A caring, compassionate and human rights informed drug policy for Scotland
Outlines what a progressive, evidence-based drugs policy would look like with public health and the reduction of harm as its underlying principles.
A Caring, Compassionate and Human Rights Informed Drug Policy for Scotland
Ministerial Foreword: National Mission to Improve and Save Lives
Every single drug death is a tragedy, behind each statistic is a grieving family and community. The scale of the drug deaths emergency in Scotland requires us to use every lever at our disposal, and we are clear that our actions to resolve this crisis must be comprehensive. This government’s position has consistently been that tackling the drugs emergency requires a concerted and radical public health approach.[1],[2]
Within the powers currently devolved, we are doing all we can through our National Mission to improve and save lives.[3] We are investing an additional £250 million over the lifetime of this Parliament to ensure treatment and support is available at the point of need across all parts of Scotland and to get more people into the life‑saving and life‑changing treatment that is right for them.
In the first two years of the Mission we have already made significant progress, improving services by rolling out our medication assisted treatment (MAT) standards and increasing the capacity of residential rehabilitation services and access to them, increasing funding to community and grass-roots organisations and changing how we work with families.[4] Crucially, we are listening to the voices of people with lived and living experience in what we do and implementing wholesale culture change to ensure people are treated with respect and compassion, empowered to be actively involved in choices around their recovery and to tackle the discrimination and stigma they face.[5],[6]
Through our devolved powers, then, we already have a clear evidence-based plan that aligns our investment and service delivery to reduce deaths and improve lives.[7] What is still missing is legislation that complements this approach, that cares about the people behind the statistics, and treats drug dependency as the health condition it is[8], and in doing so, achieves equity with the treatment of other health conditions.
We therefore call for a change to the legal framework within which Scotland responds to its drug deaths crisis, to enable us to appropriately tailor policy decisions to our unique challenges. We cannot simply import one model or approach from another country – any measures must be adapted to suit our context – but there is robust international evidence that we must learn from.
This paper outlines what a progressive, evidence-based policy would look like. The legislative powers to achieve this are not currently devolved to Scotland, but there are different routes to delivering the changes we call for: they could be implemented by the Scottish Government through a Section 30 order and the devolution of specific powers to Holyrood (including the Misuse of Drugs Act 1971); or through wider constitutional changes such as Scottish independence. The simplest and quickest way for these policies to be enacted, however, would be for the UK Government to use its existing powers to change its drug laws. Scotland needs a progressive policy to help tackle our drug deaths crisis, like many countries around the world are adopting in order to reduce the harm caused by drugs.[9] To be quite clear, this is not in any way incompatible with an ambition to tackle organised criminals who profit from the misery of our communities.
Scotland needs a caring, compassionate and human rights informed drugs policy, with public health and the reduction of harm as its underlying principles, and we stand ready to work with the UK Government to put into practice the progressive policy set out here.
Elena Whitham MSP
Context: Scotland’s Public Health emergency
Drug deaths have increased substantially over the past few decades. In 2021, there were 1,330 drug misuse deaths registered in Scotland, a decrease of 1% (9 deaths) compared with 2020 but the second highest annual total on record. People in the 20% most deprived areas were more than 15 times as likely to have a drug misuse death as those in the 20% least deprived areas – that ratio has widened over the past two decades. Scotland’s drug death rate is the highest in the UK, and higher than that of any European country.[10]
In January 2021, Scotland’s then First Minister Nicola Sturgeon announced a National Mission to reduce drug deaths and improve lives, to be spearheaded by a dedicated Minister for Drugs Policy.[11] This is supported by an additional investment of £250 million over the five-year life of the Parliament.[12]
The Mission takes a holistic, public health response to the challenge. This includes mobilising an emergency response, focusing on harm reduction and preventing fatal overdoses; reducing risk by improving treatment and recovery services; and reducing vulnerability by addressing the social determinants of health by improving access to quality housing, social security, employment and social connection. It also recognises the need to address stigma, respond to the voices of people with lived and living experience and support a resilient workforce.
