Research into protests and vigils that take place outside clinics and hospitals offering abortion care
Research into protests and vigils that take place outside healthcare settings providing abortion care in Scotland.
Appendix two: Rapid evidence review on the impact of protests and vigils that take place outside healthcare facilities that offer abortion care
1. Executive Summary
This rapid evidence review was undertaken to examine what the international literature can tell us about the impact of protests or vigils outside healthcare facilities that offer abortion care. This section provides a summary of key findings.
2. Impact on women
The studies reviewed indicate that while abortion vigils and anti-abortion protests are very different types of activity, both have the potential to:
- Create, reproduce and maintain abortion stigma (Lowe and Page, 2022; Biggs, Brown and Foster, 2020; Hussein and Ferguson, 2019), which is described by Kumar (2009: 628) as being “a negative attribute ascribed to women who seek to terminate a pregnancy that marks them, internally or externally as inferior to the ideals of womanhood”.
- Exacerbate and play a part in gender-based discrimination (Lowe and Page, 2022; Lowe and Hayes, 2018; Penovic and Sifris, 2018).
- Have a negative and long-term impact on women’s emotional and psychological health (Biggs et al., 2019; Sifris, Penovic and Henckels, 2020; Nguyen et al., 2018, Seewald et al., 2019; Lowe and Page, 2019a).
- Act as a barrier to women being able to access good quality and timely sexual and reproductive healthcare (Jackson and Valentine, 2017).
- Have a disproportionately negative impact upon women who are already experiencing health inequalities and marginalization (Hussein and Ferguson, 2019; Foster et al., 2022).
3. Impact on people accessing health services for other reasons
The studies reviewed indicate that vigils and protests that take place outside healthcare facilities that offer abortion care can also:
- Create physical barriers that make it difficult for patients to access healthcare facilities by blocking pavements and entrances (Jackson and Valentine, 2017).
- Cause a range of emotional responses including anger and anxiety from passers-by, staff and patients attending healthcare facilities (O’Shea, 2023; Lentjes et al., 2020; Robinson, 2017; Ennis et al., 2023).
- Lead to the unplanned, temporary closure of general practice settings for fear of a negative impact upon patients (Fitzsimmons, 2022).
4. Motivations
The studies reviewed suggest that while motivation can be highly individualised, there are some common motivations among those who take part in vigils and protests outside healthcare facilities that offer abortion care. These include being motivated in relation to some or all of the points outlined below.
- To provide a compassionate presence for women who may feel that abortion is their only option (Ottley, 2022; Ntontis and Hopkins, 2018).
- To promote the belief that human life begins at conception, and to be part of a movement that seeks to preserve human life (Hanafin, 2022).
- To promote to others the view that motherhood is a natural and pre-destined part of being a woman, and to uphold notions of a ‘traditional family’ (De Sordo, Marre and Smietana, 2022; Ahrens, Gaweda and Kantola, 2022; Strange, 2022; Vaggione and Machado, 2020).
- To express opposition to abortion (Sifris and Penovic, 2018; Cromer and Bjork-James, 2023).
5. Introduction
There is a developing body of research evidence which indicates that anti-abortion campaigning, in its many forms, can have a negative impact on women who are seeking abortion healthcare (Lowe and Page, 2022; Sifris, Penovic and Henckles, 2020; Lowe and Hayes, 2018; Jackson and Valentine, 2017). The current review was undertaken to examine what the international evidence base can tell us about the impact of protests and vigils that take place outside healthcare settings that offer abortion care.
This review seeks to address the research questions that are outlined in the list below.
What does the international literature tell us about:
- The impact of abortion vigils and protests upon people who are accessing abortion healthcare
- The impact of vigils and protests on users of other healthcare services
- The impact of vigils and protests on people who work in healthcare settings that provide abortion healthcare
- The motivations of people who attend or organise protests or vigils that take place outside clinics and hospitals that offer abortion healthcare
The impact of restrictions and measures that have been put in place in other parts of the UK and/or other countries, for example, safe access zones or safe access zones around clinics and hospitals.
The remainder of the review is set out as follows:
- Section 2: Sets out how language and terminology is used within this review.
- Section 3: Outlines the methodology for the review.
- Section 4: Discusses what the international literature tells us about the impact that protests and vigils can have on women who are accessing abortion healthcare.
- Section 5: Considers what the international literature tells us about the impact of protests and vigils on people who are accessing healthcare facilities that provide abortions, for other general healthcare reasons.
- Section 6: Covers what the international literature tells us about the impact of protests and vigils upon people who work in abortion healthcare.
- Section 7: Explores what the international literature tells us about what motivates people to become involved in protests or vigils.
- Section 8: Discusses restrictions and measures that have been put in place in other countries and the impact of these.
- Section 9: Provides a conclusion for the review.
6. Language and terminology
In the writing of this review, we acknowledge that there is a high level of polarisation embedded within the topic. We acknowledge that there is no neutral language to describe some of the issues discussed. In conducting the review, we noted that a lot of existing research uses the term ‘pro-life’ as an umbrella term that refers to the stance taken by people who oppose abortion. The term ‘pro-life activism’ also appears within the literature, where it is used to describe both abortion vigils, campaigning, and anti-abortion protests (Mattalucci and De Zordo, 2022). We recognise that the nature of these activities is different, and so in writing the review, we have tried to be clear what type of activities each of the research papers we discuss are referring to.
In section seven of this review, we discuss the potential motivations of people who take part in activities that take place outside abortion healthcare facilities in which they express views or offer advice on abortion. We note that existing studies related
to people’s motivation for engagement in such activities tends to feature the words ‘activism’ and ‘campaigning’ which are sometimes used interchangeably. We note that some studies that are discussed within this review differentiate between protests and vigils, and others discuss both as being forms of ‘abortion activism’ (Machado, Peñas-Defago and Malca, 2022; Strange, 2022, Brown, 2019). The term ‘abortion activism’ is an umbrella term, which includes activity that can range from prayer vigils outside abortion healthcare facilities, to protests involving holding banners emblazoned with graphic words and images. We note that neither activism, nor campaigning is a perfect fit for the nature of activity that is sometimes referred to as an abortion vigil. We acknowledge that the terms are also not an ideal fit for pavement counselling, or other forms of activity where the expressed motivation of those who engage in the activity is often to offer women support and/or to adopt a prayerful presence.
