Coronavirus (COVID-19) Scotland's Strategic Framework update – February 2022: evidence paper
This evidence paper accompanies the Strategic Framework update and provides an overview of the key analysis and evidence underpinning the Framework, published on 22 February 2022.
2. Where we are now
2.1 Introduction
This section starts off by describing the pattern of the epidemic since November 2021, the date of the last Strategic Framework update. It then considers the impact of new variants, recent changes in testing practice and the range of measures applied in Scotland to reduce the impact of Omicron.
The analysis continues to set out the current position regarding health and social care, society and the economy to complete the 4 harms analysis.
2.2 The pattern of the epidemic since November 2021
The November publication of the Strategic Framework followed a period of fairly level number of cases which fluctuated throughout the month of October 2021, see Figure 1.
The average number of PCR (polymerase chain reaction) confirmed cases each day remained fairly level throughout November, see Figure 1. By 30 November 2021 there was an average of 2,656 PCR confirmed daily cases by specimen date. Omicron was first reported in Scotland on 29 November 2021 (based on a sample from 23 November)[2] and became the dominant strain on 17 December. Throughout December cases rapidly increased to a peak on 3 January 2022 of 16,407 (7-day average) PCR confirmed cases per day by specimen date. This peak was considerably higher than previous peaks in September 2021 (6,439 average daily PCR cases) and July 2021 (3,318 average daily PCR cases).
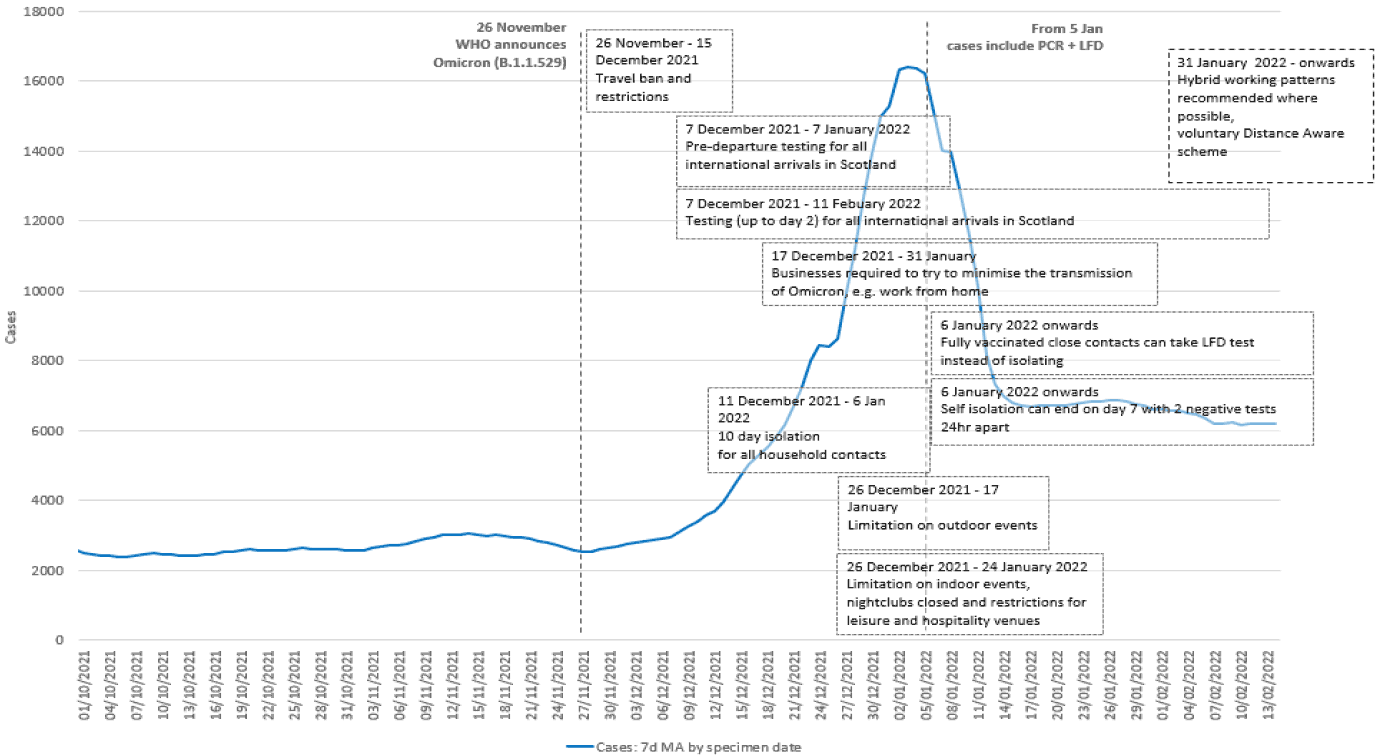
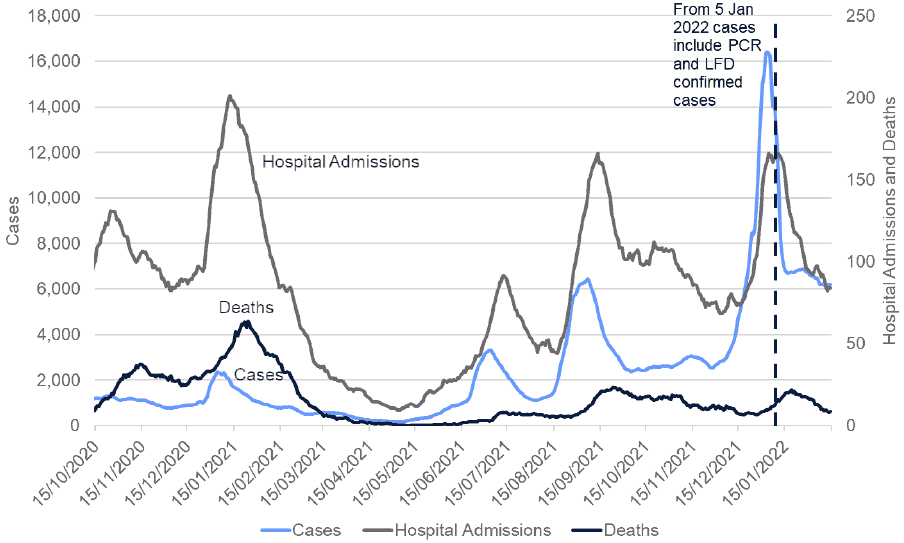
On 5 January 2022, the Scottish Government announced[4] that people who do not have symptoms of COVID-19 would no longer be asked to take a PCR test to confirm a positive Lateral Flow Device (LFD) result. Instead, anyone with a positive LFD, who does not have symptoms, is required to report the result online as soon as the test is done. This means that those without symptoms who previously would have taken a confirmatory PCR test, no longer do so. Data has been updated to reflect the new case definition for those who have recorded a first positive PCR or LFD from 5 January 2022, see Figures 1 and 4.
