Building standards - non-domestic buildings - ventilation: research
Project to identify any evidence of where the guidance in Standard 3.14 needs to be updated in order to provide greater assurance that adequate ventilation is provided in new non-domestic buildings, which mitigates the transmission of infectious diseases such as COVID-19.
Part of
Literature Review
1. Context
1.1 The University of Strathclyde has been commissioned by the Building Standards Division (BSD) of the Scottish Government to undertake research to identify effective ventilation guidance and practice to mitigate the indoor airborne transmission of infectious diseases in new build non-domestic buildings.
1.2 Under the Building (Scotland) Act 2003[2], the Scottish Building Standards system sets minimum standards applicable where new building work is proposed. These mandatory standards, and guidance on how they may be complied with, are published in the Building Standards Technical Handbooks. The building standards system is administered by local authorities who are appointed as verifiers for their own geographical areas.
1.3 Standard 3.14, Ventilation, in Section 3, Environment, of the Building Standards Technical handbook 2022[3]: non-domestic, states: every building must be designed and constructed in such a way that ventilation is provided so that the air quality inside the building is not a threat to the building or the health of the occupants. This requirement is applied at the point construction work takes place and does not apply retrospectively to buildings constructed to lesser previous standards. As such, existing buildings require to have their ventilation systems effectively managed by their owners, operators and occupiers to ensure good levels of indoor air quality (IAQ) are maintained.
1.4 This project is intended to be a short, focussed exercise aimed at gathering evidence that will be used to assess whether application of the current ventilation guidance in the Non-Domestic Technical Handbook provides an adequate basis for simple operational practices that can be used to effectively mitigate the indoor airborne transmission of diseases such as COVID-19. Or whether there are specific further provisions that would be beneficial in enabling this.
1.5 The objective of this project is to identify any evidence of where the guidance in Standard 3.14 needs to be updated in order to provide greater assurance that adequate ventilation is provided in new non-domestic buildings, which mitigates the transmission of infectious diseases such as COVID-19.
1.6The project will identify what guidance is being used by industry and the practices being followed for new buildings and new building work. Work will also be required to establish where the guidance in Standard 3.14 does not align with current industry guidance or practice being followed.
1.7 The study will establish how ventilation currently operates as part of a COVID-19 strategy for a buildingand describe what an effectively ventilated building should achieve in terms of mitigating COVID-19 transmission. Detail will be provided on what this should look like in practice.
2. Background
2.1 People spend a substantial amount of time in non-domestic buildings engaging in various activities including working and socialising. The air quality within these buildings can have a significant effect on occupants' health and wellbeing therefore the provision of adequate ventilation to ensure good IAQ is maintained is important.
2.2 The subject of ventilation and IAQ has been further highlighted by the global COVID–19 pandemic. Transmission of the virus that causes COVID–19 can occur via direct, indirect, or close contact with infected people, including through the inhalation of the airborne respiratory droplets (>5-10μm in diameter) and aerosols (<5μm) exhaled by infected individuals.
2.3 Infected aerosols can be held in the air for long periods of time as well as being carried over short distances. Therefore, in an indoor environment which is poorly ventilated, the risk of infection through inhalation of aerosol pathogens increases.
2.4 These findings have underlined the need to establish and maintain good quality ventilation in buildings in order to mitigate the airborne transmission of infectious diseases, such as COVID - 19 and Flu, in workplaces and public buildings.
2.5 Well-designed natural ventilation has many benefits, including financial and environmental. However, it is recognised that IAQ can only be as good as the outside air quality and in some cases careful positioning of air intakes or use of filtration may be necessary. In other cases mechanical systems or systems that combine natural with mechanical (hybrid) may be the best ventilation solution for the building.
2.6 Evidence suggests that in poorly ventilated indoor spaces, airborne aerosols are a possible transmission route of COVID-19.
2.7 The World Health Organization[4] published a scientific brief on 9th July 2020 advising that SARS-CoV-2, the virus that causes COVID-19, could be spread from person-person through the airborne transmission of infected aerosols, particularly in indoor settings with poor ventilation.
2.8 Public Health England[5] updated its guidance to note the possibility of airborne transmission in poorly ventilated indoor spaces. The Centers for Disease Control in the US recognise that transmission appears to have occurred when there is inadequate ventilation. This guidance adopts a precautionary approach with the objective of ventilating spaces with outside air by as much as reasonably possible as one measure to reduce transmission risk.
2.9 The UK Government issued a paper prepared by the Environment and Modelling Group of the Scientific Advisory Group for Emergencies[6], confirming that ventilation is an important mitigation measure in controlling SARS-CoV-2 transmission.
2.10 The Scottish Government has also published COVID-19 guidance identifying ventilation as an important factor in reducing the risk of aerosol transmission of the virus indoors.
2.11 Maintaining good levels of ventilation remains a key focus in the overall strategy to mitigate the spread of COVID-19 and other airborne pathogens. This will be important particularly in the colder months of the year where adequate non-recycled air ventilation will be crucial.
2.12 It is recognised that the higher the rate of ventilation, the lower the risk of airborne transmission. However, occupant thermal comfort, energy demands and associated carbon emissions will also need to be considered as part of a building ventilation strategy. Ventilation in the workplace or in a publicly accessible building should be considered as part of any COVID-19 risk assessment plan. Building and facilities managers should engage with suitably qualified building service engineers to ensure that they are operating their ventilation system, be it natural, mechanical or a mix of both, effectively.
2.13 Regulation 6 of the Workplace (Health, Safety and Welfare) Regulations 1992[7], places a duty of care on employers, as far as is reasonably practical, to ensure the health of their employees by requiring that, 'Effective and suitable provision shall be made to ensure that every enclosed workplace is ventilated by a sufficient quantity of fresh or purified air'.
3. Industry, NGO and Governmental Guidance
3.1 Current published industry guidance does not address indoor transmission of pathogens and has traditionally focused on the removal of chemical contaminants rather than airborne transmissible pathogens. Recent guidance on how pathogens such as COVID-19 are transmitted in aerosol droplets in indoor environments highlights the need to amend all ventilation standards and guidance in order to reduce / avoid airborne pathogen transmission in indoor environments.
3.2 CIBSE[8] acknowledged in recent guidance the potential for airborne aerosol transmission of SARS-CoV-2. This guidance adopts a precautionary approach, advocating that indoor spaces should be ventilated as much as reasonably possible.
3.3 WHO[9] updated its guidance to acknowledge the possibility of airborne transmission of SARS-CoV-2.
3.4 The UK HSE[10] updated its guidance noting the possibility of airborne transmission particularly in poorly ventilated indoor spaces.
3.5 Centers for Disease Control and Prevention[11] in the US recognises that transmission appears to have occurred when there is inadequate ventilation.
3.6 SAGE-EMG[12] issued a paper confirming that ventilation is an important mitigation measure in controlling SARS-CoV-2 transmission.
3.7 HMSO[13] highlights employers have a duty of care to ensure, as far as reasonably practical, the health of their employees at work. Providing adequate ventilation is an important component of a healthy work environment and is prescribed by law in regulation 6 of the Workplace (Health, Safety and Welfare) Regulations 1992.
3.8 HSE provided updated guidance on building safety in general, and on air-conditioning and ventilation in particular. This is applicable throughout the UK and can be found at:
HSE[14], (2021). Coronavirus (COVID-19): working safely:
HSE[15], (2021). Ventilation and air conditioning during the coronavirus (COVID-19) pandemic.