Approaching this issue from a public health, and not a criminal justice, perspective is key. The rise in drug deaths has been significant enough to contribute to the fall in life expectancy in Scotland. From 2017-2019 to 2019-2021, drug misuse reduced life expectancy by 5.9 weeks for males and 2.5 weeks for females.[13] Drug use disorders pose a sizable threat to Scotland’s population health and wellbeing, and were the third leading cause of health loss in the most recent Scottish Burden of Disease Study, surpassed only by ischaemic heart disease and Alzheimer’s and dementias in healthy life lost as a result of disability and premature death (number of Disability Adjusted Life Years), (Figure 1).[14]
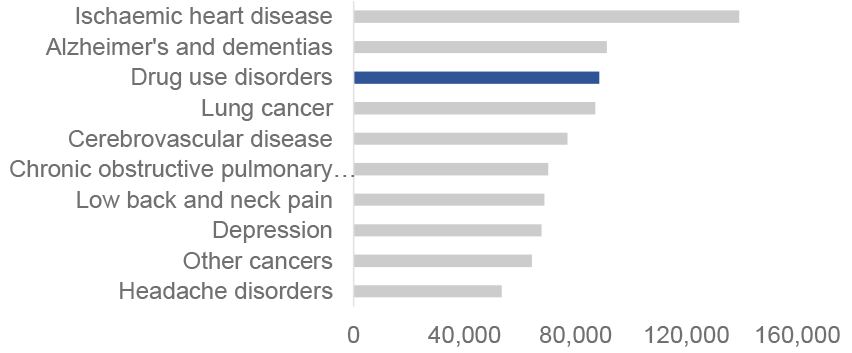
Source: Scottish Burden of Disease Study, Public Health Scotland, 2021
Yet it is the only one of these conditions where we criminalise the people experiencing it. Reducing drug deaths would not just make us safer – the traditional criminal justice measure of success – but crucially, reduce suffering, increase wellbeing and improve Scotland’s health.[15]
This paper argues how the reform of the UK’s drug laws offers an opportunity to contribute to a public health approach. It begins with a summary of how drug laws can affect drug harms, before calling for immediate legislative changes to support harm reduction measures; arguing for decriminalisation of possession for personal supply; and examining the opportunities for a future debate on strict regulated markets.
The current approach to drug law
The law on the control of drugs, set out in the Misuse of Drugs Act 1971[16], is reserved and limits the effectiveness of our public health approach.[17],[18] It criminalises people who experience the inequalities that drive drug use[19] and presents a barrier to seeking treatment.[20] The limits of the devolved competence of the Scottish Parliament in this domain means that we are unable to pursue meaningful reform. In working with people who use drugs, we are often restricted to reactive responses, supporting individuals only when they reach crisis points or are not able to offer help until people have already been criminalised.[21]
This criminal justice approach is not just an obstacle to people’s recovery but is also less effective than a more public health focussed approach at encouraging positive behaviour change. This approach has seen a significant cost around the world both economically and for public health.[22],[23] A 2019 survey of public attitudes to drugs in the UK by the Conservative Drug Policy Reform Group (CDPRG), found that 76% of respondents think that the threat of criminal punishments is not effective at deterring individuals who unlawfully use drugs.[24] Attitudes in Scotland towards the legality of drugs are changing. The percentage of those who agreed that people should not be prosecuted for possessing small amounts of heroin has almost tripled from 15% in 2001 to 42% in 2021/22.[25]
The high levels of drug deaths in Scotland[26], and the continuing increase across England and Wales[27], highlight the need to examine whether our drug laws – especially the Misuse of Drugs Act 1971 – achieve their stated objectives. The onus should be on defenders of the status quo to demonstrate how increasingly hard-line policies of criminalisation, which impact on countless lives across the UK, reduce harm from drugs. The need for reform is not just in line with the evidence, but public perception, as evidenced by the CDPRG survey which reported that 70% of respondents said that “current UK drugs policy has been unsuccessful at reducing the harm done by drug abuse”.[28]
The independent Scottish Drug Deaths Taskforce examined the links between the law and the prevention and treatment of drug harms and recommended that the Misuse of Drugs Act 1971 be urgently reviewed to align with a public health approach.[29] It called for changes to support the provision of harm reduction interventions like heroin assisted treatment, supervised drug consumption facilities, drug checking and the reclassification of naloxone, as well as changes to remove the exemption which exists in the Equality Act 2010, which excludes people identified as “addicted” to drugs and alcohol from the scope of provisions prohibiting discrimination against people with disabilities.[30] It stated that if the UK Government is not willing to reform the Misuse of Drugs Act 1971, it should commit to exploring all options openly with the Scottish Government to enable Scotland to take a public health approach.
