal record.
The next section characterises each of these orders in more detail.
4. Characterising DTTOs
A Drug Treatment and Testing Order (DTTO) is a disposal given instead of a sentence. DTTOs operate under s234B – 234K of the Criminal Procedure (Scotland) Act 1995 (inserted by s89-95 of the Crime and Disorder Act 1998), and are supported by Scottish Government "DTTO Guidance for Schemes" (2011).[10]
As first conceived, the DTTO drew heavily and consciously on the principles of the US Drug Court model (Collins, 2019) – focussing primarily on drug treatment and rehabilitation, while using the authority of the court to encourage compliance.
Main features of a DTTO
- The key legislative criteria for a DTTO are that it may only be imposed where the court is satisfied that:
- the person is dependent on or has a propensity to use drugs and
- their dependency or propensity to misuse drugs requires and may be susceptible to treatment and
- they are a "suitable person" for the order
- Additionally, there should be a suitable justice social work team in place to supervise the order, and local services that will meet the person's drug treatment needs, which they can access within a short timeframe.
- While not a legislative requirement, practice guidance suggests that the person should be "facing the likelihood of custody" due to the seriousness, frequency or pattern of offending.
- The order is considered intensive and 'high tariff' due to its use of resources and the demands it makes on the person's time. On the order, the person will be expected to:
- Attend scheduled drug testing, as frequently as specified by the court in the order
- Regularly submit to random unscheduled drug testing
- Enter residential drug treatment, if required as part of their treatment plan
- Regularly attend drug treatment appointments and engage with drug treatment
- Regularly maintain contact with their supervising justice social worker so they can monitor treatment engagement and progress
- Attend court for review every month, where the judge will consider their testing results, treatment engagement and progress, and determine whether they may continue on the order
The order is intended to focus solely on treating substance use, and legislation specifically limits the social worker's role to only facilitating this. Therefore, the person is not required to engage with, and the officer is neither required nor allowed to expect the person engage with support or interventions for any other criminogenic or wellbeing needs they have.
DTTOs are widely, but not universally, available across Scotland. In order for DTTOs to be available, local authorities need to:
- provide assessments and supervision of orders, through a justice social worker (the "supervising officer" in the legislation's language). Guidance states this should be a specialist DTTO team, or designated DTTO staff, within a wider justice social work department.
- develop arrangements for people on DTTOs to receive multi-disciplinary assessment and rapid access to treatment and testing. There is no prescriptive guidance on how this should be structured or managed, and different areas currently take different approaches.
5. Characterising CPOs
Community Payback Orders (CPOs) replaced community service orders, supervised attendance orders and probation orders in 2011. They are a sentence, and operate under s227A-227ZO, and schedule 13 of the Criminal Procedure (Scotland) Act 1995.
A CPO is a general order, not necessarily focussed on addressing a specific need for the person convicted. The legislative eligibility criteria are only that the person is convicted of an offence punishable by imprisonment, and the court is of the opinion that the offence (or combination of offences) is "serious enough to warrant" such an order.
Additionally, there must be a "responsible officer" (in practice, a justice social worker) in place to supervise the order.
Main features of a CPO
- Each CPO is centred on a requirement that the person either attend supervision appointments with a justice social worker, perform unpaid work or another activity, or both. In addition, the court may add other requirements in order to tailor the sentence to the person's needs. The additional requirements may be for the person to:
- pay compensation
- attend a specific programme
- reside at a specific address
- engage with agreed mental health treatment
- engage with agreed drug treatment
- engage with agreed alcohol treatment
- engage in any particular "conduct" the court specifies in the order
- restrict their movement (which may or may not be electronically monitored).
- In order to impose a drug treatment requirement as part of a CPO, the legislative criteria are very similar to a DTTO: the person must be "dependent on", or have a "propensity to use", drugs, and be "potentially susceptible to treatment". Additionally, there needs to be local services that will meet the person's drug treatment needs, which they can access within a short timeframe. Drug treatment requirements can only be imposed with supervision.
- Due to their flexibility, the intensity of a CPO can vary widely. They are considered relatively high tariff, in that they are an explicit alternative to a prison sentence. However, for people with substance use problems, when compared to a DTTO, some aspects of the CPO may be seen as less intensive or demanding. Practice guidance suggests that CPOs with a drug treatment requirement should be considered for those whose offending history is not high tariff enough to warrant a DTTO.
- On a supervised CPO, the person will be expected to:
- Regularly attend supervision appointments with their justice social worker, and engage with the interventions they instruct to address their criminogenic needs
- Receive unannounced home visits from their justice social worker
- Only attend court for review if required
- On a supervised CPO with a drug treatment requirement, the person will be additionally expected to:
- Enter residential drug treatment, if required by their treatment plan
- Regularly attend drug treatment appointments and engage with drug treatment
CPOs are available in all areas across Scotland, and delivering them is one of the major functions of all justice social work departments.
6. Eligibility, targeting and assessment
Eligibility criteria
At a macro level, CPOs and DTTOs are available for similar populations. Both are for people whose offending is sufficiently severe that they have not been diverted from the justice system earlier, are imposed in situations where the person might otherwise receive a prison sentence, and can provide (and require compliance with), drug treatment for people who use substances problematically.
However, being a more flexible and general-purpose order, a CPO is potentially both available and suitable to a wider range of people. For example:
Offending seriousness: DTTOs and CPOs have similar "maximums" for offending seriousness, being determined by the point at which a court feels it is necessary or appropriate to imprison the person. However, in practice CPOs may, on average, have a lower "minimum" offending severity, giving them a wider range overall. This is because DTTO practice guidance recommends them only for circumstances where the person is "facing the likelihood of custody" because of the seriousness, frequency or pattern of their offending. For a CPO the person needs to have been convicted of an offence punishable by imprisonment, and for the court to consider the offending "serious enough to warrant" a CPO (s227B(2) of the 1995 Act). DTTO IIs were brought in with the intention of encompassing people whose offending is not sufficiently high tariff to warrant a full DTTO, but these are not widely available across Scotland.
Substance use: In relation to imposing drug treatment through either order, both a DTTO and a CPO Drug Treatment Requirement have the same eligibility criteria: that the person has a "dependency on or propensity to use" drugs, and that this behaviour may be susceptible to treatment. However, the practice guidance for each order encourages social workers conducting assessments to consider DTTOs as being suitable for people with more severe or complex drug issues.
Readiness for change: The legislation only requires, for both orders, that the person consents to the order being made. However, practice guidance indicates that CPOs may be more appropriate when "the person is earlier in developing readiness to change". The practice guidance for DTTOs also suggests that motivation to comply with the order may be a factor in considering whether the person meets the additional requirement that they be a "suitable person".
Wider needs: Eligibility is potentially affected by the requirement to be a "suitable person" for a DTTO. There is no legislative definition, but the practice guidance indicates that this includes the person's motivation to comply with the order, and also that schemes may not be suitable for people with co-occurring mental health problems or insecure housing.
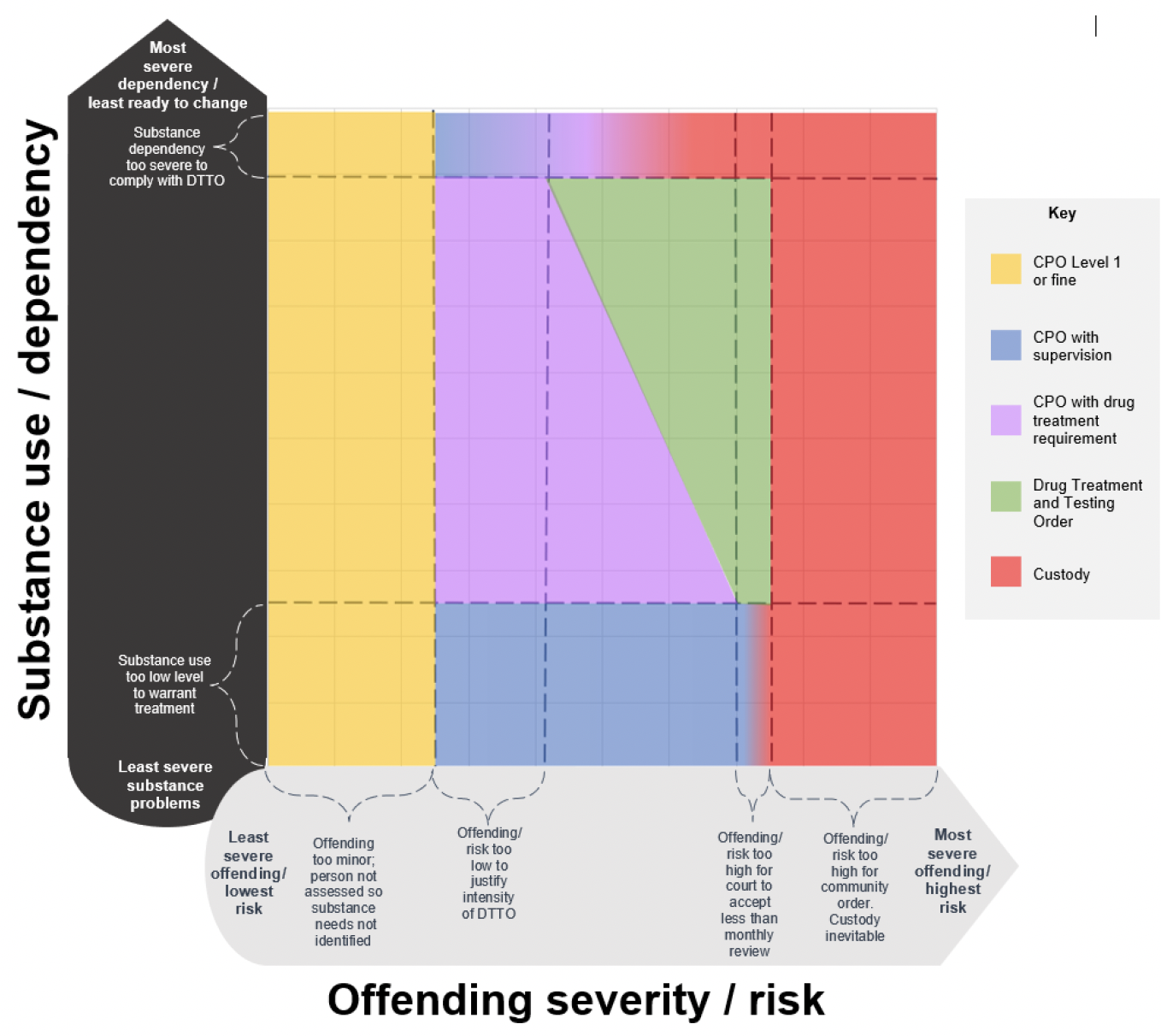
Eligibility for each order in relation to the other
The figure below is highly reductive, but seeks to illustrate, broadly, where the eligibility criteria for the different Orders sit in relation to one another, based on the two main factors governing court and social work decision-making in relation to DTTOs and CPOs:
- offending related considerations such as severity and risk, and
- substance use related considerations such as degree of dependency and motivation to change.
It is based on interpreting the logic and thresholds of the legislation and guidance, not on data about the number of orders or distribution of the population. It is presented here only to show how the orders' criteria relate to one another in who they are intended for, and does not reflect the actual size of the relevant populations. Additionally, the boundaries presented are based only on the judgments that are made in the process of applying the legislation and guidance. In reality, these are not strict lines, but threshold ranges that would vary based on the other factors not presented in this chart.
While this diagram does not show the number of people in each population, it does help to highlight some particular types of situation that may either not be well served, or pose difficulties in tailoring an appropriate response. In particular, the areas of the chart circled on the smaller illustration below:
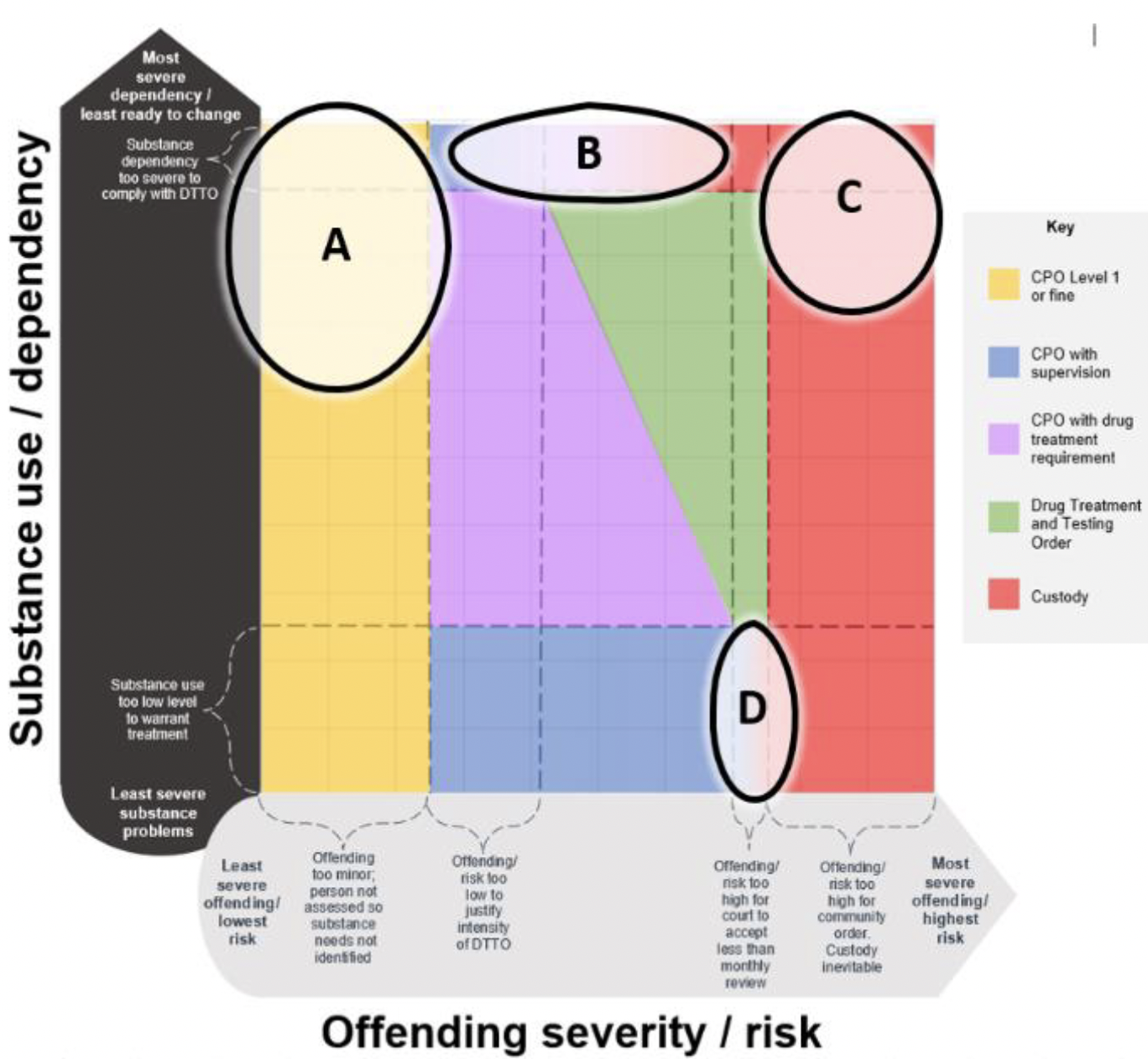
A. These people have relatively high substance related problems or severe dependency, but whose offending is too low level to trigger a social work assessment.
Their needs are therefore not identified or made known to the court. While a treatment-based order would not be appropriate to most people in this category because it would reflect up-tariffing, by not assessing them the opportunity is missed for social workers to support them into voluntary treatment or refer them to harm reduction interventions if they are open to this. The Care Inspectorate (2021) found, across the 5 local areas they inspected, that approaches to identifying risk and need for this group varied, and that areas where a local process was established were more consistent in identifying, escalating and recording concerns and responses to this group's risks and needs.
B. These people have very high substance dependency or complete unreadiness for change, and may struggle to comply with a treatment order.
In these cases, there is no obvious alternative sentence, and the social worker and court will both need to consider carefully the best way to address the person's needs. This could result in a wide range of different outcomes including:
- SDS (Structured Deferred Sentence): If available in the area, a structured deferred sentence would provide an opportunity to develop the person's readiness to change and gather more information on which to base the judgment about their ability to comply.
- CPO: If the court is willing to accept a CPO with treatment as adequately intensive for the offending, and the person may be better able to comply with this than with the testing and monthly monitoring of a DTTO, a CPO with treatment requirement might be given.
- If the court is willing to accept a CPO with requirements addressing other criminogenic needs as adequately intensive for the offending, a CPO with other requirements may be given.
- The CPO can also be tailored to the specific case, for example by scheduling reviews. However, as this group is defined by their difficulty complying and engaging, the more oversight the court gives itself the more likely it may be that the person ultimately cannot complete the order.
- Custody: If the court does not feel that there is a community based option that is both sufficiently intense to be proportionate to the offending, and possible for the person to comply with, a custodial sentence is likely.
C. These people have high substance dependency and severe offending behaviour.
This group are unlikely to be suitable for community based orders, but also unlikely to benefit from, or make progress during, a prison sentence. Additionally, a prison sentence reduces the treatment options available, and may increase their chances of a drug related death on release, and/or of further offending. Other models of secure treatment may be more appropriate to this population, although availability of these in Scotland is limited.
D. These people have relatively low level substance related problems, but high level offending.
For this group, their substance use may not warrant the intensity of a treatment order, but the court may not be comfortable to leave them in the community without frequent monitoring. The most likely outcomes for this group are either:
- - Custody: If the court considers the severity of offending to be the main consideration in the case, or the person's reoffending risk too high, custody may be inevitable.
- - CPO: With requirements to address other criminogenic needs, and tailored with extra review hearings. This order may provide social work an opportunity to support the person to engage voluntarily with drug treatment or harm reduction.
Assessment and sentencing procedure
The specific procedures and assessments used will vary depending on local court practice, local authority social work arrangements and local health board and ADP arrangements. However, generally speaking, the following describes a simplified, typical process for someone with a substance use problem facing sentencing.
Step 1 – Assessment
All people convicted of a crime will have a date set for their sentencing. The process for arriving at either a DTTO or a CPO with a treatment requirement begins the same way – with the court requesting a justice social work report before sentencing.
Sentencers do not have to request a report in all cases (further information is available in the Scottish Government's 'Justice social work reports and court-based justice social work services' practice guidance). A report is, however, usually requested where a community sentence is being considered.
The court can not impose a CPO unless it has obtained, and taken account of, a justice social work report (an exception to this is a CPO with a Level 1 unpaid work requirement only).
How are people assessed?
The Justice Social Work Report is an important source of information that the court will consider when sentencing the person, but not the only source. It is intended to complement a range of other considerations, including victim information or impact statements, and narratives from the Procurator Fiscal. Justice Social Work Reports appear to be generally high quality sources of information – the Care Inspectorate (2021) rated most they reviewed (across 5 local areas) as good or better, and very few as weak, and noted that Sheriffs viewed them as helpful to their decision-making regarding community disposals. However, stretched workloads and time pressure do appear to reduce the quality of these reports, with the Inspectorate noting that "a higher proportion of assessments we rated as very good or excellent had been completed in accordance with the 20-day threshold than those we rated adequate or weak, where almost half were outwith the 20-day timescale".
Who gets a Justice Social Work Report?
It is important to note, in relation to understanding people's drug use, that no data are available for people who are not assessed.
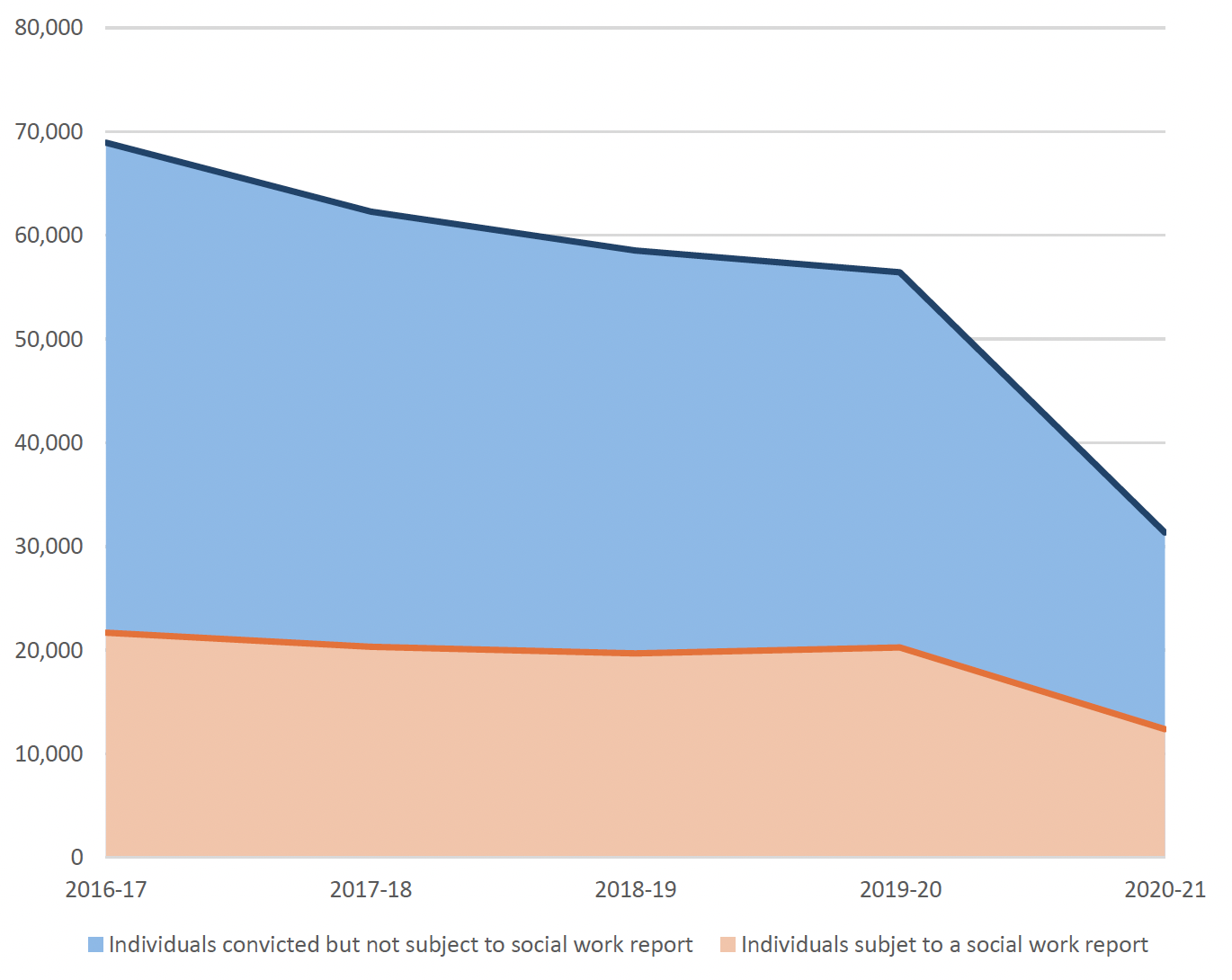
Criminal Proceedings statistics show that 31,344 individual people were convicted in 2020/21, while Justice Social Work statistics show just 12,383 individual people were subject to Justice Social Work reports in the same year. This leaves 18,961 people who were sentenced without a social work report (or, potentially, relying on an older social work report), and about whom no data is available in relation to their drug use. Moreover, 2020/21 is an anomalous year in the data as the LS/CMI IT system was offline from March 2022 to August 2023, and assessments were done offline during that time period. It should be noted that in preceding years the gap between people convicted and people receiving social work reports is even larger.