We discuss these concepts in detail throughout the review, and in so doing, we acknowledge the complexity of the language currently available. We seek to adopt and use as clear and neutral concepts as we can throughout while acknowledging this is an imperfect and complex endeavour.
7. Methodology
This is a rapid evidence review, conducted in line with the 2020 Cochrane Rapid Reviews Guidance. The review represents the first stage of a research project aiming to explore the impact of protests and vigils that take place outside healthcare facilities that provide abortion care, carried out by Rocket Science on behalf of the Scottish Government. The purpose of the review was to inform the design and scope of the research being carried out in Scotland, and to identify key gaps in literature.
A rapid evidence review is defined as a process of knowledge synthesis that is more streamlined, and that enables evidence to be put forward to decision-makers in a more rapid manner than traditional systematic reviews (Thigpen, Puddy, Singer and Hall, 2012). The process of conducting the review, and the decisions that were made are presented in the sections that follow.
Topic refinement: setting the research questions
The Rocket Science research team liaised with the Scottish Government and the Research Advisory Group (RAG)[10] to agree the research questions that would inform the review. This is recognised as being of fundamental importance to the review process (Garrity et al., 2021). We met with the RAG to agree search terms, and then conducted an initial review of the evidence base.
Following this initial review, we consulted again with the RAG to further refine the research questions, ensuring that these were the questions most likely to obtain the desired results. This process is often referred to as ‘mapping’ (Popay et al., 2006). Mapping is considered to be particularly useful when seeking to assess the volume and relevance of potentially relevant literature. Given the complexity of the topic, this process was particularly helpful as it enabled detailed discussions to take place within the Rocket Science research team, and with the RAG, on the scope of the review.
Once the questions had been reviewed, and refined, the research team then began to develop a strategy for the search. This involved making decisions about what information should be extracted from individual studies, and how the information would be used to address the research questions. At this point, we further considered the research questions to identify which studies to include within the review, and the impacts that were to be assessed. The agreed focus for the review was to assess the impact of protests and vigils on:
- Women who are seeking, or accessing, abortion healthcare
- Staff who provide abortion healthcare
- People who are accessing healthcare facilities that provide abortion healthcare for other reasons.
The review also aimed to examine the potential motivations of people who engage in protests and/or vigils outside abortion healthcare facilities. It was necessary at this stage to clearly identify the types of impact that we would explore in the review. From the initial assessment of existing empirical evidence that was conducted as part of the mapping exercise, we determined that an appropriate focus would be on emotional and psychological impacts as well as impacts related to access.
Validity assessment
Once the initial focus was clear, and well defined, we engaged in a validity assessment. The validity assessment was a process of assessing the methodological quality of the identified studies. Indicators of quality included consideration of the journal in which papers were published, the methods used and the extent to which peer-review processes had been conducted. We obtained and checked the peer review process that was followed by the publishers of the included articles and excluded any that had not been through a minimum standard of a blind, anonymous peer-review process with two or more reviewers. This ensured that the included articles had been through quality assurance processes, and that ethical processes had been reviewed and checked as part of each publisher’s peer review process. We also conducted an internal process of quality checking, where we assessed, analysed, and discussed the methodologies used in each paper to ensure that the research team were satisfied that the included research papers were based on robust, rigorous and well-executed methodological approaches.
Inclusion criteria
We liaised with the RAG to clearly define the inclusion criteria, as described in the previous section, in May 2023. Following these discussions, we conducted further literature searches to assess the scope and scale of the literature for the review. Following an internal discussion, the Rocket Science research team took the decision to limit the scope of the review by excluding articles published before 2018. The rationale for this criterion was firstly pragmatic, and designed to reduce the number of studies included, but was also driven by the assumption that cultural, political, and contextual shifts were likely to be relevant to the interpretation of the results. Therefore, the most up to date research was required, to limit the potential for influencing factors that were no longer relevant due to the passing of time.
However, one researcher was responsible for going through the abstracts and titles of the excluded articles to consider this decision, and their responsibility was to flag potential research that may require to be included on the grounds of relevance and/or significance to the research questions. None of the excluded articles were deemed to be necessary for reconsideration. Where available, we prioritised systematic reviews and meta-analyses, and assessed the reference lists of each of these articles to ascertain whether any key articles may have been missed within preliminary searches. Only peer reviewed papers were included, which meant that grey literature, student papers, dissertations and news pieces were excluded. We prioritised synthesised results where these were available to streamline the evidence.
We included only English language papers, again, on pragmatic grounds. The identified studies and included papers were primarily from the UK, US, Canada, Australia and South America. This limited geographical focus was unintended and reflects where the majority of published research relevant to the topic has been undertaken since 2018. Only one Scotland specific study was identified through the review.
Despite limiting the search results to articles that were published after January 2018, several articles appeared in search results that had a published date in 2017. When we examined this anomaly further, we discovered that this occurred because
there is often a time lag between an article being accepted, and the article being published and in circumstances where this occurs at the end of a calendar year, the published date remains as the date the article was first accepted, despite it appearing publicly the following year. Several such articles were assessed for their relative value to the research questions and were included on the grounds of relevance. One article, published in 2016 was also included as the article was cited in one of the search result articles, and the topic was highly relevant to the point being discussed and explored.