This, and similar recommendations from the Scottish Affairs Committee[31],[32] and Westminster Health and Social Care Committee[33],[34] have so far been rejected by the UK Government. It is instead continuing, and in some cases expanding, criminal sanctions[35] that have no proven efficacy in preventing drug deaths. We have seen this most recently with the forthcoming criminalisation of nitrous oxide[36], against the recommendation of the Advisory Council on the Misuse of Drugs (ACMD).[37]
The United Nations Office on Drugs and Crime estimate that in 2021, one in every 17 people aged 15-64 in the world had used a drug in the past 12 months. The estimated number of users grew from 240 million in 2011 to 296 million in 2021 (5.8% of the global population aged 15-64), an increase of 23%, partly as a result of growth in the global population.[38]
Among the estimated 296 million people who used drugs in the past year in 2021, some 39.5 million people were estimated to suffer from drug use disorders, meaning that their pattern of drug use is harmful, or they may experience drug dependence and/or require treatment. This is an increase of 45% over 10 years.[39]
Prohibition is also incredibly expensive. It is estimated that policing and interdiction of illicit drugs globally costs over U.S. $100 billion a year.[40],[41] As a strategy to reduce drug use, the global war on drugs has failed in its objectives.
A Caring, Compassionate and Evidence Based Approach
“We must stop the so-called war on drugs. Instead let us focus on transformative change, crafting drugs policies which are based on evidence, put human rights at their centre, which are gender sensitive and which ultimately improve the lives of millions of people affected”
Volker Turk, UN High Commissioner on Human Rights at the 66th UN Commission on Narcotic Drugs.[42]
There is no denying that Scotland’s ambition to implement evidence-based policies based on a public health approach is limited by the UK’s legal framework within which it must currently operate. Moreover, it can be argued that the UK government’s legal framework on drugs limits its own stated commitment to a whole systems approach.
The Scottish Government has called for a review of our drug laws[43], including the Misuse of Drugs Act 1971 and has supported the many calls of experts to do the same.[44] Other UK legislation also inhibits a public health approach, and in the past we have also called for the reclassification of naloxone through the amendment of the Medicines Act 1968 and removing the exemption in the Equality Act (Disability) Regulations (2010) , which excludes people with substance dependency from the protected characteristic of disability.[45]
We hold that the purpose of any drug law reform must be the reduction of harm. As a general principle, that harm can be exacerbated both by excessive prohibition but also excessive legalisation. A balance is needed between strict prohibition at one extreme, which perpetuates harm through criminalisation, stigma, discrimination and a thriving illicit market[46]; and an unregulated legal market with no controls at the other, perpetuating harm through a profit-driven commercial market. Both produce poor public health outcomes. Any legal framework must therefore operate in between these two extremes, with public health as its primary driver, investing in research and evaluation and being guided by experts, including those with lived and living experience and taking account of public attitudes. At present, the legal framework Scotland operates in is characterised much more by prohibition than legalisation and as a result, represents an active barrier to adopting more evidence-based approaches to reduce drug harms.