In Figure 3 below, the blue line shows all people convicted, with the orange shaded area reflecting the proportion receiving a pre-sentencing social work assessment. It shows that between 2016/17 and 2019/20, around one third of people convicted have typically received a social work report before sentencing.
How is the Justice Social Work Report compiled?
If a report is requested, a Justice Social Worker will interview the person and review documented sources of information such as their file and Offender History Form. Guidance on conducting these interviews and writing justice social work reports (2023) suggests that where relevant 'the context of trauma in their life – including the presence and impact of mental health issues, substance misuse and any current treatment plan'.
During the interview, if the person discloses that they have a problem with any kind of substance use, the social worker will then seek more details about their usage, their perception of its relationship to their offending, and their interest in treatment or making change. These details will then be summarised in the report to the court, and will inform the social worker's recommended sentence.
- If the person does not disclose their drug use, the social worker will not be able to make the court aware of it. They cannot receive a sentence with specialised drug treatment.
- If the person does disclose that they use drugs (and/or have mental health difficulties), the social worker may request additional time from the court to do a full drug needs (and/or mental health needs) assessment.
- If the court agrees to this, the additional assessments take place and detailed information from them can be taken into account at sentencing, enabling the court to impose a sentence with specialised drug treatment, if they wish.
- If the court does not agree, the additional assessments do not take place, and at sentencing the court will be informed in the Justice Social Work Report of the person's disclosures, but no more detailed information will be available for the court to take into account. Without a detailed assessment, they cannot receive a sentence with specialised drug treatment.
The Practice Guidance for delivering DTTOs states that for the purposes of identifying people who may be suitable for a DTTO via the social work report process, the service should develop its own clear criteria for the target group, and ensure social workers have access to both consultation and line management input to assist assessment and decision-making.
Data on those who may have a drug problem
Background on data presented
The assessment and reporting structure uses an abbreviated form of the LSIR (Level of Service Inventory - Revised). LSIR is a validated and widely used assessment tool for understanding a person's context, offending and criminogenic needs (Raynor, 2007).
Data on the items in this tool are recorded in the LS/CMI database held by the Risk Management Authority. However, quantitative data relating specifically to drug use at this assessment stage is very limited. The social worker's report should draw the court's attention to any specific concerns in relation to drug or alcohol use, but this is generally recorded as part of a narrative about the person's circumstances and offending.
The only quantitative variables recorded in the LSCMI database for this stage of assessment are:
- Whether the person has any drug crimes in their offending history (i.e., convictions for offences such as dealing or possession)
- A variable called "alcohol or drug problem: school/work", which is selected if the person has disclosed that their relationship with alcohol or drugs is having a negative impact on their ability to maintain a healthy or functional relationship with their work or education.
These two variables are not ideal proxy measures for identifying people with drug dependency in the data set. This is because:
- The first variable relates to detected, proven offending history, not the person's relationship with substances.
- People may be charged with drug crimes regardless of whether they have a dependency or problematic relationship with drugs, while many people with drug problems may never be charged with drug crimes. This means this variable may capture some people whose relationship with drugs may not be problematic, while missing others. Consequently, it could be higher or lower than the "true" rate.
- Moreover, past offending may relate to a period of dependency that the person has now recovered from. This means this variable may capture some people who should no longer be classed as having a problem with drug dependency. Consequently, it could be higher than the "true" rate.
- The second variable conflates alcohol and drug-related problems.
- This means the number it captures will be higher than the number of people whose problems specifically relate to drugs, or to codependency on both drugs and alcohol.
- The second variable also limits substance-related problems to the person's relationship with work or education. While this item has been validated as a criminogenic factor for assessing risk of reoffending, it may exclude people whose substance use primarily impacts other domains such as their relationships or physical health. Consequently, it could be lower than the "true" rate.
Notwithstanding these limitations, as the best measures available, these variables are presented here to give some idea of the order of magnitude of people who may have a drug problem identified at this stage.
Numbers of those who may have drug problem
Between 2017 and 2021, 7,163 people met one or both of the criteria outlined above, and therefore may have a drug problem, this averages 1,433 per year.
For this group any information about their relationship with drugs that the social worker gathers in their initial interview is likely to be provided to the court in a narrative form as part of their social work report. This means that the court can take this information into account in their sentencing decision. However, no more detailed data is recorded in a format suitable for analysis at this stage. For the majority of this group, more detailed data about their drug-related problems is not available: 4,660 (65%) do not go on to receive a more detailed social work assessment. Typically, this will be because they receive a low-tariff disposal such as a fine or Level 1 CPO, which does not require supervision.
Outcomes for those who may have a drug problem
- Compared to the remainder of the population receiving initial assessments, between 2017 and 2021 people potentially likely to have drug related problems are:
- More likely to be identified as requiring supervision or intervention (83%, compared to 67% for those with no indication of a drug problem), but only slightly less likely to be identified as feasible for community disposal (94%, compared to 96% of those with no indication of a drug problem)
- Slightly more likely to be identified as being on a trajectory of worsening offending (47%, compared to 43% for those with no indication of a drug problem)
- Somewhat more likely to be identified as meriting fuller assessment (7%, compared to 5% for those with no indication of a drug problem)
Additionally, LS/CMI data suggest that people with drug related problems are more than twice as likely to be assessed as having motivation as a barrier – this is marked as a potential responsivity issue for 48% of people with drug related problems, compared to 23% without drug related problems. This pattern also holds for denial/minimisation, although the discrepancy is not as great – 55% of people with drug related problems have this recorded as a potential responsivity issue, compared to 46% of those without. Women with drug related problems are also more likely to have gender-specific responsivity issues noted than women without drug related problems (7% compared to 4%).
Step 2 – Additional Assessments
If the court agrees to delay sentencing for additional assessment[11], they can request either:
- A specialist medical report. This will enable the court to impose a Community Payback Order with a drug treatment requirement if they wish at sentencing.
- A full multi-disciplinary assessment. This will enable the court to impose a Community Payback Order with a drug treatment requirement or a Drug Treatment and Testing Order if they wish at sentencing.
However, such an assessment is not a requirement. - An assessment for a Structured Deferred Sentence (if available in the area)
The Practice Guidance for DTTO schemes recommends that to improve reliability, these assessments should be carried out in the community if at all possible, although decisions on bail and remand are matters for the court.
Step 3 – Justice Social Work recommendation
Once the assessment is complete the social worker will determine with health colleagues whether or not there are suitable services in the local area to meet the person's needs.
- If the person's needs are not severe enough to warrant treatment, the social worker will recommend the sentence that they feel would best address the person's other criminogenic needs and risks.
- If there are no suitable treatment services for the person, the social worker will provide all reports and information to the court, and recommend what they view as the most appropriate alternative sentence to the court.
- If there are suitable treatment services for the person, the social worker will develop a treatment plan or plans with health colleagues, and all the relevant documentation is shared with the court.
- i. If only a specialist medical report was requested, the recommended treatment plan will be general, and suitable for a CPO with a drug treatment requirement.
- ii. If a multi-disciplinary assessment was requested, the social worker may recommend a treatment plan suitable for either a CPO or DTTO depending on their professional assessment of what would best serve the person's needs. If recommending a DTTO they must also present a more detailed and complete treatment plan, and an alternative option that can be implemented as a CPO if the court is not minded to support the DTTO.
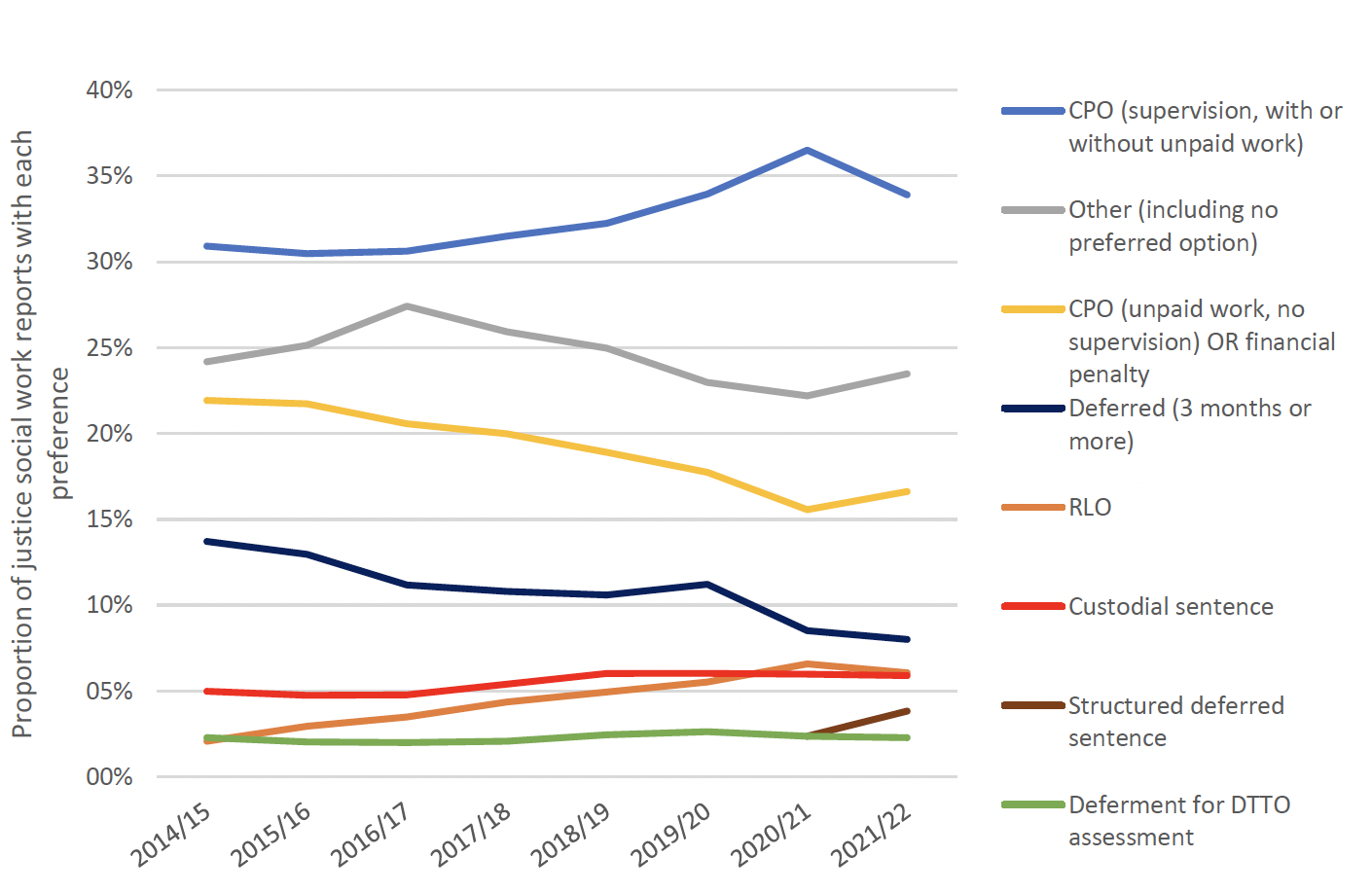
As noted above, data is not available on the specific population of people who have substance use problems in the justice system. However, the chart below summarises the data on options recommended to the courts following all social work reports:
Step 4 – Sentencing hearing
At the sentencing hearing, the court will apply the purposes of sentencing (see Scottish Sentencing Council's 'Principles and purposes of sentencing' guidelines) and proceed through the required steps to arrive at a decision. The steps involve:
- Assessing the seriousness of the offence, based on the person's culpability and the degree of harm caused
- Considering any aggravating and mitigating factors. Committing the offence under the influence of substances voluntarily consumed is a possible aggravating factor, while mental illness is a possible mitigating factor, as is demonstrating willingness to address drug problems.
- Considering the principles and purposes of sentencing, and how the different purposes should be weighted.
- Considering which sentence option will best serve the chosen purpose(s) while being fair and proportionate in light of all the facts and circumstances of the offence[12]
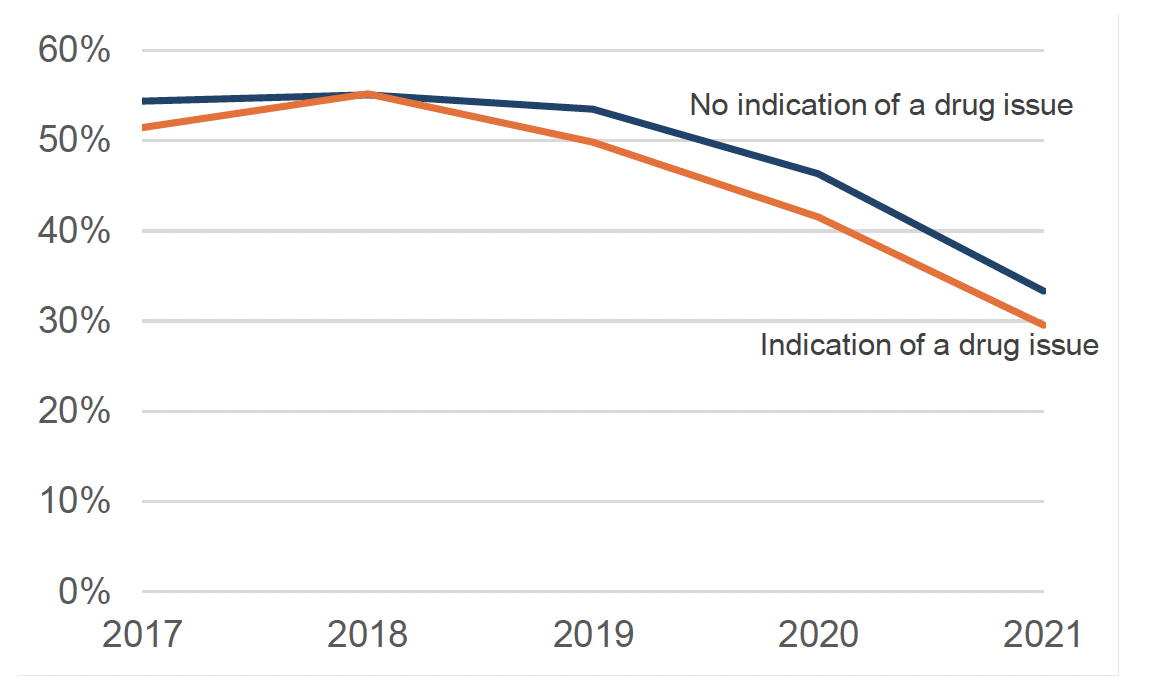
Compared to the remainder of the population receiving initial assessments, between 2017 and 2021 people potentially likely to have drug related problems are slightly less likely to receive the disposal that social work recommend to the court (47%, compared to 50% for those with no indication of a drug problem). It is also notable that the disposals recommended by social work, and those imposed by the courts, appear to have diverged over time. The chart below shows the proportion of people receiving the recommended disposal for both people with and without indications of potential drug related problems:
Disposals for those who may have a drug problem
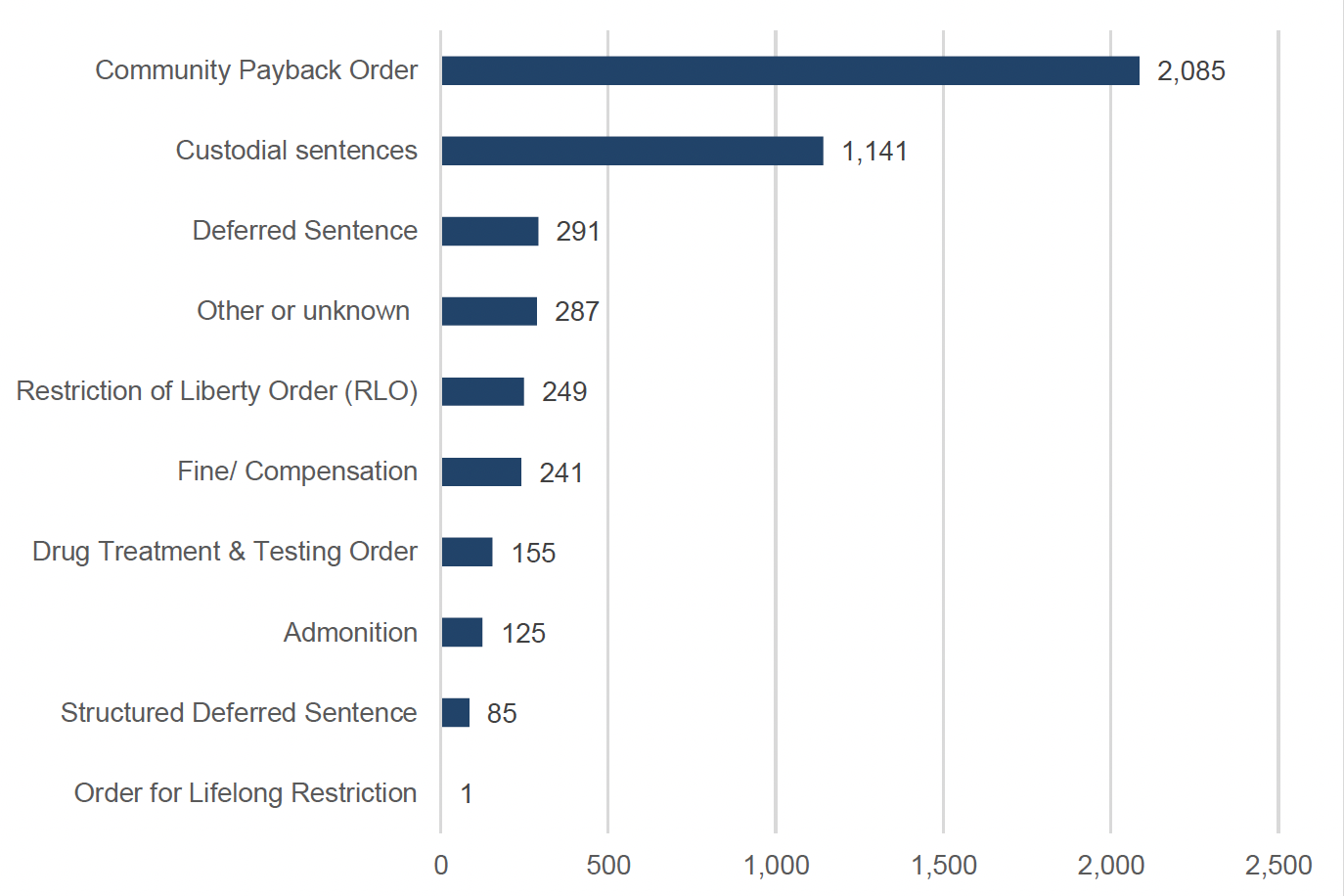
For this group (whose initial assessment shows they may potentially be likely to have drug related problems, but who do not have a more detailed social work assessment recorded), the most common disposal is a CPO, followed by custody. It is notable that a proportion of DTTOs also fall into this category each year, and the reasons that someone may be recorded as receiving a DTTO but not have a more detailed assessment recorded in the LS/CMI database may warrant further exploration with stakeholders. The full distribution of disposals for this group is shown in Figure 6 below.
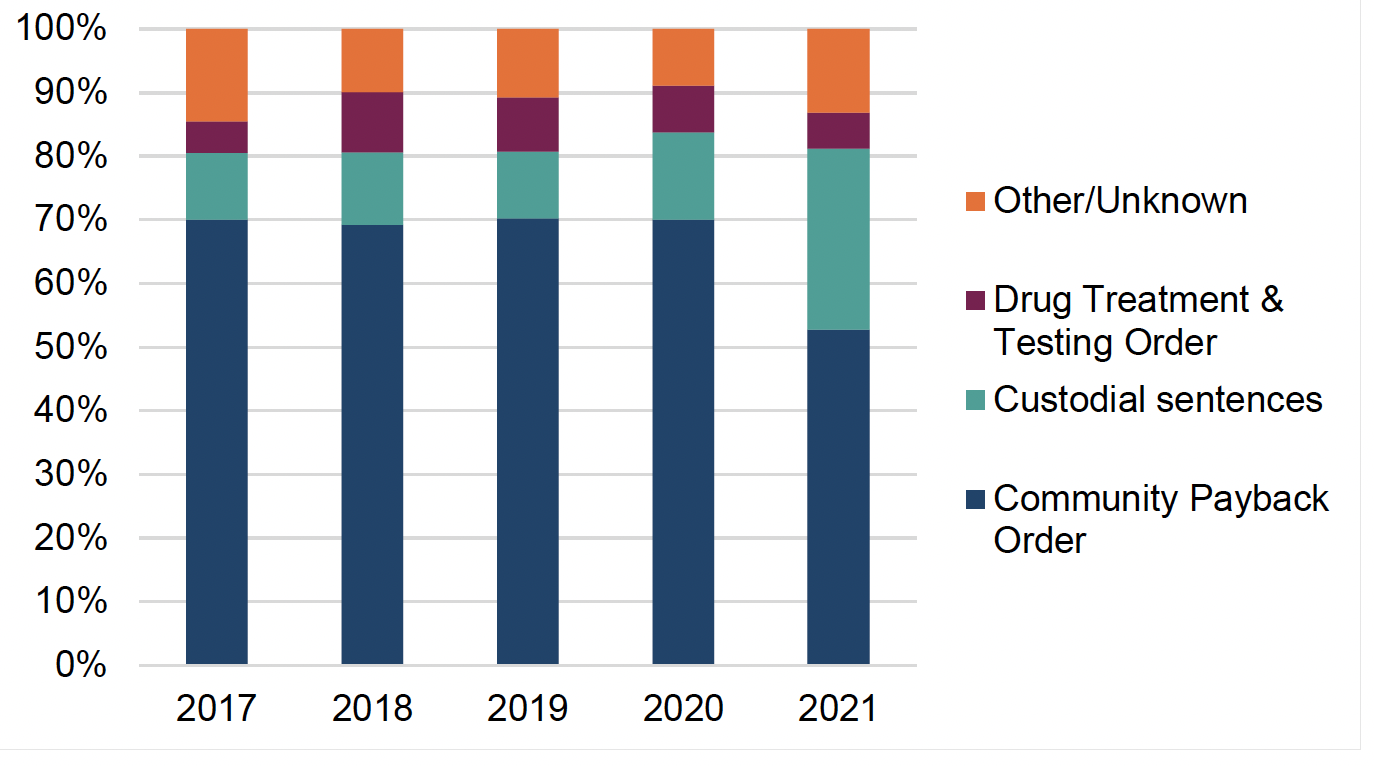
Between 2017 and 2021, the most common outcome for people who may have a drug problem has been Community Payback Order (68%), followed by custody (13%) then Drug Treatment & Testing Order (8%). However, as Figure 7 below shows, there has been a shift away from CPOs in favour of custody for this group in 2021. The reasons for this cannot be easily inferred, but could possibly be related to prioritisation of the most serious cases during the Covid-19 pandemic.