Exclusion criteria
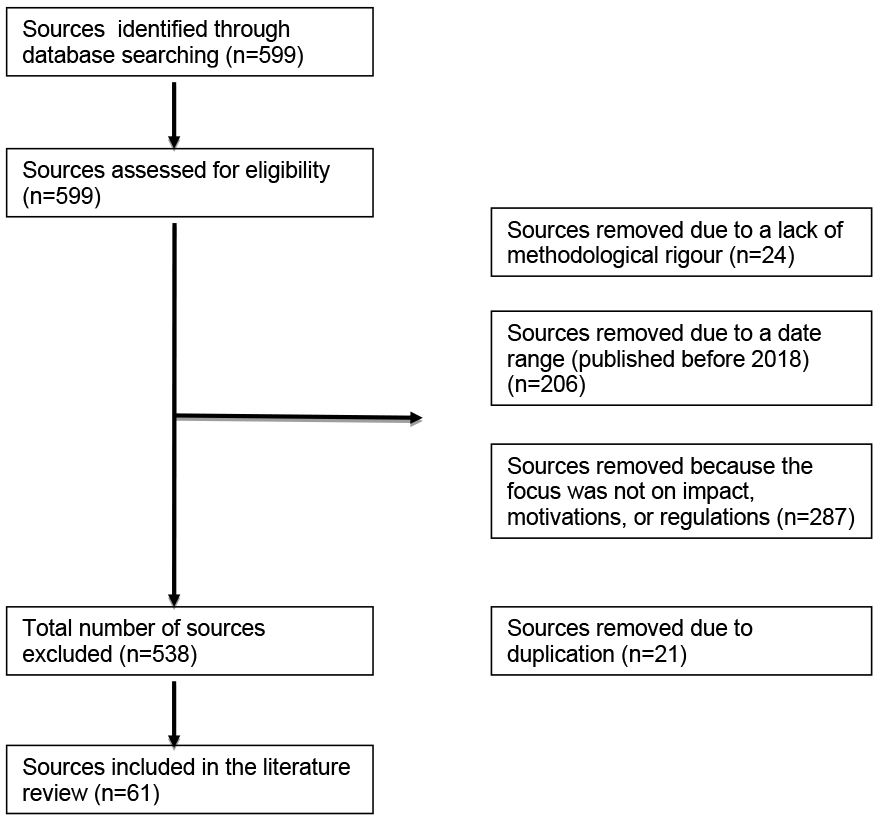
The focus of the rapid evidence review was to assess the impact of protests and vigils that take place outside clinics, hospitals or other facilities that provide abortion healthcare on women and those accessing for other reasons, and to explore the motivations of people who take part in vigils and/or protests. Due to this, studies were excluded if the focus was on more general forms of abortion protests, such as marches that take place in public settings, or those that take place outside of other types of buildings, such as parliament buildings. Research studies that were about abortion and religion, but which did not relate to protests or vigils were excluded, as these fell outside of the scope of the research. We also excluded articles that focused upon legislative changes, such as the banning or restriction of abortion that have taken place in some nations, as this was deemed to be outside of the scope of the current review. A high number of studies (287) were excluded because their focus fell outside of the scope of the current research. The vast majority of these exclusions were studies where the focus was on contexts where abortions had been banned, and many related to the construction of gender, biopolitics and the role of the nation-state. These were deemed not relevant on the basis that they were highly context-specific and focused on the political context, rather than the impact of protests or vigils that take place outside healthcare facilities that provide abortion care. Studies were deemed outside of the scope of the research if their focus was related to legal, constitutional, or political contexts rather than the impact of restrictions, or the impact of protests or vigils. Duplicates were also excluded (n=21).
Figure one, below, shows the number of articles included and excluded as per the inclusion/exclusion criteria.
Some further sources are cited within the current document. These include 13 sources that relate to specific legislation or court cases that are discussed within the primary sources described in Figure 15. A further six sources are included that relate specifically to the methodology section of this report.
Search terms and searching
The Rocket Science research team met with the Scottish Government, and the RAG and agreed search terms. These are listed below:
- Abortion protest
- Abortion vigil
- Pro-choice protest
- Pro-life protest
- Pro-life activism
- Pro-choice activism
- Abortion rights
- Abortion protest rights
- Abortion activism
- Pro-life campaigning
- Pro-choice campaigning
- Pro-life vigil
- Pro-choice vigil
- Healthcare access
- Abortion access
- Safe access zones
- Exclusion zones
- Healthcare workers
- Healthcare services
- Abortion healthcare
- Abortion clinic
Boolean search strings were developed based upon the search terms above. Database searching using the Boolean search strings were conducted within the abstract and citation database Scopus. Scopus was selected because it is a source-neutral database that contains approximately 91 million sources from over 7000 publishers, all of which have been peer-reviewed by independent subject matter experts. A single database was used following the Cochrane guidelines (Garritty et al., 2021) which suggest that using a single database, or a very small number of databases enables the principles of a systematic review to be followed within tight timeframes, thereby enabling the rapid evidence review approach.
The search was conducted using a standardised title and abstract form. Two reviewers conducted a process of dual screening of the abstracts and titles. The aim of this was to reach agreement on studies to include and exclude. This also served as a method for piloting, to ensure replicable results. Once agreement was reached, the first reviewer assessed the included studies, and categorised these into their relevance to each of the research questions. The second reviewer assessed the excluded articles to ensure agreement and resolve any conflicts. This process resulted in 5 articles being discussed, re-evaluated, and included.
Risk of bias assessment
The Cochrane risk of bias tool was used (Millward, 2021)[11]. A single reviewer completed an assessment of bias using the tool and checked all judgements and supporting statements. These were then reviewed by a second reviewer.
Synthesis
As advised within the Cochrane guidelines for rapid evidence reviews (Garrity et al., 2021), a narrative synthesis approach was used. This involved an iterative process of thematic analysis. Thematic analysis is a process of organising and summarising findings from a large body of evidence, whereby researchers identify commonly occurring concepts that exist across multiple studies (Proudfoot, 2023).
An approach combining elements of inductive and deductive analysis[12] was used. This means that the reviewers did not set out with a pre-existing hypothesis. Instead, the reviewers worked with the findings of the studies and reflected the conclusions and concepts that were evident within the studies.
The reason a combined approach was used is that the inductive approach has been criticised by those who come from a positivist school[13] of thought, on the basis that it includes some interpretivism[14], which can make it challenging for those outside of the core research team to understand how thematic categories were developed (Azungah, 2018; Fan et al., 2022). Integrating elements of inductive and deductive thematic analysis therefore ensures policy-relevant and transparent findings. The integrated combination of inductive and deductive analysis is considered particularly valuable in policy-related research due to its ability to generate relevant, clear and concise findings while also managing complexity (Pacheco-Romero et al., 2021).
The inductive themes were treated as sub-themes that were mapped onto the research questions. To maximise rigour and create the potential for reflection and further analytic discussion, a further reviewer undertook an assessment of the categorisations and decisions made. Decisions made were then assessed by a further reviewer.
8. The impact of vigils and protests on people who are accessing abortion healthcare
This section explores the international literature in relation to the impact that protests and vigils can have upon women who are accessing abortion healthcare.
Long-term negative impacts on self-identity
Hussein and Ferguson (2019) define stigma as being a social phenomenon that relates to both context and society. They suggest that stigma comprises multiple implicit processes in which a person or group comes to be identified and/or marked out as being different from a given ‘norm’. Once labelled negatively, or marked as different, the person experiences societal and/or community shame, discrimination and disapproval. Stigma has been defined and explored by many authors, and in relation to a range of circumstances and social groups, and the relevance of stigma to understanding the impact of protests and vigils outside abortion healthcare facilities is explored throughout this subsection.
