Junior doctors - 48-hour maximum working week (without averaging): expert working group report
This report was led on by Professor Philip Cachia to consider the challenges of the maximum 48 hour working week and provide recommendations for the Scottish Government to consider.
Appendix 2: Hairmyres 48 hour maximum (without averaging) working week pilot rotas and analysis:
Following on from the formulation of ‘48hour’ rotas, based on those currently in place within NHS Lanarkshire, and continuing to adhere to other parameters as outlined above, an analysis was undertaken to assess the impact of such a change on doctors in training working and the wider NHS. This would be conducted as a tabletop exercise to ensure patient safety and service continuity, and allow the collection of data, to model the impact of the proposed change on existing services.
A number of proxy measures were adopted to measure the impact of the proposed shift to 48 hours maximum grouped into 3 main topic as follows:
| Proxy Measure | Work Experience (WE) | Work Life Balance (WLB) | Employee Experience (EE) |
|---|---|---|---|
| Loss of Normal Working Days | X | ||
| Change from Days to Nights/Nights to Days | X | X | |
| Ability to Take Leave (1 week)# | X | X | |
| Impact of Teaching/Training | X | X | |
| Effect on other team members | X | X | |
| Effects on life outside of work | X | X | |
| Number of Weekends Worked | X |
# As a proxy measurement we have assessed the ability within the rotas being analysed to take 5 continuous days of annual leave, without the need to swap on call shifts and without working either weekend. The requirement of taking leave on standard days will result in a further reduction in the overall number of standard days that any trainee, of any level is at work, as is currently the case in most rotas.
The first five of these items were assessed quantitatively by analysis of formulated 48-hour compliant rotas. The subsequent areas were assessed qualitatively by collection of information from relevant stakeholders, e.g. Educational leads with regards to training impact, and others who work in the departments in terms of effects on life and team.
As per guidance from the 48-hour EWG, the tabletop exercise has used rotas which do not exceed 48 hours in any Monday – Sunday 7 day period. Therefore it is possible that >48 hours could be worked if considering any consecutive 7 day period. Early modelling based on a 48-hour maximum in any 7-day period strongly suggests there would be a starker impact on rotas, which would further adversely impact training time, ability to take leave, changes from days to night, weekends worked and all other proxy measures analysed
Indicative Sum Effects on Training Time & Service Delivery
FY1
Assuming a 4-month placement in the FY1 specialties above (2x medical, 1 surgical), it is possible to indicate how training time is affected by the proposed 48 hour change:
- Increase of 30 zero days (28 v 58)
- Corresponding decrease in standard days by 28 (144 v 116)
- Reduction in training time in FY1 of 6 weeks of training
FY2
Assuming a 4-month placement in the FY2 specialties above (1x medical, 1x surgical, 1x emergency medicine), it is possible to indicate how training time is affected by the proposed 48 hour change
- Increase of 35 zero days (34 v 69)
- Corresponding decrees in standard days by 32 (123 v 91)
- Reduction in training time in FY2 of 7 weeks of training
Overall across the foundation program this would result in the loss of almost 3 months of training over a two-year training programme and 60 days of daytime clinical service cover per doctor on the rota
Junior Surgery
The analysis above covers a 6month junior surgical placement; given this is a role covered by a variety of levels (FY2, GPST and CTs). In order to allow full we will assess the impact of an absolute 48hour rota on a year within this rota.
- >50% increase in zero days
- 30% increase in night to day/ day to night shift changes
- Loss of 54 standard days of training per annum.
Overall this equates to a loss of over 10 weeks ‘daytime’ training per annum.
Senior Surgery
The summary analysis above covers a typical yearlong higher surgical placement.
- Double the number of zero days; from 41 to 82 annually
- 30% increase in night to day/ day to night shift changes
- Loss of 46 standard days of training per annum.
Overall this equates to a loss of over 9 weeks ‘daytime’ training per year.
Extrapolated up over a 6 year higher surgical training program this equates to a loss of 54 weeks of training or an entire year of training.
Overall this would result in the loss of 74 weeks (~17 months) of training over an eight-year surgical training programme & 384 days of daytime clinical service cover per doctor on the rota (~77 days p.a.)
Junior Medicine
The analysis above covers a 6month junior medical placement; given this is a role covered by a variety of levels (FY2, GPST and CTs). In order to allow full we will assess the impact of an absolute 48hour rota on a year within this rota.