3.9 BEIS[16] representing the UK government and devolved administrations, has produced guidance for employers, employees and the self-employed to help them understand how they can work safely during the pandemic. This guidance reminds employers of their legal responsibility for the safety of all those entering workplaces. To help employers decide which actions to take, they will need to carry out an appropriate COVID-19 risk assessment, just as they would for other health and safety related hazards. This risk assessment must be done in consultation with unions or workers. Undertaking this risk assessment may require advice from competent persons, such as professionally registered engineers who are chartered or incorporated engineers registered with the Engineering Council.
3.10 CIBSE[17] recently provided guidance on using ventilation as a way of diluting airborne pathogens. It is stated that: "there is good evidence that demonstrates room occupants are more at risk of catching an illness in a poorly ventilated room than in a well-ventilated room."
3.11 CIBSE[18] recently provided guidance on recirculation of air from one space to another. It is stated that: "It is preferable not to recirculate air from one space to another. However, in certain weather conditions, closing recirculation dampers in some systems may make the supply air unacceptably cold (or hot), and this may lead to a reduction in the supply rate of outside air to occupied spaces below the recommended minimum (10 l/s/person for typical offices) so that a comfortable temperature can be maintained. In these instances, there is a balance between two risks: the risk of recirculating contaminated air between multiple rooms or zones against the risk of reducing the supply of outside air and increasing the build-up of contaminants (including the virus) in a single room or zone. Recirculation should be considered only if there is no other way of maintaining an adequate provision of outside air to occupied spaces without causing undue occupant thermal discomfort or energy demand".
3.12 CIBSE[19] recently provided guidance on natural ventilation. It is stated that: "In naturally ventilated spaces, windows and vents are often the mechanism for providing outside air. In colder months, the natural forces that drive air through these openings (wind, indoor/outdoor temperature difference) are greater, so windows and vents do not need to be opened as wide. Opening only high-level vents can increase the mixing of the incoming outside air with air in the space and ensures that incoming air is warmed before it reaches the occupied zone. This makes it possible to introduce more cold outside air into the space without causing significant discomfort. It is better to open all windows or vents only a small amount to aid mixing and warming. If natural ventilation openings are the only mechanism for delivering outside air into a space, it is important that these are not completely closed when the spaces are occupied; this can result in very low ventilation rates, and increased risks of airborne viral transmission."
3.13 CIBSE[20] recently provided guidance on Nondispersive infrared (NDIR) CO2 monitors. It is stated that: "Nondispersive infrared (NDIR) CO2 monitors are useful devices that help to assess whether adequate ventilation is being provided to an occupied zone. In many spaces, a supply of outside air at 10 l/s/person is prescribed, which will result in a maximum CO2 concentration of 800-1000ppm. Indoor ventilation dilutes exhaled CO2 from occupants, and so the CO2 concentration in a space is often used to help indicate ventilation rates. CO2 concentrations that regularly exceed 1500ppm indicate poorly ventilated spaces, and attention should be given to improving the outside air provision to such spaces".
3.14 CIBSE[21] recently provided guidance on Germicidal ultraviolet (GUV) devices. It is stated that: "Germicidal ultraviolet (GUV) devices have been proposed for air cleaning. These use light on the UV-C spectrum and have been shown to inactivate coronaviruses. There is significant emerging evidence of the efficacy of UV-C sources at a wavelength of 254nm to deactivate SARS-CoV-2. There are still uncertainties about a variety of factors affecting UV performance, including dose and exposure time, and how these might depend upon the ventilation rate of outside air. In addition, consideration will need to be given to the specific room and system configuration, air flow, distribution, and humidity, as well as the safe deployment of UV for occupants and building operations personnel".
3.15 ASHRAE[22] recently provided guidance defining acceptable Indoor Air Quality as "air in which there are no known contaminants at harmful concentrations, as determined by cognizant authorities, and with which a substantial majority (80% or more) of the people exposed do not express dissatisfaction".
3.16 ASHRAE[23] recently provided guidance outlining that if airborne infectious particles are to be counted as harmful even in small concentrations, either the amount of fresh air supplied to a room needs to be dramatically increased or the ventilation strategy needs to be reconsidered to protect the occupants. Current standards already have predetermined values to meet the acceptable indoor air quality. For example, the ASHRAE standards dictate a minimum ventilation rate of 5 l/s per person or 0.9 L/s.m2 in educational facilities. For office buildings, the minimum values are 2.5 l/s per person or 0.06 l/s.m2.
3.17 ASHRAE[24] recommend, 'Mitigation of infectious aerosol dissemination should be a consideration in the design of all facilities, and in those identified as high-risk facilities the appropriate mitigation design should be incorporated. The design and construction team, including HVAC designers, should engage in an integrated design process in order to incorporate the appropriate infection control bundle in the early stages of design. Based on risk assessments, buildings and transportation vehicles should consider designs that promote cleaner airflow patterns for providing effective flow paths for airborne particulates to exit spaces to less clean zones and use appropriate air-cleaning systems.'
3.18 SAGE-EMG[25] recommend, 'In the longer term consideration of infectious disease transmission needs to be embedded into building ventilation regulations and associated statutory guidance in the same way that energy, comfort and air quality have been incorporated. Building regulations should identify performance standards and enhanced measures taken to ensure that compliance is achieved in use. As Part F: Ventilation in England is currently under review there is an opportunity to consider this further and immediately as part of the current review process. Further regulation and guidance may be required to ensure that existing buildings can meet necessary standards.' Note also the recent revisions to Part L which require CO2 sensing for all new-build offices and within 'high-risk' occupiable rooms - https://airqualitynews.com/2022/01/26/feature-what-the-updated-building-regulations-mean-for-air-quality/
3.19 REHVA[26] note that infection risk is not currently addressed in current ventilation standards as a design criterion. As such, REVHA (p.27) recommend, 'Building codes, standards, and guidelines should be revised and updated to improve preparedness for future epidemics'.
3.20 The European guideline, Indoor Air Quality and its Impact on Man[27], report N 11, expresses the dilution of pollutants as a function of the ventilation rate effectiveness which can be engineered to suit the room, occupant type, and the risk at hand.
3.21 REHVA[28] in the case of infected particles it is recommended to supply as much outside air as possible. According to REHVA, mechanical ventilation should be activated more often (24/7) when possible, with lower rates during quiet times) and at least to start ventilating before and after busy hours while the density of occupancy needs to be decreased, when possible. This will increase the distance between people and lower the pollutant emission rate. With or without mechanical ventilation, window airing should be used to boost the air exchange rate. Toilet windows on the other hand need to remain closed and mechanical extraction activated at all times to create negative pressure and prevent contaminated particles from entering other parts of the building through doors or by an unforeseen route through nearby open windows.
3.22 REHVA[29] recommend avoiding the use of centralized recirculation as typical local air filters within these systems are not effective at filtering out viral material which tends to be too small for the filter as confirmed in recent studies by REHVA (2020)
3.23 The European Centre for Disease Control (ECDC)[30] emphasise the importance of ventilation in mitigating COVID-19 transmission by concluding that appropriate ventilation of indoor spaces could be critical to help lower the risk of COVID-19 transmission in the community.
3.24 ECDC[31] provide a comparison of national COVID-19 guidelines for heating, ventilation and air-conditioning (HVAC) systems in EU/EEA countries and the UK, which are complemented by guidelines from other countries and from international professional associations.