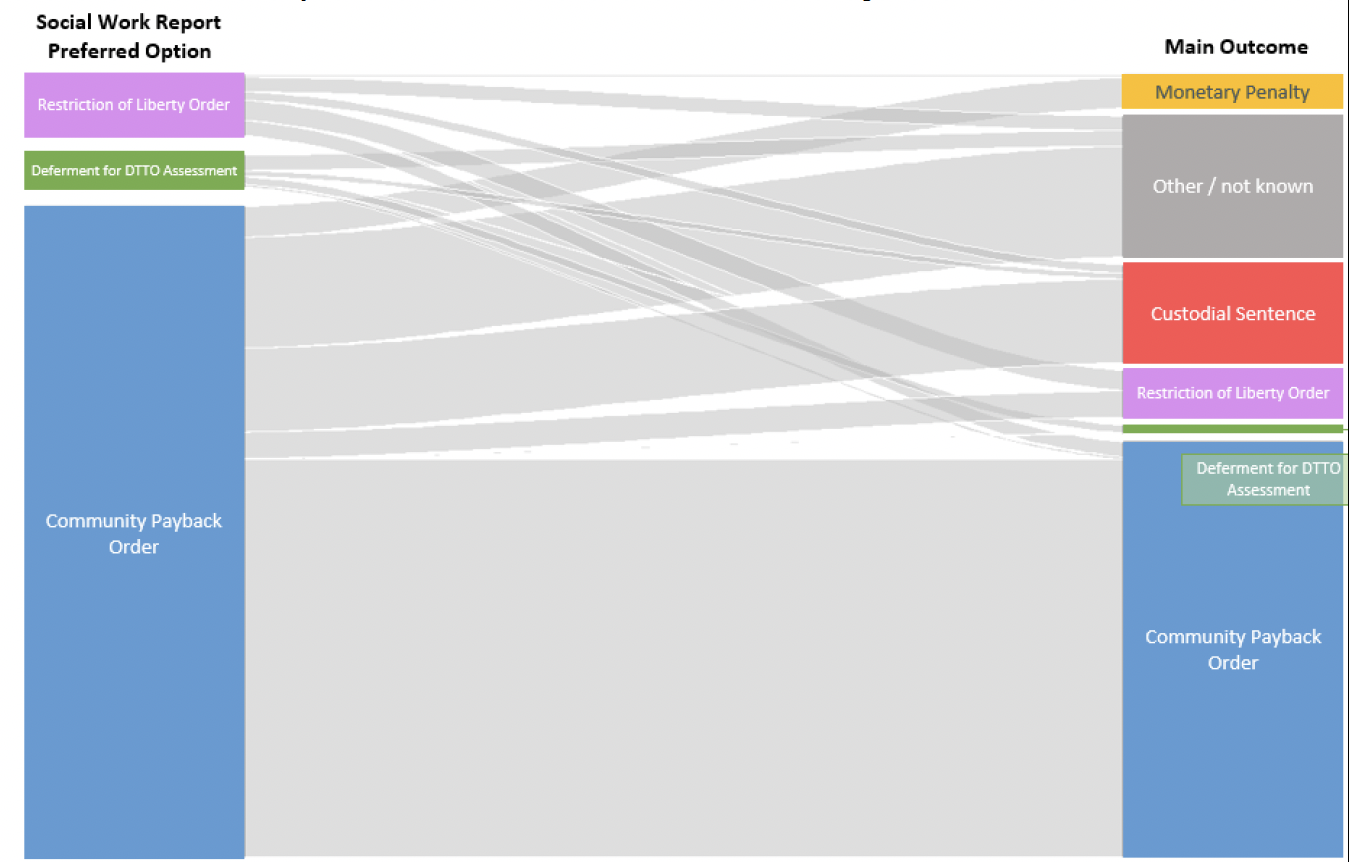
Preferred option vs main outcome
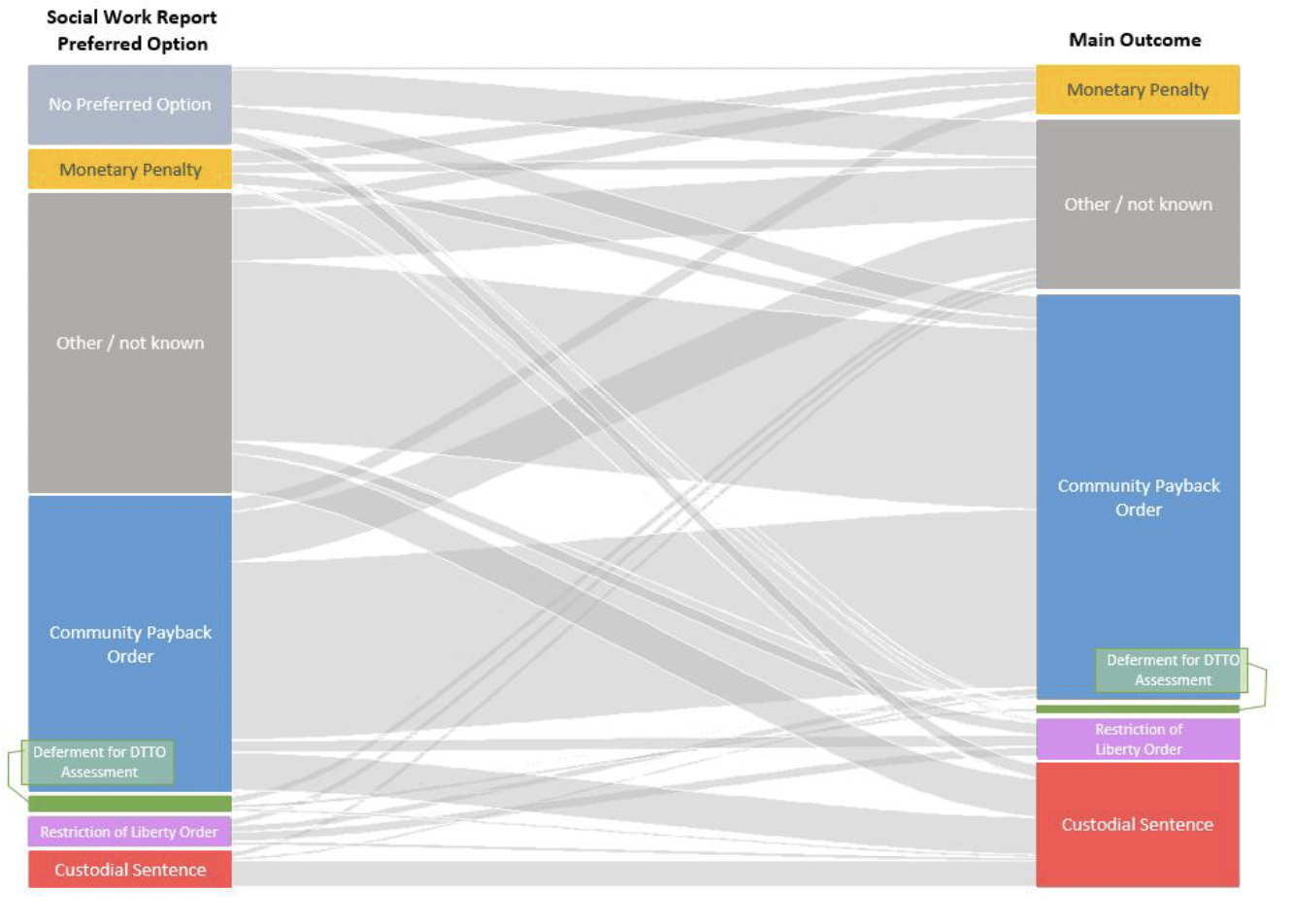
The data on social work reports' "preferred option" and the "main outcome" imposed by the court are imperfect measures for understanding the relationship between recommendations and judicial decision-making, but are all that is available to this review at this time. The chart below is based on all cases, not just those where the person may potentially have drug related problems and while challenging to interpret, shows the complexity of the pattern in the overall data as well as the significant number of cases in the "other" and "unknown" categories. To note, for both main outcome and preferred option, the 'other' category includes deferred sentences, structured deferred sentences as well as actual 'others'. In addition, for main outcome, admonition, warrant for apprehension/recall and absolute charge are also included. The chart also shows that where the outcome differs from the (known) recommendation, the biggest flow is made up of people whose social work report recommends a CPO, but who receive a custodial sentence instead.
If we limit the analysis to just those cases where the social work report's preferred option is known, and they have recommended an option that involves some form of supervision within the community, we see that where the preceding recommendation is known, almost all CPOs follow a recommendation for a CPO. Where the court decides not to follow the recommendation for a CPO, this is usually in favour of a higher tariff sentence – where the outcome is known, a significant proportion of cases ultimately resulted in custody or, less commonly, a Restriction of Liberty Order, while a much smaller proportion of CPO recommendations result in a monetary penalty:
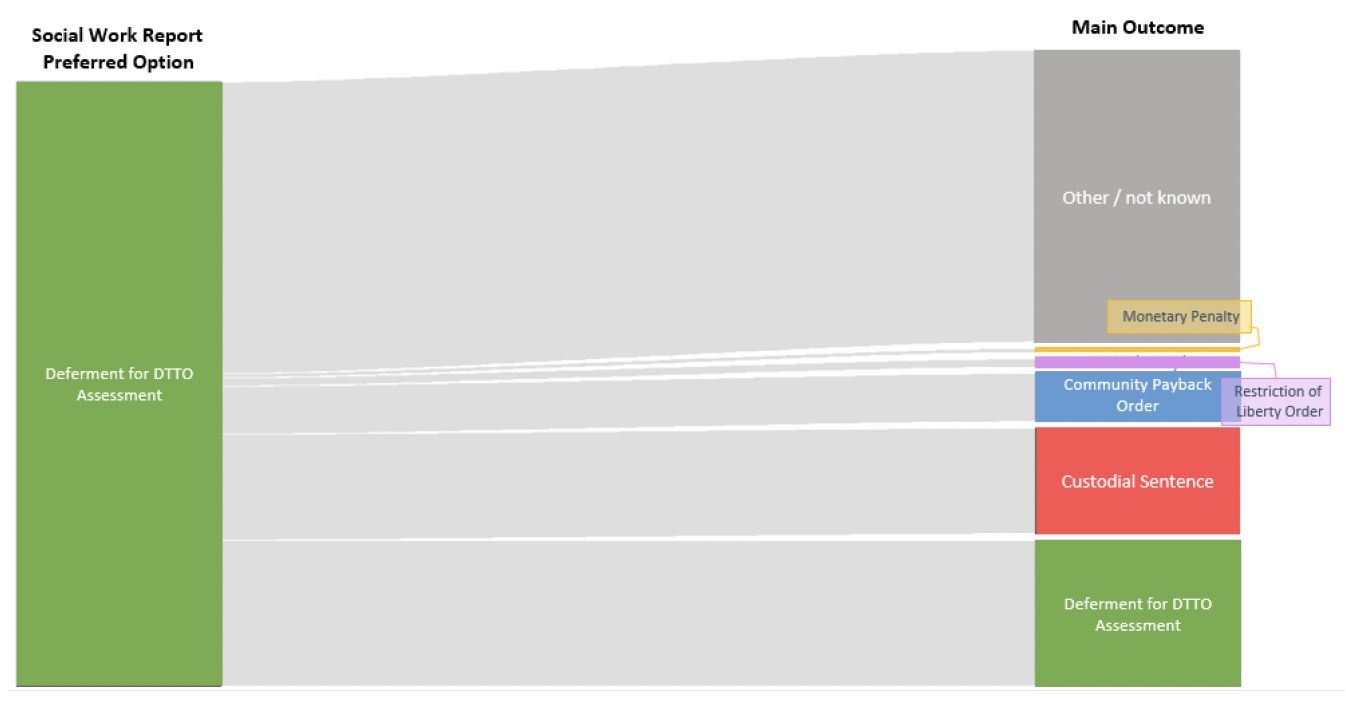
Zooming in even closer, to look specifically at those for whom a DTTO assessment is recommended, we see that there is a particularly high rate of "other" or "unknown" outcomes for cases with this recommendation. Where the outcome is available, less than half of social work reports recommending deferment for DTTO assessment have this as their outcome, and one third result in a custodial sentence.
Due to limitations in the data, we cannot look specifically at the outcomes of assessments for CPO drug treatment requirements, or which recommendations tend to lead to them being imposed. However, we can place the number of drug treatment requirements in the context of the total number of CPOs imposed – which shows that only a very small proportion of all CPOs have a treatment requirement, and their rate is consistently lower than that of DTTOs. Overall, CPO alcohol requirements constitute just over one percent of all CPOs issued in 2021-22, and drug treatment requirements just under one per cent.
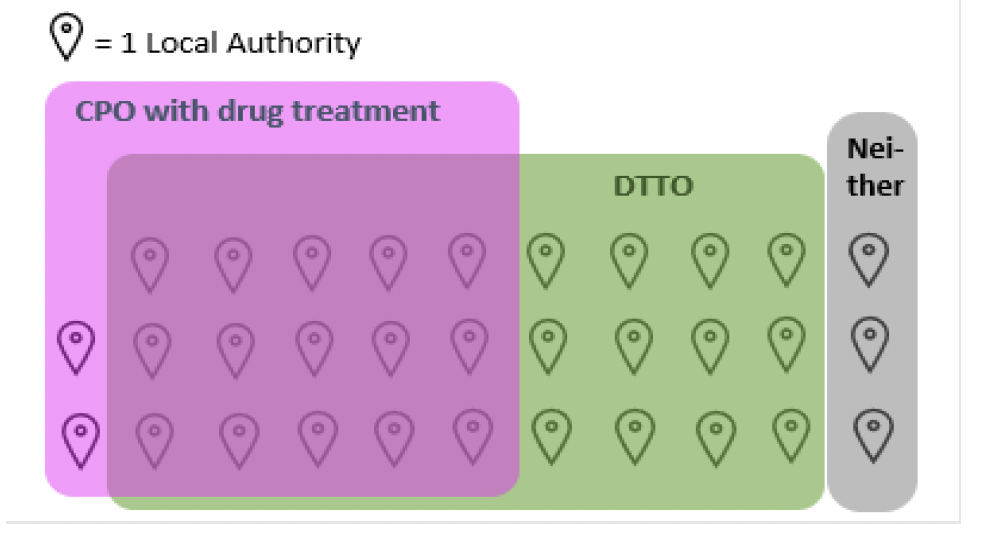
Looking across the regions, it is also clear that there is some variability in the rates with which different types of order are made, although it is impossible to tell from the data how much this is caused by local variation in offending and substance use patterns, and how much may be attributable to differences in local service provision, professional practice or sentencing preferences. In 2021/22,17 (out of 32) local authorities delivered at least 1 CPO with a treatment requirement, with 110 imposed in total. By contrast, 27 local authorities delivered at least one DTTO, with a total of 361 imposed.
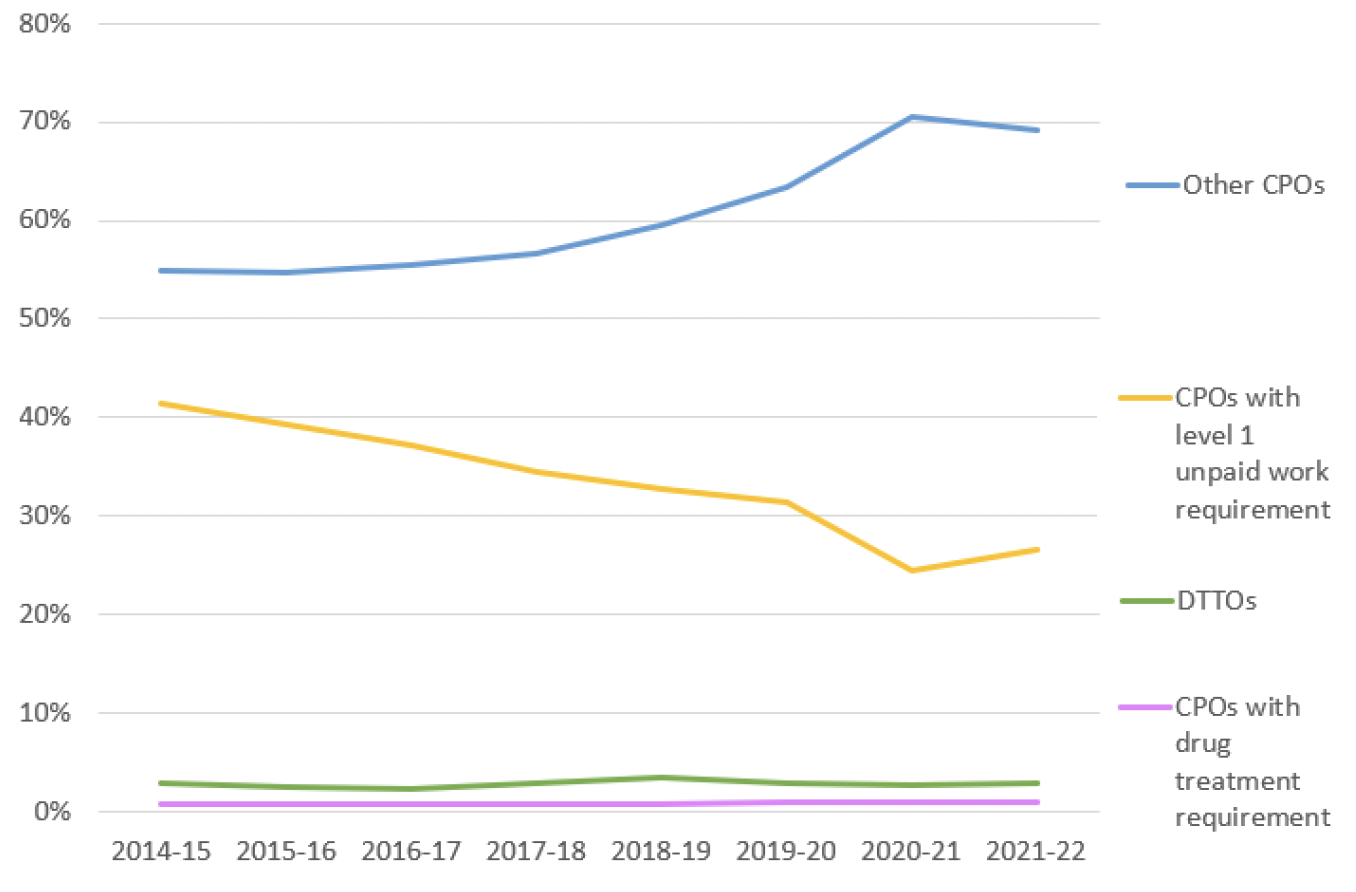
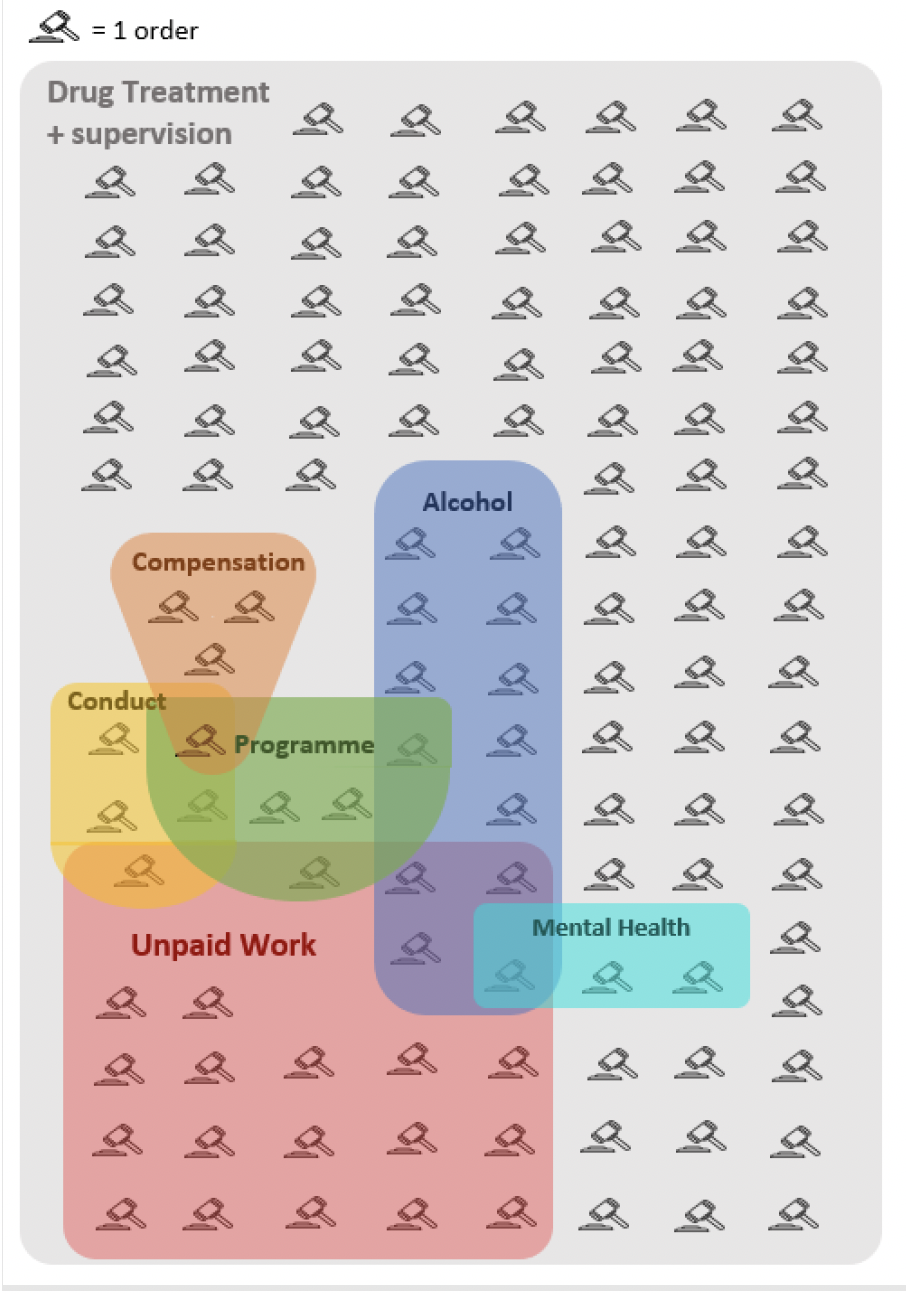
All Community Payback Orders must have either unpaid work or supervision. Apart from a small reversal due to the effects of the pandemic, recent years have seen a general trend towards increasing use of supervision and reducing use of unpaid work. Apart from these core requirements, the most common additional requirements for all CPOs are Conduct or Programme.
In 2021/22, 125 CPOs contained a drug treatment requirement. All those who receive a drug treatment requirement will also have supervision. Over half of all 125 drug treatment requirements in 2021/22 were made without any additional requirements being imposed. A further 34 had one additional requirement, most commonly unpaid work, followed by alcohol treatment. The distribution of all requirements added to CPOs with a drug treatment requirement is shown in the figure below.
