General Practice Access Short Life Working Group: access principles
High level core access principles to support and enhance people’s experience of accessing ‘The Right Care, Right Time, Right Place’.
3. Introduction and Background
Even before the Covid 19 pandemic, access to General Practice has been a longstanding challenge for the public across Scotland. Over many years, there have been a number of national attempts at improving this with initiatives like the RCGP Practice Accreditation Scheme, the Primary Care Access Collaborative, Productive General Practice, and the inclusion of access indicators in the Quality & Outcomes Framework (QOF). More recently there has been the work of Healthcare Improvement Scotland (HIS) with the development of the Practice Administrative Staff Collaborative (PASC) to support the introduction of Care Navigation[2] and Workflow Optimisation[3] toolkits and the more recent Primary Care Access Programme[4] (PCAP).
We also recognise that the availability of good medical care can vary inversely with the need for it in the population served. This is known as the Inverse Care Law[5] and was first described in 1971. Difficulties in access in more socio-economically deprived areas are known to be driven by a number of factors: higher levels of need, lower levels of workforce, and higher consultation rates. Any proposed solutions to improve access to primary healthcare must consider these factors (ref: The Inverse Care Law - The Lancet. See also this Editorial DOI publication regarding Inverse Care Law[6]).
Prior to the pandemic, the way people accessed General Practice was already changing in some areas with the introduction of telephone first approaches (sometimes called telephone triage), video consultations (usually known as Near Me in Scotland), Digital Asynchronous Consulting systems (DACs) such as eConsult® and AskMYGP® with online appointment booking and online reviews of conditions using platforms such as MedLink®. These developments varied across the country with many practices continuing with traditional ways of providing care with most appointments made by telephone and consultations provided face to face.
At the beginning of the pandemic, National Infection Prevention Control measures, including screening healthcare requests over the telephone before attending a practice, were introduced. While General Practice remained open, these changes made General Practice more difficult to access at times and created a misperception that General Practice was closed to the public and that services were not operating. This misperception has endured in some areas, even for General Practices where access has diversified and improved and these more stringent Infection Prevention Control measures have long since eased.
The way care is provided by General Practice has also changed with the introduction of the Primary Care Improvement Fund established in 2018 resourcing a large expansion of the wider MDT(Advanced Nurse Practitioners, Pharmacists, Physiotherapists, Mental Health Workers, Community Link Workers etc.) in addition to the traditional practice team of General Practitioners (GPs), General Practice Nurses and Health Care Support Workers. This has meant that services may be notably different compared with five years ago. There is now an increased range of how, and where, people can access care, but these changes are not always well understood by the public, nor are they always easy to explain.
These developments have meant that the need for practice administration staff, such as Receptionists, to support people to find the most appropriate service or member of the team to meet their needs has greatly increased. These new roles are now widespread and are sometimes known as signposting or Care Navigation. These roles are not clinical decision making roles but support the clinicians to prioritise the care they provide, particularly when there is limited capacity.
Some practices have, in addition to Care Navigation, introduced triage systems to manage the daily demand to prioritise those who are most in need, particularly where there is limited clinical capacity. Triage is defined in the OED as[7] :
‘To perform a preliminary assessment of (a patient) in order to determine the nature and degree of urgency of treatment required.’
Triage is a clinical role which should normally be conducted by a doctor or other clinician such as an Advanced Nurse Practitioner. Although the information gathered by administrative staff (receptionists), as mentioned above, supports the clinician to carry out the initial triage process before speaking to or seeing the person. Some practices call this ‘telephone triage’ or have a telephone consultation first system. However, whilst remaining useful for ‘on the day care’, for routine (non-urgent) care this is reducing with more practices re-introducing systems where people can decide, in discussion with the receptionist/ care navigator, if they wish a face to face or telephone consultation. Every General Practice has a different appointment system depending on their population’s needs and available clinical capacity within the practice.
The changes in how General Practice provides care, at a time when both demand for general practice services is understood to be increasing and capacity is constrained (for a number of reasons), has meant that people’s experience of accessing care varies depending on the arrangements in their general practice. There are many examples of people receiving good, high quality, person-centred care. However, this may not be the case everywhere, especially in practices with capacity issues.