Since the peak in early January 2022 there has been a decreasing trend in both PCR confirmed cases and in PCR and LFD cases reported to mid-January. The seven-day average number of combined PCR or LFD daily cases has levelled off since around 18 January, with a slight overall decrease in the most recent two weeks, see Figure 4. The Covid-19 Infection Survey also shows that the number of people in the private residential population testing positive for COVID-19 decreased from a peak on 3 and 4 January 2022 and then fluctuated from mid to late January[5].
Since November 2021, those aged 60 and over have consistently had lower case rates, than those aged under 60. The peak in case rates in early January 2022 was largely driven by those in the 20-39 age group, followed by those aged 40-59 and those aged under 20[6]. PCR and LFD case rates have levelled off for those aged 25 and over since mid-January, and have remained at similar levels with minor fluctuations throughout the weeks. Among those aged 19 or younger, weekly case rates increased from mid-January, peaking on 26 January. The weekly case rate for this age group has since decreased, but in the week to 12 February the weekly case rate for those aged 16 to 17 remained similar to the previous week[7].
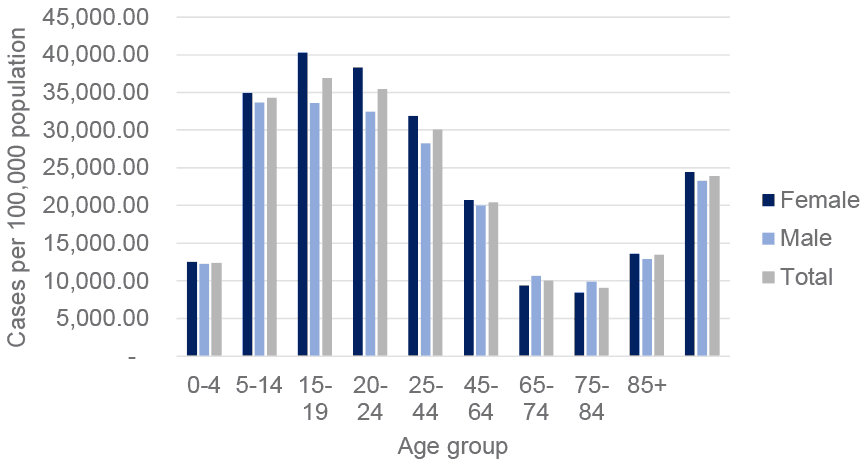
Overall, males and females have typically had a similar case rate, with females having a slightly higher number of cases per 100,000, see Figure 2. Females aged 64 and under tend to have higher levels of Covid case rates than males in the same age groups, and the trend is reversed for those aged 65 to 84. The Equalities Impact Assessment, will be published at a later date and provides more detail on COVID-19 inequalities.