4. Effective ventilation to mitigate the spread of airborne contaminants
Table 1. Summary of ventilation measures to mitigate the spread of airborne contaminants
| Mitigation strategies suggested |
CIBSE 2021 |
REHVA 2020 |
ASHRAE 2020 |
SAGE-EMG 2020 |
|---|---|---|---|---|
| IAQ monitoring (including CO2) in the occupied zone to ensure ventilation is operating adequately in multi-occupant spaces |
✔ |
✔ |
✔ |
|
| During an epidemic, default CO2 sensor settings should be changed so yellow/orange warning is set to 800ppm and red warning up to 1000ppm in order to trigger prompt action to achieve sufficient ventilation |
✔ |
|||
| Ventilation systems should be examined to identify areas / spaces that may be under ventilated and to verify that systems are functioning as designed |
✔ |
✔ |
||
| Carry out regular filter replacement and maintenance of mechanical ventilation systems, performed with common protective measures including respiratory protection |
✔ |
✔ |
||
| Increased use of natural ventilation provision as much as possible, without compromising occupant thermal comfort |
✔ |
✔ |
✔ |
✔ |
| Where rotary/thermal wheels are installed to recover heat, a competent engineer or technician should inspect the heat recovery equipment to ensure that leakages are under control |
✔ |
✔ |
✔ |
|
| Disable or reset sensors (e.g. change CO2 setpoint to a low value) in demand-controlled ventilation systems, in order to maintain operation at nominal speed |
✔ |
✔ |
✔ |
|
| Temporary purge ventilation / airing through intermittent window/door opening or extraction fans. When flushing spaces between occupied periods, operate systems for a time required to achieve three air changes of equivalent clean air supply. |
✔ |
✔ |
✔ |
|
| Maintain heating, cooling and possible humidification design setpoints |
✔ |
✔ |
||
| Break or fallow periods between occupants |
✔ |
|||
| Direct airflow should be diverted away from groups of individuals to avoid pathogen dispersion from infected subjects and transmission |
✔ |
|||
| Maximise outdoor air flow from mechanical systems and avoidance of recirculation of air wherever possible |
✔ |
✔ |
✔ |
✔ |
| Extended operation of mechanical ventilation systems (such as intermittent extract fans) before and after the regular period. For instance, switch ventilation on at nominal speed at least 2 hours before building opening time and set it off or to lower speed 2 hours after the building usage time. |
✔ |
✔ |
✔ |
|
| In toilets with mechanical extraction, windows should remain closed and mechanical extraction activated at all times to create negative pressure and maintain the right direction of air flows |
✔ |
✔ |
✔ |
|
| Enhanced filtration /UVC within recirculating centralized HVAC systems (only in systems designed for use with these and correctly sized and installed) |
✔ |
✔ |
✔ |
✔ |
| Installation of new passive (louvres/ air bricks) or mechanical (extract fans, HVAC) systems |
✔ |
|||
| It is recommended to flush the toilets with lids closed to minimize the release of droplets and droplet residues from air flows. Water seals must work at all times. |
✔ |
✔ |
||
| Use of local in-room HEPA or UVC air cleaning devices as a short-term mitigation measure, with due consideration to the clean air delivery rate. Only use air cleaners for which evidence is effective and safety is clear. |
✔ |
✔ |
✔ |
✔ |
4.1 A summary of industry ventilation guidance to mitigate the spread of airborne contaminants is provided in Table 1.
4.2 REHVA[32] note that to reduce the risk of airborne transmission, ventilation has to be increased and occupancy time reduced, however in existing ventilation systems it may not be possible to increase the fan speed significantly. It is recommended therefore that at the very minimum, the national ventilation regulations for outdoor air ventilation rate should be met. Where these do not exist, local 'good practice' building laws should be followed.
4.3 REHVA[33] recommend conducting a cross-infection risk assessment to improve ventilation solutions during a COVID-19 type outbreak. To support this, REHVA provide an infection risk calculator for different rooms and activities, to estimate the effect of ventilation on COVID-19 airborne transmission. The calculator is based on the standard airborne disease transmission Wells-Riley model and has been calibrated to the SARS-CoV-2 virus with correct quanta emission rates (source strength). REHVA (2020, p.4) state that, 'current technology and knowledge already allows the use of many rooms in buildings during a COVID-19 type of outbreak if ventilation meets existing standards and a risk assessment is conducted'.
4.4REHVA[34] state, 'Regarding the airflow rates, more ventilation is always better, but to dilute the aerosol concentration the total airflow rate in L/s per infected person matters. This makes large spaces ventilated according to current standards reasonably safe, but smaller rooms occupied by fewer people and with relatively low airflow rates pose a higher risk even if they are well ventilated. Limiting the number of occupants in small rooms, reducing occupancy time and applying physical distancing will in most cases keep the probability of cross-infection to a reasonable level. For future buildings and ventilation improvement, Category I ventilation rates can be recommended as these provide significant risk reduction compared to common Category II airflow rates according to ISO 17772-1:2017 and EN 16798-1:2019.'
| Category |
Total design ventilation air flow rate for the room |
Corresponding CO2 concentration above outdoors in ppm for non-adapted persons |
|
|---|---|---|---|
| L/(s per person) |
l/(s*m2) |
PPM (above outdoors) |
|
| I |
20 |
2 |
550ppm |
| II |
14 |
1.4 |
800ppm |
| III |
8 |
0.8 |
1350ppm |
| IV |
5.5 |
0.55 |
1350ppm |
4.5 SAGE-EMG[36] and CIBSE[37] recommend that multi-occupant spaces that are used regularly and are poorly ventilated (below 5 l/s/person or above 1500ppm CO2) should be identified and prioritised for improvement. Spaces where there is likely to be an enhanced aerosol generation rate (e.g. through singing, loud speech, aerobic exercise) should aim to ensure sufficient ventilation to maintain CO2 concentrations below 800ppm (typically 10-15 l/s/person). Additional mitigations are also recommended, such as face coverings for audiences and restricting the size of groups and duration of activities.
4.6 SAGE-EMG[38] highlight that engineering expertise may be required to assess ventilation effectiveness and any mitigation measures should be building specific, taking into consideration the ventilation type, nature of the building and users, activities and the length of exposure.
4.7 SAGE-EMG[39] explain that, 'Virus survival in air decreases with increasing temperature and humidity. In most environments this effect is likely to be less important than the ventilation rate, however environments with low temperature and low humidity (e.g. chilled food processing, cold stores) may pose an enhanced risk (medium confidence)'.
4.8CIBSE[40] note that, 'The risk of exposure follows a law of diminishing returns as the ventilation rate is increased. That is, the ventilation rate should be increased above the minimum statutory rates wherever possible, but this must be balanced against the need to moderate energy demand and carbon emissions and to ensure the thermal comfort of occupants.'
5. Use of Ventilation Guidance within Industry
5.1 The HSE conducted a national YouGov survey of 12,890 workplace employees (between 16th March and 6th April 2022) on COVID-19 and ventilation. The survey found that almost one third of ventilation controllers and users feel that their organisation is following government guidance 'completely' on how to reduce the risk of Covid-19 infection. More than a quarter of ventilation controllers received their guidance on ventilation from Public Health England (Figure 1). Written guidance was the most popular form across all providers (Table 3).