Given that several studies suggest that protests and vigils that take place outside abortion healthcare facilities act as vehicles for abortion stigma, the concept of abortion stigma is central to an exploration of their impact. Biggs et al. (2020) suggest that abortion stigma can be seen as a negative attribute that is ascribed to women that serves to mark them out as being inferior because they do not subscribe to the notion that motherhood is one of the fundamental ‘ideals of womanhood’. They suggest that encountering protests or vigils outside abortion healthcare facilities can be experienced, and internalised as stigma, and can thereby have a negative impact on a woman’s felt sense of self in the longer term. Biggs et al. (2020) note that in their study, women who had experienced abortion stigma at the pre- and post-abortion stage were significantly more likely to report psychological distress many years later.
Seewald et al. (2016) also found that protests and vigils had the potential to create immediate distress for women, while also leading to increased likelihood that of experiencing long-term mental health issues due to the internalisation of abortion stigma, and the guilt and shame that could exist for some for many years. They also found that the fear of experiencing further stigma could prevent women from coming forward for medical help when they began to notice possible post-abortion complications. As such, abortion stigma can cause short-, medium- and long-term mental health impacts, and also has the potential to create barriers to accessing care.
Characteristics of vigils and/or protests
When conducting this review, we sought to understand and explore potential differences between the impact of abortion vigils and anti-abortion protests. In so doing, we noted that the term ‘abortion activism’ was commonly being used within existing literature as a broad, and all-encompassing term to encapsulate both protests and vigils. We acknowledged that due to the polarised nature of the topic, no language could be considered neutral, and so where the literature being presented differentiates between protests and vigils, we also do so. We note, however, that it is not always been possible to do so due to the use of umbrella terms, such as ‘abortion activism’ and ‘pro-life’ activity within the current evidence base. While we acknowledge the importance of language and clear terms, we also note that several studies have suggested that it is not necessarily the nature of the activity that takes place outside clinics and hospitals that provide abortion healthcare that creates impact, but rather, it is the presence of people who are questioning women’s judgements at a time and location where they are experiencing distress, and thereby vulnerable to internalising stigma (see: Lowe and Page, 2022; Sifris, Penovic and Henckels, 2020; Nguyen et al., 2018). We now discuss this in more detail.
According to Steinberg et al. (2016) protests and vigils differ in terms of the nature of the activity people participate in, and the actions they take, and yet, the emotional and psychological impact that women experience can be similar (see also Lowe and Page, 2022). This, they argue, is because both protests and vigils call into question women’s decisions around abortion, and thereby, have the potential to create stigma. Like Biggs et al. (2019) and Seewald et al. (2019), Steinberg et al. propose that abortion stigma is something that needs to be understood and taken seriously due to the potential for long-term mental health impacts and psychological distress. Steinberg et al. (2016) suggest that when women are entering a clinic or hospital seeking abortion healthcare, they are frequently experiencing heightened stress and anxiety, which makes them particularly vulnerable to internalising stigma following encounters with protesters and/or vigil participants. Abortion stigma and the psychological impact of protests and vigils is further explored by Lowe and Page (2022). In common with Steinberg et al. (2016), Lowe and Page (2022) suggest that approaching women who are already experiencing distress and attempting to impose views is a form of gendered harassment. They argue that this should be considered as a component of gendered violence. Lowe and Page (2022) define gender-based violence as a form of social control, which results in women feeling the need to be constantly aware of their personal safety when in public areas.
Short-term distress and longer-term psychological harm
Lowe and Page (2022) describe street-based anti-abortion activism as being a form of discursive violence on the basis that those questioning, offering counselling, protesting or praying feel that they have the authority or power to question women. They note that often the type of activity that occurs outside abortion healthcare facilities in the UK is prayer, and they suggest that many people who engage in prayer vigils outside abortion healthcare facilities argue that prayer causes no harm and instead offers support to women. Lowe and Page (2022) note, however, that it is important to consider who is being prayed for, and why, and what this produces in regard to power differentials, particularly the power to question women’s decisions. In their earlier research, Lowe and Page (2019a) interviewed women who had encountered this form of activity outside abortion healthcare facilities. They note that most commonly, women used words such as ‘upset, intimidated, uncomfortable, distressed and stressed’ to describe the emotional impact of encountering this type of activity when attending medical appointments related to abortion.
The concept that abortion vigils and protests can produce distress, and stigma is further explored by Foster et al.’s (2022) research, which found that women described the experience of having to walk past people who were engaged in abortion activism (whether peaceful or otherwise) as stigmatising. This aligns with the position adopted by Sifris et al. (2020), whose study also found that prayer vigils had the potential to convey judgement and create distress. As the evidence presented so far indicates, therefore, protests and vigils outside abortion healthcare facilities have the potential to create short-term distress for women, and to exacerbate the long-term psychological impact associated with internalising stigma, which can lead to negative self-perception (Lowe and Page 2022; Biggs et al. 2020; Seewald et al., 2019; Foster et al., 2022).
There is evidence that being accompanied to abortion healthcare appointments can reduce women’s likelihood of experiencing the long-term mental health impacts of stigma and shame (Nguyen et al., 2018). Often, those who accompany women to appointments are men (Arey, 2020). Arey’s (2020) ethnographic study cited several examples of situations where people who were engaged in activism would approach male companions, using concepts consistent with what Arey described as ‘toxic masculinity’. Arey defined this as being the use of patriarchal notions of gender norms, where men were criticised for their role in accompanying women when they ‘should’ be making decisions to protect their potential future families. Arey suggests that the pavements directly outside abortion clinics and hospitals are frequently becoming sites where both men and women are being asked by strangers to justify both their decisions and their gender roles.
Discrimination and disproportionate impacts on marginalised groups
Hussein and Ferguson (2019) note that stigma and discrimination are different, yet related concepts that are both relevant to understanding the impact of protests and vigils outside clinics and hospitals that provide abortion healthcare. According to their (2019) research, discrimination can be considered to have occurred when societal conditions, and the beliefs of others create situations that constrain the wellbeing of people who are seeking to access good quality care. Their research aligns with the perspective of Foster et al. (2022) who suggest that the experience and impact of abortion stigma is not equal across all social groups. Both Foster et al. (2022) and Hussein and Ferguson (2019) argue that people who are already experiencing marginalisation and inequalities are more likely to internalise abortion stigma after encountering protests or vigils outside abortion healthcare facilities. Hussein and Ferguson (2019) also note that abortion stigma can have a particularly acute negative psychological impact on women who are already experiencing processes of marginalisation, many of whom already face barriers to accessing healthcare. They note that the impact of abortion stigma can vary depending on women’s age, disability status, sexual orientation and marital status. They also note that religion and culture can also play a role in the level and scale of long-term impact on women’s identity, and suggest that women who are experiencing violence, poverty and those who have refugee status may experience stigma, and related discrimination more acutely.