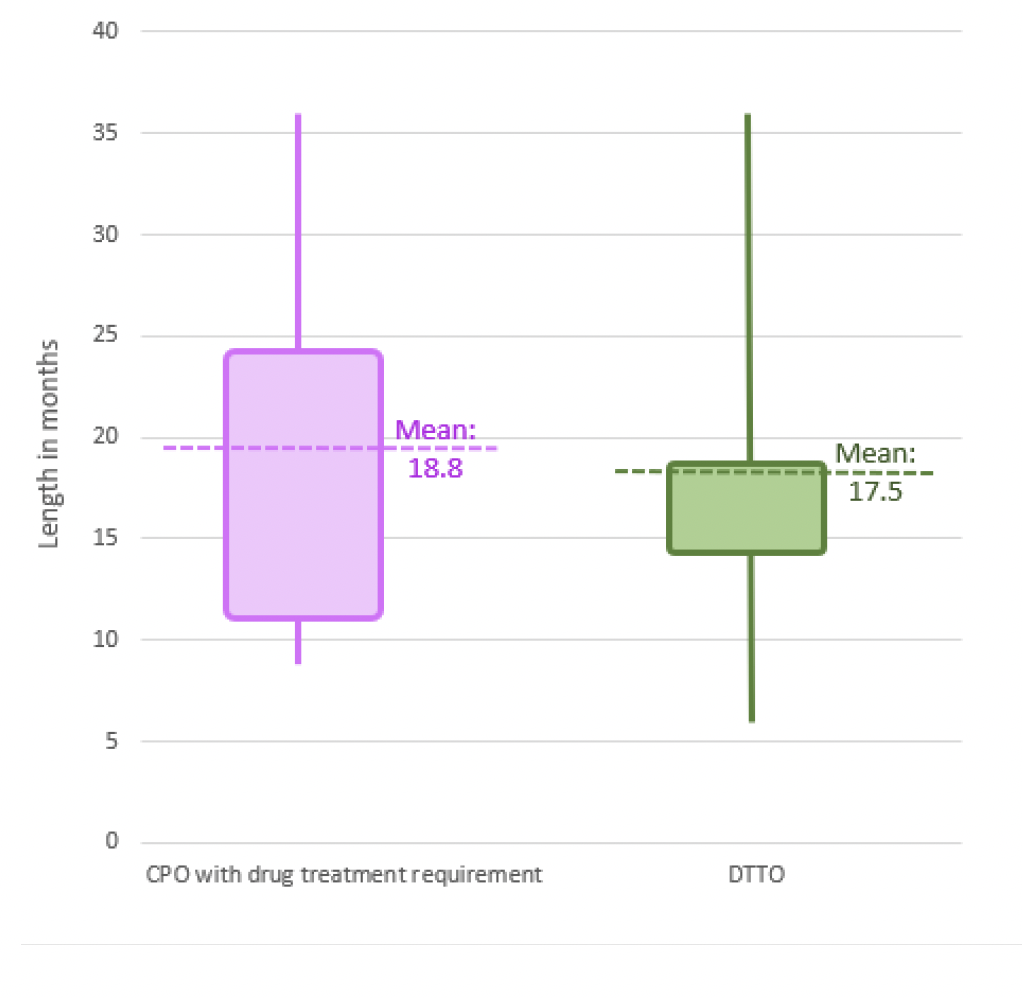
In terms of order length, both CPOs with treatment requirements and DTTOs tend to be imposed for similar lengths of time – the average is 18.8 months for CPOs with drug treatment requirements, and 17.5 months for DTTOs. DTTOs show a slightly wider range in lengths, but also a notably greater tendency to cluster near the mean, while CPOs are more distributed across their range of lengths.
Step 5 – Structured Deferred Sentences
If the court is unsure whether the person is likely to comply with a community based order, or with treatment specifically, in some areas it is possible to defer the sentencing decision in order to allow the person to engage with a Structured Deferred Sentence (SDS). This means that instead of giving a sentence, the court orders the person to engage with justice social work support for a specific period of time before returning to court for sentencing. During that time, their ability to comply and engage will be assessed. When the person returns to court, the same options are available to the court as at the time of conviction, but they have additional information on which to base their decision.
- In some specific schemes like the Aberdeen Problem Solving Approach, the SDS can be used to support people into treatment and then, if the court is satisfied with their progress, avoid the harms of high tariff criminalisation by admonishing the person instead of imposing a more intensive disposal.
- In other areas, SDS might be used to support the person into treatment and assess their ability to engage and comply. If the court is satisfied with their progress, this may make them willing to impose a treatment based community order instead of a prison sentence, or a less stringent community order than they would otherwise have given.
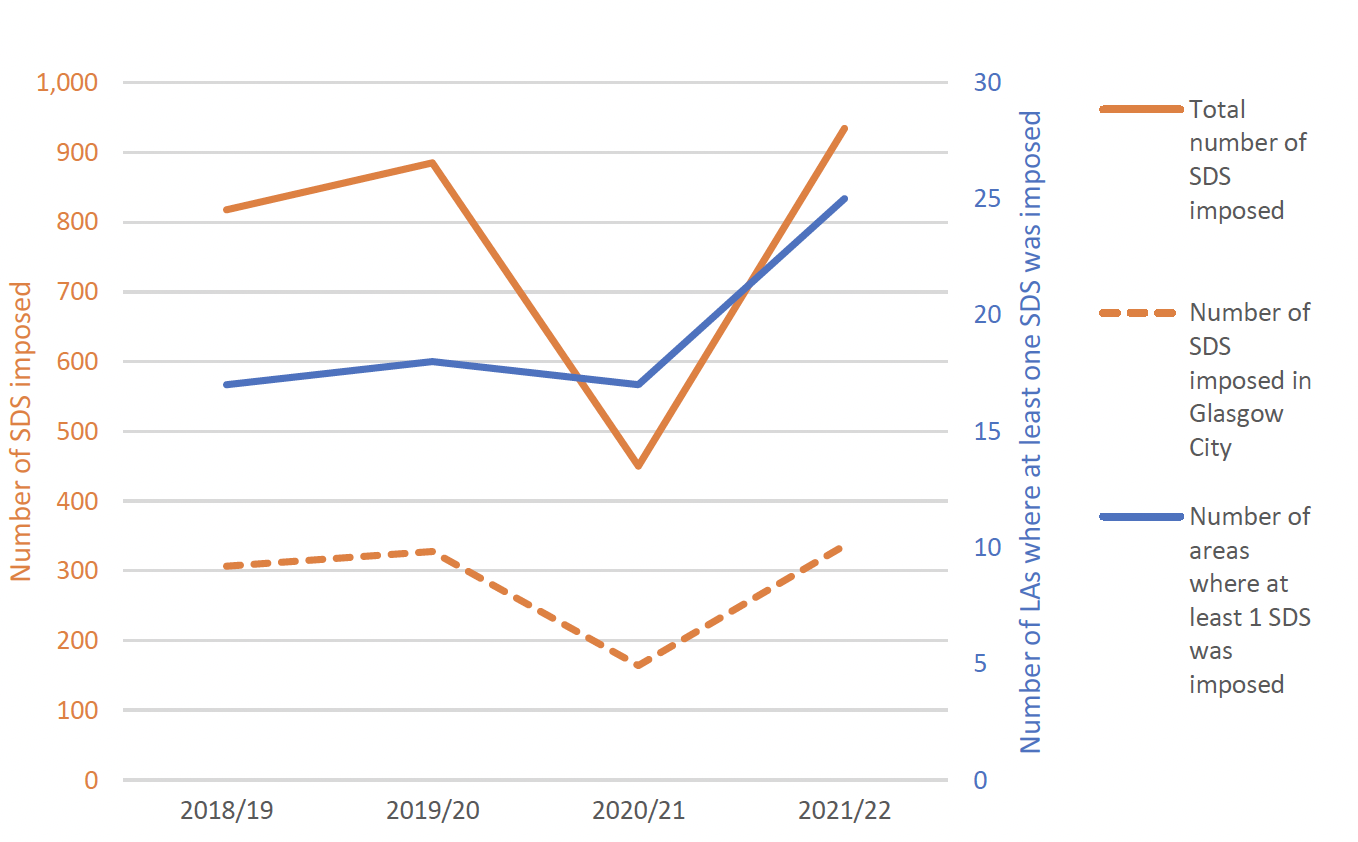
In 2021/22, the highest number of SDSs to date was recorded, with 934 SDSs imposed, and 882 individual people receiving at least one SDS. 2021/22 also saw the highest number of areas offering SDSs, with 25 areas providing at least one SDS in 2021/22, compared to 17 in the first year of data. Glasgow City consistently provides the highest number of SDSs, and accounts for over one third of all SDSs in all years.
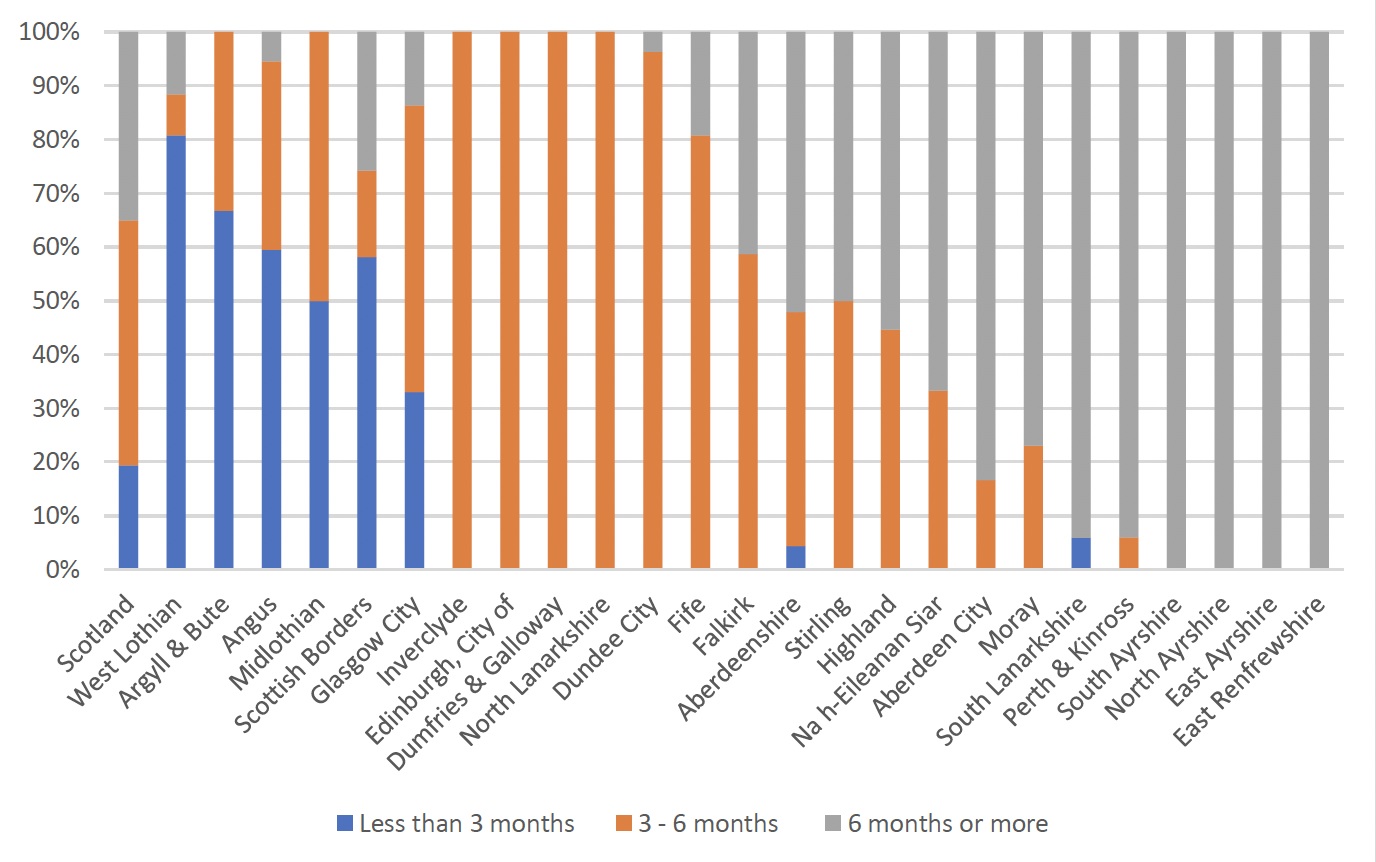
In 2021/22, just under half of all SDSs were for between 3 and 6 months. Both the typical length, and the variability of length, varies significantly between areas.
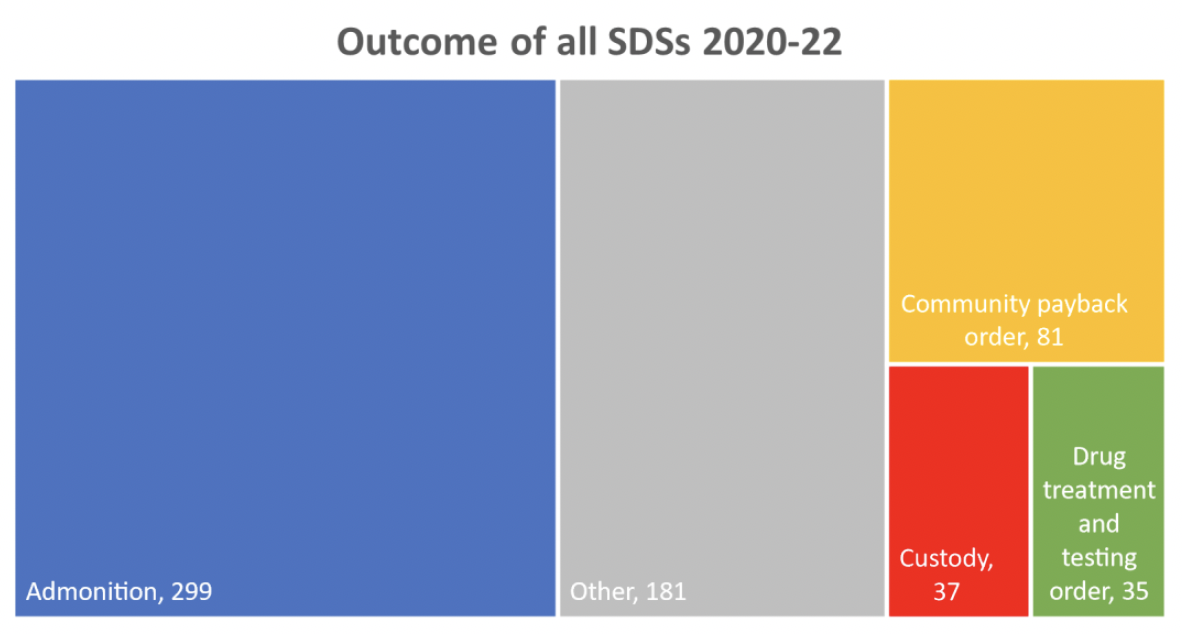
Following a Structured Deferred Sentence, when the person returns to court for sentencing, the most common outcome in 2020/21 and 2021/22 was for the person to be admonished – this happened in around 50% of all SDSs. Again, the main outcome, and variability in outcomes, vary significantly across areas – which is to be expected, since SDS schemes may operate in different ways, and with different purposes, depending on local need and resource.
Step 6 – Delivery of the order
Once the order has been imposed:
- If the court imposes a Drug Treatment and Testing Order, the person will begin working with their justice social worker and treatment provider(s) in line with the treatment plan presented to the court.
- If the court imposes a Community Payback Order with a drug treatment requirement, the person will continue working with their social worker on their full needs assessment and treatment plan, then once this is complete they will begin working with treatment providers (or their social worker if appropriately trained), in line with the agreed plan.
- If the court imposes a supervised Community Payback Order with no drug treatment requirement, the person will begin working with their justice social worker to complete the order, and as part of this work their social worker may use their supervision appointments to deliver some drug-related interventions (if they are appropriately trained to do so), or encourage them to access third sector support.
- If the court imposes a custodial sentence, the person will enter custody and their health and treatment needs will fall under the prisoner healthcare system.
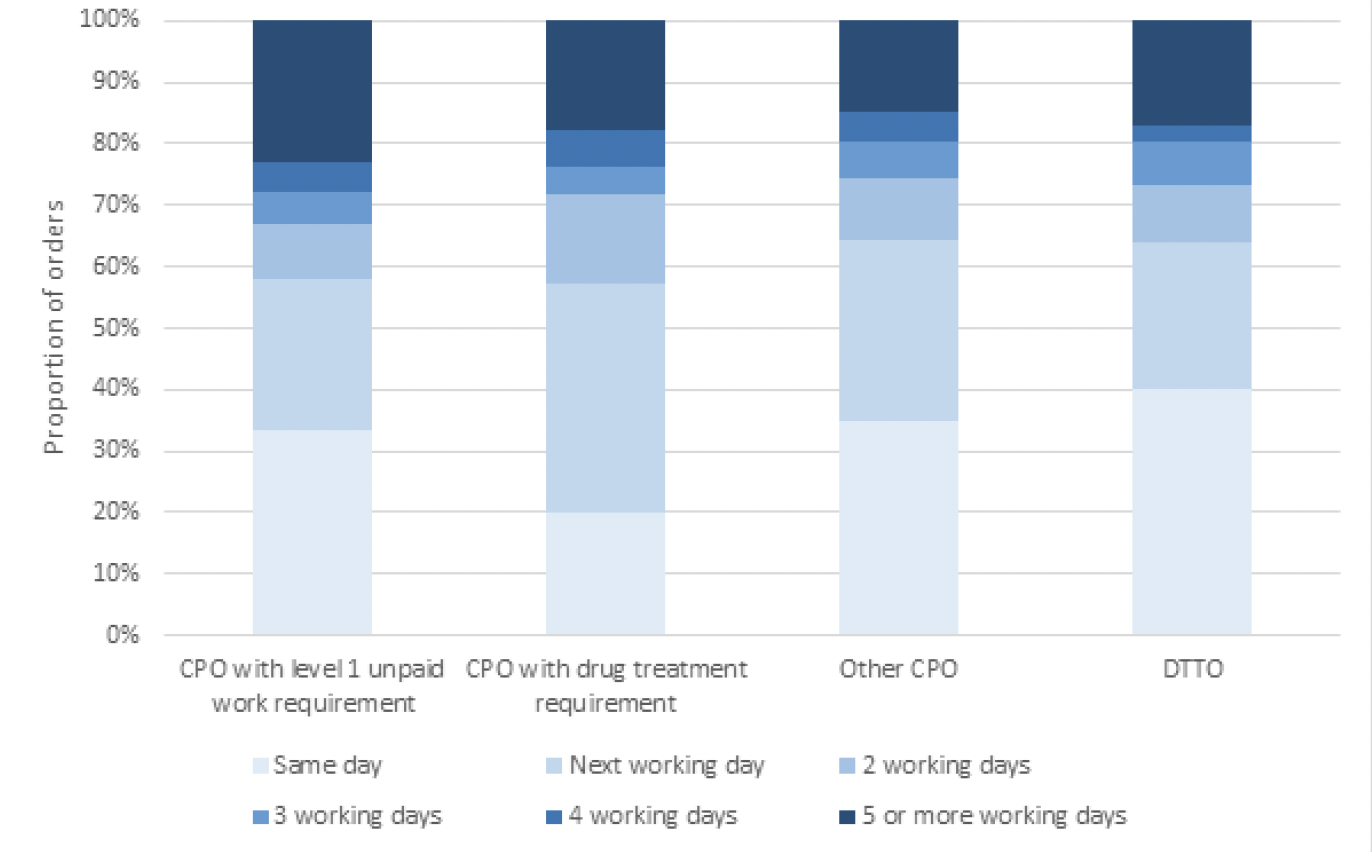
The chart below shows the length of time taken between an order's imposition and the person's first contact with justice social work. Level 1 unpaid work requirements have the longest waiting time, at 7.2 working days. Other CPOs, with or without treatment requirement, average 3.9 days, and DTTOs average 2.7 days.
7. Assessment of practice against the evidence base: conclusions and areas for exploration in relation to eligibility, targeting and assessment
Overall, the process established by legislation and practice guidance is complex, containing multiple pathways and many key decision or transition points – each of which reflects a potential opportunity for someone with substance related problems who needs treatment to "fall off" of the pathways to a treatment-based community order. That is not to say that these are problematic process steps that should necessarily be considered "holes" in the system – there are many factors that need to be balanced in each decision, and not every person with substance related problems would benefit from a treatment based community order, so these opportunities to exit the pathway to one may be entirely appropriate. What is important is that, at each point, the best decisions possible should be made in order to offer and retain those who would benefit on a treatment based pathway, and channel those who would not, to other pathways without up-tariffing them.
Eligibility and targeting
Overall, it is clear that the sentencing system does include options which can keep people out of prison – however, without detailed data on the people passing through the courts, it is difficult to say what impact these options have on outcomes. One area which may benefit from further exploration is the apparently high number of people in prison who have substance use problems, and the relatively low number of people who receive DTTOs or CPOs with a treatment requirement. The data demonstrates a mismatch between the proportion of people recommended for community based sentences, but receiving a custodial sentence instead. This would seem to indicate that social workers generally assess more people as appropriate for community based rehabilitation (based on the person's risks and needs) than the judiciary considers appropriate for sentencing that way (based on applying the purposes of sentencing to the specific facts of the case). However, without further details regarding the nature of the index offences or the person's criminal history it is not possible to draw any firm conclusions, but further research in this area may be merited.
Assessment
The community sentencing process in Scotland is largely based on individualised assessment, uses a well-validated tool (the LSIR or LS/CMI) to assess Risk, Need and Responsivity (RNR), and aims to tailor the sentence and interventions a person receives based on RNR principles – all of which are generally supported by the evidence. The most common community order, the CPO, can be tailored by the court in terms of length, intensity, requirements and activities, and frequency of review. The treatment offered in a DTTO or CPO drug treatment requirement is also based on the individual's assessed needs, but the fidelity between needs and treatment received may be higher in CPOs with treatment requirements than DTTOs, because the treatment details are not specified by the court. The advent of Structured Deferred Sentences provides an additional opportunity for even more detailed individual assessment and tailoring, although these are still used infrequently and in variable ways.
However, while this general approach is consistent with the evidence, there remain questions about whether this approach is implemented in optimal ways. For example:
- Timing and coverage of assessment: Some people who would benefit from receiving an assessment may not be assessed. This is most likely to happen if their offending is relatively low level, or they have been to custody before – meaning opportunities may be missed to engage people in treatment earlier in their offending careers, or to engage some people who have been harmed by prison sentences already instead of returning them to custody. Whether there may be opportunities for earlier assessment or triaging of cases is a question worthy of exploration with stakeholders.
- Criteria for orders: Although the legislative criteria for substance dependency are the same, it is justice social workers who assess people's risk and needs, and make recommendations to the court about the most appropriate sentence. Taking a more detailed look at the practice guidance for each order, there are some potential tensions that may be difficult for social workers to negotiate. For DTTOs, social workers are advised to prioritise those with high-risk use patterns, such as poly drug use (especially in "chaotic circumstances"), injecting, high frequency, worsening chronic long term use, and the most harmful substances such as opioids, benzodiazepines, cocaine and crack (DTTO Guidance for Schemes, 2011). However, they are also advised that CPOs may be more suitable for people if complex social circumstances might impede their focus on treatment, there are additional issues related to the offending that would not be addressed, or the person requires medium to long term residential treatment. One possible reason for the low rates of DTTO usage, is that it is unlikely that there will be many, if any, people whose substance use is sufficiently problematic to make them eligible for a DTTO, who don't also have the kind of co-occuring problems that then exclude them. This may be a significant factor in the low numbers of DTTOs issued – there are simply not many people with the relevant needs profile of very high substance use and offending behaviour, but no other issues that may interfere with treatment or need to be addressed to reduce their risk of reoffending.
- Assessment tools: while the LSIR and LS/CMI are well validated and widely used tools, they are not specialised for exploring substance use. As noted earlier, the two main items of relevance are simply binary variables about whether the person has a substance use problem currently, or has had one ever. Beyond this, the discussion will be driven primarily by the Justice Social Worker's professional training, along with any specific local guidance or supplementary assessment tools. There are benefits to the flexibility and rapport-building of unstructured discussion, but also potential risks in practice variability causing some people to be missed. Whether the appropriate balance is currently struck in this area should be explored with stakeholders.
- Resources and time required: It is not possible to tell from the available data what impact (if any) is caused by the different levels of assessment required for each order, but there are obvious considerations in relation to: court resource involved, acceptability of delayed justice outcomes, social work capacity/case-loads and health colleagues' availability to contribute to assessment.. How these factors are balanced against one another, and against the value courts place on detailed information, warrants further exploration with stakeholders.
DTTOs and CPOs vary in the extent to which they might be considered to take a realistic approach to recovery that recognises goals other than abstinence and accommodates the need to build the person's motivation and readiness to change. CPOs with a treatment requirement generally provide more flexibility for these factors, as the order only requires the person engage with treatment. This leaves more room for the person and their treatment provider to develop goals and tasks together, potentially incorporating harm reduction as appropriate, or changing approach as the person's needs change. However, DTTOs include the specific treatment activities and testing frequency that must be adhered to. This means a gradualist approach is harder to take; the goal of treatment is often set (or at least strongly implied) by the court's expectations about testing results, and treatment is less flexible in terms of providing harm reduction alongside other treatments, or adapting to the person's changing needs. This is understandable if one takes the perspective that the increased monitoring is necessary in order for the court to be comfortable keeping people with higher reoffending risk levels in the community instead of custody. However, it is less aligned with the perspective that people with the highest risks and needs are also those who may be slowest to make progress, and require the most flexibility and accommodation in order to remain engaged in treatment. The way both orders and expectations are calibrated for different target groups may therefore also warrant further exploration with stakeholders.