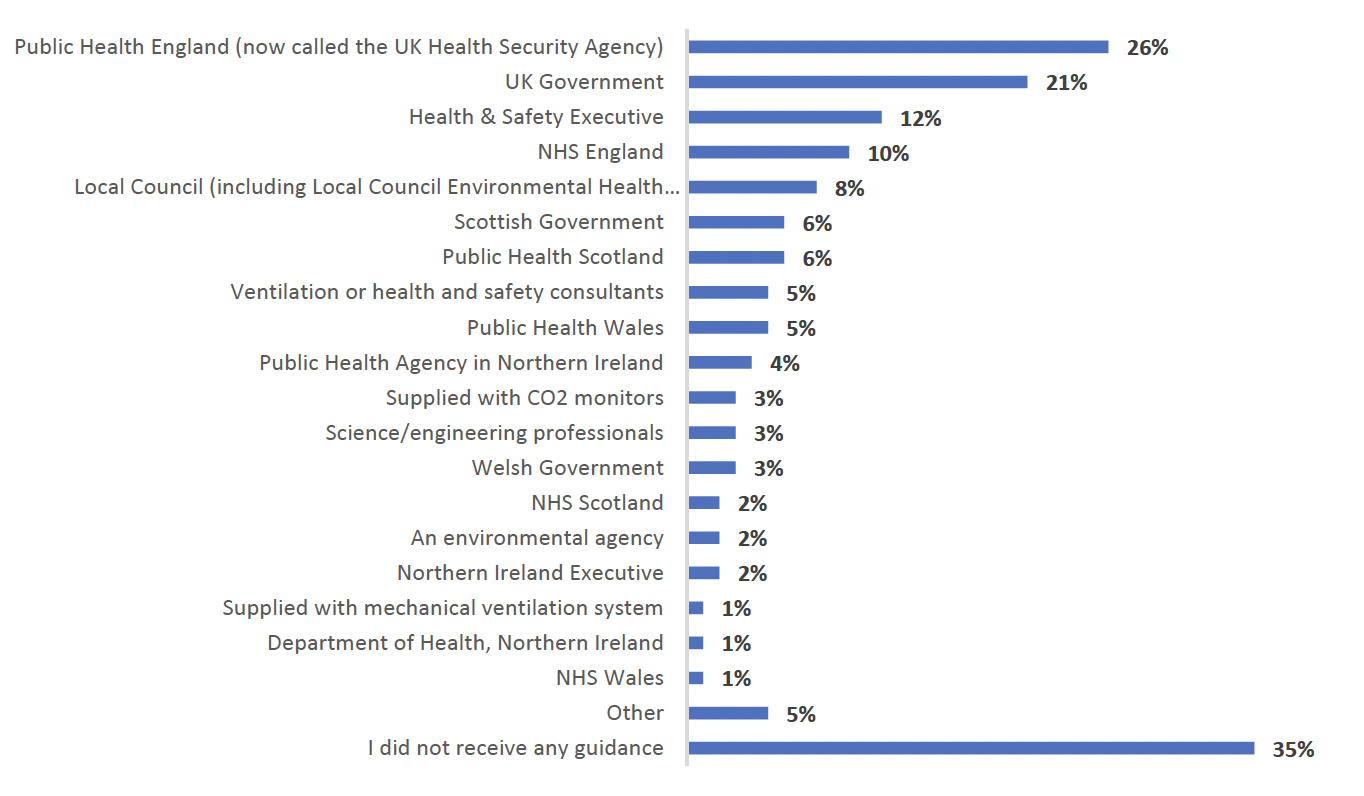
5.2 Of all guidance sources, ventilation / health and safety consultants and NHS Wales were deemed the most successful. Some suggestions were provided by respondents to make the guidance on improving ventilation more useful, as illustrated in Table 4.
| Base |
Written guidance |
Video guidance |
Verbal guidance |
I'm not sure |
|
|---|---|---|---|---|---|
| Public Health England |
390 |
68% |
13% |
8% |
11% |
| Public Health Scotland |
90 |
53% |
23% |
10% |
13% |
| Public Health Wales |
80 |
39% |
34% |
19% |
9% |
| Public Health Agency in Northern Ireland |
67 |
27% |
42% |
28% |
3% |
| Health & Safety Executive |
183 |
58% |
19% |
16% |
7% |
| UK Government |
318 |
66% |
15% |
9% |
10% |
| Scottish Government |
92 |
57% |
20% |
14% |
10% |
| Welsh Government |
39 |
46% |
28% |
13% |
13% |
| Northern Ireland Executive |
30 |
43% |
37% |
13% |
7% |
| Local Council |
123 |
60% |
18% |
17% |
5% |
| Ventilation or health and safety consultants |
71 |
35% |
20% |
39% |
6% |
| An environmental agency |
32 |
47% |
28% |
13% |
13% |
| NHS England |
157 |
64% |
18% |
6% |
12% |
| NHS Scotland |
33 |
67% |
18% |
9% |
6% |
| NHS Wales |
21 |
57% |
24% |
10% |
10% |
| Department of Health, Northern Ireland |
20 |
65% |
15% |
15% |
5% |
| Science/engineering professionals |
46 |
52% |
17% |
28% |
2% |
| Supplied with CO2 monitors |
50 |
56% |
18% |
10% |
16% |
| Supplied with mechanical ventilation system |
22 |
68% |
14% |
- |
18% |
| Other |
75 |
59% |
5% |
21% |
15% |
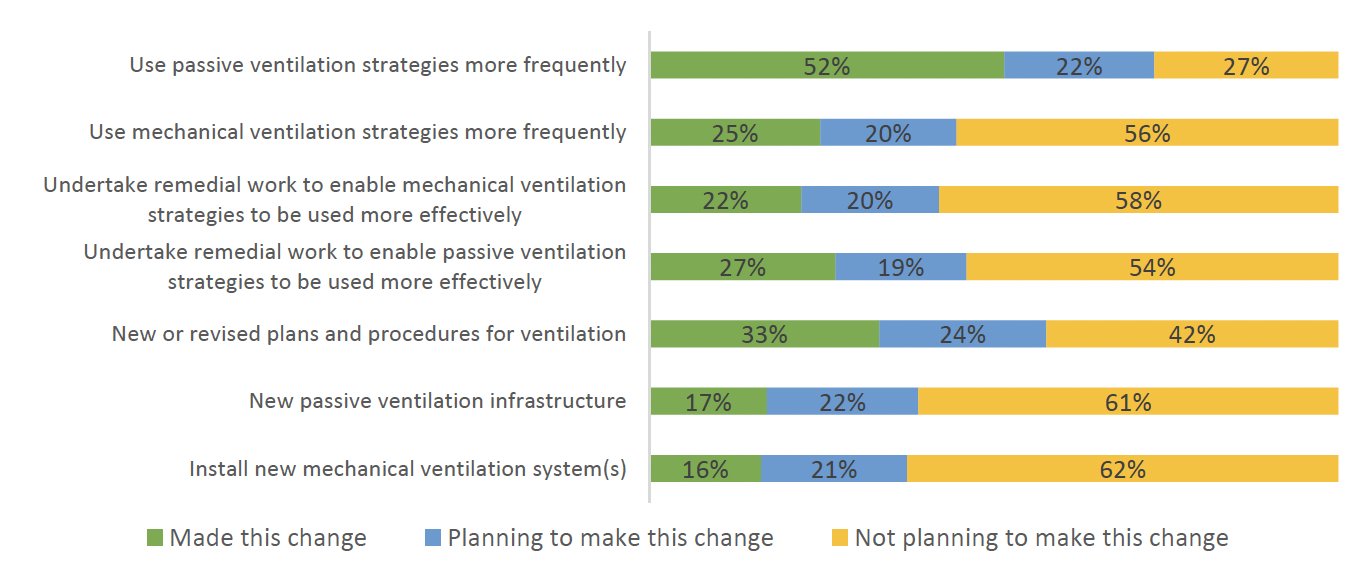
5.3 As a result of guidance, more than half of those who have control over ventilation in their workplace have used passive ventilation strategies more frequently (Figure 2).