Intimidation
Both Arey (2023) and Jackson and Valentine (2017) note that there are situations where women are likely to experience feelings of intimidation as a result of abortion activism. Arey’s (2023) paper, for example, suggests that the number of people present is a significant factor to understand when assessing impact, as higher numbers of people can lead to increases in feelings of intimidation. Arey (2023) suggests that in some countries, and in some localities, the pavements outside clinics and hospitals that provide abortion healthcare are becoming a place where moral, political and religious tensions play out. Likewise, Jackson and Valentine (2017) have argued that this is a space where those who are opposed to abortions often seek to engage patients in conversations about their decisions. Jackson and Valentine (2017) suggest that this type of conversation is distressing for all patients who are seeking abortion healthcare, but perhaps more acutely distressing in circumstances where the patient has no choice and is having the abortion on medical grounds. As noted earlier, however, Steinberg et al. (2016) have argued that many women are in a heightened emotional state when entering abortion healthcare facilities, and so, this type of conversation taking place outside has the potential to increase distress for all.
As the literature that we have presented so far has demonstrated, existing evidence suggests that all forms of activity that questions women’s decisions outside healthcare facilities that provide abortion care have the potential for psychological harm. In conducting this review, we sought to explore potential differences between the impact of abortion vigils and anti-abortion protests in more detail and found that there was a dearth of literature available to examine this. There is, however, some evidence to suggest that the more extreme version of abortion activism may create stronger reactions from the general public. For example, Jackson and Valentine (2017) suggest that when large groups of protesters gathered and were holding banners and posters featuring graphic wording or imagery, there tended to be more of a reaction from the general public, who tended to object to protestor presence. Jackson and Valentine (2017) noted that during this type of activity, protesters tended to physically block entryways to abortion healthcare facilities, which made physical access challenging and that, for some women, this type of experience was intimidating.
Summary
This sub-section has examined the impact of several forms of anti-abortion activism that are known to occur outside abortion healthcare facilities. It has been noted that the term ‘activism’ encompasses a broad range of activities. The literature presented in the section has highlighted that all forms of anti-abortion activism have the potential to create and exacerbate abortion stigma. The studies that have been explored throughout the section have noted that when women are approaching clinics and hospitals to access abortion healthcare, they are often experiencing higher than average levels of anxiety and distress, and so are particularly vulnerable to internalising negative messages about their decisions. Some of the studies presented here have emphasised the gendered element of abortion activism, noting that protesters and vigil attendees often deploy discursive tactics that are reliant upon a particular construction of women and men’s gender roles. This questioning of ‘natural’ and/or predestined gender roles at a time of heightened vulnerability has been described in many of the presented articles as something that can have a lasting psychological impact upon women.
9. The impact of vigils and protests on people who use other healthcare services
The hospitals and sexual health clinics that offer abortions in Scotland offer many other services to a wide range of patients. For example, in addition to abortion services, people may access Scottish sexual health clinics for sexually transmitted infection (STI) testing, contraception, HIV services and in some cases gender identity services or services supporting rape or sexual abuse victims. In this section, we present existing literature related to the impact of vigils and protests on people who are accessing healthcare facilities for general healthcare.
In their analysis of a survey sent to Irish healthcare professionals, Fitzsimons (2022) suggested that the presence of protests and vigils outside primary healthcare settings had a negative impact upon patients who were accessing both general healthcare and abortion healthcare. Their study found that in some cases, staff within GP clinics in particular had felt that it was necessary to cancel appointments for all patients on certain days because the presence of protesters was felt to be distressing for all patients, especially those attending family planning appointments. Similarly, O’Shea’s (2023) review found considerable evidence that protester presence could have negative impacts on all patients entering GP clinics and maternity hospitals. According to O’Shea (2023), encountering protesters was an issue that caused considerable distress to women who were attending appointments for medical care following miscarriage.
10. The impact of vigils and protests on people who work in healthcare settings that provide abortion healthcare
There are currently very few studies that look specifically at the impact that abortion vigils and anti-abortion protests may have upon staff who work in healthcare facilities that provide abortion care. Those that do exist tend to focus on both vigils and protests as being mechanisms that convey abortion stigma, and examine the potential impact of stigma on healthcare, and health inequalities. An exception to this is the work of Lentjes et al. (2020) who argue that in the USA, abortion clinics have become spaces of conflict where patriarchal views about the role of women are loudly shared in a ‘soundscape’ that is described as ‘sonic patriarchy’. Lentjes et al. (2020) suggest a need for greater regulation of the ‘soundscape’ around clinics and note the ‘emotional and physical labour’ that many healthcare staff are forced to endure as they try to shield their patients from having to take part in non- consensual listening to messages that have the potential to cause emotional and psychological harm. They argue that enforced listening can be conceptualised as a form of sound-based violence, which creates increased pressure for healthcare staff who seek to protect their patients.
Robinson (2017) suggests that there is a sense of low prestige that is sometimes associated with working in the field of abortion healthcare, and that this is exacerbated by abortion activism outside healthcare facilities. They note that doctors and other healthcare professionals, however, are often drawn to this field of work because they are passionate about what they do and firmly believe that women should have the right to make their own decisions concerning abortion. In an Australian study (2018), Penovic and Sifris found that the stress involved in regularly encountering protesters on their way to work had led to reduced numbers of staff choosing to work in abortion healthcare, which had led to reductions in service provision due to low staff numbers and ongoing recruitment issues.
Some studies have demonstrated that the presence of vigils and/or protests outside abortion healthcare facilities can constrain the delivery of services. For example, Ennis et al.’s (2023) Canadian study found that some staff felt concerned about advertising their services, for fear that this may attract protesters/activists to the location of the clinic/hospital. This was also found to constrain the nature of services provided by some clinics. Some sexual and reproductive health clinics reported that they had stopped providing abortion healthcare due to abortion stigma. Some of the findings of this study related to the impact of abortion stigma more broadly, while acknowledging that protests and vigils produce and exacerbate stigma. Several practitioners who took part in Ennis et al.’s (2023) study expressed that abortion stigma impacted their relationships with other professionals, which had led some to move practice, move to a new city, or change job roles because of the stigma they had experienced due to the nature of their job roles.
