Inpatient census 2022: parts one and two
Results of the sixth Mental Health & Learning Disability Inpatient Census and Out of Scotland NHS Placements Census, 2022.
2. Ward Type Breakdowns
- The largest category of available beds in NHS Scotland were those in acute wards (34%)
- Length of stay varied greatly between ward types, from an average of 7 days in addiction wards to 1,564 days in a Learning Disability Unit
- Bed occupancy varied by ward type from a low of 70% in Eating Disorder wards to a high of 93% in Admission & Assessment wards
Pressures and demands vary across different ward types. Some, such as continuing care/long stay wards, may have more stable populations compared with acute wards. This section presents statistics broken down at ward level.
Overall, the bed occupancy rate for NHS Scotland was 85%, though this varied between ward types, with Eating Disorder wards having an occupancy of 70% and Admission and Assessment wards an occupancy of 93%. Addiction wards in 2019 show an occupancy rate of 102%, this can occur if a patient is “On Pass”, temporarily freeing up a bed even though that patient is still counted as an inpatient. Wards also differ in the number of available beds. One in three beds in Scotland were in an Acute ward, while one in five were in a Dementia ward.
| 2017 | 2018 | 2019 | 2022 | |||||
|---|---|---|---|---|---|---|---|---|
| Ward Type | No. Beds | Occupancy | No. Beds | Occupancy | No. Beds | Occupancy | No. Beds | Occupancy |
| Acute | 1,525 | 88% | 1,331 | 86% | 1,352 | 88% | 1132 | 87% |
| Intensive Psychiatric Care | 139 | 76% | 144 | 87% | 133 | 78% | 126 | 87% |
| Rehabilitation (non-addict) | 318 | 81% | 311 | 85% | 378 | 85% | 336 | 89% |
| Addiction Wards ¹ | 72 | 82% | 40 | 83% | 44 | 102% | 41 | 73% |
| Continuing care/long stay | 500 | 74% | 402 | 68% | 239 | 86% | 274 | 84% |
| Perinatal | 10 | 90% | 12 | 100% | 12 | 92% | 6 | 83% |
| Forensic (non-LD) | 391 | 88% | 410 | 90% | 399 | 90% | 356 | 90% |
| Forensic (LD) | 82 | 91% | 79 | 85% | 68 | 88% | 79 | 81% |
| Dementia Wards ² | 795 | 86% | 814 | 87% | 858 | 75% | 619 | 77% |
| Young People/Children ³ | 54 | 70% | 54 | 98% | 54 | 87% | 54 | 87% |
| Learning Disability | 179 | 90% | 170 | 87% | 190 | 77% | 150 | 88% |
| Eating Disorder | 22 | 95% | 22 | 55% | 22 | 82% | 10 | 70% |
| Admission & Assessment | - | - | 173 | 89% | 161 | 91% | 183 | 93% |
| Other | 118 | 83% | 113 | 76% | 12 | 92% | - | - |
| Scotland | 4,205 | 85% | 4,075 | 84% | 3,922 | 84% | 3,366 | 85% |
¹ Addiction wards are the combination of addiction rehabilitation and addiction detox wards.
² Dementia wards are the combination of dementia assessment and dementia care & treatment wards.
³ Young People/Children wards are the combination of Young people’s units and children’s units.
Ward Security Levels
Wards have different levels of security which can determine the level of unrestricted communication patients are allowed or restrict visitors and the movements of patients. The majority of patients, 1,879 (65%), in the 2022 Census were in a “General Psychiatric Ward”. A futher 20% of patients (580) were in a ward with a security level of low, medium or high. Patients in these wards likely require extra levels of attention and therefore require a higher level of staff resources. Since 2014 there has been a decrease from 74% to 65% in the proportion of patients being treated within general psychiatric wards, although there has not been a corresponding increase in the proportion in wards with extra security.
For most ward types, “General Psychiatric” is the most common security level, and for six ward types; Acute, Addiction, Continuing/Long Stay, Young People/Children, Perinatal, and Eating Disorder, this security level makes up 100% of the ward’s security level. However, some ward types have more varied security levels which likely reflects the complex nature of the cases these wards deal with. Only Forensic wards included a “High Security” level.