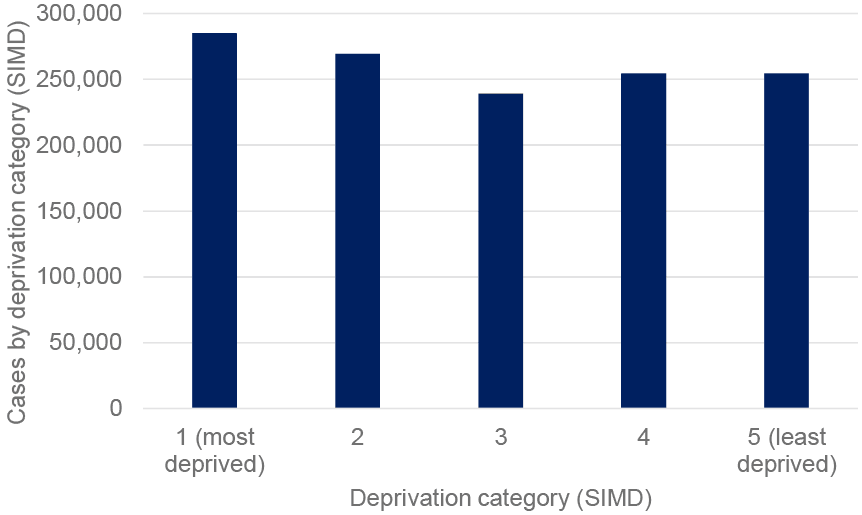
Over the course of the pandemic, the total rate of positive cases per 100,000 in Scotland is highest in the most deprived quintile, followed by the second most deprived, see Figure 3.
The relationship between infections and serious health harms has weakened significantly compared to earlier stages of the pandemic. Serious health harm continues but at much lower levels for a given number of cases than in the past.
However, the rapid increase in PCR confirmed cases as a result of the spread of the Omicron variant translated into a high level of COVID-19 hospital admissions, peaking at a seven day average of over 160 per day at the beginning of January 2022. This was at a similar level to the previous peaks in September 2021 (peaking at an average of over 160 per day) and lower than the peak in January 2021 (peaking at an average of over 200 per day), see Figure 4. COVID-19 hospital admissions have continued to decrease since the peak in early January 2022.
In general, throughout the pandemic, older age groups have had the highest COVID-19 admissions to hospital[11]. Those aged 65 and over have had more admissions to hospital per 100,000 compared to the average for all ages (899 admissions per 100,000), while those aged 85 and over have had over 5,400 admissions to hospital per 100,000. Overall, through the course of the pandemic, males and females have typically had a similar hospital admissions rate, with males having a slightly higher number of COVID-19 related hospital admissions per 100,000. Females aged between 5 and 44 have tended to have higher levels of admissions than males in the same age groups, and the trend is reversed for those aged 45 and over[12].
COVID-19 admissions to hospital have also been highest for those in the most deprived quintile, and lowest for those in the least deprived quintile[13] [14]. The latest data available shows that as at 30 September 2021, compared to White Scottish, rates of hospitalisation or death were estimated to be around 4-fold higher in Pakistani and Mixed groups, and around 2-fold higher in Indian, Other Asian, Caribbean or Black, and African groups. Higher rates were also observed in White Other. Lower rates were observed in patients recorded as White Irish[15] [16].
In the past four weeks, from 8 January 2022 to 4 February 2022, the age-standardised rate of hospital admissions per 100,000 were 2.9 to 3.8 times lower in individuals with their third dose or booster dose of vaccine compared to unvaccinated individuals or have received one or two doses of a COVID-19 vaccine[17].
Deaths were on a decreasing trend throughout November and December 2021, there was an average of 18 daily deaths in the first week in November, compared to over 8 in the last week in December 2021. Deaths have increased in January 2022 to over 21 deaths per day on 19 January 2022 and have since decreased, see Figure 4.
Throughout the pandemic, deaths involving COVID-19 have been highest for those aged 75 and over[18]. From the start of the vaccination programme, there have been 6,268 confirmed COVID-19 related deaths with a positive PCR result and where COVID-19 was recorded as an underlying or contributory cause on the death certificate[19]. In the week from 29 January to 4 February 2022, 74 individuals tested positive for COVID-19 more than fourteen days after receiving their booster or third dose of vaccine and subsequently died with COVID-19 recorded as underlying or contributory cause of death. The majority of these individuals had several comorbidities which contributed to their deaths and the mean age was 82 years old[20].