The complex geographical arrangements in the court, community justice, and health systems may mean that in cases where a person is convicted in an area other than where they live, the court may have less information about, understanding of, experience with, or trust in, the community services they can receive. While the court can still request a report from the justice social work department in the person's local area, this reduced familiarity may have an impact on the decision to request an assessment, and about what sentence is believed will best serve the intended purpose.
8. Delivering orders and treatment
Overall, both treatment based orders provide a similar framework, based on accessing treatment relevant to the person's assessed substance-related needs, while keeping them in the community. However, DTTOs may be seen as offering less flexibility in how they are delivered. This is for because:
- The treatment details are specified in the order, making it more difficult to respond flexibly if the person's circumstances or needs change over time.
Although the treatment provided is needs based, the order itself is only focussed on substance use. Whilst this limitation exists in legislation, we are aware that social work practice has evolved over the years, and many areas undertake a holistic approach, working with the person on addressing other criminogenic needs. It should be noted that it may however be desirable to exclude these areas of the person's life from their order, because enforcement action or judicial scrutiny linked to their progress can arguably be a means of de facto criminalisation of need.
On the other hand, a CPO with a drug treatment requirement may offer less formal scrutiny of the person's progress in drug treatment (because tests are not reported to the court, and court reviews are less common). The supervising officer's role and scrutiny applied should however be noted here. CPOs can also involve support and more scrutiny of progress in other domains of life. Depending on the person and their circumstances, and the court's and social worker's expectations, this could either be an enabling factor or a barrier to successful completion of the order. As noted above, such scrutiny and enforcement may have the unintended consequence of de facto criminalising need, but on the other hand it may also be a necessary level of control to hand the courts in order for them to be willing to keep the person out of custody. This dynamic, and the legislative framework in relation to the social work's role in supporting people on DTTOs, may therefore warrant further exploration.
While DTTOs may offer less flexibility in the delivery and management of individual cases, Justice Social Work departments and Alcohol and Drug Partnerships have a wide degree of flexibility in terms of how they structure and deliver services for their local area, which is described in the following section on service structures.
9. Service Structures
Because community orders are delivered by each area's justice social work department (and health services or local ADPs), service provision, structure and approach vary across the country and there is no standard model. Orders are delivered within a complex organisational landscape. Additionally, provision can change depending on local resourcing, policy and sentencing practice. Notwithstanding this, recent work by Social Work Scotland (McPartland, 2022), and triangulated by additional information gathering carried out by Scottish Government and Health Improvement Scotland in 2023, provide an indicative snapshot.
Across these three surveys of local areas, only one area was not represented in at least one of the samples. Combined, the samples indicate that the majority of areas provide DTTO services, however:
- A number of areas report being unable to take on new cases, or being able to take on only a tightly capped number.
- Some areas reported that people on existing DTTOs were receiving only a partial service.
- Some areas reported no current DTTOs, but the ability to deliver them if required.
- One area reported currently offering a service, but that it was "not sustainable".
- One reported not offering a service because of lack of local demand.
- One area had been forced to suspend its provision due to prolonged staffing shortages, preventing new DTTO orders from being made in their own area and neighbouring areas where they also provide delivery.
Both service and funding structures appear to vary significantly between areas, and some areas reported being in the process of either reviewing their model, or rolling out changes. The below is based on the snapshot in the data available, and is not necessarily an exhaustive list.
The following approaches appear to be used to fund DTTO delivery:
- Justice social work s27 ring-fenced funding is used to employ non-clinical staff who provide social work and wrap-around support, while the NHS employ clinical staff who are co-located and work together to assess and deliver cases.
- Justice social work service s27 ring-fenced funding may be used to employ non-clinical staff, and also to buy in or second clinical staff from the local NHS service, who work in a multi-disciplinary team to deliver cases.
- Formal working partnership between a separate justice social work team and local Drug and Alcohol services.
- Justice social work s27 ring-fenced funding is supplemented by local ADP funding, in order to employ additional staff, to make it possible to provide a service for people in remote and rural areas.
- No official model or formal working arrangements, due to DTTO not having been ordered in a number of years.
The following observations can be made about variations in service structure:
- Most Justice Social Work services are within a local Health and Social Care Partnership, but not all.
- Most Justice Social Work services partner with local NHS drug dependency services to provide treatment for people on DTTOs, however some others may:
- Employ their own clinical staff in order to provide a more bespoke and intensive intervention than the local NHS can provide
- Partner with other, third sector organisations to provide treatment
- Partner with a different local area's service to access treatment
- Some Justice Social Work services facilitate fast-track access to drug treatment and/or mental health services including residential rehab, but people in other areas will access services at whatever the mainstream wait time is locally.
- Some Justice Social Work services facilitate access to, or directly provide, various additional services or groups not offered to the mainstream population in NHS drug treatment. Examples include acupuncture, dental, groupwork programmes, overdose prevention interventions, peer support, and blood borne virus clinics. Other services only facilitate and supervise access to mainstream NHS services.
- Most Justice Social Work services reported positive relationships with their partners for treatment provision, although some reported that communication, limited resources and personnel could be problematic. Most, but not all, have transitional or follow up support to improve transfer into mainstream services.
- Some Justice Social Work services have dedicated DTTO staff, while in other areas DTTOs fall in the general caseload of criminal justice social workers.
- Some services utilise only mainstream services that would be available to any person presenting for treatment, regardless of their involvement in the justice system, while others provide a dedicated or additional service specifically for people on DTTOs.
- In addition to justice social workers, a range of different staff roles and titles may be employed in the service, including support workers, community justice assistants, drugs workers, resource workers, doctors, nurses, specialist drug treatment nurses, nursing assistants, medical officers, and admin assistants.
- Some areas co-locate clinical and non-clinical staff.
- Some areas have collaborative arrangements in which one area provides DTTO services for neighbouring areas. This can mean that, if an area providing services to other areas experiences difficulty in resourcing or otherwise delivering DTTOs, the result can be their suspension in multiple areas at once.
The following issues and challenges have been noted by services:
- Small and highly variable numbers make it hard to plan and resource services appropriately.
- Inadequate funding for both social work and clinical services, and funding not keeping pace with rising costs.
- Increasing complexity of cases over recent years makes each one more time consuming for staff to deliver, reducing capacity and contributing to staff burnout.
- Lack of staff, especially specialist staff, and lack of access to psychiatry and psychology.
- Lack of the full range of NHS services they would hope for clients to access, particularly psychosocial interventions.
- DTTO Guidance, and the service model it implies, are outdated in relation to current practice, and that it requires revision, particularly in light of changes in both community justice and substance use trends since it was published.
- The benefits of a dedicated, bespoke service can be undercut if transition into mainstream services on completion of the order does not have a clear pathway and strong communication.
- There is no standard set of outcomes that services all measure, and a range of different health board and social work systems are being used to record activity. Most services report partially meeting their identified outcomes.
Some local case studies can also be highlighted as demonstrating specific challenges, and potential innovations or solutions being tested in local areas. These are from Community Justice Scotland's 2021/22 summary of CPOs, except where otherwise stated. Because many of these relate to areas of active development work, the facts below may now be out of date, but nonetheless may be worthy of further exploration:
- One area appointed an 18-month post, shared between Justice Social Work and the Alcohol and Drug Partnership, to develop a "shared care" model between substance use services and JSW. At the time of reporting, they stated that mental health services continued to be hard to access, but learning was being shared through the local Forensic Pathways Review Group, and staff training was being sought.
- One area identified a disconnect between Sheriffs' understanding of local treatment orders, and what was actually being delivered – specifically, that Sheriff's believed that by imposing a drug or alcohol treatment requirement, they were enabling the person to access additional support they otherwise would not have access to, but in fact the services accessed to deliver these requirements are the same as those available to the general public. Whether such misunderstandings exist in other areas too, and whether it can be addressed through improved communication channels or additional training, may be a question that warrants further exploration.
- The same area detailed that substance use assessment is not carried out until an order had been imposed and the referral then made, which has been problematic in cases where the court imposes a treatment requirement on someone who, upon detailed assessment, does not meet the usual thresholds for accessing these mainstream treatment services. This issue, compounded by communication challenges between social work and the treatment service, can result in people being provided with inadequate or suboptimal treatment and support. At the time of reporting, a proposal had been put forward to recruit two specialist workers to be based within the mainstream treatment service, but work specifically with people subject to drug and alcohol treatment requirements.
- The Care Inspectorate (2021) report that in some local areas, specific case manager or social work assistant roles have been created to provide additional support to people with Level 1 unpaid work requirements. These orders do not include supervision, and so the people on them do not typically receive support to address criminogenic needs. However, the roles mentioned above have provided capacity to offer such support, without the strict enforcement of engagement, and has helped to increase engagement particularly for people with complex needs. The Inspectorate report that "This helped to reduce the need for community payback orders to be returned to court due to non-compliance. People welcomed these additional arrangements and made effective use of the supports available to attend appointments, address housing and benefits issues and improve their general life circumstances and sense of wellbeing". This type of arrangement may be one worth exploring, as a model for providing support to address wider needs, without making progress on them enforceable, and thereby criminalising need.
10. Addressing drug use
Treatment services vary locally
Suitable services must be available locally that can meet the person's treatment needs. In each area, Alcohol and Drug partnerships provide a forum for partners to come together to plan, develop and deliver alcohol and drug services.
The vast majority of treatment services are not directly linked to the justice system, but rather are NHS, social care or third sector services, which someone on a treatment order would be required to engage with. In some places the treatment available via DTTOs is additional to that which can be accessed by other routes, while in others, DTTOs only utilise the same services that can be accessed by anyone in the community who needs them.
Each NHS Board and Integration Authority may develop or commission the services they consider are necessary in their area. There is no detailed map of the types of services available across areas in Scotland, or centralised evidence on their quality or evaluation. Services are regulated and guided by a range of different sources and organisations. Most notably for this review:
In relation to service design and development:
- Service design advice and recommendations are developed by Health Improvement Scotland for policy makers, NHS Boards and Integration Authorities to take into account in planning their services.
- Specific standards for delivery are also developed by Health Improvement Scotland, with an expectation that Boards and Integration Authorities meet all standards. This includes the Medication Assisted Treatment Standards for substance use, which were developed collaboratively with several partners in the sector, with an implementation programme hosted by Public Health Scotland.
- Public Health Scotland further support service quality through provision of data and intelligence and monitoring and evaluation support.
In relation to front-line delivery:
- Front line health professionals are mostly regulated at the UK level: doctors by the General Medical Council, Nurses by the Nursing and Midwifery Council, and allied professionals by the Health and Care Professions Council.
- Practitioners are guided by evidence-based clinical guidance developed by the Scottish Intercollegiate Guidelines Network (SIGN) and the Scottish Medicines Consortium. Independent professional Royal Colleges and Faculties also provide specialty-specific information and advice to practitioners.
- Justice social workers are regulated by the Scottish Social Services Council. They utilise accredited risk assessment tools, and work within national practice guidance.
- Premises are inspected by the Healthcare Environment Inspectorate and the Care Inspectorate.
- Justice social work and wider support services are inspected by the Care Inspectorate.
In this context, there is no consistent model across Scotland in terms of which services are available, how they are delivered, what eligibility criteria are applied, or how quality is monitored and assured. Additionally, the sector is currently in a phase of rapid change and some expansion, as the new Medication Assisted Treatment Standards are gradually implemented and additional funding linked to the drug deaths emergency is used to implement new services, approaches and research.
Consequently, it is not possible to provide a clear or straightforward idea of which services might be offered to someone on a treatment-based community order. Some impressions can be gleaned, however, from Public Health Scotland data, annual reporting on ADP activity and implementation of the MAT standards, in the sections that follow.
Sectoral capacity, access and quality
- Although variation in clinical policies and practices in relation to the MAT standards has decreased significantly as implementation has progressed, some variability remains. In particular the proportion of people being prescribed long acting injectable buprenorphine and the number of days to receive opioid substitution therapy are noted as having wide ranges.
- The sector faces challenges to ensure services remain consistent and resilient. In particular recruitment and retention of staff.
- An Audit Scotland update on drug and alcohol services in 2022 noted that the sector has only recently begun to recover from previous gradual declines in funding: "Overall funding to alcohol and drug partnerships reduced over several years, but by April 2021 it returned to around the level it was six years ago in cash terms, but with no real terms increase in funding." The announcement of the National Mission on Drugs and the supporting additional £250 million made available in 2021 by the Scottish Government, mean the real terms increases in funding from 2014/15 were a 16 per cent increase in 2020/21 (total funding was £98.2 million) and a 67 per cent increase in 2021/22 (total funding was £140.7 million). Recent uplifts in funding mean that ADPs now receive the highest level of funding on record, a continued 67% increase in real terms to £161.6m in 2023/24. Audit Scotland raised in their 2022 report that it was difficult to track how spend was distributed, spent and monitored. Since then Scottish Government have taken action to improve financial transparency primarily through the publication of two annual reports (21/22 and 22/23) which set out how funding was distributed across Scotland. ADPs are now also required to submit bi-annual financial reporting which monitors spend in services. ADP funding allocations are published annually on the Scottish Government website.
- The justice system relies on multiple data systems that are not set up to record the data required to enable implementation and measurement of the MAT standards, and that do not communicate across the justice system or community systems. Mapping work carried out to support MAT standards implementation identified no capacity for data collection and analysis within the current workforce.
- The MAT standards implementation review (Public Health Scotland, 2023a) found that despite operating procedures – including pathways between secondary care, justice, housing and primary care – the proportion of referrals from these sources is very low, indicating "a lack of effective operational pathways and data sharing agreements between some partners and the need for stronger links with hospital admissions." Particularly in support of assertive outreach (MAT Standard 3), there is a need to develop guidance aimed at ensuring consistent multi-agency risk assessments and assertive outreach whenever someone at risk of drug harm is identified by any agency.
- The MAT Standards Implementation Review also identifies a number of risks to the sustainable success of the MAT Standards, including:
- that unsustainable and under resourced systems may prevent improvement work from happening;
- that funding uncertainties could lead to a decrease in the quality and quantity of care that can be provided;
- that small ADP teams will be overwhelmed;
- that senior and intermediate management support will wane; and
- that an overemphasis on achievement of RAGB scores will undermine the focus on ensuring that there is meaningful benefit to people as a result of the changes implemented.
Treatment types
The figure below shows Public Health Scotland data on the treatment types that people are referred to from different justice services in 2021/22. Caution should be used when interpreting this data, particularly because:
- Individuals may be recorded in the dataset for multiple episodes of treatment, each treatment episode may involve multiple referrals, and each referral may result in multiple types of treatment. Consequently, the counts below reflect referrals to each treatment type, rather than the number of individual people.
- The treatment type is recorded at the point that a person receives a treatment start date, and due to challenges with the implementation of the new DAISY database, a large number of cases are either missing this data, have no treatment type recorded because they are on an ongoing waiting list, or have ultimately ended their engagement without commencing treatment.
- Treatment type is determined by both the person's needs, and what is available locally for them to be referred into. This data is therefore not an accurate measure of the service needs for this group, as it does not record unmet treatment needs, or cases where someone is referred into a sub-optimal treatment type because it is the only option available for them.
- Additionally, this data covers only Tier 3 and 4 treatment services. There is some variation in how the treatment tiers are defined for data collection purposes in different areas, but broadly speaking: Tier 1 and 2 services include information, advice, risk screening, brief psychosocial interventions, harm reduction interventions, needle exchanges and aftercare. These are not reflected in the data, but such services can still play an important role in minimising harm, promoting wellbeing, engaging people in the earliest phases of contemplating or seeking help to recover (Smith and Massaro-Mallinson, 2010).
- Not all residential facilities (Tier 4) submit data to DAISY, so residential treatment may be under-represented.
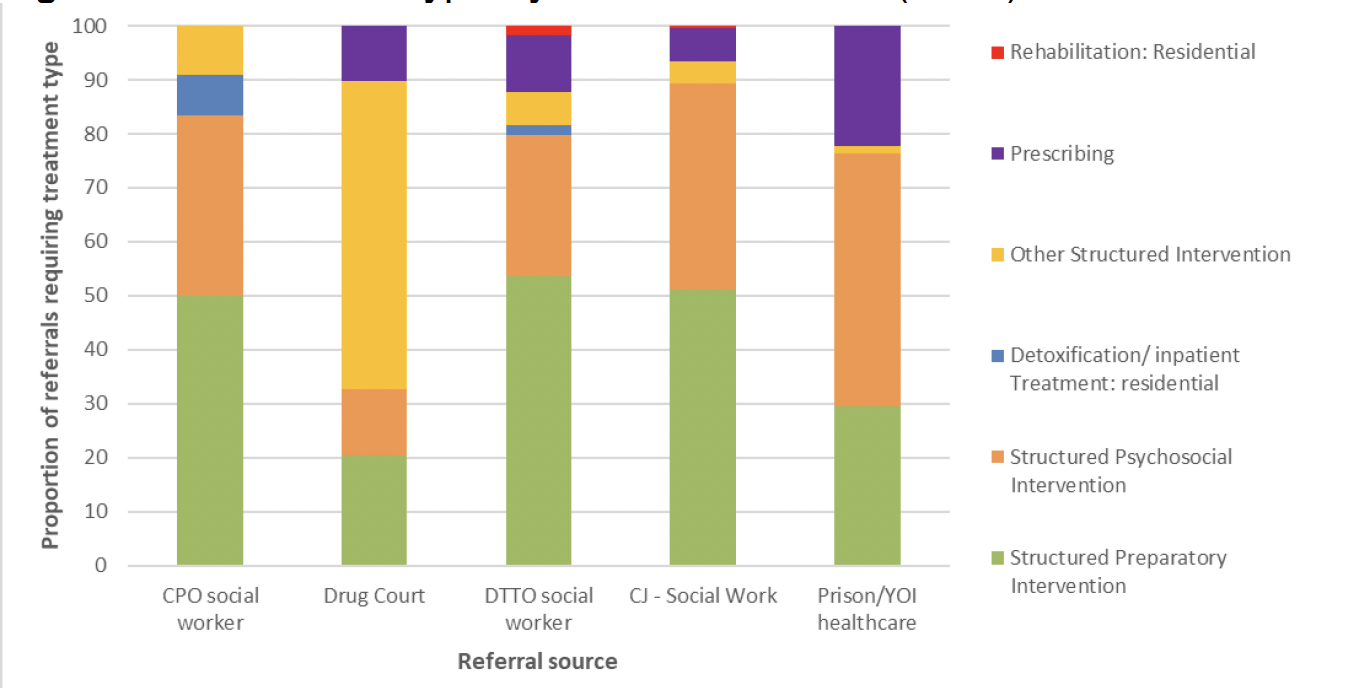
With the caveats above in mind, the following observations may be made about the data presented in this chart:
- Amongst community justice based referrals (ie those coming from a justice social worker), the most common treatment type was structured preparatory interventions. For all three of these groups, the rate is around or just over 50%, which is the same as for the general public referred from non-justice related services.
- While the evidence on mandated recovery suggests that, generally, those entering mandated treatment might be expected to be earlier in their contemplation of change, and therefore more in need of preparatory interventions than the general population, some features of the justice system may contribute to the rate remaining similar across populations. These features include:
- Social work's incentive to support people likely to succeed, and avoid setting people up for failure, may mean that people who are early in their readiness for change are not recommended for treatment based orders.
- Faced with the prospect of custody, people being assessed may have an incentive to overstate their readiness for change, or understate the severity of their drug problems, and consequently be referred directly to more intensive services before they are ready for them. While social workers are trained to consider this possibility and have tools to aid discernment, this is a process of individual human judgment and it is inevitable, in the context of an incentive as strong as avoiding custody, that some misalignment between need and treatment type may occur.
- Structured Deferred Sentences may be used in some cases to assess a person's readiness for change, rather than referring into a preparatory intervention. During the deferment, the social worker may utilise techniques like motivational interviewing to try to move the person through the early phases of readiness to change, without referring to a formal preparatory programme.
- Because of the large proportion of preparatory interventions, it is worth considering whether reporting test results to the court is appropriate in these cases, particularly before the preparatory work for change has been completed. At this stage, it is not generally expected to see significant reductions in usage, and so the purpose of reporting test results to the court can be questioned.
- People referred via CPOs appear highly unlikely to be referred for Prescribing or Residential Rehab. The rates of prescribing for DTTO and Drug Court referrals (10.5% and 10.1% respectively) are only slightly lower than for non-justice related referrals (11.3), while referrals from custody-based health teams have almost twice the rate of prescribing (22.3%).
- Detoxification / Inpatient Residential Treatment is significantly more common for people referred via CPO (7.5%), than either general non-justice related referrals (2.5%) or people referred via DTTO (1.8%). This may appear counter to expectations, since both DTTOs and residential treatment tend to be aimed at only the most entrenched drug problems. However, it likely reflects the paradox, highlighted in the section on eligibility criteria, that beyond a certain threshold of severity the person is likely to struggle to comply with a DTTO and social work or the courts may consider a CPO more appropriate in order to avoid the person being "set up to fail".
- There are additional categories of treatment in the data set – specifically structured day programmes and community-based detoxification – that are used occasionally in the wider population, but have no recorded cases of people entering via a criminal justice related referral in this time period.
The specific details of service types and delivery modes are not collated anywhere, so it is not possible to assess the extent to which people in Scotland have access to the comprehensive "matrix model" that reflects gold standard service for people in mandated treatment. Drawn primarily from reporting on the implementation of the MAT Standards (2023a) (unless stated otherwise), findings that provide a partial picture are:
- Range of services: In 2022, the Scottish Parliament's Criminal Justice Committee reported on the need for urgent justice sector reforms. Witnesses before that committee indicated that "there is a need for a wider range of community services for people for whom prison should not be an option", and for treating "the reasons for drug use, such as trauma, poverty, neglect and abuse".
- Harm minimisation: In the most recent annual returns, all ADPs reported that they have drug services that supply Naloxone, and the majority offer Hepatitis C testing, injecting equipment and wound care in community health care services, pharmacies, and/or third sector drug services. All ADPs also reported undertaking activities to support the development of recovery communities in their area, such as mutual aid groups, Self-Management And Recovery Training (SMART) groups, recovery cafes, recovery support groups, family support groups, and kinship care support. The groups reflect a variety of organisations, including delivery partners, churches, community interest companies and third sector organisations.
- Retention: OST treatment services appear to be effective at retaining people in treatment, with a reported 91% retained for at least six months. However, a two month sample showed that the majority (63%) of discharges were defined as "unsupported".
- Residential facilities: Recent analysis of residential rehabilitation facilities carried out by the Scottish Government's Population Health Directorate highlighted a number of issues with access to residential rehabilitation. Of particular relevance to the community justice population is the lack of structured preparatory work to ensure people enter treatment with the best chances of success. As noted earlier, people entering treatment via the justice system are likely to be less advanced in the process of change than the general population of people entering treatment, making preparatory work especially important. This work highlighted a need for more preparatory work to be available to people, and a challenge in the current variability of programmes offered, agencies involved, and ease of access.
- Similarly, the report also highlights a lack of suitable detox services, and of structured pathways between detox and rehabilitation services. This is particularly the case for people who use benzodiazepines, or who require a complex detox. Issues highlighted include:
- Lack of funding for residential rehab spaces, and a wide variety of different funding arrangements in different areas.
- Substantial barriers to accessing rehab for people who use benzodiazepines, potentially caused by clinical staff shortages and difficulty accessing in-patient detox.