A recent Irish study, carried out by O’Shea (2023), examined the case for safe access zones to create an exclusion zone around abortion healthcare facilities where protests and vigils are not permitted. Their research found that several abortion healthcare practitioners had experienced harassment by ‘pro-life’ activists when entering their place of work. They noted that this experience had, in some cases, impacted practitioners’ willingness to remain in this area of work. Several practitioners who took part in their study had received letters from activists that were described as ‘unsettling’. Several described the presence of people engaged in protests or vigils outside as being ‘chilling’. Many expressed feeling unsafe working within this environment due to having experienced protesters’ conduct outside as being threatening, intimidating and harassing. O’Shea (2023) argued that exclusion zones were required for reasons of staff safety and to reduce the implications of there being issues around staff recruitment and retention.
In their Australian study, Sifris and Penovic’s (2018) examined the case for safe access zones. The abortion healthcare practitioners who took part in their study commonly reported feeling intimidated by protesters when leaving or entering their places of work. Sifris and Penovic (2018) also noted the challenges involved in frequently having to try to shield patients from hearing anti-abortion chants and yelling that had been taking place outside the abortion healthcare facility where they worked. Both O’Shea (2023) and Sifris and Penovic (2018) studies also contained reports of staff members having been followed home. Both studies noted that staff members had also experienced circumstances where protesters/activists had acquired their personal details and reached out to them with unsettling messages at other times. In both studies, it was noted that such events had led to staff changing their jobs due to the fear associated with the threats they had received, and for fear of repercussions for members of their family. It is important to note that the study by Sifris and Penovic (2018) focuses primarily upon protest-type activities, which include attendees shouting at staff and patients, the use of graphic imagery, and issuing threats against staff.
11. The motivations of people who attend and/or organise vigils or protests that take place outside clinics or hospitals that offer abortion healthcare
This section presents an overview of what the international literature says about the motivations of people who attend and/or organise protests or vigils related to abortion. Wasserman and Wasserman (2020) define motivation as being the reason or driving force behind an individual’s actions. The individualised nature of motivation, and the multiple factors that can influence it, means that it is unlikely that the studies discussed in this section will be representative of all views and all motivations. Within this section, we have sought to provide a synthesis of the concepts that appear in existing literature to explain some of the motivations of people who engage in ‘pro-life’ activism, while acknowledging that this could never adequately represent all individual views or motivations. As already noted, it is challenging to make a clear distinction in this section between abortion vigils and anti-abortion protests as these distinctions do not come through strongly in the existing literature. We have tried to be as clear as possible about the nature of activity being discussed within this section.
Compassion and support
Ottley (2022) notes that many people who engage in abortion vigils, rather than protests, are motivated by a desire to change individual women’s decisions on abortion, rather than to influence legislative or policy decisions around abortion. Penovia and Sifiris’ (2018) Australian study found that many organisers of abortion vigils described being motivated by a desire to provide a ‘loving, compassionate presence’ outside abortion healthcare facilities to offer support, and alternatives to women (Reilly, 1998). In their semi-ethnographic observational research, however, Penovia and Sifris found that although many of the organisations encouraged vigil attendees to engage in peaceful, prayerful acts, they often had very little influence over the conduct that was occurring at a ‘street level’. Penovic and Sifiris (2018) noted that those who were engaged in activities outside abortion healthcare facilities also described being motivated to provide a compassionate presence. Despite this, there were several examples within Penovic and Sifris' (2018) paper of people utilising violent rhetoric’s within the materials they were holding, and in their interactions with staff who walked by, sometimes referring to staff as murderers.
They also noted that the expression of being motivated by providing compassion and support sat diametrically opposed to behaviour on the street, which sometimes extended to taking video recordings of women who were accessing clinics and sharing these on social media, resulting in public shaming and exposure to local communities, thereby compromising women’s rights to privacy. In some such examples, those in attendance were found to be holding up graphic images with misleading information, including claims that abortions could lead to infertility, mental illness and cancer. While motivation is important to understand, these studies indicate that there may be a gap between the publicised aims of organisations and the interactions between people who take part in vigils and the general public at a street level.
Several studies suggest that those who take part in protests and vigils outside healthcare facilities that provide abortion care often state that they are motivated to offer support and/or advice to women. According to Fitzsimon’s (2022) study, many conceptualise their presence outside healthcare facilities as pavement counselling and are motivated to be present at such locations to provide advice. Fitzsimons (2022) note that many are motivated to engage with women to ensure that they do not later regret their decision. In their (2018) research, Ntontis and Hopkins (2018) suggest that many people who engage in vigils are motivated to do so out of a belief that providing advice, support or counselling may make women change their minds, which, they believe, will reduce the likelihood of women experiencing ‘post- abortion syndrome’. Ntontis and Hopkins (2018) noted that post-abortion syndrome is understood to be a form of Post-Traumatic Stress Disorder (PTSD). During the interviews they conducted with vigil attendees in Scotland, they found that many held strong beliefs about the psychological and emotional impacts, such as grief and guilt, following an abortion. Several of their research participants described being motivated by a desire to support women and reduce the likelihood of them experiencing post-abortion syndrome.
Hanafin (2022) suggests that the majority of existing literature constructs people who engage in ‘pro-life’ activism as being a monolithic and largely conservative group. They argue that this obscures the diversity of views, beliefs and motivations that exist among people who identify as being ‘pro-life’. Hanafin (2022) argues that the one motivation that appears to be consistent is a desire to be involved in ‘pro- life’ activity due to shared belief that human life begins at the point of conception. Those who take part in activism, therefore, tend to be motivated by a desire to protect and preserve human life.
Religion
Cromer and Bjork-James (2023) also found that many people who engage in both protests and vigils are motivated by a belief that human life begins at conception. For those who adopt this view, abortion ends a human life (Bridges, 2021), and it is for this reason that the term ‘pro-life’ is sometimes used by those who engage in vigils and/or protests. Lowe and Page (2019) suggest that many people who engage in ‘pro-life’ activism within the UK identify as being members of the Christian faith, with the vast majority being Roman Catholic.