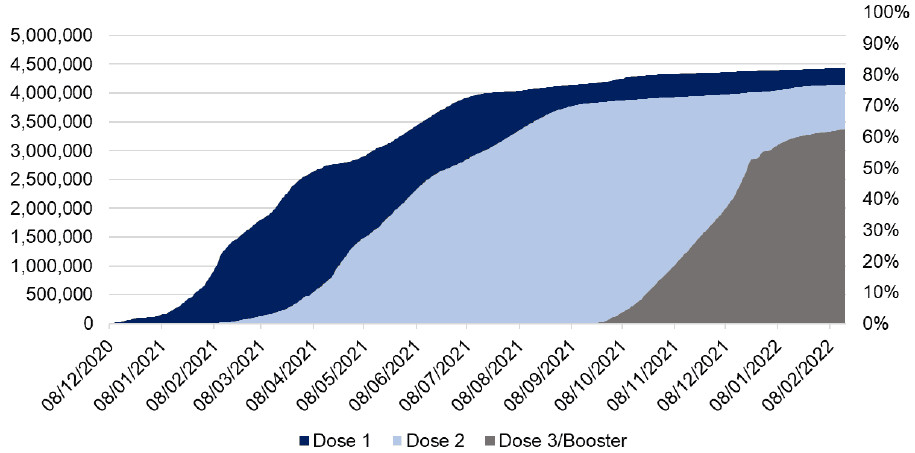
In response to Omicron, the booster vaccination roll out was scaled up during November and December, see Figure 5. In line with advice from the Joint Committee on Vaccination and Immunisation (JCVI), a booster dose or a third dose of the vaccine is now available in Scotland, including all adults aged over 16 for whom it has been at least 12 weeks since their second dose[24]. Over 3.3 million people (70.6% of those over 12 years of age) have received their dose 3 or booster vaccine by 18 February 2022[25]. Antibody data indicates that Scotland’s COVID-19 antibody levels in adults have remained high[26].
Booster vaccine uptake is at least 92% amongst both males and females aged 60 or over, and around 90% for those aged 55 to 59. However, there is a difference between male and female vaccine uptake among those aged between 18 and 49 with females showing a higher uptake compared to males[27]. The analysis shows that across all age groups, vaccination uptake for the third or booster dose has been the highest among White ethnic groups. Vaccine uptake was lowest in African ethnic groups, except for those aged 40 to 49 and 50 to 54 years. In these two age groups, vaccination uptake was the lowest among the Caribbean or Black group. There is variation across age within each ethnic group, with higher uptake in older age groups. These trends mirror the uptake of the second dose of the vaccine, as the third or booster dose relies on previous doses being administered.
In their report published on 2 February 2022[28], Public Health Scotland (PHS), provided an analysis on vaccination equality in Scotland[29]. Vaccination data are from 8 December 2020 to 30 January 2022, and the analysis contains comparisons by ethnicity and socio-economic deprivation by age bands. These analyses highlight differences in uptake between demographic groups and areas, but they do not examine causative factors for the inequalities, which will be numerous and complex.
In the four weeks from 8 January 2022 to 4 February 2022, in an age-standardised population, the death rate in individuals that received a booster or third dose of a COVID-19 vaccine was between 4.6 and 9.5 times lower than individuals who are unvaccinated, or have only received one or two doses of a COVID-19 vaccine.[30] [31]
2.3 An overview of Omicron
Omicron was first reported in Scotland on 29 November 2021 from a sample taken on 23 November and it quickly became the dominant variant, with more than half of COVID-19 cases being Omicron on 17 December 2021[34] [35] [36] [37]. It has spread rapidly around the world and caused large waves of infections in many countries[38].
Omicron has a significant growth advantage over Delta, the previous dominant variant in Scotland[39]. Omicron can infect people who have been vaccinated or who have had a previous infection more readily compared to Delta. Omicron has multiple genetic mutations allowing it to evade antibodies and other immune responses developed through vaccination or natural infection[40].
The Office for National Statistics (ONS) estimates the risk of reinfection was 16 times higher in the Omicron-dominant period (20 December 2021 to 9 January 2022) compared with the Delta-dominant period (17 May to 19 December 2021)[41]. The risk of reinfection with Omicron was estimated in a modelling study carried out by Imperial College London, where results suggested that due to the immune evasion properties of Omicron, protection against infection reduced to 19%[42].
However, Omicron infections are generally less severe and less likely to result in hospital admission than Delta[43] [44] [45]. Preliminary data from the UK Health Security Agency (UKHSA) indicated that the risk of attending hospital or emergency care is estimated at around half for Omicron compared to Delta, and the risk of being admitted from emergency care around one third of Delta[46] [47]. Early data also indicated that the severity of disease once in hospital, assessed by, for example admission to ICU, is lower than observed in early phases of previous waves[48]. The most recent analysis showed that the risk of hospital admission with Omicron compared to Delta varied by age, with similar risk of hospital admission among children aged under 10 years old, with an approximate 75% reduction in the risk of hospital admission among those 60 to 69 years old. The risk of death was approximately 60% lower among Omicron cases compared to Delta[49].