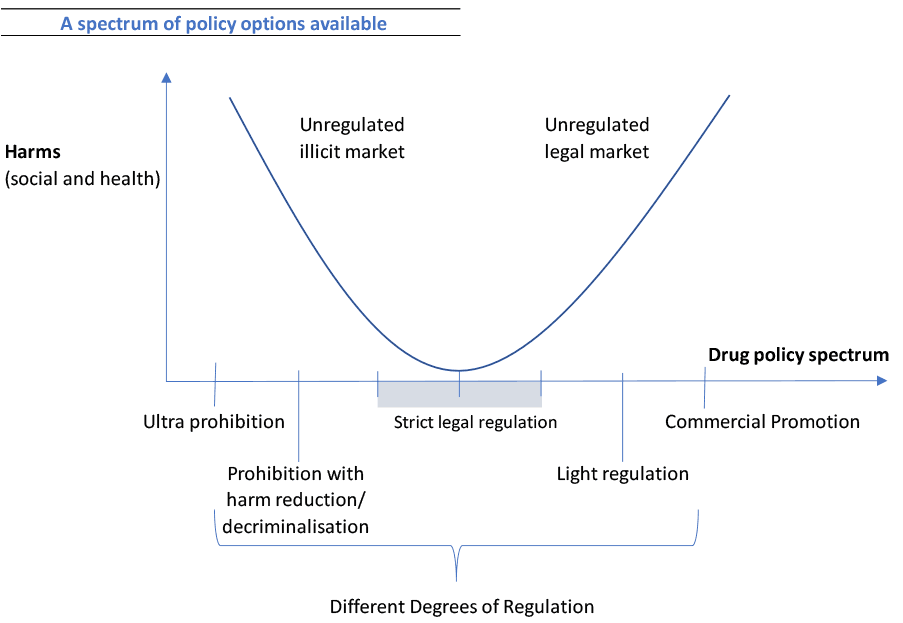
Graphic adapted from the Global Commission on Drug Policy (2021)[47]
Drug law reform is often mis-characterised as promoting free, uncontrolled use of substances. The graphic above illustrates the view that at both ends of this spectrum free access to uncontrolled drugs either through an illegal or legal market perpetuates significant harms. Our goal with any changes would therefore be to find the point of lowest harm. In doing so, it is also important to consider the evidence from various sources: the existing regulation of substances in the UK such as alcohol and tobacco; and evidence from countries that have progressed drug law reform, whether decriminalisation of all drugs for personal supply, like Portugal[48], regulated markets for cannabis, like Canada’s[49], or other regulated drug markets, like Uruguay’s.[50]
But in doing this, we must start applying the general principle that any drug law reform should be carefully managed and driven by experts, which must include people who use drugs, their families and people who work with them.
Evidence-Based Harm Reduction
The scale of the drug deaths crisis demands that we use every tool available to us to improve and save lives. Immediate and bold action is needed to seize the opportunities available. In recognition of the public health emergency we face, urgent legislation is needed to deliver rapid, targeted and meaningful action while considering the longer term reform of our drug laws, including the Misuse of Drugs Act 1971. These are changes which should be implemented without delay.
Illicit drugs are currently regulated according to classification systems that purport to relate to the harms and risks of each drug. However, in fact, classification is often driven by other factors. A 2007 study by Professor David Nutt, et al, noted that “the methodology and processes underlying classification systems [were] generally neither specified nor transparent, […] thus reducing confidence in their accuracy and undermin[ing] health education messages. […] The ranking of drugs produced by [Prof. Nutt’s] assessment of harm [within this study] differed from those used by current regulatory systems”.[51]
The Advisory Council on the Misuse of Drugs (ACMD)[52] should in the first instance be empowered to review the drug classification system, exploring whether the current classification is in line with the most up to date evidence and, if appropriate, develop a new system of classification based on the scientific consensus of their harm, rather than cultural norms or political discourse. Within this framework, all drugs must be considered on a case by case basis and this assessment must be evidence-based and fully transparent. Classification should therefore be the result of a transparent weighing of the evidence on harms, not politics.
In addition to this review of classification, there are many critical changes that the UK Government could make now, in favour of a public health approach, to tackle Scotland’s drug deaths crisis. These are changes that already have an established evidence base. Through targeted legislation some legal barriers could be removed and other harm reduction measures could be placed on a clear statutory footing.