| Base |
Make the guidance briefer |
Make the guidance simpler |
Include more detail in the guidance |
Tailor guidance to building / business |
Make guidance available in more languages |
Make guidance available in a video format |
Make guidance available in a paper format |
Make guidance available in an online format |
I'm not sure |
|
|---|---|---|---|---|---|---|---|---|---|---|
| Public Health England |
390 |
12% |
8% |
11% |
12% |
3% |
5% |
5% |
11% |
34% |
| Public Health Scotland |
90 |
11% |
16% |
10% |
19% |
4% |
11% |
2% |
6% |
21% |
| Public Health Wales |
80 |
9% |
15% |
11% |
25% |
9% |
4% |
4% |
4% |
20% |
| Public Health Agency in Northern Ireland |
67 |
10% |
9% |
15% |
19% |
10% |
18% |
10% |
3% |
4% |
| Health & Safety Executive |
183 |
5% |
13% |
12% |
19% |
5% |
5% |
7% |
7% |
27% |
| UK Government |
318 |
11% |
12% |
11% |
14% |
5% |
5% |
5% |
5% |
32% |
| Scottish Government |
92 |
13% |
12% |
9% |
12% |
9% |
10% |
5% |
8% |
23% |
| Welsh Government |
39 |
8% |
8% |
10% |
28% |
5% |
15% |
3% |
- |
23% |
| Northern Ireland Executive |
30 |
13% |
30% |
10% |
7% |
13% |
3% |
17% |
- |
7% |
| Local Council |
123 |
3% |
8% |
7% |
22% |
7% |
13% |
9% |
6% |
24% |
| Ventilation or health and safety consultants |
71 |
8% |
13% |
11% |
13% |
4% |
13% |
7% |
7% |
24% |
| An environmental agency |
32 |
13% |
16% |
9% |
19% |
6% |
16% |
3% |
6% |
13% |
| NHS England |
157 |
11% |
10% |
8% |
10% |
7% |
4% |
6% |
10% |
34% |
| NHS Scotland |
33 |
6% |
9% |
21% |
9% |
6% |
6% |
3% |
12% |
27% |
| NHS Wales |
21 |
5% |
10% |
10% |
24% |
- |
10% |
10% |
5% |
29% |
| Department of Health, Northern Ireland |
20 |
15% |
15% |
20% |
5% |
15% |
10% |
- |
15% |
5% |
| Science/engineering professionals |
46 |
11% |
11% |
13% |
11% |
2% |
7% |
11% |
15% |
20% |
| Supplied with CO2 monitors |
50 |
8% |
6% |
14% |
8% |
4% |
6% |
- |
10% |
44% |
| Supplied with mechanical ventilation system |
22 |
9% |
18% |
14% |
- |
5% |
9% |
5% |
9% |
32% |
| Other |
75 |
4% |
5% |
7% |
19% |
- |
1% |
- |
4% |
60% |
6. Contemporary research findings
6.1 Sick Building Syndrome and the spread of Viruses and other pathogens
6.11 Studies by Bodin-Danielsson et al.[41] (2014) prior to COVID-19, explained that densely packed open-plan offices were already suspected of making employees sick.
6.12 Recent Studies by Lu J. et al.[42] highlight those viruses and other pathogens are not the typical pollutants and even small and temporary exposure has been proven to lead to infections. Studies of viral infections spread through indoor spaces document clearly that mechanically induced, mixing airflow can pose a greater risk of infection spread as it pushes turbulent air deep into rooms, possibly picking up infected droplets along the way.
6.13 T. Lipinski et al.[43] recognised that COVID-19 is one of the most contagious viruses that mankind has experienced.
6.2 Airborne Transmission of Pathogens
6.21 T. Lipinski et al.[44] highlighted that the widely accepted mechanism of COVID-19 transmission is by droplet and contact methods as backed-up by the WHO, but the possible air transmission route has been broadly documented by new scientific research and the WHO is not ruling out this possibility.
6.22 T. Lipinski et al.[45] highlighted that since COVID-19 has an approximate diameter of 60140 nm, Stokes' law applies for ventilation in buildings whereby the air flow exhibits a laminar behaviour. For very small diameter particles of less than 0.1mm, the terminal velocity is almost negligible which further amplifies the fact that if COVID-19 was proven to be airborne then the virus and its potent materials could be airborne for long durations especially if enclosed environments are not ventilated adequately. These droplets are small enough to remain airborne for long periods of time (up to several hours), until they are inhaled by or land on the uninfected person. Airborne transmission is not yet widely accepted for various transmissible respiratory diseases.
6.23 Roy and Milton[46] outlined in their research into airborne transmission of communicable infection that measles and tuberculosis for example are proven to be preferentially airborne transmitted diseases. These diseases have been controlled with widely available drugs and vaccines however prior to the development of suitable vaccines and available drugs, ventilation was a key component in tackling the epidemics by quickly removing foul air from buildings using natural ventilation.
6.24 Talic and colleagues'[47] systematic review and meta-analysis assessed many public health measures for reducing COVID-19 but did not assess the effectiveness of interventions designed to reduce the presence of virus in inspired air, such as filtration, window opening, or the installation of ventilation.
6.25 Ashworth[48] highlighted in his BMJ article that the climate implications of some of these measures mentioned above could be challenging, but they are potentially important considerations in the design of buildings, workplaces, and homes for "antiviral sustainability." These factors are also potentially important modifiers for other measures like home isolation and social distancing or people density. In addition, ventilation may be a key determinant of the propensity for superspreading events, which seem to be a major determinant in the transmission of COVID-19.
6.3 The Transmission of Pathogens in poorly ventilated spaces
6.31 Fennelly[49], Morawska & Milton[50], and Guo Z.-D et al.[51] state that poorly ventilated places are considered to be high risk, and, on a precautionary principle, current advice is for buildings to be as well ventilated as possible[52].
6.32 Ventilation is a primary strategy used in hospitals and other facilities to control infectious diseases[53].
6.33 According to Chirico et al.[54], ventilation may lead to the infection spread. Ventilation systems are capable of acting as a route to transfer infectious diseases such as SARS, measles, tuberculosis, chickenpox, influenza, rhinovirus, and smallpox[55],[56]
6.34 The infectious agents of several other diseases (tuberculosis, measles, chickenpox) are recognised to be transmissible via the air-borne route, either by short-range (face-to-face, conversational) exposure or by longer-range aerosols[57]. Measles and varicella zoster (the virus causing chickenpox) can also be efficiently transmitted through direct contact during their acute phase of infection (e.g. by kissing). During a close contact situation, all transmission routes can be potentially responsible for infection.
6.35 As the most important climate factor, solar radiation was significantly correlated with the COVID-19 prevalence[58].
6.36 Temperature, simulated sunlight, and humidity are among significant factors affecting the infectious SARS-CoV-2 durability in aerosols[59],[60].
6.37 Additionally, in enclosed spaces, low humidity, air conditioning, and low UV light may cause viral aerosol to survive longer[61].
6.38 REHVA[62] states, 'Relative humidity (RH) and temperature contribute to virus viability, droplet nuclei forming, and susceptibility of occupants' mucous membranes. The transmission of some viruses in buildings can be altered by changing air temperatures and humidity levels to reduce the viability of the virus. In the case of SARS-CoV-2, this is unfortunately not an option as coronaviruses are quite resistant to environmental changes and are susceptible only to a very high relative humidity above 80% and a temperature above 30 ̊C which are not attainable and acceptable in buildings for reasons of thermal comfort and avoiding microbial growth'.
6.39 Results from this study indicated that the main transmission route for COVID-19 was person to person contact.
6.310 Gordon et al.[63] suggested in their recent studies considering traditional infection control hierarchy outlined below:
1. Elimination (to physically remove the pathogen),
2. Engineering Controls (to separate people and pathogen),
3. Administrative Controls (to instruct people what to do)
4. Personal Protective Equipment (to use masks, gowns, gloves, and other smart PPE), respectively.
6.311 Pathogens and other respiratory viruses like e.g., coronaviruses, influenza, respiratory syncytial virus, and tuberculosis transmit through the air[64],[65],[66]
6.312 SARS-CoV-2 is a common disease between humans and animals that has turned into a pandemic[67].
6.313 A number of outbreaks in confined indoor crowded spaces such as offices, churches, restaurants, ski resorts, shopping centres, worker dormitories, cruise ships and vehicles indicate that virus transmission is particularly efficient in these types of indoor environments[68].