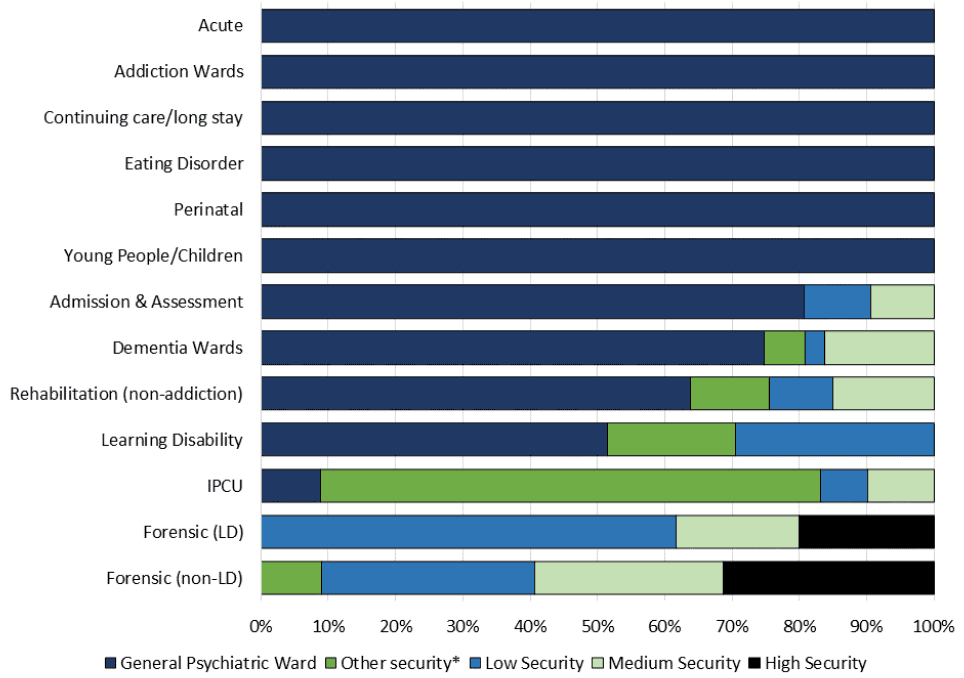
*Other security includes: Open Forensic Ward; Community Facility; Intensive Psychiatric Care Unit
** Excludes a number of cases where ward security returned 'Not applicable' - 235 in total.
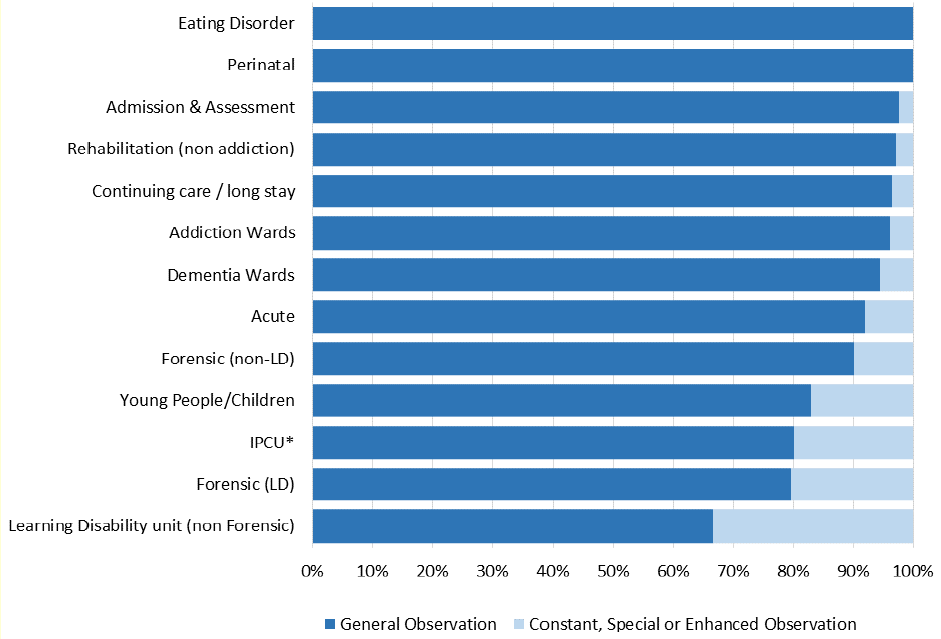
Observation level
As well as wards varying by security levels, individual patients will also receive varying levels of observation depending on their individual needs. This can impact on staff resources within a ward. Based on current guidelines the level of observation of patients at the time of the Census was recorded. The observation levels are:
- “General Observation” – Staff should have a knowledge of the patients’ general whereabouts.