- Lack of appropriately trained staff for supporting people with severe and enduring mental health conditions, and low staffing levels meaning such people cannot be managed safely within facilities.
- Mental health: Most ADPs report that mental health support is available for people who use drugs but do not have a diagnosed co-occurring mental health problem. This is mainly done through multi-disciplinary team working, and practices like colocation of drug treatments and mental health staff. However, most areas did not yet have protocols for referring people with co-occurring problem drug use and mental health problems, and a variety of formal and informal referral procedures appear to be used across the country. As covered earlier in this report, co-occuring mental health issues are particularly prevalent in the population of people who both use drugs and commit offences.
- Non-opioid substances: While OST has seen rapid expansion, insufficient progress has been made in the care and treatment of people using benzodiazepines, stimulants and gabapentinoids. The MAT standards implementation report discusses a 2 month sample from October-November 2022, in which a quarter of post-mortem toxicology reports detected no opioids, while 63% did detect benzodiazepines. Additionally, there has been a large increase in cocaine deaths in recent years: between 2015 and 2020 the number more than quadrupled from 93 to 459. Also of concern is that the injection of stimulants is particularly destructive, and a factor in recent HIV transmission, putting this population at particular risk.
- While medication itself has limited evidence in relation to stimulants and benzodiazepines, people suffering from the problematic use of these substances can benefit from many of the other features of the MAT standards, in particular: psychological therapies (MAT standard 6), mental health support (MAT standards 9), trauma-informed care (MAT standard 10) and harm reduction (MAT standard 4) interventions. While the growing diversity of drug-use in Scotland is a general concern across the sector, the growing use and danger of street benzodiazepines was highlighted by those in the justice sector who contributed to the Drug Deaths Task Force's Report on Drug law Reform (2021), and is worth highlighting considering the historical focus on opioids amongst DTTO services in particular.
Wait times
According to Public Health Scotland data from 2021/22, the majority of people accessing treatment through a criminal justice referral pathway have a wait time of two weeks or less. It is notable that Drug Court referrals have a substantially larger number waiting just one week or less. Whether other services can learn from the approach that enables this would be worthy of further exploration.
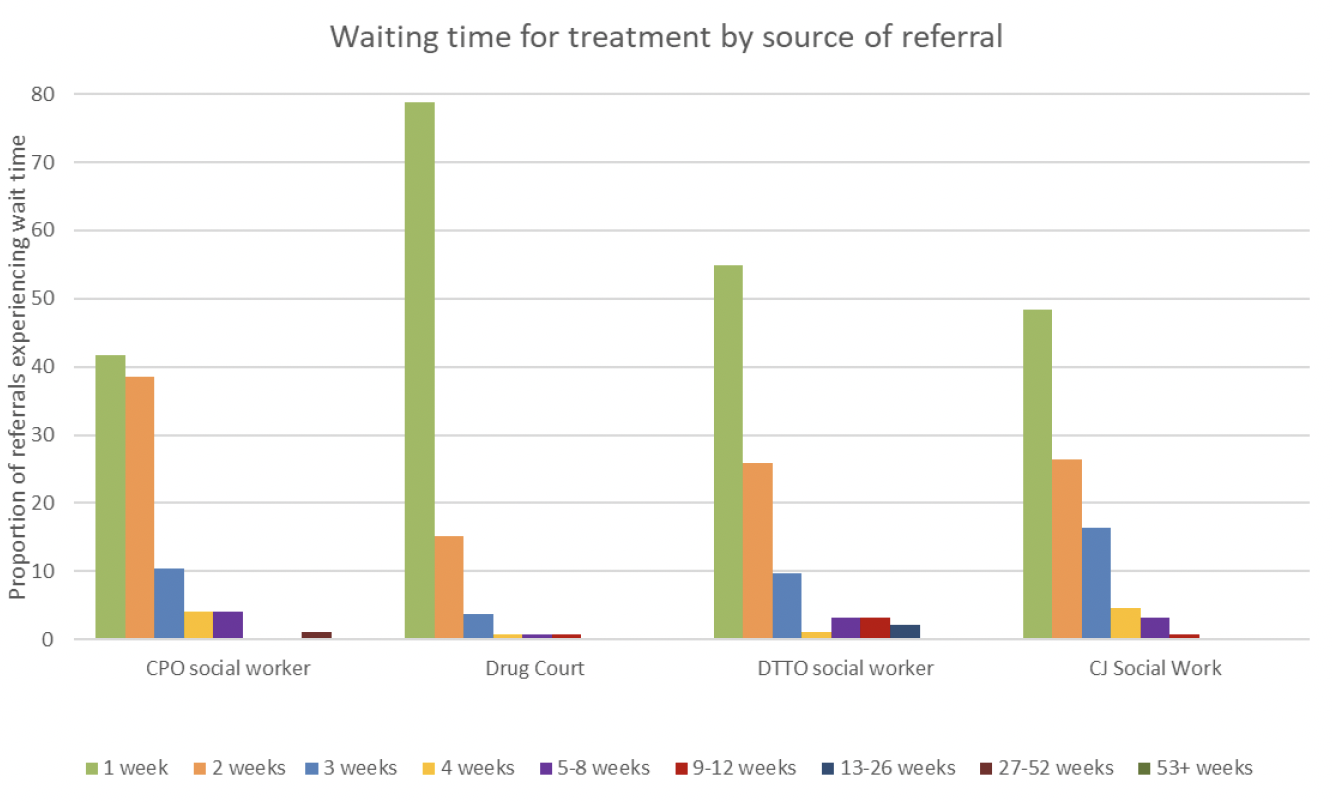
Role of testing
Testing is likely to form a part of many treatment programmes, regardless of what type of order the person is on, however it is only a mandatory and integral part of the order for DTTOs.
People who are tested regularly as part of treatment accessed via a CPO treatment requirement will generally have the frequency of tests set by the treatment service, and the results are used only to monitor their progress and facilitate honest engagement within the therapeutic relationship. Depending on the treatment type and policies of the programme, some people accessing treatment via a CPO may not be regularly tested at all.
In contrast, testing is an integral part of all DTTOs. The minimum testing frequency is set by the court, and the social worker must report all test results to the court. This requirement has received some criticism for limiting the treatment provider's and social worker's ability to engage flexibly with the person in response to failed tests. Professionals contributing to the Drug Deaths Taskforce's work on drugs and the law noted, for example, that a person may be engaging well with treatment and support but still test positive for drugs – for example, if their treatment is focused on preparatory work and building readiness for change, if they are managing to cut back on their drug use but have not yet fully stopped all consumption, or if they experience a lapse after a period of abstinence. Knowing that a failed test will be reported to the court, these people may sometimes choose to miss a testing appointment, which interrupts their regular contact, putting them at risk of disengaging from treatment, as well as then being reported for breach. The Taskforce notes that the level of compliance expected of people may often be unrealistic. Courts' expectations about levels and pace of progress and compliance, coupled with their access to all testing results, may be one reason for DTTOs' high rates of revocation at review.
Additionally, the purpose of regular testing in drug treatment is generally to enhance treatment and the therapeutic relationship by facilitating completely frank disclosure to the treatment provider, and creating opportunities for the person to experience an understanding and non-judgmental response from the treatment provider, regardless of the testing results, so that trust, confidence and self-worth is built up over time. Bringing the court, and its enforcement role, into this process may therefore harm the therapeutic relationship rather than supporting it.
The role of testing warrants further exploration, in order to better understand people's lived experiences of testing during mandated treatment, how the results are regarded by courts, and whether the mandatory reporting of results to courts strikes the best balance between incentivising people to continue engaging with treatment, while maintaining the courts' willingness to keep people out of custody wherever possible.
11. Addressing offending and social support needs
Access
As explained in detail in earlier sections, the legislation and guidance give DTTOs and CPOs different levels of focus and resource for addressing needs other than drug treatment. Social workers will develop case plans for the people they supervise, based around supporting the person to address their various criminogenic needs – both directly, in supervision meetings and home visits, and indirectly, by referring them to services and activities.
These services and activities are typically provided by either public or third sector organisations. Since 2017, community justice has operated under the Community Justice (Scotland) Act 2016, which places duties on a group of statutory partners to engage in community justice planning, and many of the services and activities will fall within the local Community Justice Partnership arrangements. These arrangements are intended to create systems that are highly tailored and flexible to local needs, but require a high level of effective communication and close partnership working to be successful.
All DTTOs and CPOs with treatment requirements will have a supervising social worker, and may receive some support from them in the course of supervision.
Practice Guidance for the delivery of CPOs, for example, includes the suggestions that:
- The case plan should be collaboratively developed with the person and, where appropriate, family members or other agencies. "The case management plan should take account of both criminogenic and other needs to meet the specific goals of the individual on their unique journey towards desistance. This may involve improving significant relationships, restoring health and well-being, securing sustainable/stable accommodation, achieving financial stability or maximising benefits, taking advantage of meaningful learning opportunities and developing new employment skills."
- Delivering CPOs is likely to require involvement from "community justice partners and […] individual mainstream agencies, such as Jobcentre Plus, the health service and local authority housing departments" as well as "voluntary and private sector organisations".
- Individual Engagement Contracts could include "a wide range of issues, including: education and training; help with family issues & parenting; advocacy – benefits and housing; participation in offending behaviour programmes; participation in drug and alcohol programmes; constructive use of leisure time; and physical and mental health."
- Literacy and numeracy needs, in particular should be assessed and addressed if necessary.
- Providing practical help to people who lack settled accommodation should be considered part of the normal duties of a social worker supervising a CPO, because suitable accommodation helps people to stabilise their lives, and improves their prospects of engaging with other interventions aimed at reducing the risk of re-offending.
The role of the supervising social worker in a DTTO is, uniquely, limited by statute. Section 234C, sub-section (8) of the Criminal Procedure Scotland Act 1995 states that "supervision by the supervising officer shall be carried out to such extent only as may be necessary for the purpose of enabling him to:
a. report on the offender's progress to the appropriate court;
b. report to that court any failure by the offender to comply with the requirements of the order and;
c. determine whether the circumstances are such that he should apply to the court for the variation or revocation of the order."
It should also be noted that social work practice has evolved over the years . Many areas have developed a holistic approach adopting the Recovery Model for their DTTO teams. This provides additional wraparound support, without adding compulsion to engage. This, along with the current legislative framework, is worthy of further exploration.
Variety and quality of support offered
The Community Justice Scotland's Annual Report on Community Payback Orders reported that areas were attempting to use contact with the justice system as an opportunity to identify and address wider needs, and many were taking active steps to help people into services (although, as with health treatment, devolution to local areas means services and approaches are not consistent across all areas). For example:
- Many areas described providing practical assistance to people, such as food parcels, toiletries, mobile phones and travel support. The report notes that this indicates a significant basic unmet need within the justice-involved population.
- Some areas have bespoke local approaches to mentoring, particularly involving people with lived experience. An example cited is the Edinburgh and Midlothian Offending Recovery Support Service, which has recruited a "recovery motivator" with lived experience to support people with both recovery and desistance.
- Some areas report using Housing First or Rapid Rehousing approaches, although it remains unclear how well integrated these are with community justice, and success is limited by structural challenges such as housing availability and the complexity of justice-involved clients. One example that does appear to be specifically integrated with justice services is Highland's Rapid Rehousing project, which targets complex cases that are not eligible for the local Housing First programme. However, overall, the CJS annual report on CPOs found that "Securing suitable housing for people subject to CPO continues to be problematic for some local authority areas, particularly for a cohort that generally requires single occupancy and flexible tenure options."
- Some areas provide interventions focussed on mental health for those in the justice system, which take various forms including community psychiatric nursing contact, specialist psychiatric assessment, crisis suicide prevention, and broader wellbeing and resilience interventions. However, Community Justice Scotland's Annual Report on Community Payback Orders also found that "A dual diagnosis of mental health and addiction difficulties continues to act as a barrier to services for individuals, often due to how service criteria is linked to funding." One area has partnered with their local Autism service to commission training for all justice staff on awareness and bespoke interventions, with longer-term practitioner forums being developed.
- Some areas have approaches intended to engage people with employability services. In one example, one-to-one employability support is offered, intending to address people's individual needs.
While attempts to identify and address the underlying needs of people in contact with the justice system is positive from the perspective of both addressing offending and connecting vulnerable people with the support they need, the context that makes this necessary should also be considered. In the report Hard Edges Scotland (2020) "a standout finding across all six case study areas was the extent to which the criminal justice system was used as the last resort 'safety net' for people facing SMD whom other services routinely failed to provide with the help they desperately needed."
The relationships between Community Justice partner services and Alcohol and Drug Partnerships vary across the country, although CJS's annual report on CPOs found that "Many areas report excellent links with their local Alcohol and Drug Partnerships in supporting people subject to CPO who have a substance use issue." Local recovery communities are cited as a valuable and commonly available resource, and a smaller number of areas collaborate with residential rehabilitation services. In one practice example, an 18 month post was created for a development officer to develop a "shared care" model between substance use and justice social work.
In terms of outcomes and effectiveness of community justice, Audit Scotland highlighted that improvements should be made in its 2021 report on Sustainable Alternatives to Custody. A revised Community Justice Performance Framework was published in March 2023, and work is ongoing to improve relevant data access and reporting. The Community Justice Performance Framework sets out nationally determined outcomes which are to be achieved in each local authority area, and national indicators which are to be used in measuring performance against these. Assessment of progress towards these national outcomes is examined by statutory partners acting jointly at a local level, and by Community Justice Scotland.
Justice social work services are also subject to scrutiny by the Care Inspectorate, and its evidence suggests that justice social work services tend to be of high quality.
The Care Inspectorate's overview report on Justice services (2021) drew on findings from inspections of 5 local areas. While not necessarily nationally representative, it's findings are informative. In particular, that:
- Relational working
- Most people on community payback orders were positive about their relationships with community justice social work staff, felt treated with respect, and felt that the relationship encouraged them to attend regularly and engage with their requirements. The highest quality relationships had a transformative impact on people's lives. These were characterised by continuous, consistent contact with compassionate and trauma-informed staff who individualised the person's support.
- Accessing support
- People on CPOs valued the opportunity to be connected with third sector agencies such a Turning Point, Venture Trust and Shine Mentoring. Access to women's centres or hubs was also valued, although not all areas inspected provide these.
- A range of national and third sector agencies provide various forms of support, although some concerns were noted about diminishing local services, and in some cases a need for more clarity and communication on which agencies are responsible for which roles.
- Generally, people had access to the required interventions during their community payback order. Offence-focussed work was particularly evident where services had invested in, or ensured access to, a range of structured interventions and resources.
- Referrals to other support agencies were generally prompt and made as early as possible, and collaboration between community justice social work and service providers was generally positive.
- Where a comprehensive, strategic needs assessment is available, it usefully supports services and partnerships to direct resources to where they will have the greatest impact.
- Service culture and policies
- "There was a high degree of correlation between an individual's identified risks and needs and the intensity of supervision. Staff management of non-compliance and the use of discretion was an overall strength."
- Services are appropriately flexible in respect of accommodating people's personal commitments, responsibilities and travel constraints.
- Greater consistency is required in community justice social work practice in relation to the frequency and focus of reviews and home visits.
- Reporting
- Overall the standard of reports prepared by community justice social workers is "a strength".
While the evidence suggests these are generally quality services, resources are necessary to ensure that quality is sustainable. Justice social work statistics show evidence that the labour required of social workers to deliver each case may be increasing over time. For example, over the last decade the number of same-day reports requested by courts has increased, and courts are now significantly more likely to request these be written reports rather than presented orally. Similarly, since 2015/16 the proportion of community payback orders requiring supervision has increased, while the proportion requiring only unpaid work has decreased. Audit Scotland's 2021 report also noted that impacts from the Covid-19 pandemic, "including court backlogs, pressures on finances and a delay in offenders being able to complete unpaid work hours, will add further stress to the system".
12. Enforcement and outcomes
Opportunities for revocation
There are three main ways a community based order can come to an end: the person may successfully complete the order, the court may revoke the order due to a breach by the person, or the court may revoke the order at a review hearing, if they no longer view the order as appropriate for the person or their circumstances. If the order is revoked, it will be replaced with an alternative sentence. Orders may also be terminated within the dataset if the person moves to a new area or dies.
The chart below provides an overview of the proportion of orders with each of these outcomes between 2015 and 2022. It is notable that the successful completion rate for DTTOs is lower than for either CPOs with a treatment requirement or other types of CPO. This is to be expected, since the people who receive DTTOs are likely to be, on average, those with the most serious / entrenched drug problems. Amongst orders that are revoked, DTTOs are significantly more likely to be revoked at review, while other orders are more likely to be revoked due to breach. There are a number of ways to interpret this finding, but some possible factors are:
- People on DTTOs may be complying with their treatment order in a way that their social worker finds satisfactory, but that their Sheriff, upon review, considers inadequate in terms of the progress made in their drug use or other behaviour. People on CPOs of any sort are less likely to face court review, and to face it less frequently, than people on DTTOs - reducing their opportunity for revocation due to review.
- On some occasions when a social worker perceives that a person may have breached their order, they may not consider it necessary to submit a separate breach report if the person has a regular review hearing in the near future, as they can alert the court to the breaching behaviour at that review. Such cases may be recorded in the data as revocation due to review, but are, at least in part, triggered by the breaching behaviour. Again, because of the higher frequency of reviews for DTTOs, this may be more likely to happen in a DTTO than a CPO.
Additionally, it is noteworthy that, although completion rates for all the orders shown below increased during the pandemic, this increase was particularly substantial for DTTOs. The reason for this cannot be inferred from the data available, but some relevant factors may have been:
- the decrease in socialising, nightlife and time outside the home making it harder for some people to access or use drugs, or to commit other offences or breaches;
- the significant reduction in testing carried out, since this can only be done in-person;
- the significant resource put into accommodating homeless people, and making tenancies more secure, during lockdown measures; and
- the shift to virtual contact with supervising social workers removed the need for most people to attend at an office, which may have made it easier for people to consistently attend supervision.
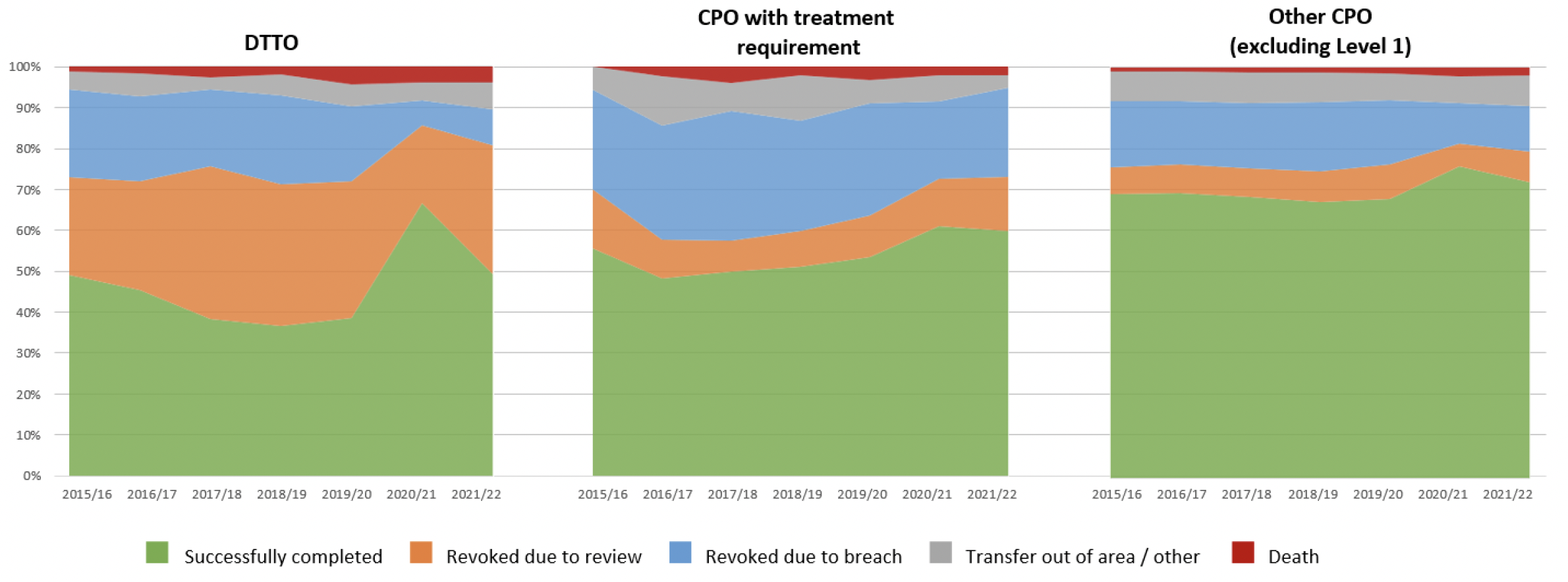
Breach applications should be lodged as promptly as possible once the social worker has decided it is necessary report a breach to the court. Over the last 5 years, the proportion of breach applications lodged within 5 working days has steadily increased for DTTOs and is now at almost 100%. In this time, all other categories of CPO have fluctuated around a lower mean.
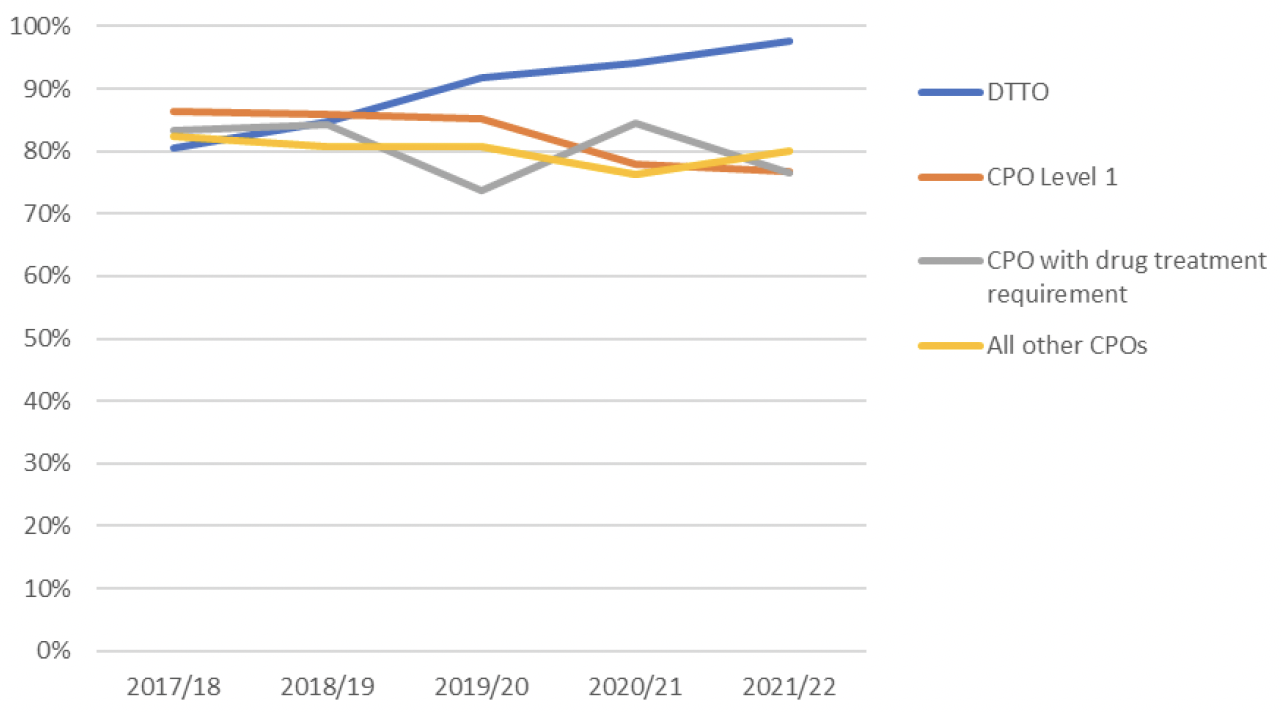
The chart below shows the proportion of each type of order that have one, two, or 3+ breach applications made to the court. The proportion of orders that proceed without any breach applications being made is relatively similar across the three types of order: the rate varies from 81% for both the DTTO and "other CPO" category to 71% for CPOs with a drug treatment requirement.