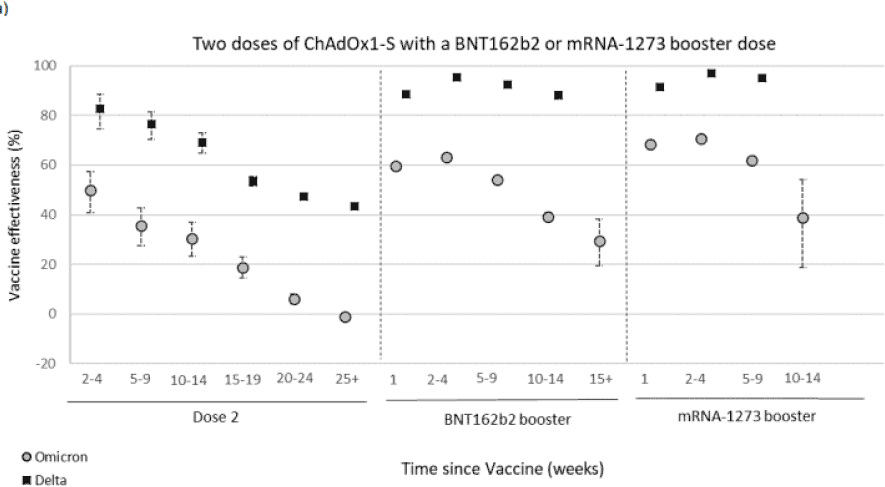
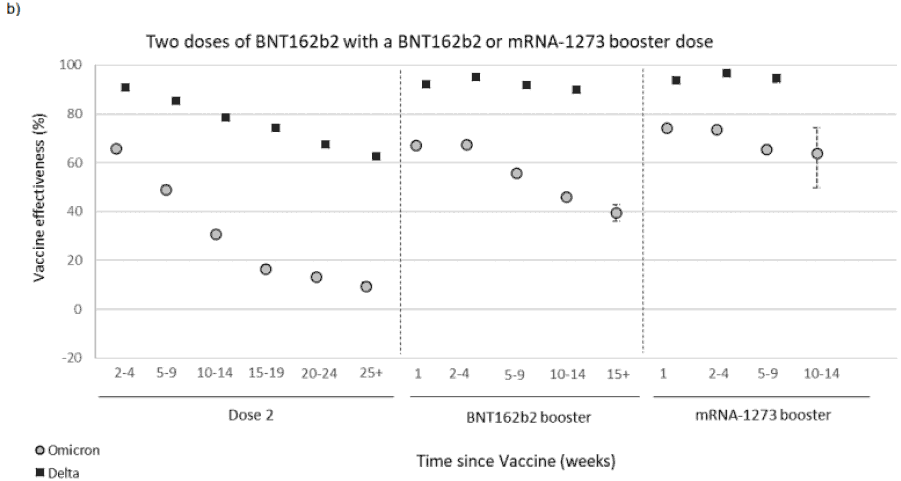
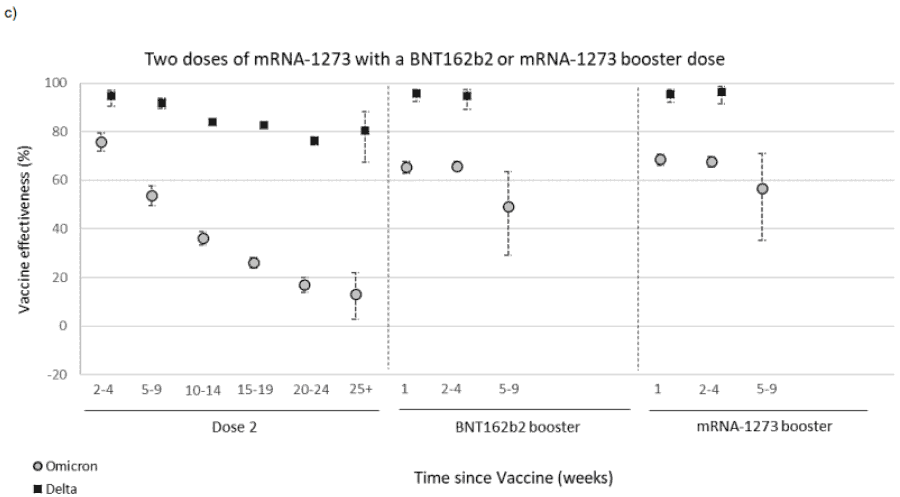
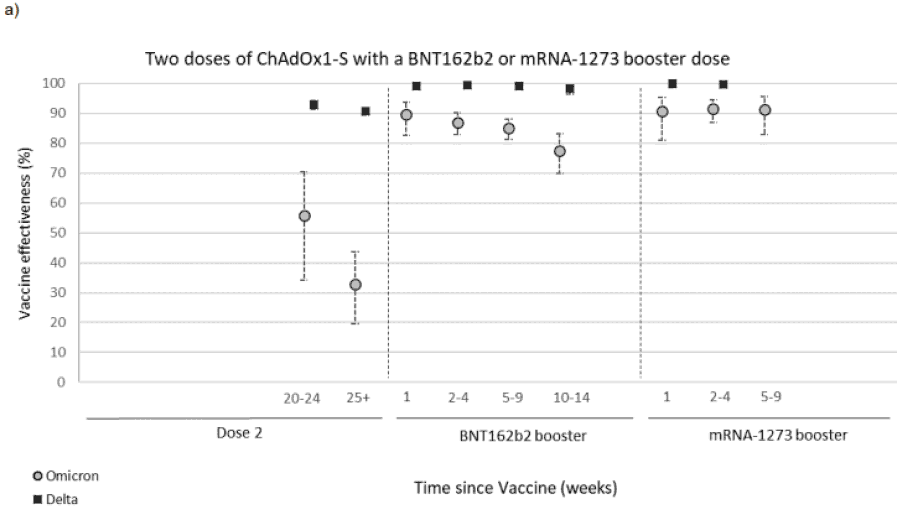
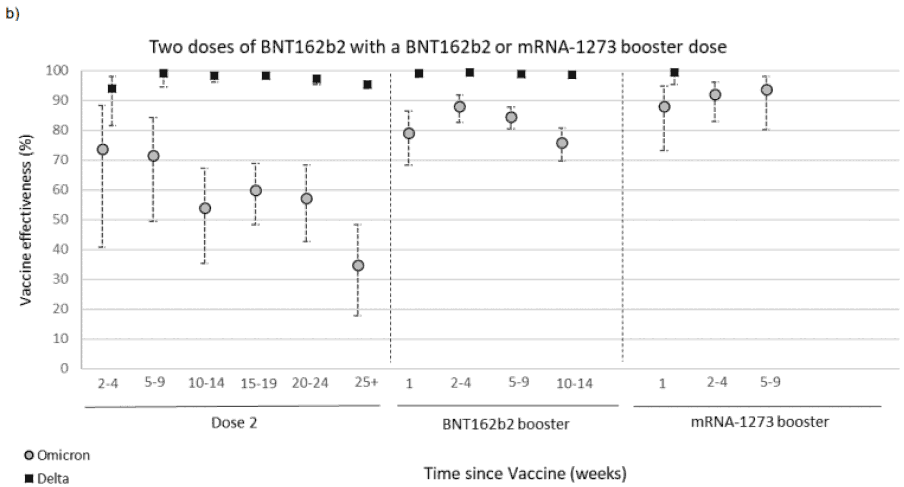
Vaccine effectiveness against symptomatic disease with the Omicron variant is lower compared to the Delta variant and wanes rapidly. Protection against symptomatic disease from two doses of vaccine is very low (10% or less) after 20 weeks. With a booster, vaccine effectiveness varies according to the vaccine administered but ranges from around 60 to 75% two to four weeks after vaccination dropping to between 25-40% after 15 weeks[50], see Figure 6.
Protection against hospitalisation from vaccination is greater than that against symptomatic disease, in particular after a booster dose, with data showing vaccine effectiveness over 75% 10 to 14 weeks after receiving a Pfizer/BioNTech booster dose. Vaccine effectiveness against hospitalisation remains at 90-95% up to 9 weeks post-vaccination when receiving a Moderna booster dose[51], see Figure 7.
Protection against mortality from vaccination drops to 59% 25 weeks after the second dose. Two weeks after the booster dose protection is restored to 95% for people aged 50 or over[52].
2.4 The impact of BA.2