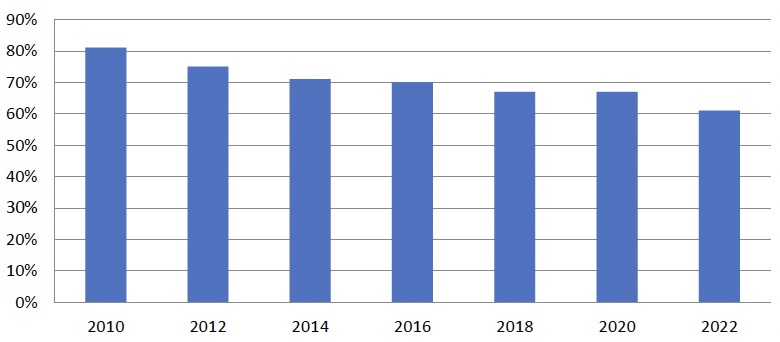
The Scottish Health and Care Experience Survey[8] (HACE) is run every two years and asks people across Scotland their experiences of accessing and using their General Practice and local Out of Hours services. It provides a national and local picture of the experiences of health and care services from the perspective of those using them. The last survey was carried out in November 2021 with the results for each General Practice, GP Cluster, Health and Social Care Partnership (HSCP) and Health Board[9] published in Spring 2022. Against a backdrop of increasing activity against the number of GPs, overall positivity in arrangements to see a GP in Scotland is steadily decreasing.
Health and Care Experience Survey (available on the Scottish Government Website[10])
General Practice in Scotland
At the time of writing there are approximately 900 General Practices across Scotland (See Public Health Scotland data[11]). There are three main types of General Practice in Scotland. Across each type of contractual arrangement, access can have similar challenges, and successes.
General Medical Services (GMS) contract (17J): these General Practices have a standard, nationally negotiated contract[12] and are normally run by GP partners (although there is an increasing number of other types of partners). Within this, there is some local flexibility for practices to opt out of certain services (such as additional services) or opt into the provision of other services (such as Enhanced Services). Enhanced Services are services which practices are commissioned to provide by their health board under a local service level agreement and are funded in addition to their GMS contract.
Primary Medical Services agreement (17C): these General Practices have locally negotiated agreements, enabling, for example, flexible provision of services in accordance with specific local circumstances.
Directly-run (2C): these General Practices are run directly by the local Health Board rather than by GP partners.
The contractual requirements of access to GMS General Practices) are set out in, The National Health Service (General Medical Services Contracts) (Scotland) Regulations 2018 (legislation.gov.uk)[13] and this forms the basis of all GMS contracts between General Practices and NHS Health Boards.
The Regulations advise that General Practices “must provide the (essential) services… throughout core hours.”
“The services described... are… for the management of its registered patients and temporary residents who are, or believe themselves to be—
(a) ill, with conditions from which recovery is generally expected;
(b)terminally ill; or
(c)suffering from chronic disease,
delivered in the manner determined by the practice in discussion with the patient.
“The services … includ[e]..—
(a)the provision of advice in connection with the patient’s health, including relevant health promotion advice; and
(b)the referral of the patient for other services under the Act.”
General Practices with GMS contracts (17J) or Primary Medical Services agreements (17C) are known as “independent contractors”. As independent contractors, General Practices decide how they want to make services available to their patients. The type of telephone system, number of telephone lines, number, and type of appointments available and other access arrangements, such as number of receptionists, are for the General Practice to determine depending on the needs of their local populations and available capacity with the practice team.
Neither a GMS contract nor a Primary Medical Services agreement stipulates the form that arrangements should take, only that they should be “delivered in the manner determined by the practice in discussion with the patient” as set out above in the GMS contract.
Independent contractors (the GP partners) also employ their own staff such as Practice Managers, Administrative staff (receptionists) and General Practice Nurses. As such, access arrangements in each General Practice are different depending on a number of factors including workforce configuration, overall capacity, premises, telephony systems, digital systems and people’s needs set within local geographic and demographic factors.
The GMS contract also sets out other requirements such as compliance with the Patient Rights (Scotland) Act 2011[14] (which sets out how complaints should be managed – more guidance from SPSO is available online[15]), Health and Safety at Work etc. Act 1974[16] and other legislation.
As part of their contract, General Practices must be available to their registered patients from 8 am – 6.30 pm (core hours or as previously agreed through local negotiation) Monday-Friday (NHS24 and the Out of Hours service will be available out with these hours). General Practice contracts also specify the practice area which the practice covers and sets out where the practice will accept new patients from. General Practices can refuse applications from people to join the practice if they live out with this practice area.