6.314 Qian et al.[69] studied 318 COVID-19 outbreaks with three or more cases of transmission, and in all except one, the virus transmission occurred in indoor spaces.
6.315 Park et al.[70] reported an incidence of COVID-19 outbreak in an eleventh-floor office of a call centre in South Korea where 44.5 % of the occupants (94 out of 216 people) were found to be infected; however, the rate of secondary infections to the household members of the symptomatic patients was only 16.2 %
6.316 Increased rates of transmission occur not only for buildings, but also on public transportation where people are likely to be in the presence of an infected person in a crowded indoor space for relatively long periods of time and, therefore, exposed to airborne particles[71].
6.4 The use of Natural Ventilation and Stratification Ventilation Methods to reduce pathogen transmission
6.41 Ventilation is the process of providing outdoor air to a space or building by natural or mechanical means[72].
6.42 Appropriate distribution of ventilation (e.g. placement of supply and exhaust vents) ensures that adequate dilution is achieved where and when needed, avoiding the build-up of viral contamination[73],[74].
6.43 Good ventilation practices are already in place in many hospital settings, as part of everyday and emergency measures to protect against droplet and contact transmission[75],[76].
6.44 Bhagat et al.[77] summarised in a recent study of the most effective ventilation systems that despite the various mechanisms generating disturbances indoors, it is clear that in many cases stratification 'wins'.
6.45 Bhagat et al.[78] noted that a small temperature difference across a doorway or window will organise the flow so that the cool air flows through the lower part and warm air through the upper part of the opening.
6.46 Linden[79] explained that it is notoriously difficult to mix a stratified space with mixing efficiencies (the ratio of the kinetic energy needed to change the potential energy required) typically well below 20 %.
6.47 Bhagat et al.[80] further detailed that the presence of stratification emphasises the need to measure CO2 at a height where individuals are breathing, and away from sources of fresh air such as an open window, where concentrations are typically much lower than the room average, if one is to obtain an estimate for the load of potentially infectious particles. Consequently, if designed properly, displacement ventilation, which encourages vertical stratification and is designed to remove the polluted warm air near the ceiling, seems to be the most effective at reducing the exposure risk. Mixing ventilation distributes the air throughout the space and does not provide any potentially clean zones. It also has to work against the tendency of the room to stratify, while displacement ventilation takes advantage of it, and can simply and cheaply be implemented by installing extraction vents or fans at the top of the space.
6.48 Gilkeson et al.[81] explained in a study that many hospitals are naturally ventilated in ward areas, including in some rooms used for critical care. However, if the airflow passage is obstructed (e.g. by closing windows and doors), airborne pathogen concentration can sharply rise leading to an increased risk of airborne transmission and infection.
6.49 Natural ventilation concepts apply to healthcare facilities in both developed and resource-limited countries in favourable climatic conditions. The design, operation and maintenance of naturally ventilated facilities is not straight forward, and comprehensive guidance is available. For instance, WHO[82] in March, specifies that in a COVID-19 infective ward at least 160L/s/patient have to be provided if natural ventilation is used.
6.410 If ventilation is provided using window openings (aeration) or other means (fixed openings, e.g., natural ventilation), an estimation of the possible outdoor flow rate can be made using CEN Standard, EN16798-7:2017[83].
6.5 The role of Sunlight and Ultra-Violet Irradiation
6.51 In environments where it is difficult to improve ventilation, the addition of local air cleaning or disinfection devices such as germicidal ultraviolet (GUV, or UVGI-ultraviolet germicidal irradiation) may offer benefits. Under laboratory conditions GUV has been shown to be effective against a suite of microorganisms including coronaviruses[84], vaccinia[85] and Myco-bacteria[86] and even influenza[87],[88]. Several studies show that inactivation decreases with increased humidity for both bacterial and viral aerosols[89]. Darnell et al.[90] showed that SARS-CoV-1 could be inactivated by UV-C, while Bedell et al.[91] showed a UV-C decontamination device could inactivate MERS-CoV at 1.22 m, with almost a 6 log reduction in 5min. There is no data yet for SARS-CoV-2, but the data for other coronaviruses suggest it is highly likely that it is susceptible to UV-C.
6.52 Noakes et al.[92] concluded in their studies of airborne virus transmission that one application that grew dramatically during the multi-drug resistant tuberculosis outbreaks of the 1980s documented by Young and Wormser[93], is the 'upper-room' system in which lamps are placed in the upper part of the room, either on the walls or mounted on the ceiling, directing the UV light into the upper zone with louvers and limiting UV exposure in the occupied space[94]. Upper-room GUV is a good technology to consider in crowded, poorly ventilated environments where aerosol transmission could occur and where the ability to increase ventilation is limited. McLean[95] presented data showing interruption of influenza transmission in a hospital setting. It has been estimated that upper-room GUV may reduce infection risk by an amount equivalent to doubling the ventilation rate.
6.6 The use of CO2 sensing as a marker for inadequate ventilation (including natural and mechanical ventilation)
6.61 Rudnick & Milton[96] explained that it seems reasonable to consider CO2 as a marker for air that has been exhaled. Indeed, it has been shown that CO2 concentration can be linked to the probability of infection.
6.62 Bhagat et al.[97] concluded that even though CO2 is denser than air, our observations show that it is carried with the flow as would virus particles. A simple balance of a person breathing out at a concentration of 45 000 p.p.m. at a rate of 10 l min−1 and supplied with the recommended 10 l.s.p., implies that a steady concentration above the background would be 750 p.p.m. Carbon dioxide concentrations above this value, especially at the breathing level, may indicate that the ventilation is inadequate and that remedial action should be taken. The risk of infection is thought to increase with exposure time. It is also the case that CO2 levels increase over time once people begin to occupy a space. Consequently, it may be appropriate to add some exposure time as well as simply the CO2 concentration level to a warning system.
6.7 The transmission behaviour of pathogens in mechanical ventilation systems
6.71 Recent studies by Wessendorf et al.[98] closely examined the prerequisite of a unique super-spreading event in Germany during the SARS-CoV-2 pandemic, where nearly half of the participants became infected including children. The study systematically analyzed infection rate, potential individual, and environmental risk factors for infection as well as the role of the ventilation system.
6.72 Wessendorf et al.[99] highlighted that an important factor associated with infection risk was the ventilation system and the individual proximity to the ventilation outlets. Individuals close to the air-outlets that contained air with low amount of fresh air had the highest infection risk compared to those close to the air-inlets.
6.73 The results of the study by Wessendorf et al.[100] are in line with previous studies by Santarpia et al.[101], Günther[102] and Pokora et al.[103], that demonstrated SARS-CoV-2 to be able to become air-borne under certain conditions and that the ventilation system can have an influence on virus spread.
6.74 Wessendorf et al.[104] concluded that the air filters in the venue were not capable of intercepting virus particles supporting the notion outlined by Pokora et al.[105] and Nazarenko[106] on the importance of proper indoor ventilation systems.
6.75 Wessendorf et al.[107] explained that spending the break of the event outside decreased the possibility of infection underscoring the benefit of proper ventilation to lower the amount of aerosols. Due to the nature of the event, the spatial distribution of the participants was not fixed throughout the evening, and not perfectly recapitulated, so this information carries some error. However, allowing for multiple positions per person we used all available information. Assuming further error in the spatial data to be random, this might lead to a dilution of effects, i.e. true associations may remain undetected. Complementary analyses including e.g. the persons' functions during the event show consistent results, so we see no evidence suggesting bias in the findings of the study.