A sub-lineage of Omicron, termed BA.2, was designated a VUI by the UKHSA (VUI-22JAN-01) on 19 January 2022[55]. BA.2 does not have the spike gene deletion at 69-70 that causes S gene target failure (SGTF), seen in the Omicron BA.1 sub-lineage[56]. BA.1 and BA.2 share 38 nucleotide and amino-acid mutations and BA.2 contains an additional 28 mutations and a deletion at 25-27[57] [58]; BA.1 has additional 20 mutations[59].
As of 18 February, there had been 893 cases of BA.2 reported in Scotland[60]. BA.2 has spread globally, overtaking the BA.1 lineage and making up the majority of sequenced cases in Denmark, India, Philippines, South Africa, Qatar and Sri Lanka as of 7 February 2022[61] [62].
The UKHSA risk assessment[63] of 9 February identifies with a moderate confidence, that BA.2 has an overall growth advantage over BA.1 with preliminary data showing increased household secondary attack rates in the UK (13.4% vs 10.3% in other Omicron cases)[64]. Evidence also suggests that the transmissibility of BA.2 is greater than BA.1 and/or serial interval (time from symptom onset of a primary case to symptom onset in their identified contacts) of BA.2 is shorter than BA.1, however there is currently no evidence to suggest that immune evasion is different between the two lineages of Omicron. There is also currently insufficient data to determine any difference in infection severity[65].