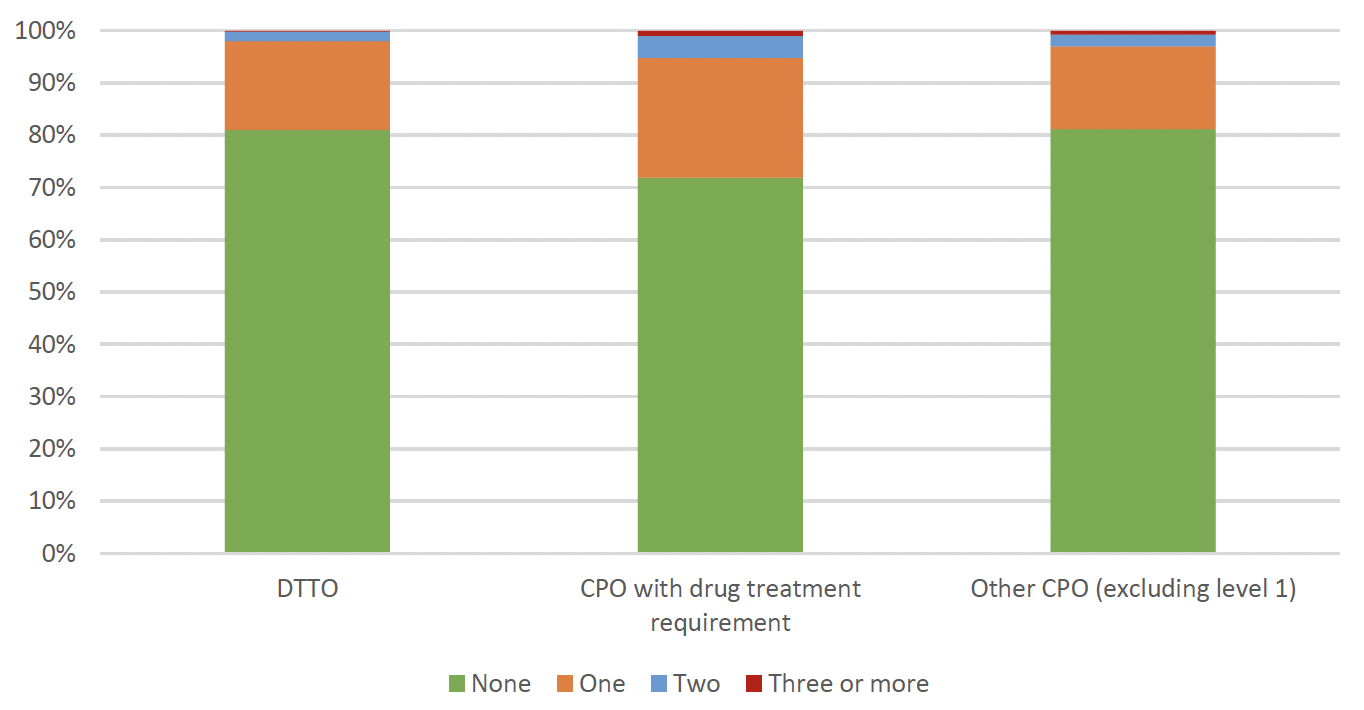
However, the proportion of cases with a breach application that are ultimately revoked due to breach is more variable. Looking only at those cases with at least one breach application, we see that:
- 39% of DTTOs with at least one breach application are ultimately revoked due to breach
- 72% of CPOs with a drug treatment requirement, that receive at least one breach application, are ultimately revoked due to breach
- 56% of other CPOs (excluding Level 1 orders) that receive at least one breach application are ultimately revoked due to breach.
Again, the reason for this is not readily inferred from the data. One possibility is that the court may be more likely to allow a person to continue on their order, despite a breach, if they know they will review the person again soon. Consequently, the frequency of review hearings for DTTOs may make the court more confident in allowing the person a second chance after a breach, knowing that they will have another opportunity to revoke the order relatively promptly if the person does not change their behaviour.
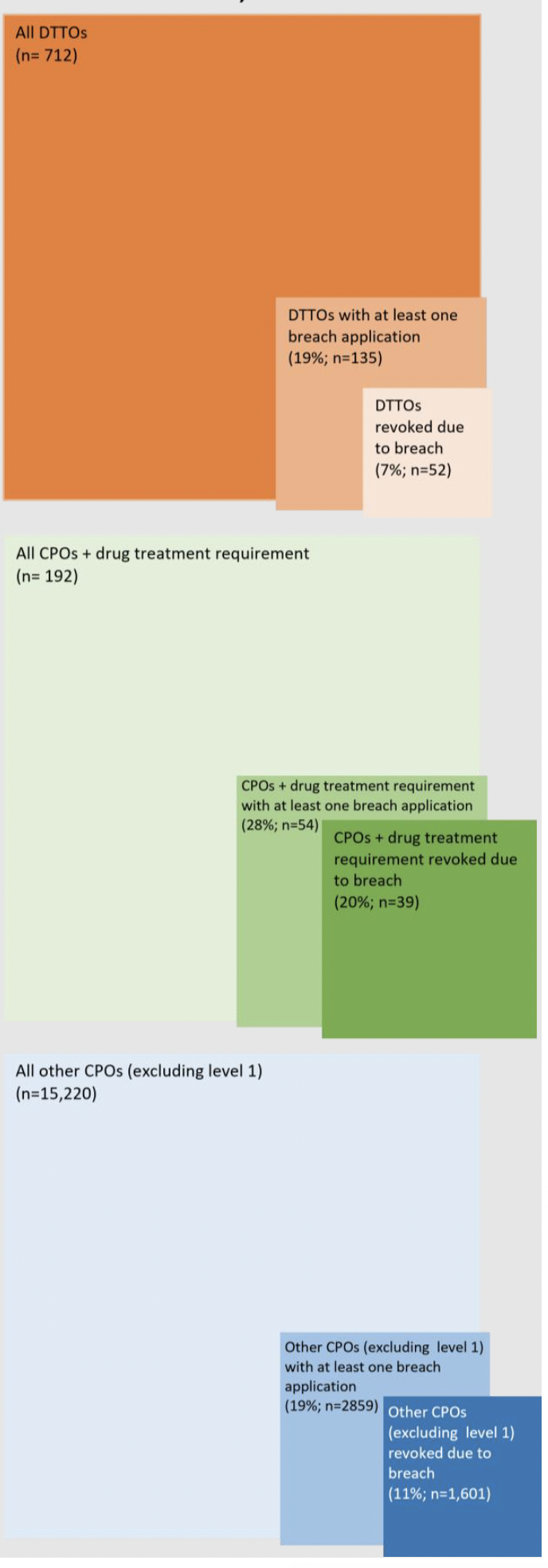
Outcomes following revocations
The chart below shows DTTOs, and CPOs with a treatment order, alongside all other CPOs (excluding level one orders) for context. It shows the break down in terms of completion, mode of revocation and alternative outcome once revoked. It is notable that:
- DTTOs and CPOs with a drug treatment requirement have, over the past two years, had similar overall completion rates. While they differ in terms of whether a revocation is more likely to come about due to breach or review, the probability of revocation itself does not vary between the two groups. It should be noted, however, that this is influenced in part by the unusually large spike in completions caused by pandemic measures (discussed above), and that in the years prior, DTTO completion rates were generally slightly lower than those of CPOs with treatment requirements. It remains to be seen how this pattern will proceed over subsequent years as the pandemic recovery continues.
- This is in contrast to the "all other CPOs" category (which excludes Level 1 orders), which has a notably higher completion rate at 81%. This is to be expected, since substance use is a significant criminogenic need in itself, and also tends to be correlated with, or even compound, other criminogenic needs.
- Additionally, rates of "other penalty" and "other outcome" categories are also similar between DTTOs and CPOs with a treatment order.
- Custody is slightly more common for orders revoked at review than for those revoked due to breach, across all order types. Overall, 33% of revoked DTTOs, and 38% of revoked CPOs with a drug treatment requirement resulted in custody. The higher rate for the latter category is mostly accounted for by a greater proportion of custodies following review. Only 21% of all other CPOs (excluding Level 1 orders) revoked resulted in custody – as above, this is to be expected because this group is likely to have, on average, less severe criminogenic needs.
- The number of unknown outcomes is consistently higher for revocations due to breach, compared to revocations at review. This may indicate an issue in data recording or flow in the breach process, which may warrant further consideration.
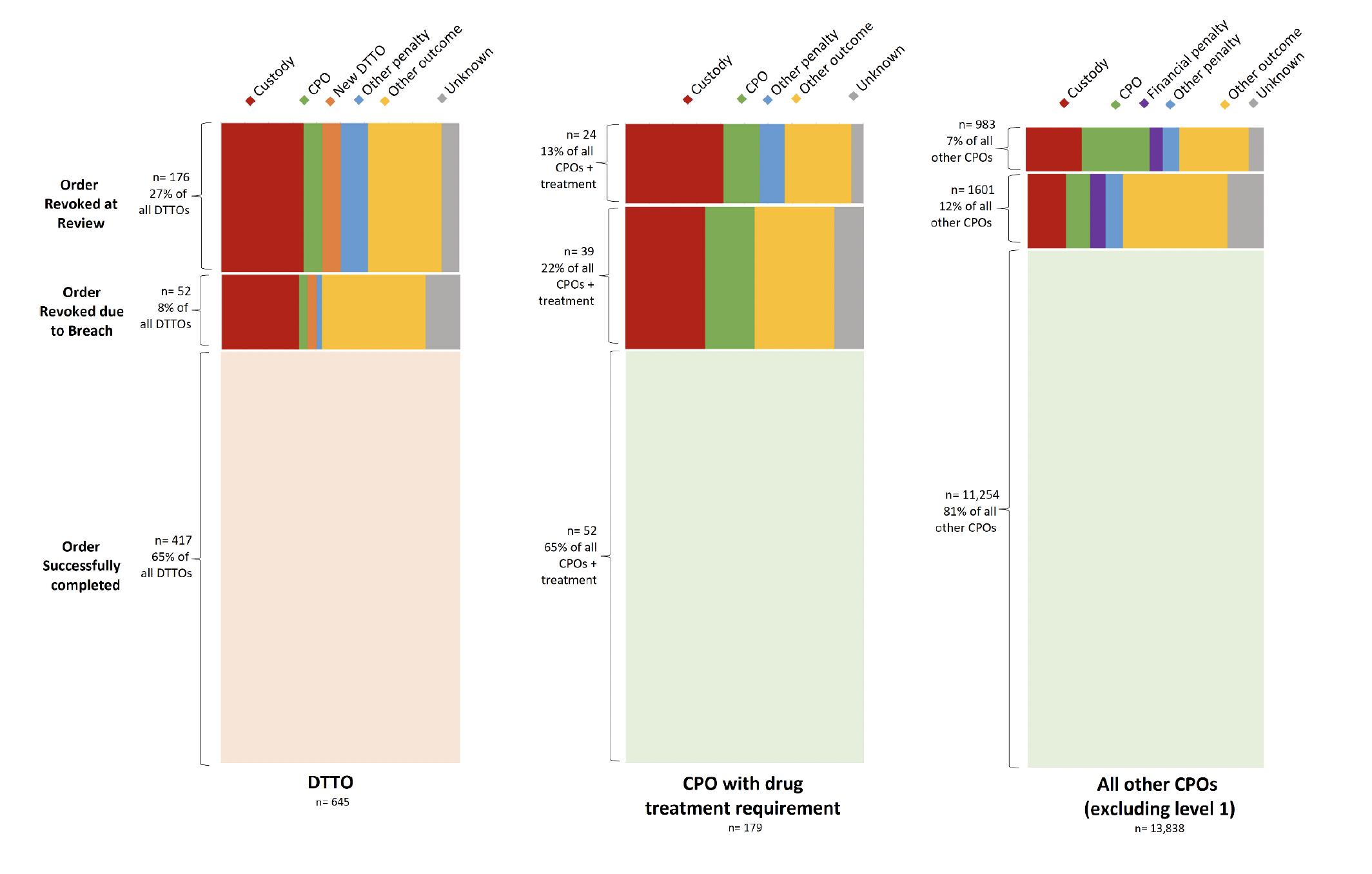
Reconvictions
Before considering reconviction rates for DTTOs, some important limitations of this data must be borne in mind.
- Data on reconvictions are only available for the 12 months following sentencing, so long term reconviction trends are not available and it cannot be known whether differences between different orders persist beyond 12 months.
- Reconvictions data looks at the first time a person is given a disposal in a specific time period, and whether they reconvict within a year. It is possible that they may have received other disposals prior to this time period.
- Additionally, since most DTTOs and CPOs with treatment requirements are made for more than 12 months, most people reconvicted in this timescale will still be on the order at the time of the new conviction. This fact, coupled with differences in the ways cohorts are recorded in the data sets, means it is not possible to look at whether successful completion of a treatment based order is associated with any difference in reconviction rates. Consequently, the reconvictions data that is available must be interpreted with significant caution.
- Finally, reconvictions data does not disaggregate the different requirements attached to a CPO, so it is not possible to compare DTTOs to CPOs with a treatment requirement. Because of the significantly wider breadth of offender characteristics and offense types represented in the general CPO group, this is not an appropriate or informative comparator.
With these caveats noted, the data show that people given a DTTO have the highest likelihood of being reconvicted within 12 months, and the highest number of new convictions within 12 months of any disposal, varying between 58% and 67% over the last decade. This is to be expected, considering that people receiving DTTOs will have, on average, the most entrenched drug problems and some of the highest criminogenic needs in the community-sentenced population. Consequently, as noted in the National Statistical Bulletin on Reconviction Rates, this should not be interpreted as indicating a particular lack of effectiveness for these orders. Over time, both the reconviction rate, and number of reconvictions per offender, have fluctuated with no clear directional trend.
After receiving a DTTO, if a person is reconvicted within a year they are relatively unlikely to receive another community based sentence. Over the last decade, the proportion of such people receiving a second DTTO has never exceeded 3.6%, and at times has dropped below 1%. Due to the time required to complete a DTTO, it is unlikely for a person to receive another DTTO within a year. Most people in this position will receive a custodial sentence, with about half as many receiving a CPO. These high rates of custodial sentences likely reflect the fact that to have received a DTTO in the first place, the person's offending record must already be sufficiently severe to put them at risk of custody. However, whether the low rates of offering a second DTTO (or a CPO with a treatment requirement) reflect good practice may warrant further exploration.
It is also notable that, over the last decade, the number of custodial sentences for reconvictions following a DTTO are significantly higher than the number of individual people receiving them, indicating that people sent to custody for a reconviction following a DTTO often receive multiple short sentences within a 12 month period. While this indicates relatively prolific offending, it suggests that the relevant offences are not necessarily severe. This pattern is less strong in the data for the 2019-20 cohort than for preceding years, likely due to the pandemic affecting all parts of the justice system. It may also reflect an impact from the presumption against short sentences.
Considering that it is normal to require multiple attempts at treatment and recovery, people who struggle or falter either during or following a treatment order may not necessarily be "set up to fail" if given another one. The first DTTO can arguably serve as a learning experience for both the person, and the professionals supporting them, so that on a subsequent order they can derive more benefit from, for example, beginning treatment with more preparatory intervention than previously, working with treatment providers or modes that suit them better, and drawing on the perspective and adjusted expectations they may have gained from the first experience. Current legislation does not prevent this from taking place, so the low levels of DTTOs (or other community based disposals) for reconvictions following a DTTO should be explored with stakeholders to better understand the reasons for current patterns and whether they are considered to reflect good practice.
13. Assessment of practice against the evidence base: conclusions and areas for exploration in relation to delivering orders and treatment
Again, the evidence reviewed in this chapter shows a complex system and a high degree of local variability. While limitations in the data make it difficult to draw a complete picture, in general the evidence suggests that justice social work services tend to provide quality assessment and support, while drug treatment services can be more variable, but are working through a period of implementing change and are aware of key challenges the sector faces.
There are some findings from this review that suggest specific pieces of work that may be necessary.
DTTO guidance
The guidance for DTTO schemes is now significantly out of date: having been published in 2011, it pre-dates the current Community Justice structures that have been in place since 2017, as well as the current crisis of drug deaths. It also refers to a number of outdated features in the justice system, including Probation Orders (replaced by Community Payback Orders) and Social Enquiry Reports (replaced by Justice Social Work Reports). Other elements of the guidance appear to be inconsistent with current day practice or service structures, and the advice it contains on both mental health and homelessness are ambiguous. To make the practice guidance fit for purpose in the current context, consideration of review and update in line with current evidence and best practice is warranted.
Reviewing the current delivery of support and treatment through these orders also highlights a number of areas that warrant further exploration with stakeholders (including people with lived experience) and consideration by policy makers. In particular:
The balance between support and enforcement
The dynamic between the offer of support, and the enforcement of engagement with that support, is a nuanced one. This is particularly true in the context of the present legislative limitations on supervision in DTTOs. The evidence review found that one feature of effective mandated community drug treatment is responding to multi-problem clients with an integrated and comprehensive care package. Compared to a DTTO, a CPO with a drug treatment requirement may offer less scrutiny of the person's progress in drug treatment (because tests are not reported to the court, and court reviews are less common), but also involves both more support and more scrutiny of their progress in other domains of life. Depending on the person and their circumstances, and the court's and social worker's expectations, this could either be an enabling factor or a barrier to successful completion of the order. Such scrutiny and enforcement may have the unintended consequence of de facto criminalising need, but on the other hand it may also be a necessary level of control to hand the courts in order for them to be willing to keep the person out of custody. This dynamic, and the legislative limitation on social work's role in supporting people on DTTOs, may therefore warrant further exploration. Some areas have developed models where additional, voluntary support is offered to people on Level 1 CPOs (who are not required to engage with supervision). This may be one model worth considering within the bounds of the current legislation for providing additional support to people on DTTOs as well, and indeed this Review was made aware that some areas may already be doing this. Considering the generally positive findings regarding the quality of justice social work services, there is reason to believe they may be a valuable asset to many people on DTTOs.
Therapeutic alliance and harmonising expectations
The crux of designing effective approaches to mandated treatment is balancing the justice system's need for accountability and enforcement with effective treatment's reliance on a compassionate and patient therapeutic alliance. Whether this balance is appropriately struck by current approaches is worthy of deeper consideration, particularly from the perspective of people with lived experience of court mandated treatment. For example, how can the justice system's intrusion into the treatment provider's therapeutic alliance with the person be minimised? How can the social worker's relationship with the person be made as therapeutic as possible, notwithstanding their enforcement role? How can courts and sheriffs learn from models of therapeutic alliance to interact with the person in a way that minimises the potential criminogenic harms? Some potential answers to these questions have been identified in the evidence review, but the experiences of people both subject to, and working within, the justice system will be paramount to identifying practices that will work in the Scottish context specifically.
Within this general theme, some areas that may be fruitful to explore are:
- the role professionals and sheriff's see drug testing results as having in their current practice, and whether the current levels of test reporting are necessary to achieve an order's goals.
- how to deliver the specialist training on substance use, sub-conscious stigma and the skills of therapeutic alliance building that this evidence review has found to be features of an effective mandated treatment system.
- ways that judicial, social work and health providers' expectations of people on orders might be better harmonised around a realistic, public-health oriented model of recovery journeys, with a view to reducing the need for revocation, and potentially increasing the possibility of additional opportunities in the community for people who do not complete their order, or are reconvicted.
Service structures and funding
This review has found a high degree of variation in service structures and funding, the appropriateness of which may warrant consideration. The delegation of community justice and health care is intended to provide flexibility to local needs, and it is a natural consequence of this model that community sentences and drug treatment will vary in different areas. However, the high variation in arrangements presently observed, coupled with the grave seriousness of both the public health emergency and the prospect of using the state's coercive power to mandate drug treatment, raises questions about what consistency might reasonably be expected, and in turn about equality before the law. It may be appropriate to consider whether more should be done to standardise provision, or to facilitate systematic learning between services so that over time we might expect to see more convergence on models that are most effective.
Relatedly, consideration should be given to the specific resource and logistical challenges highlighted by services, and experienced in key parts of the social work and health sector work forces. The evidence review suggests that adequate specialist staff, co-location of justice and treatment staff, pre-review meetings, dedicated coordination roles, and joint training and awareness raising are all features likely to improve service quality. Services that are delivering these features may be useful sources of learning. Additionally, the notably shorter waiting times for entering treatment via a drug court, compared to other community justice referral sources, may also be something that can be learned from.
Service available
Generally, more work is needed to better understand the range of treatment types available in each area, and whether they reflect a model that is, per the recommended "Matrix Model" sufficiently:
- Intensive (model recommends 4-5 days per week)
- Extensive (model recommends minimum 18 months)
- Comprehensive (incorporating multiple approaches)
The literature reviewed suggests that, in particular, there may be gaps in terms of integrated mental health support, treatments for people who use stimulants or have complex poly-drug use patterns, availability of residential rehabilitation, and intensive structured day programmes.
Consideration may be warranted in relation to whether the interventions offered are sufficiently ambitious in terms of engaging people early in the process of considering change, and whether current standards of motivation and readiness for change being applied in assessments are appropriate. These vary locally depending on the specific eligibility criteria for each programme, and are not laid out in the guidance. While people should not be "set up to fail" on community orders, any opportunity to engage someone in potentially life-saving treatment should be taken seriously. It may be possible that interventions could be developed with a greater role for preparatory drug counselling utilising evidence-based techniques like motivational interviewing and motivational enhancement therapy, aimed specifically at overcoming the engagement challenges of "mandated, coerced or concerned" patients. Similarly, facilitation of 12-step programme engagement, peer support, and early access to harm reduction, are all known to support eventual engagement with for formal treatment. On the other hand, the need to direct scarce specialist resources where they can make the most difference must also be borne in mind.
Ensuring that sheriffs also accurately understand the support and treatment available, both in each area and on each order, is also essential.
Opportunities for, and following, revocation and reconviction
A key difference between DTTOs and CPOs are the opportunities they present for revocation. While this consideration should not be overstated, due to the similar completion rates for DTTOs and CPOs with a treatment requirement, the CPO model is arguably closer to that which the evidence canvassed in this review supports. Consequently, it is worth exploring the role that each opportunity for revocationplays in an order overall. In particular, how important do sentencers consider the monthly DTTO review to be in their decision about whether they are comfortable keeping someone in the community? A more tailored, and evidence-based, approach may be achieved through the CPO model, where reviews are scheduled only if the court feels they are necessary. Similarly, how important do sentencers consider the monthly testing results to be in their decision to maintain or revoke an order? A more evidence-based approach recognising that people can engage well with treatment but still test positive for drugs, may be for justice social workers (collaborating with health and social care professionals) to interpret the meaning of testing results within the context of the person's broader engagement – and raise the results with the court if they consider them a cause for concern.
Relatedly, it may be valuable to explore the factors that affect decision-making when a person either has a treatment-based order revoked, or is reconvicted after serving one. Current legislation does not prevent multiple treatment-based orders from being made, so the low levels of DTTOs (or other community based disposals) for reconvictions following a DTTO should be explored with stakeholders to better understand the reasons for current patterns and whether they are considered to reflect good practice.
Finally, the gap in the quality of care between community and custody settings, and disruption to treatment in transitioning settings, is concerning, particularly for the significant number of people receiving a custodial sentence following revocation or reoffending. While not a primary focus of this report, these findings form an important part of the context in which sentencing decisions are made, and custody is the most likely counter-factual for many, if not most, people on mandatory treatment orders.