According to Lowe and Page (2019a), public displays of religion tend not to be culturally endorsed within the UK and so many UK-based ‘pro-life’ organisations project a public-facing image in which they construct themselves as secular organisations. Despite this, Lowe and Page (2019a) suggest that most are motivated by views that are influenced by religion. They give an example drawn from their observational research in which they found that many of the materials used by those attending pro-life vigils outside abortion healthcare providers featured biblical quotes, and often communications would describe children as being a “gift from God”.
Motivations may not always be overtly expressed, but rather, may be evident within actions taken. Lowe and Page’s (2019b) research analysed the meaning of the religious iconography that is most commonly used within abortion vigils in the UK. They noted that images of the Virgin Mary and the Our Lady of Guadalupe are often used. According to Lowe and Page (2019b), the Our Lady of Guadalupe imagery serves as a signal to those of the Catholic faith as she was said to have appeared in Mexico in 1531 as a sign that those of the Aztec belief should end child sacrifice. The presence of this symbol is considered to be used to convey the notion that abortion is a form of child sacrifice, which thereby goes against the teachings of the Catholic faith. Lowe and Page (2019b) also note that images of the Virgin Mary are also often contained within posters and leaflets that are used by those who attend vigils. They suggest that these images are used to symbolically convey the concept of sacrificial motherhood, portraying the notion that women should sacrifice for their children. Lowe and Page (2019b) argue that these images are both used to appeal to any Catholic women who may walk past on their way to abortion healthcare facilities, and these images may be used to try to induce guilt and to influence Catholic women to change their minds on abortion.
In a further article, Lowe and Page (2019a) suggest that many people who take part in ‘pro-life’ vigils are motivated to do so because of a belief that motherhood is a woman’s role, or main purpose in life and thereby abortion undermines a woman’s ability to fulfil her ‘destiny’. They suggest that those who take part in abortion vigils use a very specific construction of womanhood as motherhood as part of their
stance against abortion. As other studies presented here have done, Lowe and Page (2019b) suggest the notion that women are ‘naturally’ inclined toward motherhood relates to religion. Lowe and Page (2019a) argue that sacrifice is central to the understanding of motherhood for many of those engaged in pro-life activities. The natural sacrifices that women should make for their children, born and unborn, are constructed as a central component of being a woman, and that women who do not make these sacrifices are “endangering her existing or future children and, more broadly, the reproduction of societies”.
Vita politics and the ‘traditional family’
Several studies suggest that a growing number of people are motivated to take part in ‘pro-life’ campaigning (in its many forms) due to beliefs about a ‘need’ to protect ‘traditional family values and the traditional concept of family structure’. For example, Brown (2019) suggests that there has been an increase in protests against abortion in some countries because of a growing number of people who are motivated by moral conservative and neoliberal forces. This has created a ‘pro-life’ activism which is a form of political resistance to what they describe as ‘sexual morality’ and a conservative focus on the notion of ‘family values’. This perspective aligns with the findings of Machado et al. (2022) who note that although there are some regional differences, there has been a surge in interest in the ‘pro-life movement’ in many countries because people are motivated to assert their views because of a strengthening political movement where conservative politics have started to come together with religious ideals related to the ‘traditional family’ and the ‘need’ to preserve it. Machado et al.’s (2022) international review concluded that for many decades, the Catholic Church had been an invisible network behind a lot of ‘pro-life’ campaigning. They note, however, that this has changed in recent years and there has been a coming together of religious and non-religious organisations who seek to motivate people to become involved in the ‘pro-life movement’.
Similarly, De Zordo, Marre and Smietana (2022) suggest that people who engage in protests or vigils may be motivated to preserve a notion of a ‘natural’ or ‘traditional’ family, featuring ascribed gender roles, where women are conceptualised as mothers, and men considered to be decision-makers and providers. Mattalucci and De Zordo (2022) refer to this concept as ‘vita politics’, and they suggest that these concepts often sit behind people’s motivation to become involved in ‘pro-life’ activities. They define vita politics as being a moral regime that seeks to maintain life by condemning abortion, while also being opposed to other forms of reproductive medicine. According to the authors the concepts associated with vita politics motivate many people who identify as being ‘pro-life’ and who take part in abortion activism. They also note that vita politics, and the beliefs associated with it prioritise the heterosexual family as being normative and extoll the belief that motherhood is the destiny of women. They suggest that the norms embedded within this concept and belief system mean that some organisations and individuals who are involved in anti-abortion campaigning are also involved in campaigns which speak out against LGBTQI+ rights (Ahrens, Gaweda and Kantola, 2022).
The conceptualisation of abortion as immoral as it appears within the literature on vita politics is intrinsically linked to a heteronormative construction of gender (Strange, 2022). There have been concerns within international literature about the growing power of governmental and non-governmental bodies who ascribe to concepts associated with vita politics (Mattalucci and De Zordo, 2022; Vaggione and Machado, 2020). A 2020 United Nations General Assembly also made the connection between religious motivations and the political sphere, suggesting that religious belief has become a seemingly legitimate reason for discriminatory policies toward women and girls. According to Vaggione and Machado (2020), the anti-abortion movement is now more transnational than ever before, and that there are similarities across nations, where the issue of abortion is often mobilised as part of discussion on gender and LGBTQI+ rights by promoting hetero-normative and patriarchal construction of the nuclear family. De Zordo, Marre and Smietana (2022) argue that declining fertility rates globally may have contributed to a growth in support for ‘pro-life’ activism from both political and non-political actors.
This section has explored what the international literature says about the motivations of people who engage in activities such as vigils and protests. The section has demonstrated that people who engage in ‘pro-life’ activism are motivated by a range of factors, including beliefs about gender roles, the construction of family, and the concept of preserving human life (Cromer and Bjork- James, 2023; Ntontis and Hopkins, 2018; Penovic and Sifris, 2018; Sifris and Penovic, 2018). The section has also demonstrated that those who take part in abortion vigils are often motivated by a desire to offer women a supportive presence (Mattaluci and De Zordo, 2022; Lowe and Page, 2019; Ntonis and Hopkins, 2018). Some studies presented here, however, have questioned this expressed motivation by demonstrating that there can be a difference between expressed motivations, and the motivations that can be discerned via a critical analysis of the behaviour and actions that some individuals engage in (Lowe and Page, 2019; Penovic and Sifris, 2018; Sifris and Penovic, 2018). The literature presented here has also noted that motivations tend to exist at an individual, rather than a group level, so while political and religious beliefs may play a part in motivation, they may tell only fragments of a fuller, and individualised story (Hanafin, 2022; Mattaluci and De Zordo, 2022). The literature presented in this section suggests that there may be a range of complex factors that motivate people to take part in pro-life activism.