Current evidence suggests vaccine effectiveness against symptomatic disease is similar for BA.1 and BA.2 sub-lineages of Omicron. After 2 doses effectiveness was 10% (9-11%) and 18% (5-29%) respectively for BA.1 and BA.2, after 25+ weeks. This increased to 69% (68-69%) for BA.1 and 74% (69-77%) for BA.2 at 2 to 4 weeks following a booster vaccine and decreased to 49% (48-50%) for BA.1 and to 46% (37-53%) for BA.2 after 10 weeks post vaccination[66]. Preliminary (not yet peer reviewed) analysis of transmission of BA.1 and BA.2, in Danish households indicate that transmissibility from unvaccinated primary cases in BA.2 households was increased compared to BA.1 households with an odds ratio of 2.62 (95%-CI 1.96-3.52). This pattern of increased transmission in BA.2 households was not observed for fully vaccinated and booster-vaccinated primary cases. Susceptibility of infection with BA.2 was increased when compared to BA.1 regardless of vaccination status[67].
2.5 Changes in testing
In the last few months since the November update to the Strategic Framework, the Omicron variant has emerged and cases rates increased steeply. Part of the response was a shift in guidance to encourage the use of lateral flow testing with lateral flow devices (LFDs). Current guidance is to use LFD tests regularly when you have no symptoms. You should test twice a week, as well as before socialising or travelling[68].
Although LFDs are less sensitive than molecular tests such as PCR, they are easier to perform and provide a rapid test result, within 15-30 minutes.
How well LFDs work at detecting SARS-CoV-2 in a person, depends on many factors, such as how infectious the person is, if they have symptoms, the time since their symptoms started and how well they do the test. Although estimates for how sensitive the LFDs are when detecting COVID-19 vary between studies and situations, numerous studies found that LFDs are around 95% effective at detecting SARS-CoV-2 when used at the onset of symptoms or for cases with high viral concentrations [69] [70] [71] [72] [73] [74] [75] [76]. These studies were done before Omicron emerged. However, initial data from laboratory studies indicates a comparable sensitivity of LFDs to Omicron as to that observed for previous strains of SARS-CoV-2 including Delta[77].
In general, LFDs are less sensitive than PCR at detecting the virus and it is possible to miss an infection just before the peak of infectiousness that a PCR test would pick up[78] [79] [80]. Therefore it is best to take a LFD test as close as possible before meeting other people for the best chance of detecting infectious individuals and avoiding transmission[81] [82] [83].
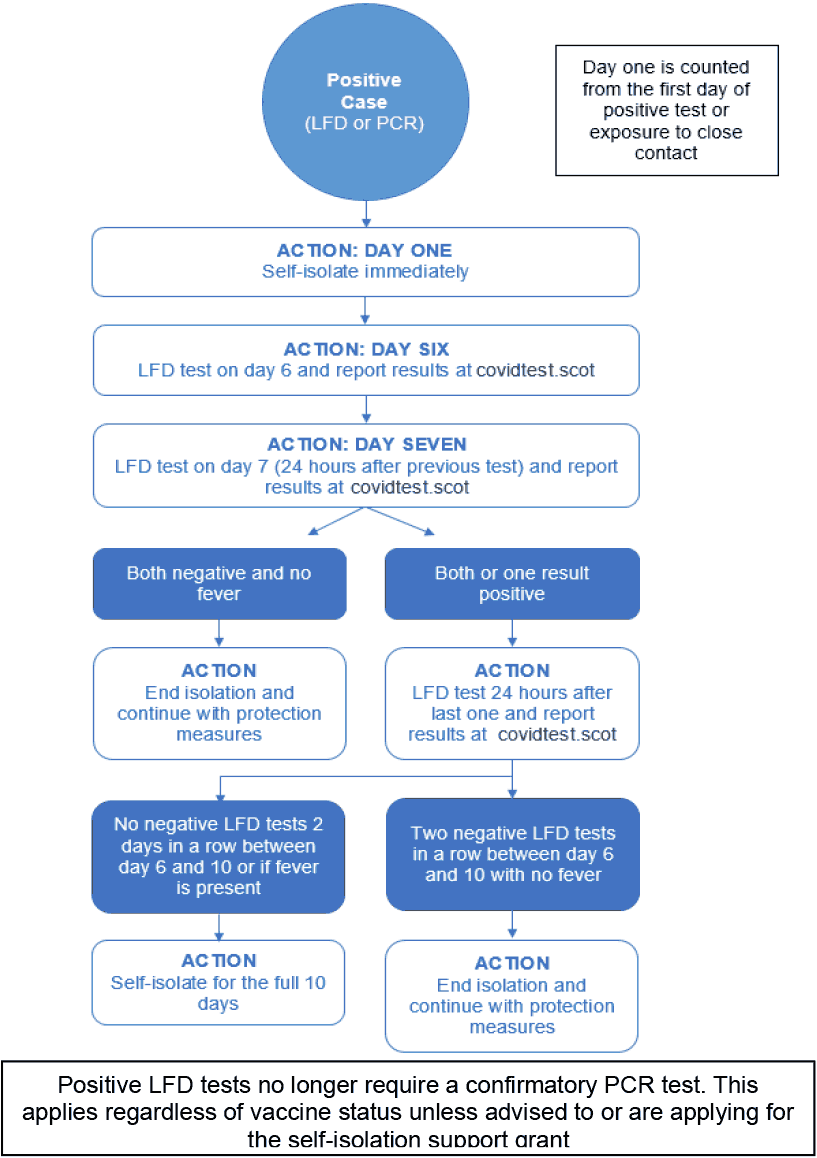
Current guidance is to isolate for 10 days if you've had a positive PCR or LFD test result but no symptoms. You may be able to end self-isolation early if you have 2 negative LFD test results in a row from day 6 onwards, taken 24 hours apart. The key to this regimen is that people should not end isolation early without the two negative LFD tests as there is significant risk that they could still be infectious[84] [85] [86], see Figure 8.