Characteristics of the relevant populations
The data presented below are based on LSIR data, an explanation of the variables is given above in section 3.2.1.
Data on those who receive a full assessment after sentencing
More detailed data on people with drug related problems is available for those who receive a full assessment after sentencing. This generally takes place if they have received a sentence that requires supervision, or some custodial sentences. In these assessments, social workers assign a score based on the extent of the person's "current drug problems", where 0 = "substance abuse seriously interferes with maintaining a prosocial lifestyle", and 3 means the person does not have drug related problems. The figure below shows how these scores have been distributed in the last 5 years, including a gradual downward trend in the proportion who are recorded as having no drug problem:
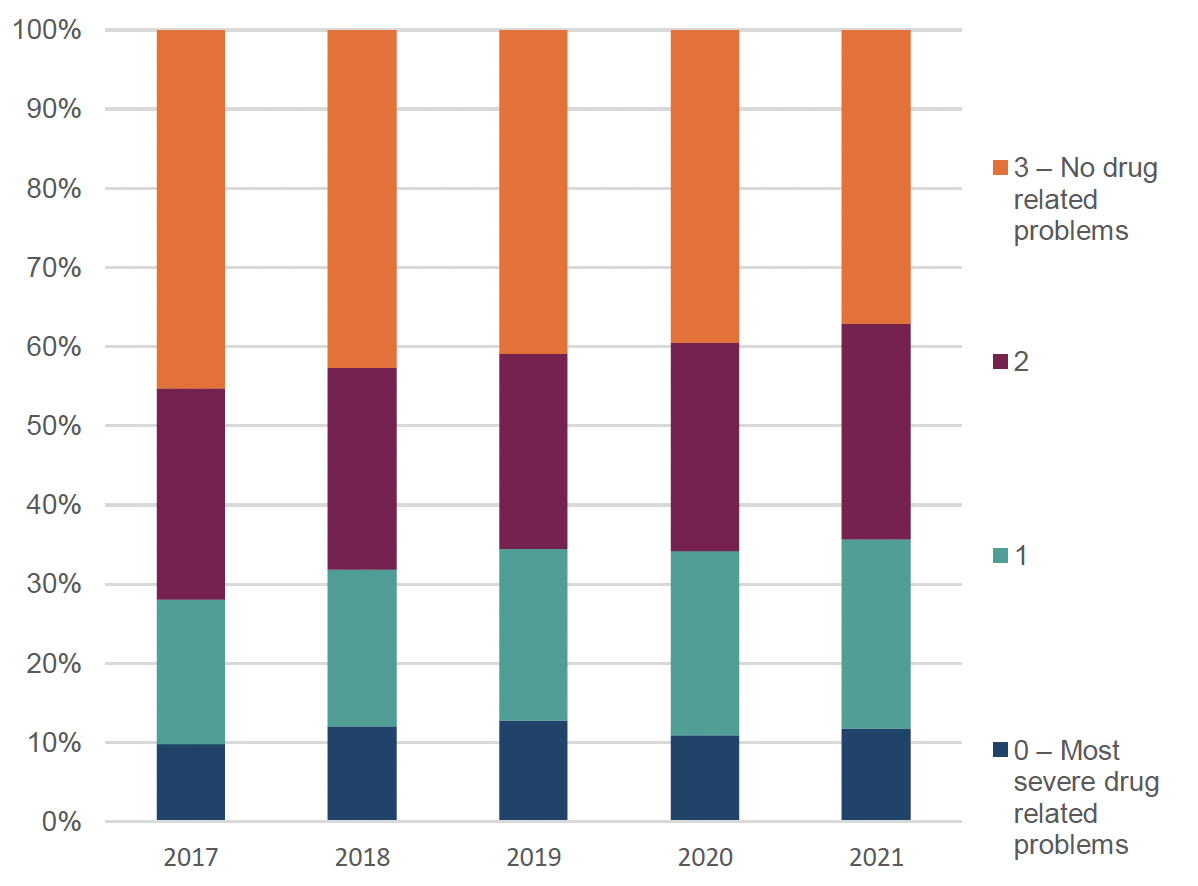
For the purposes of this analysis, people scoring 0 or 1 (on a scale from 0-3) on the LSCMI variable "current drug problem", meaning those with more than minor drug related problems, have been compared to the remainder of the population receiving the same assessments. For ease, these groups will be referred to as "people with drug-related problems" and "people without drug related problems" in this section of the analysis.
Demographics in the populations of interest
Sex
Amongst people receiving initial assessments to inform pre-sentencing justice social work reports, men are slightly more likely to fall into the group that is potentially likely to have drug related problems, than show no indication of drug related problems. Between 2017 and 2021, 84% of those in the "no drug related problems" group were male, while in the group potentially likely to have drug related problems, 86% were male.
The most recent release of justice social work statistics (data up to 2021-2022) shows that over the preceding 5 years, around 80% of DTTO recipients have been male – suggesting that men with drug related problems may be less likely to receive a DTTO than women with drug related problems (although the analysis did not control for other factors that may influence this outcome such as offending type or severity).
In the same time period, 85-86% of CPO recipients have been men (although this does not separate out those with drug treatment requirements).
Amongst referrals into treatment services in 2021/22, Public Health Scotland data records that between 80 and 86% of referrals made by community-based justice professionals were for males, as were 93% of referrals from prison or YOI health teams. Across all justice referral sources, DTTOs had the highest proportion of females, at 20%.
Age
Amongst people receiving initial assessments to inform pre-sentencing justice social work reports between 2017 and 2021, people who are potentially likely to have drug related problems tend to be clustered towards the middle age brackets, with 72% falling between 30 and 49 years of age. There is a particularly large difference in the proportion of people aged 40-49, compared to those with no indication of a drug problem. A higher proportion of those with no indications of drug problems are either older or younger, with 20-29 year olds and those over 60 both significantly more likely to fall into this group.
The most recent release of justice social work statistics (data up to 2021-2022) shows that over the preceding 5 years, people aged 31-40 have been the most likely to receive a DTTO. In relation to Scotland's population, two people per 10,000 for this age range got a DTTO in 2021-22. Compared to the other age ranges, those aged 25 and under and over 40 were the least likely to receive a DTTO (both 0.6 people per 10,000 population in 2021-22).
The average age for someone receiving a CPO has been gradually increasing – from 30 to 35 over the last 10 years. Those aged over 30 accounted for just over half of orders in 2017-18 but now account for 60 per cent in 2021-22 (although again it should be noted that this applies to all CPOs, and those with a drug treatment requirement have not been separated out).
Amongst referrals into treatment services in 2021/22 from justice sources, Public Health Scotland data records that people referred to treatment by a CPO supervisor are, on average, slightly younger than those referred via a DTTO. Over 46% of CPO referral episodes in 2020 were for people under 30, but only 26% of DTTO referrals.
Insights into needs of the populations of interest
In Community Justice Scotland's Outcome Activity Across Scotland Annual Report (2023), "partners reported that service users were presenting with needs linked to alcohol and substance use, physical and mental health, wellbeing, employability, housing and more. Many individuals were experiencing more than one issue concurrently." Data on the extent of the different issues people in the justice system face remains limited, but this section provides a snapshot of available insights from justice social work and Public Health Scotland data.
Public Health Scotland data on treatment episodes in 2021/22 show that people referred for treatment are disproportionately from the lower SIMD brackets. Amongst justice referral sources, this pattern is most pronounced in CPO referrals, where 35% of people are from the 10% most deprived areas. Similarly, 28% of DTTO treatment referrals are for people from the 10% most deprived areas. This is comparable to the rate for all non-justice system related referral sources, which is also 28%. Notably, police referrals are significantly less concentrated in the most deprived areas – only 16% of police-referred treatment episodes in 2020 came from the 10% most deprived areas.
Amongst people who receive a full assessment, 55% of those with drug related problems have been imprisoned following a conviction, while only 34% of those without drug related problems have. It is important to note that this analysis does not control for other factors that may contribute to this pattern, or follow individuals longitudinally, so it is not possible to infer the extent to which this pattern is influenced by factors like severity of offending patters, and how much may be attributed to the experience of having been in custody before. However, it is relevant to consider here that the biennial Scottish Prisoners' Survey most recently found that 12% of respondents reported that they started using drugs in prison for the first time.
Additionally, in full LSCMI assessments four main areas that may be affected specifically by drug use are recorded. Amongst these, shown in Figure 27 below, the most common issues people with drug related problems face are related to law violations (93%). Medical / clinical indicators of dependency are the least frequently identified issue, but still affect over 1/3 of this group (37%). This is notable particularly in light of the relatively low proportion of people identified as warranting further assessment in the initial screening process. While these are different populations and the proportions cannot be directly compared, there may be merit in further work exploring what processes are triggered, referrals are offered, or assertive outreach occurs, for people who social work assess as showing medical / clinical indicators of dependency.
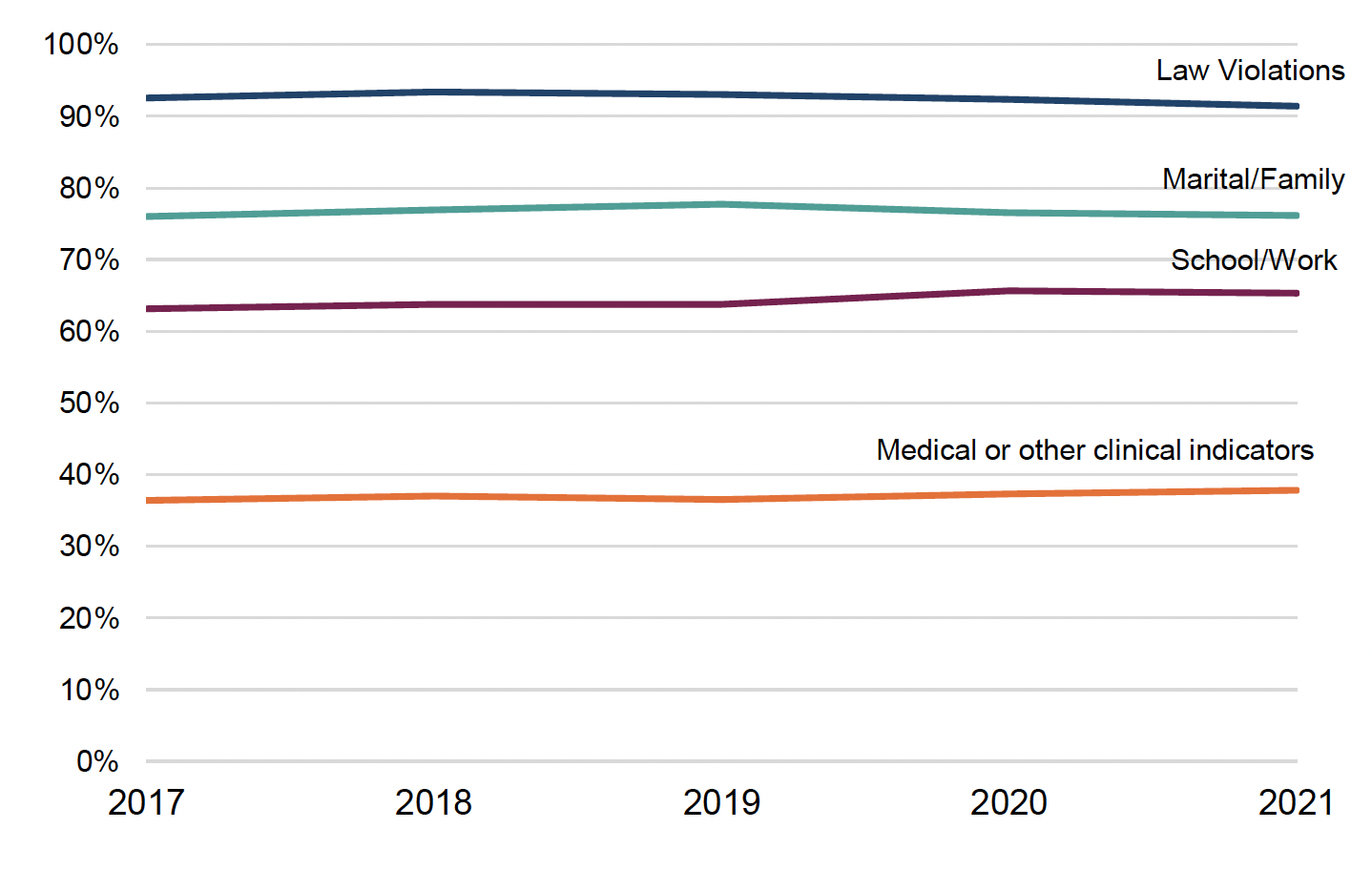
Accommodation and homelessness
Amongst those receiving detailed assessments, people with drug related problems are more likely than those without drug related problems to face housing issues. For example, as shown in Figure 28 below, between 2017 and 2021, they are more than twice as likely to be recorded as "homeless or transient" (23% compared to 10%), or to be recorded as having "accommodation problems" (42% compared to 21%). Notably, this gap has increased over time as housing issues appear to have grown more rapidly amongst those with drug related problems than those without.
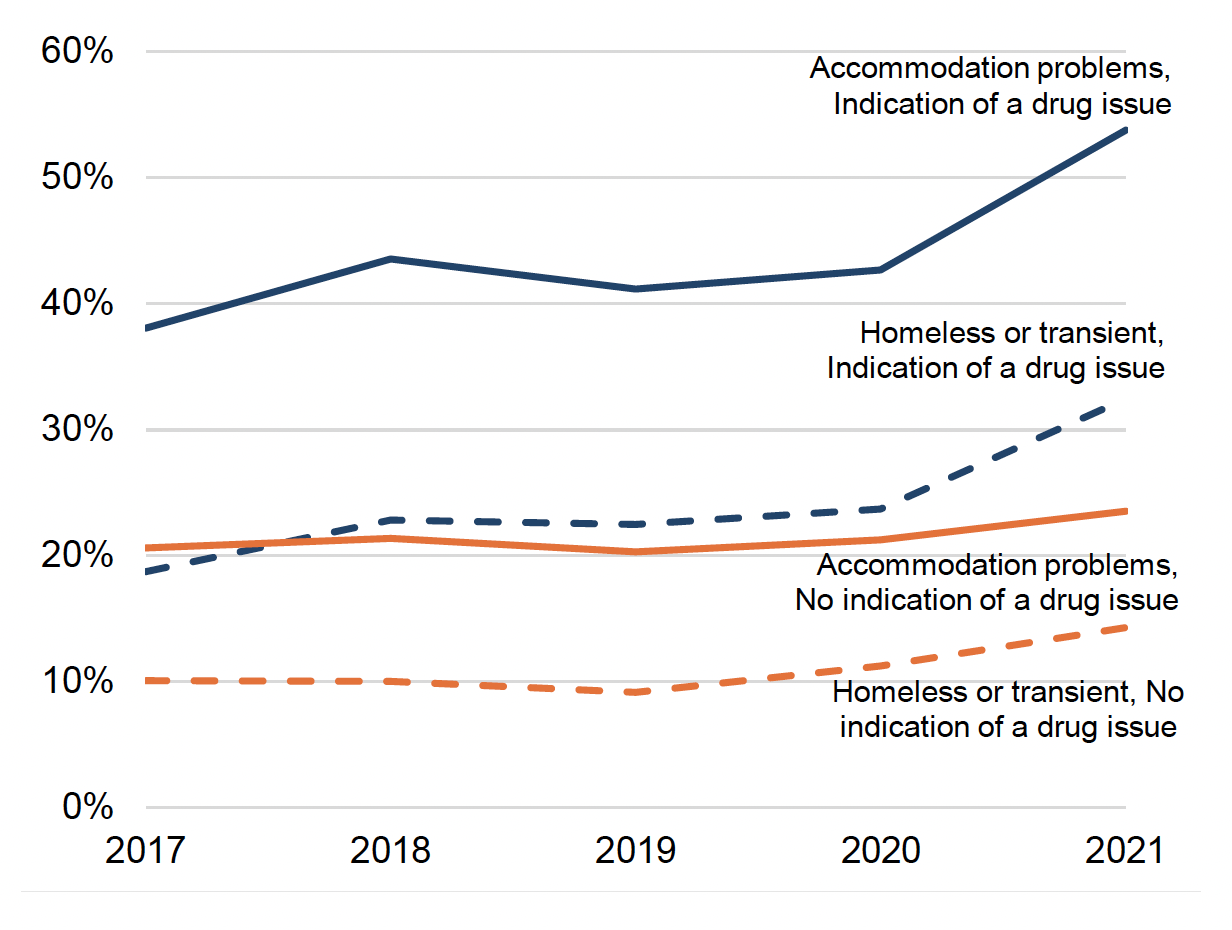
Public Health Scotland's data on referrals into drug treatment from criminal justice sources are incomplete and should be interpreted with caution, but amongst those for whom it exists, people on CPOs and DTTOs appear about equally likely to be recorded as homeless.
Mental health
Amongst people receiving detailed assessments, people with drug related problems show indications of significantly poorer mental health than those without drug related problems, as shown in Figure 29. For example, they are recorded as having:
- Higher prevalence of attempted or threatened suicide (28% compared to 20%)
- Higher prevalence of self-harm and self-mutilation (22% compared to 13%)
- More likely to show low self esteem (44% compared to 28%), being shy and withdrawn (13% compared to 11%), being interpersonally anxious (23% compared to 16%) or showing signs of emotional distress (38% compared to 26%)
This group also has a higher likelihood of being diagnosed with a serious mental illness (9% compared to 6%). However, it is notable that these rates are significantly lower than might be expected considering the much higher rates of markers that are strongly indicative of serious mental illness, such as suicidality. The fact that this population has a rate of attempted or threatened suicide of 28%, yet only 9% are diagnosed with a serious mental illness, raises questions that may warrant further consideration regarding whether this population is accessing the mental health diagnosis and treatment they need, whether information about diagnosis and treatment is adequately available to social work assessments, and whether there are adequate opportunities for referral pathways from justice social work assessment to the mental health services these people may need, regardless of the disposal imposed.
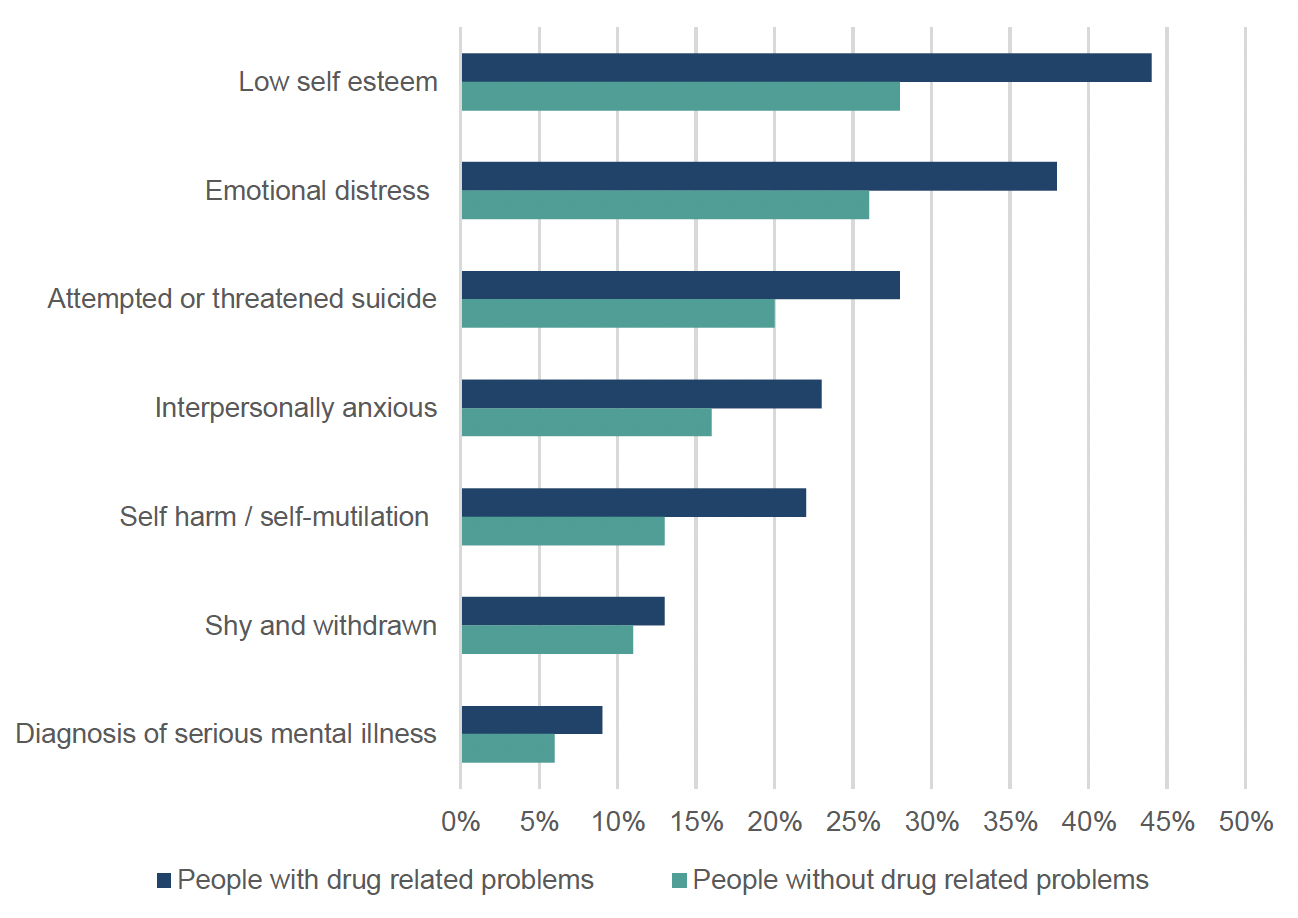
Relatedly, a survey of mental health needs amongst over 250 clients at one Scottish Justice Social Work service found that over 70% had some kind of mental health issues, and that "there is little point in asking solely about mental health without asking about drug/alcohol use and prescribed medication" (Community Justice Scotland, 2021).
Whilst mental health and trauma are different for these two sub-populations of those assessed, it should be noted that this does not mean that those with drug related problems have greater cognitive or intellectual challenges. For example, learning difficulty and communication barriers are equally prevalent for those with and without drug-related problems (both measure 4% in both groups). Cases where "low intelligence" is recorded as a responsivity issue, where the person is recorded as having a cognitive impairment, or where specific literacy difficulties are recorded, all have just one percentage point difference between those with and without drug related issues.
Co-dependency
Public Health Scotland's data on referrals into drug treatment from criminal justice sources suggests that rates of alcohol co-dependency appear to be higher amongst those receiving a CPO than a DTTO. In 2021/22, 48% of referrals via a CPO social worker were for co-dependency, but only 17% of referrals via a DTTO social worker, and only 6% of referrals via a Drug Court.
Data on alcohol co-dependency should be recorded in the LSCMI database for those receiving detailed assessments, but could not be accessed in sufficient time for this review. This may be a useful area for future analyses of this data to look at.
Drug types
While significant gaps in Public Health Scotland's data on referrals into drug treatment from criminal justice sources make analysis of detailed measures like specific substance types difficult, some general patterns can be noted from the data that are available. Across all criminal justice referral sources, opioids, stimulants, depressants and cannabinoids appear to be the most commonly used substances. While the data are not adequate to confidently differentiate trends, they suggest that stimulants and cannabinoids may be more prevalent amongst those referred via CPOs, while opioids may be more prevalent amongst those receiving DTTOs. Opioids also appear to be even more prevalent amongst those referred into treatment from custodial settings. Again, this analysis does not control for any other factors that may contribute to this pattern.
Contact
Email: socialresearch@gov.scot