12. The impact of restrictions and measures that have been put in place in other parts of the UK and/or other countries
The section explores current studies that have been undertaken to explore the impact of regulations, and the legal challenges that have been mounted in some areas.
According to Ottley (2022), the intent of implementing safe access zone legislation is to allow patients unimpeded access to abortion services and facilities and to try to prevent the psychological, emotional, and physical harm that can arise to patients and healthcare staff from vigils and protests. Foster et al. (2020) suggests that many women who have accessed abortion care have experienced fear, apprehension and anxiety about encountering protesters when approaching abortion healthcare facilities. Foster et al. (2020) argue that safe access zones would minimise distress and increase the wellbeing of those using services. Their 2020 Canadian study indicates that in areas where safe access zones have been established, women have reported that the zones help to ease feelings of harassment and stigma when accessing abortion healthcare.
Penovic and Sifris (2018) found that the enactment of a safe access zone in Australia had played a key role in helping to maintain the privacy of staff, who had previously received hate mail, threats and other forms of upsetting and invasive behaviours from those engaged in anti-abortion activism. The individuals interviewed for their research unanimously agreed that the legislation helped distance those seeking an abortion from harassment and protesting. This contributed a feeling amongst those participating in the research that the safe access zone had helped to protect them by de-personalising them, so the protesters could not associate them as individuals to their work and target them later. Penovic and Sifris (2018) also note that, from the perspectives of staff, there had been a dramatic improvement in the need for patients to be referred to clinical psychologists during their care and treatment. Several staff members suggested that this was due to patients having experienced less stigma and shame when approaching the clinics/hospitals. De Mayer’s (2020) Irish research also suggests that safe access zones have a key role to play in reducing barriers to accessing care, as well as reducing psychological impacts.
Another impact of safe access zones that is discussed in the literature relates to privacy. Several studies suggest that safe access zone legislation has helped to protect patient’s rights to privacy. Rankin’s (2020) Australian study proposed that the safe access zones that had been enacted in Australia had played a key role in protecting women’s rights to access reproductive healthcare, as well as their rights to privacy. A Canadian survey, conducted by Ennis et al. (2023) suggested that safe
access zones would make it easier to recruit and retain abortion healthcare staff because of a general feeling that staff members’ rights to privacy would be better protected. Several staff member participants in Ennis et al.’s (2023) study expressed that a newly enacted safe access zone had led staff to feel safer when entering and leaving work. Several had previously experienced breaches of privacy and had received harassing letters and emails. Those who took part felt that the safe access zone would make breaches of privacy less likely, resulting in feelings of increased personal safety.
13. Conclusion
This review has examined the international evidence base to assess the potential impact that protests and vigils can have on women who are accessing abortion healthcare, staff, and those who are accessing healthcare facilities for other reasons. It has also examined published research related to the motivations of people who take part in protests or vigils outside healthcare facilities that provide abortion care. The international literature suggests that although protests and vigils involve different types of activities, the impact of both forms of activity are similar (Arey, 2023; Lowe and Page, 2022; Sifris, Penovic and Henckles, 2020; Jackson and Valentin, 2017). This appears to be particularly the case when considering the immediate and long-term psychological impacts on women who are accessing abortion healthcare facilities where vigil and protest activities are taking place (Arey, 2020; Sifris, Penovic and Henckles, 2020; Nguyen et al., 2018). Many studies presented within this literature review suggest that all forms of activity where people publicly share views about abortion and seek to change the minds of women has the potential to exacerbate distress and produce abortion stigma (Biggs, Brown and Foster 2020; Hussein and Ferguson, 2019; UNAIDS, 2017). As has been noted throughout this review, abortion stigma has been associated with increasing the likelihood of women developing post-abortive, long-lasting mental health conditions (Seewalk et al., 2019; Steinberg et al., 2016).
The review found that within the studies that were assessed, there was evidence that protest activity also had a negative impact on those accessing services for general healthcare reasons. This included delayed and postponed appointments, and the closure of services on days when protesters were present outside.
The current review found that abortion stigma was an important concept to consider when discussing the impact of vigils and protests on people who work in healthcare settings that provide abortion healthcare. Several studies suggest that abortion stigma can affect staff as well as patients, leading to the sense that roles within the field carry less prestige than other areas of medicine. The studies presented within the review suggest that staff retention and recruitment are also negatively impacted
by abortion stigma as many are dissuaded from working within the field for fear of encountering harassment on their way to and from work.
The findings of this review indicate that the motivations of people who engage in ‘pro-life’ activities may vary significantly. While it is not possible to give a clear account of individual motivations, the review has drawn from multiple studies to give an overview of some of the factors that are known to shape people’s motivation and willingness to engage in activities that range from vigils to protests. The studies explored in section four of this report suggest that motivations for involvement in ‘pro-life’ activism, in its many forms, can be broadly defined into the themes of a desire to provide compassionate presence and support to women, a desire to express religiously motivated views, and preserving the ‘traditional family’. As section two has proposed, there is some evidence that the views, beliefs and ideals that sit beneath some of these motivators have been implicated in discriminatory policies towards women, girls and LGBTQI+ people in many countries.
The findings of this literature review, taken together, suggest that both abortion vigils and anti-abortion protests can have a significant negative impact on the mental health and wellbeing of women who are accessing abortion healthcare. The findings also suggest that protests and vigils can act as barriers to the provision of high-quality healthcare by leading to staff retention and recruitment challenges. According to the literature presented in section seven, the motivations of those who engage in ‘pro-life’ activism, regardless of the form it takes, tend to relate to the preservation of human life, as well as the protection of the ‘traditional family’ comprising traditional gender roles. Taken alongside the literature presented in section four, the reviewed literature suggests that these gender-specific impacts and motivations comprise a larger picture in which others are able to intervene in the private lives of women and attempt to influence their own assessment of the choices available to them. The review has noted that the implementation of safe access zones has led to reduced immediate distress and reduced longer-term impacts on women’s psychological and emotional wellbeing post-abortion. Safe access zones have also been shown to increase feelings of safety for staff.
Contact
Email: abortionteam@gov.scot