According to the Scottish Contact survey from 3 – 9 February, approximately 76% of individuals had taken at least one LFD within the last 7 days. This decreased from 78% for the survey from two weeks prior. Polling data shows that the proportion who reported taking a COVID-19 test ‘in the past week’ declined slightly – from 64% (18-19 January) to 58% (1-2 February 2022), although reporting of results has remained stable (47%).
After a decrease in the number of LFD tests that were reported between 27 December 2021 and 9 January 2022, there was a peak in reported LFD tests on 16 January 2022, with 810,225 reported tests[88]. The weekly total of tests reported in the week to 13 February decreased by 5% from the previous week leading up to 6 February. There were 714,319 reported tests in the week to 13 February[89].
2.6 Measures in Scotland to reduce the effect of Omicron[90]
The overall objective of these measures when implemented, were to slow the spread of the Omicron variant, to ensure that the National Health Service (NHS) could cope with potential patient numbers and to try and limit workforce absences from less serious illness. As data emerged that Omicron was less severe than Delta, resulting in reduced hospital admissions and patients requiring treatment within ICU, a lifting of the additional measures occurred in a stepwise manner.
The World Health Organisation (WHO) declared Omicron as a variant of concern on 26 November 2021[91], and in order to slow the introduction of Omicron into Scotland, 11 South African countries had a temporary travel ban imposed and were added to the UK red travel list meaning all travellers returning to Scotland from these countries were required to quarantine on arrival at a managed hotel for 10 days [92] [93] [94] [95]. These countries were removed from the UK red list on 15 December[96]. From 7 December[97] all arrivals into Scotland required pre-departure and arrival tests, which was scaled back to just unvaccinated individuals from 7 January 2022, with vaccinated travellers only requiring an arrival test[98]. From 11 February, fully vaccinated travellers no longer required to test[99].
On 29 November the first case of Omicron was reported in Scotland, from a sample taken on 23 November [100] [101]. In response to Omicron, the booster vaccination roll out was scaled up during November and December with those aged 18+ able to book an appointment from 15 December 2021[102].
From 11 December 2021, all household contacts of confirmed positive cases were required to isolate for 10 days[103]. On 6 January, this regulation was ended for triple vaccinated individuals with daily testing required instead and self-isolation for positive individuals could end with two consecutive negative LFD tests from day 6 taken 24 hours apart. The need for a confirmatory PCR test was also removed[104].
On 17 December 2021, as Omicron became the dominant variant in Scotland, legal requirements were introduced for businesses to take reasonable measures to minimise transmission of coronavirus and guidance was given to limit indoor socialising to 3 households with LFD testing before meeting[105] [106] [107].
On 26 and 27 December 2021, legislation was introduced that cancelled large events, 1m physical distancing and table service was required in hospitality and leisure facilities and nightclubs were closed[108]. Limitations on large scale outdoor events were removed on 17 January 2022 with the rest of the restrictions implemented after Christmas being lifted on 24 January, along with the guidance to limit socialising indoors to 3 households[109] [110]. Vaccine certification remains in place for these events including the use of a negative test and the requirement for a third dose which were added to the certification scheme on 6 December 2021 and 17 January 2022 respectively[111] [112].
For the start of the January school term, children aged 12-15 were encouraged to get their second dose, staff and pupils were advised to perform LFD tests before returning to school and more guidance was given to schools to grouping students and increase ventilation[113] [114] [115].
2.7 Summary
This section of the paper traces the development of the pandemic since November 2021 when the previous update of the Strategic Framework was published. It covers a period of change as Omicron BA.1 emerged and became the dominant variant followed by BA.2. Over this period changes were implemented in testing and in the measures introduced to manage the emergence of Omicron which were strengthened and subsequently relaxed in a staged approach.