6.76 In environments with lower ventilation rates intended primarily to control indoor air quality (which may also include some hospital emergency, acute admissions, general ward and clinic areas), the likelihood of infected persons sharing air with susceptible occupants is high[108],[109],[110], posing an infection risk contributing to the spread of the infectious disease.
6.77 Various studies have been performed on the survival of airborne pathogens[111],[112],[113],[114],[115],[116]. The SARS-CoV-2 virus has been shown to be stable in airborne particles with a half-life of more than one hour[117], so it can potentially be inhaled by susceptible individuals causing infection and further spreading of the disease. As 'stay-at-home' lockdown measures are gradually relaxed, much of the population may return to spending increasing amounts of time in inadequately ventilated workplaces, offices, schools and other public buildings, where they may be exposed to a risk of acquiring viral infections by inhalation.
6.78 The recirculation of air is a measure for saving energy, but care must be taken, as it can transport airborne contaminants (including infectious viruses) from one space and distribute them to other spaces connected to the same system, potentially increasing the risk of air-borne infection in areas that otherwise would not have been contaminated. This concern has been noted previously in regard to the possible recirculation of biological agents during terrorist attacks that have investigated the effectiveness of eliminating recirculation (e.g. providing 100% outside air to spaces and exhausting all of it) as a counter measure following an indoor release of the agent[118]. A study modelling the risk of airborne influenza transmission in passenger cars also provided a case against air recirculation in such situations[119].
6.8 Evidence of Aerosol Transmission of COVID-19 particles in Case Study Buildings and superspreading events
6.81 The Centers for Disease Control and Prevention, Respiratory Viruses Branch, Division of Viral Diseases[120] (2021) documented several aspects during the COVID-19 pandemic to support the risk of aerosol transmission of SARS-CoV-2. First, mounting evidence for pre- and asymptomatic transmission, where the spread of droplets through coughing and sneezing cannot be a major factor, must raise questions about aerosol transmission.
6.82 Furthermore Leung et al.[121] concluded that aerosols generated by speech could theoretically contain enough SARS-CoV-2 virus particles to support transmission, and these aerosols can remain airborne for up to ten minutes. In addition, coronaviruses can be emitted in aerosols through normal breathing.
6.83 In addition to this Guo, Z.-D. et al.[122], Ong, S. W. X. et al.[123], Chia, P. Y. et al.[124] and Liu, Y. et al.[125] outlined in their recent studies that field studies in hospital wards have detected SARS-CoV-2 RNA both in vent openings and in the air. Morawska & Cao[126], Kim et al.[127] and Yu, I. T. S. et al.[128] concluded that these findings are not unexpected seeing as similar observations have been made for both SARS and Middle East Respiratory Syndrome (MERS).
6.84 Nissen et al.[129] investigated ventilation openings in one COVID‑19 ward and central ducts that expel indoor air from three COVID‑19 wards at Uppsala University Hospital, Sweden, during April and May 2020. In this study they found SARS-CoV-2 RNA in vent openings in ward rooms harbouring COVID-19 patients. Viral RNA was also detected in fluid placed in open dishes suspended below vent openings. Similar levels of viral RNA were detected in exhaust filters and open petri dishes with cell medium at least 44 to 56 m from the three investigated COVID-19 wards. Only a small fraction of each filter was analysed implying that a large number of particles emanating from COVID-19 wards can disperse to greater distances than can be explained by droplet transmission routes.
6.85 Nissen et al.[130] explained that in previous studies, the effect of ventilation has not shown any obvious impact on the risk for spread of droplet-transmitted diseases, probably since droplets are more governed by gravity as outlined in previous studies of airborne ventilation transmission by Qian & Zheng [131].
6.86 Nissen et al.[132] concluded that the ventilation system in the investigated Uppsala University Hospital has a relatively low air flow; between 1.7 and 3 total air changes per hour (ACH) for each room, depending on room volumes. Qian & Zheng[133] summarised that the recommendation for airborne infection isolation rooms is 12 ACH in most guidelines. Notably, the relative air humidity in the investigated environment was low, between 30 and 31%.
6.87 Recent Studies by Quraishi et al.[134] outlined that low air humidity has been suggested to increase the risk of airborne SARS-CoV-2 dispersal.
6.88 Studies by Bin, S. Y. et al.[135], Ong, S. W. X. et al.[136] and Correia, G.[137] outlined that detection of SARS-CoV-2 as well as other coronavirus RNA in ventilation openings has been reported before.
6.89 Nissen et al.[138] documented, in relation to their field study of the ventilation system in the investigated at Uppsala University Hospital, the detection of viral RNA in the exhaust filters over 50 m from patient care areas was unexpected.
6.810 Nissen et al.[139] explained that the placement of the petri dishes, either just below the ceiling in ward rooms or at distances around at least 50 m from patients in central vent ducts indicates that dispersal by means other than larger droplets must occur, since larger droplets are considered to precipitate by gravity within one or two meters from a source as concluded in studies by Siegel, J. et al.[140].
6.811 Burridge HC et al.[141] outlined in detail a number of environmental factors affecting the survival of SARS-CoV-2 on surfaces this is important to understand when evaluating how the virus behaves during airborne transmission through the surfaces of ventilation and air conditioning equipment such as ductwork fans and filters.
- — Temperature effects have been reported to be significant, with higher temperatures decreasing survival times as outlined in recent studies by Dietz et al.[142]. Burridge HC et al.[143] suggested that comfortable indoor temperatures should be maintained and the use of air conditioning should be minimized wherever practical with the appropriate supply of outdoor air remaining a priority.
- — Humidity has been shown to also have an effect on the virus, with drier conditions being more suitable for virus survival as detailed in a recent study by Biryukov et al.[144]. Burridge HC et al.[145] concluded that while higher humidity is preferable to reduce viral infection, there are numerous health issues related to high humidity and promotion of mould growth. Burridge HC et al. advise that in cold weather the relative humidity should be maintained at between 40 and 50%, rather than below 30%, which is typical of many indoor environments in winter aligning with guidance provided in recent studies by Dietz et al.[146].
- — Light is also demonstrated as an effective method for SARS-CoV-2 deactivation with 90% of the virus inactivated every 6.8 to 14.3min depending on the intensity of simulated natural light as explained in recent studies by Schuit M et al.[147], Burridge HC et al.[148]. Detailed studies by Bedell, Buchaklian and Perlman[149] concluded that UV-C light has been shown to deactivate other strains of coronavirus Burridge HC et al.[150] recommended that while the use of artificial light cleaning technologies is not suggested as a replacement for disinfectant cleaning practices, well-lit rooms, particularly via natural lighting is preferred based on evidence from SARS-CoV-2 and other viruses as outlined in recent studies by Dietz et al.[151] and Schuit et al.[152].
6.812 Burridge HC et al.[153] outlined that it is now well known that SARS-CoV-2 has different survival times on different surfaces, with laboratory inoculations of SARS-CoV-2 survival rates varying from 3 h for paper and tissue to up to 72 h (3 days) on hard, smooth surfaces such as plastic and stainless steel (and also on surgical masks) as outlined in recent studies by van Doremalen et al.[154] Riddell et al.[155] outlined in studies that glass and bank notes have survival times in the region of 3 days, with cloth and wood reported at 2 days.
6.813 Burridge HC et al.[156] concluded that airborne infection risk is reduced when the ventilation provision of outdoor air is maximized. Operating the existing indoor environment conditioning and controlling equipment in a manner that fixes the outdoor air supply rate to be maximal (with due consideration to the practical limits for a comfortable indoor environment), the airborne risk can be greatly reduced by lowering occupancy in a given indoor space. For example, should the ventilation plant be kept running at the same level (i.e. unchanged absolute outdoor air supply rate) and the occupancy halved (e.g. through week in—week out working) in an indoor space then the chances that infection occurs within is approximately halved. In relation to schools and offices and public buildings Burridge HC et al.[157] highlighted that consideration should be given to purging rooms between meetings, classes and events. This would require the room to be unoccupied between consecutive events during which period all possible efforts are made to increase the outdoor air supply rate (whether by opening windows, doors and ventilation systems).