- “Constant Observation” – Staff should be constantly aware of the precise whereabouts of the patient.
- “Special Observation” – Patient should be in sight and within arm’s reach of a member of staff.
- “Enhanced Care Plan For Therapeutic Engagement” – Aims to improve observation practice through therapeutic engagement with suicidal, violent or vulnerable patients to prevent them from harming themselves or others at times of high risk during their recovery.
The majority of patients, 2,497 (87%), were under general observation during the 2022 Census. Some wards are more likely than others to have patients requiring more than general observation, for example, Learning Disability wards, both Forensic and Non-Forensic, and Intensive Psychiatric Care wards.
Patients under Constant, Special or Enhanced Observation require a high level of staff resources. Of the 228 patients under one of these observation levels, 55 (24%) required 2 or more members of staff involved in their supervision. This varied greatly between different ward types. Patients under higher levels of observations in Acute wards for example almost always only required supervision by one member of staff, in comparison to those in Forensic (Non-Learning Disability) wards where 17 (53%) patients under higher levels of observation required 2 or more members of staff.
The most common reason for a patient being on a Constant, Special or Enhanced Observation level was due to being a “risk of harm to others” (31%), followed by “risk of self-harm” (25%) and “protection of vulnerable adults” (11%). It should be noted that patients can be under observation for more than one reason, for example a patient may be under observation because they are a risk to themselves and others.
Status
Patients who have been detained under the provisions of the Mental Health (Care and Treatment) (Scotland) Act of 2003 are defined as having “Formal” status. “Informal” refers to voluntary Mental Health admissions.
Just under two thirds of patients (61%) in the 2022 Census were admitted with a Formal status. This has been increasing annually since the 2016 Census (44%) and is now 17 percentage points higher. The status of a patient can change during their stay. For example, on the day of the 2022 Census, 62% of patients had a Formal status, one percent higher than on admission.
There are large differences in the lengths of stay for people detained under Formal status compared with those with Informal status. At the 2022 Census, the average (median) length of stay for a patient currently held under a Formal status was just under 8 months (232 days) compared to just over 2 months (70 days) for patients with an Informal status.
The proportion of patients being held formally varies between ward types as shown in Table 9. Forensic Wards are almost exclusively Formal patients, while Intensive Psychiatric Care Wards also tend to have a high proportion of Formal patients. The proportion of patients being held formally is generally increasing across most ward types. Acute wards have more Formal than Informal patients for the first time across all previous censuses. Addiction and Dementia Wards tend to have more Informal patients from voluntary admissions.
| Ward Type | 2016 | 2017 | 2018 | 2019 | 2022 |
|---|---|---|---|---|---|
| Acute | 37% | 40% | 41% | 44% | 53% |
| Intensive Psychiatric Care | 88% | 94% | 92% | 99% | 94% |
| Rehabilitation (non-addict) | 65% | 69% | 71% | 73% | 79% |
| Addiction Wards | 2% | 17% | 3% | 0% | 7% |
| Continuing care/long stay | 22% | 28% | 37% | 48% | 57% |
| Forensic (non-LD) | 98% | 99% | 100% | 100% | 99% |
| Forensic (LD) | 96% | 96% | 99% | 97% | 97% |
| Dementia Wards | 21% | 22% | 20% | 20% | 38% |
| Learning Disability | 66% | 75% | 80% | 85% | 90% |
| Eating Disorder | 44% | 43% | 50% | 61% | 43% |
| All | 44% | 47% | 49% | 53% | 62% |
Hospital Based Complex Clinical Care
A patient is defined as receiving HBCCC if they have care needs that cannot be met in any setting other than hospital and require long-term complex clinical care. Under the definition of HBCCC, a patient cannot be a delayed discharge. As expected, patients with HBCCC have significantly longer lengths for stay. At the 2022 Census, HBCCC patients had an average (median) length of stay of just under one year and seven months (557 days) compared to just under four months (107 days) for patients without HBCCC.