Finally, people register with a General Practice and not with a specific named GP although patients can often express a preference for a particular doctor when they are making an appointment. As set out in the Scottish Government registration guidance[17] to practices in 2018, two key principles underpin universal access to primary care:
1. No documents are required to register with a General Practice. The inability by a person to provide identification or proof of address is not considered reasonable grounds to refuse or delay registering a person.
2. Anybody in Scotland may access primary care services at a General Practice without charge.
General Practices struggling with capacity may temporarily close their lists to new patient registrations with their Health Board’s agreement. This is difficult for practices and can be distressing for people. Although a critical issue and related to a practice’s ability to provide access, addressing capacity issues with contractual mechanisms, such as closing lists or changing practice boundaries, is out with scope of this work or the Access Principles.
2018 GMS Contract
In 2018, the Scottish Government negotiated a new GMS (GP) Contract with the Scottish GP Committee (BMA), the 2018 GMS contract[18] and associated Memorandum of Understanding (MoU), which includes GMS Contract Implementation in the context of Primary Care Service Redesign[19] and GMS Contract Implementation for Primary Care Improvement[20].
The 2018 GMS contract[21] set out a transformative new direction for Primary Care services in Scotland, as well as putting in place investment and support for Scotland’s General Practices.
The contract came into effect in April 2018 and included service redesign to establish health board-employed MDTs providing the following services:
- Pharmacotherapy
- Vaccination Transformation Programme (VTP)
- Community Treatment and Care Services (CTAC)
- Community Links Workers
- Additional Professional Roles (including MSK physiotherapists and mental health workers)
- Urgent Care Services
Access
Access to general practice has become an increasingly high-profile issue since Infection Prevention Control measures were implemented at the beginning of the pandemic. Although the need for these measures has ended, there is a continuing perception among the public in some areas that it is difficult to access care from General Practice.
While complaints about getting face to face appointments have eased, difficulties getting through on the telephone, concerns about the questions asked by practice receptionists and the availability of appointments continue. General Practices also report an increase in difficult and challenging behaviour from people, sometimes resulting in violence and aggression. These complaints are, of course, far from universal and should not detract from the excellent work done by General Practices across Scotland to provide high quality person-centred care in challenging circumstances but unfortunately, a perception that access to General Practice is poor and difficult, is widely reported (such as in this news paper article[22]).
This is also at a time when General Practice is under increasing pressure with increased demand for services for a number of reasons: the residual impact of the pandemic on hospital waiting times; an increase in mental health issues and other health issues such as respiratory infections; an aging demographic; people living longer with multimorbidity and more care being transferred from hospital to primary care; alongside an increase in people’s expectations of healthcare services.
Concerned that this perception of General Practice was damaging general practice and primary care, the then Cabinet Secretary for Health and Social Care wrote to all General Practices across Scotland on 15 November 2022 announcing the formation of the General Practice Access Short Life Working .
“The group, jointly led by Dr Scott Jamieson, a GP Partner and Quality and Safety Fellow, and Fiona Duff, an experienced Primary Care and Practice Manager, aims to understand the challenges and issues affecting access to General Practice and will establish high level core principles to support and enhance patients’ experience of accessing ‘The Right Care, Right Time, Right Place’.”
Access to General Practice continues to be a highly emotive subject and has been for many years. It is a topic of discussion by all health and social care staff, people and service users, their families and carers, wider society, politicians, policy makers and the media. There is seldom commonality of definition of what access is or what it should deliver. ‘Appropriate access’ is not universally understood and on the back of a pandemic which revolutionised practice processes, it is sensible to consider exactly what we aim to deliver from a limited, but critically important part, of our National Health Service in Scotland.
There is a sparsity of evidence or policy, especially post-pandemic, regarding what General Practice access should deliver or how this is best achieved. We know, contrary to some perceptions, some people in certain situations value continuity over speed of access and are willing to accept a longer wait for a clinician they know over rapid on the day of access (Gerard K, 2008). Continuity of care reduces the burden of illness and mortality and is especially important to prioritise for those groups who may be less vocal in expressing their needs e.g., those with complex long-term conditions, those with mental health conditions, those with complex health and social care needs. This is key to any service delivery model. British Journal General Practice Feb 2022[23] has several articles outlining how continuity reduces Out of Hours use, improves mortality and reduces acute hospitalisation. Royal College of General Practitioners (RCGP) also has a Toolkit to improve continuity[24].
Contact
Email: nicola.rae2@gov.scot