6.814 Burridge HC et al.[158] summarised that the adequate ventilation of a building space should be regarded as the primary mitigating measure against the spread of airborne diseases. There is strong evidence that COVID-19 can be spread via the airborne route as outlined in studies by Hyde et al.[159]. Burridge HC et al.[160] further concludes that in temperate climates, this leads to the simple advice that all ventilation (by which we refer exclusively to the supply of outdoor, or suitably sterilized or filtered, air) systems be operated to maximize supply and ventilation openings (e.g. windows, vents, louvres, doors, etc.) be opened to the extent permitted by design.
6.815
| WHO |
10 l/s/person, 6 ACH in healthcare settings, CO2 not indicated |
|
|---|---|---|
| USA (CDC) |
800 ppm is suggested as a broad indicator |
https://www.cdc.gov/coronavirus/2019-ncov/community/ventilation.html |
| EU (ECDC) |
800-1000ppm |
|
| EU (REHVA) |
10 l/s/p or 950ppm over long time, 800ppm over shorter time |
https://www.rehva.eu/activities/covid-19-guidance/rehva-covid-19-faq |
| Germany |
1000ppm |
|
| France |
800ppm |
|
| Japan |
Japan offices below 1000ppm, schools below 1500ppm |
https://www.covid19-ai.jp/en-us/organization/aist/articles/article001 |
| Ireland |
800ppm in schools |
https://www.hpsc.ie/a-z/respiratory/coronavirus/novelcoronavirus/guidance/empl |
7. Conclusions
From the wider literature review, the following recommendations are suggested for consideration with regard to inclusion in Section 3.14 of the Standard:
7.1 Provision of Adequate Ventilation of a Building Space to mitigate the spread of airborne diseases
The adequate ventilation of a building space should be regarded as the primary mitigating measure against the spread of airborne diseases. Standard 3.14 states, 'Every building must be designed and constructed in such a way that ventilation is provided so that the air quality inside the building is not a threat to the building or the health of the occupants'. There is strong evidence that COVID-19 can be spread via the airborne route as outlined in studies by Hyde et al.[162]. Burridge HC et al.[163] further concludes that in temperate climates, this leads to the simple advice that all ventilation (by which we refer exclusively to the supply of outdoor, or suitably sterilized or filtered, air) systems be operated to maximize supply and ventilation openings (e.g. windows, vents, louvres, doors, etc.) be opened to the extent permitted by design.[164]
The WHO and REHVA (see Table 5) recommend ventilation rates of 10 l/s/p in response to COVID-19, however for future buildings Category I ventilation rates (20l/s/p or 2 l/s*m2) have been recommended as these provide significant risk reduction compared to common Category II airflow rates (14 l/s/p or 1.4 l/s*m2)[165]. In comparison, Standard 3.14.5 'Mechanical Ventilation' recommends that mechanical air supply is provided at a rate of at least 8 l/s/p for occupiable rooms, based on sedentary occupants and the absence of other requirements (such as the removal of moisture), or compliance with guidance in BS 5720:1979 or CIBSE Guide B: 2016.
7.2 Phasing out the Recirculation of extract air in Mechanical Ventilation Systems
Recommend phasing out of recirculation of air and replacement over time with heat exchanger systems which prohibit the mixing of intake and extract air to avoid airborne pathogen transmission.[166]
7.3 Installation of Carbon dioxide sensing to identify instances of poor air quality
To note. Part F in England now requires CO2 sensing in all mechanically ventilated buildings[167] (Table 6). Linked with 7.1 above, there is a growing awareness of the need to combine fresh air per person allowances and CO2 build up, pointing the way to more flexibility in how fresh air can be provided to allow management of varying occupancy patterns – see 7.5 below. CO2 sensing is an effective proxy for ventilation and/or occupancy and is equally applicable to both mechanically ventilated and naturally ventilated buildings. To limit airborne pathogen transmission, CO2 sensing is recommended for both naturally ventilated and mechanically ventilated situations to detect instances of poor ventilation and/or high occupancy.[168]
| Notable changes in part F (Ventilation) of Building Regulations 2021 |
Notes |
|---|---|
| Proposed increase in mechanical ventilation rates for occupiable rooms in offices not adopted |
Requirement is for outdoor air to be supplied at the greater of 10 l/s/p or 1 l/s/m² floor area |
| Minimising the ingress of external pollutants through proper siting of vents |
Ventilation intakes should be located away from the direct impact of the sources of local pollution |
| Requirement to monitor indoor air quality (IAQ) in all new build offices and 'high risk' occupiable rooms |
Small spaces up to 125m³ vol or 50m² area, and large spaces over 800m³ / 320m² exempt |
| Performance based ventilation strategies can now be assessed against individual volatile organic compounds (VOCs), based on data from Public Health England |
This may prove to be more complex than testing against a total volatile organic compound (TVOC) limit |
| Ventilation systems should be capable of operating in a way that prevents the recirculation of air unless adequate filtering or disinfection systems are used |
Where recirculation is unavoidable, suitable systems include those that incorporate UV-C germicidal irradiation or HEPA filtration within the recirculated air stream. HEPA filters will need larger plant and ductwork sizes which can cause significant issues for retrofit projects |
7.4 Maintenance
Guidance to standard 3.14 states, 'A mechanical ventilation or air conditioning system should be designed, installed and commissioned to perform in a way that is not be detrimental to the health of the occupants of a building and when necessary should be easily accessible for regular maintenance.'
Updated 2022 guidance 3.14.10 (p.263-264) on commissioning and written information states, 'Correct use and maintenance of the ventilation systems will assist in delivering the designed ventilation to the dwelling whilst minimising energy use and environmental problems such as noise and thermal discomfort.' To assist with this, the guidance provides a list of information that should be provided to building occupants, including instructions of how and when maintenance should be carried out.
The Workplace (Health, Safety and Welfare) Regulations 1992 (Regulation 5) states that mechanical ventilation systems should be regularly cleaned, tested and maintained. The requirement of a building ventilation maintenance plan at design stage therefore would help support the regular inspection, cleaning and maintenance of ventilation systems in practice.
7.5 Occupancy levels
Currently air change rates are often building capacity or average room capacity based. Standard 3.14 Non-domestic provides a range of options for determining ventilation supply rates, with an occupancy-based requirement of 8 l/s/p for occupiable rooms with sedentary occupants (in the absence of other requirements such as the removal of moisture). Consideration should be given to occupancy limits based on capability of ventilation systems to supply 10 l/s/person in a room – setting room capacity levels based on this.
Moreover, an increase in the required mechanical ventilation rates from 8 l/s/p to 10 l/s/p is suggested for occupied rooms in Standard 3.14, in addition to the need for greater clarity in the definition of supply rates.
7.6 Air cleaning equipment
Recent research[170] demonstrates that air cleaners incorporated at system level may be beneficial at dealing with elimination of viral transmission, they do not provide fresh air and therefore do not override the need to eliminate recirculation of air. In this context they could be considered as a retrofit option alongside heat recovery.
In-room systems are of limited localised benefit – but on the same basis as the above and not as a substitute for elimination of recirculated air.
Research remains inconclusive regarding the use of limited recirculation plus air cleaning as an interim measure. This would need further research and would ultimately depend greatly on the quality of the air cleaning equipment.
Contact
Email: buildingstandards@gov.scot