There were 409 (14%) patients receiving HBCCC occupying a mental health or learning disability inpatient bed at the 2022 Census. Most of these patients (41%) are being treated in Dementia wards. Table 10 shows that while most HBCCC patients are being treated in wards with longer lengths of stay, a very small proportion (1%) are being treated in Acute wards. This is a five percentage point decrease from the 6% who were being treated in Acute wards at the time of the 2017 census.
| Ward Type | 2017 | 2018 | 2019 | 2022 | ||||
|---|---|---|---|---|---|---|---|---|
| HBCCC patients | % of ward | HBCCC patients | % of ward | HBCCC patients | % of ward | HBCCC Patients | % of ward | |
| Acute | 86 | 6% | 37 | 3% | 65 | 5% | c | 1% |
| Rehabilitation (non-addict) | 98 | 38% | 65 | 25% | 57 | 18% | 64 | 16% |
| Continuing care/long stay | 286 | 77% | 171 | 62% | 140 | 68% | 119 | 29% |
| Forensic (non-LD) | 131 | 38% | 64 | 17% | 101 | 28% | 12 | 3% |
| Dementia Wards ¹ | 218 | 32% | 321 | 45% | 328 | 51% | 166 | 36% |
| NHS Scotland | 924 | 26% | 731 | 21% | 742 | 22% | 409 | 14% |
¹ Dementia wards are the combination of dementia assessment and dementia care & treatment wards.
c – data suppressed due to small numbers.
Delayed Discharge
Timely discharge from hospital is an important indicator of quality and is a marker for person-centred, effective, integrated and harm free care. A delayed discharge occurs when a hospital patient who is clinically ready for discharge from inpatient hospital care continues to occupy a hospital bed beyond the date they are ready for discharge.
At the 2022 Census, 293 patients were a delayed discharge. Most of these delayed discharge patients were either in Dementia wards (92 inpatients, 31%), Acute wards (55 inpatients, 19%) or Learning Disability units (Non-Forensic), (39 inpatients, 13%).
The average (median) length of delay in the 2022 Census varies greatly between different ward types. Patients in Dementia wards (34 days), Admission & Assessment (35 days) and Acute wards (60 days) tended to have shorter delays. Patients in Forensic units tend to have longer delays, with those in Forensic units (excluding learning disability) delayed for an average (median) of 378 days at the 2022 Census. However, the longest delays to discharge are observed for patients in Forensic Learning Disability units (845 days). Non-Forensic Learning Disability units delayed discharges have more than halved since the 2019 census from 760 to 350 days in 2022.
Length of Stay
The average (median) national length of stay is 136 days. However this varies significantly between ward types. The longest average (median) length of stay was 4 years and 3 months (1,564 days) for patients in Non-Forensic Learning Disability units, followed by Forensic with Learning Disability wards (1,395 days) and Forensic (non-LD) at 1,046 days. Patients in Rehabilitation (695 days) and Continuing Care/Long Stay (694) wards also had longer lengths of stay, at just under 2 years. In contrast, patients in Addiction wards had an average (median) length of stay of only one week.
| Ward Type | 2016 | 2017 | 2018 | 2019 | 2022 |
|---|---|---|---|---|---|
| Acute | 41 | 41 | 36 | 40 | 47 |
| Intensive Psychiatric Care | 65 | 57 | 54 | 57 | 66 |
| Rehabilitation (non-addict) | 770 | 840 | 537 | 582 | 695 |
| Addiction Wards | 13 | 7 | 7 | 7 | 7 |
| Continuing care/long stay | 1,463 | 1,255 | 1,170 | 1,318 | 694 |
| Forensic (non-LD) | 861 | 832 | 779 | 922 | 1,046 |
| Forensic (LD) | 1,709 | 1,371 | 1,398 | 1,451 | 1,395 |
| Dementia Wards | 205 | 206 | 204 | 269 | 165 |
| Learning Disability | 840 | 1,401 | 447 | 799 | 1,564 |
| Eating Disorder | 90 | 85 | 88 | 100 | 68 |
Contact
Email: MHIC@gov.scot