- Nearly 100% increase in zero days
- 67% increase in night to day/ day to night shift changes
- Loss of 28 standard days of training per annum.
Overall this equates to a loss of 5.6 weeks ‘day time’ training per annum.
Senior Medicine
The summary analysis above covers a typical yearlong higher surgical placement.
- 29 more zero days, an increase >50%
- >50% increase in night to day/ day to night shift changes
- Loss of 30 standard days of training per annum.
Overall this equates to a loss of 6 weeks ‘day time’ training per year.
Extrapolated up over a 5 year higher medical training program this equates to a loss of 30 weeks of training or 7 months of training.
Overall this would result in the loss 42 weeks (~10 months) of training over a seven-year medical training programme and 206 days of daytime clinical service cover per doctor on the rota (average 77 days p.a.)
Emergency Medicine
- Analysis unclear due to atypical work patterns – would need more specialty input
- For example, the senior EM rota has only 1 standard day per cycle, but a large number of other differing shift times – it is likely some of these shifts would provide core training experience and require different degrees of input from various staff groups to provide a safe service
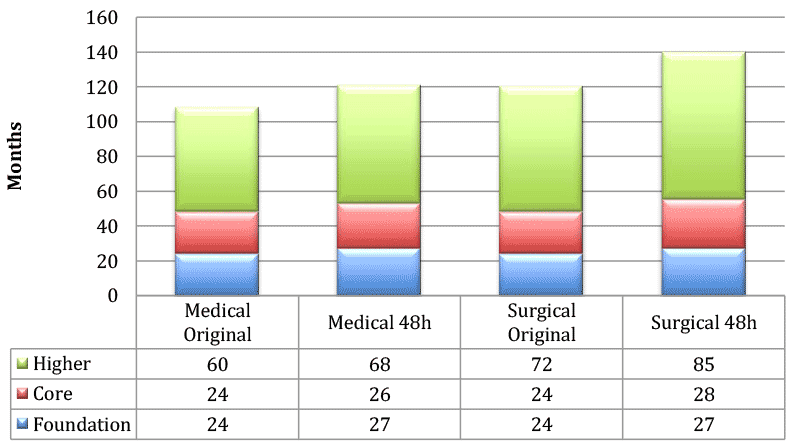
Postgraduate Training & Impact on Time to CCT
Postgraduate training is regulated by the General Medical Council (GMC) on a UK-wide basis, with medical Royal Colleges involved in producing curricula, with which all doctors much comply fully at the expected rate to complete training (gaining a Certificate of Completion of Training – CCT) and obtain work as Career Grade doctors in the NHS. Training programme lengths are fixed within curricula, with doctors in postgraduate training having to obtain certain qualifications, levels and types of clinical experience as they progress – this is often demanding particularly where there are service pressures or shortages for even part of a doctor’s training. The implementation of a 48-hour absolute week would, due to restrictions on rostering in order to meet all other legal and contractual safety rules, lead to a reduction in standard working days for trainees, reducing opportunities to meet these requirements. This risks trainees being deemed unable to progress at their mandatory Annual Review of Competence Progression (ARCP), and requiring additional training time in order to fulfil these requirements.
We have assessed the time that would be needed to counteract the loss of training time due to 48-hour working, if the same amount of training is needed as at present, as a proxy for the impact this would have on medical training in Scotland. It should be noted however that the current structures and assessments within training do not allow additional training time without awarding trainees an ‘unsatisfactory’ outcome at their ARCP.
This was examined in the context of a trainee entering FY1 then directly into specialty training without any career breaks, working full time, with no time out of programme. This has only been undertaken for medicine and surgery as further information is required on the training impact of a 48-hour absolute working week on emergency medicine rotas. In summary there would be an increase of:
- 13 months to complete medical training
- 20 months to complete surgical training.
This would have significant workforce implications in terms of the supply pipeline of qualified doctors, by increasing the time to produce a Consultant. In addition. this may make jobs unattractive to those outside of Scotland, or even to Scottish trainees who could train quicker (i.e. at the normal rate) within the rest of the UK. As mentioned above, training standards are set at UK level with expectation of progress within a fixed number of training years. It is likely extra training time could only be awarded by the deanery by giving unsatisfactory ARCP outcomes to trainees, if such rotas were approved. This has the potential to impact the long-term career progression and would disadvantage Scottish trainees unless a separate indicative training time for Scotland could be negotiated with the GM, thereby creating separate training systems with the UK.
Contact
Email: ceu@gov.scot