As the Scottish Government has consistently called for, a statutory framework could be created under which Supervised Drug Consumption Facilities (SDCFs) would operate across Scotland, providing a supervised and safe space for people who use drugs and giving immediate benefits for individuals, their families and the wider community.[53],[54] In the meantime, a request for a statement of prosecution policy is currently being considered by the Lord Advocate as part of a proposal to establish a SDCF in Glasgow within the existing legal framework. However, in the absence of a change to, or exemption under, the Misuse of Drugs Act 1971, such a facility would be constrained in ways that SDCFs in other countries are not.[55]
The evidence supporting SDCFs around the world is extensive with 16 countries with legal and operational drug consumption rooms in 2022.[56] The International Narcotics Control Board has recognised the role of SDCFs where the facilities “ultimate objective of these measures is to reduce the adverse consequences of drug abuse” and where they are operated “within a framework that offers treatment and rehabilitation, as well as social reintegration”.[57]
An extensive and easily accessible drug checking network, including low threshold front of house services like in New Zealand[58] and Canada[59], could be introduced as one of the most effective measures available to reduce harms and prevent overdoses. These services provide additional opportunities to engage individuals in treatment and accurate public health surveillance, enabling faster responses to dangerous substances.[60]
Clarification could be made to the law to ensure that services can provide all drug paraphernalia legally as, without it, people who take drugs may use makeshift and inadequate alternatives, such as unsafe inhalation equipment. This can potentially cause harms, for example, cuts and burns, blood-borne viruses, respiratory and wound infections.[61],[62] There is robust evidence that these measures do not encourage drug use or criminal activity[63], and that such programmes improve the odds that people who use drugs will seek and engage with treatment.[64]
The above changes are all low threshold interventions, which would provide additional opportunities for individuals to engage with treatment and support. As low threshold interventions, they will only be as effective as they can be if the whole system of care incorporates these interventions, providing wrap around support for individuals and ensuring that the legal framework supports their operation.
Existing licensing powers could be utilised to enable and actively encourage a full suite of treatment options, including the expansion of Heroin Assisted Treatment services where needed, as an effective treatment for those whose addiction persists even after receiving conventional treatment and care services[65], evidenced by the existing Enhanced Drug Treatment Service in Glasgow.
The reclassification of naloxone from a Prescription Only Medicine (POM) to a Pharmacy (P) or General Sales List (GSL) medicine would increase access to this lifesaving medicine to reverse the effects of an opioid overdose. The UK Government ran a consultation from May to September 2021 on ‘Expanding access to naloxone’.[66] Many organisations, including the Scottish Drug Deaths Taskforce[67], submitted responses calling for a relaxation of the regulations around naloxone, outlining how this could save lives. In the UK Government’s summary of feedback they identified “overwhelming support for allowing more organisations and individuals to supply take-home naloxone” and committed to “expanding access to naloxone” and working with the devolved governments to take this forward.[68] The UK Government’s formal response to the consultation will be published later this year and we look forward to working with them to improve access to this life saving intervention.
Outwith the Misuse of Drugs Act 1971, the exemption in regulation 3 of the Equality Act (Disability) Regulations (2010) excludes addiction from the health conditions covered by the protected characteristic of disability. Removing this would ensure people can better access, without discrimination, to the support they need to fully engage with treatment and recovery services.[69]
Taken together, the steps outlined above would create a meaningful, legislative shift towards a public health approach, such as many countries have already embarked on across the world.
Decriminalisation for Personal Use
To improve and save lives, we must be innovative, bold and radical. We are clear that nothing should be considered off the table. We must start by recognising that no country, anywhere in the world, has succeeded in eliminating drug use. As the UN High Commissioner for Human Rights has said, “decades of punitive war on drugs strategies have failed to prevent an increased range and quantity of substances produced and consumed.”[70] However, other countries have demonstrated alternative ways of tackling problematic substance use with care and compassion, recognising the complex causes of drug use.
We know that, through its illicit nature, much of Scotland’s drug use is hidden.[71] Its illegality contributes to the stigma and discrimination people face.[72],[73] This stigma is most acutely felt in our most deprived communities, where people are more than 15 times more likely to die as a result of drugs than those in the least deprived.[74] Approximately half of patients with a drug-related hospital stay live in the most deprived areas of Scotland.[75] Punishing people for addiction isolates them, resulting in further significant harms for both them and their communities.[76] Intervention can break a cycle of regular interactions with the justice system.[77] In the financial year 2020/21, there were 35,410 drug crimes recorded by Police Scotland.[78] We need to treat people with respect and give them hope, providing treatment and support to enable them to address the complex needs they may be experiencing.
Using the evidence from other countries,[79] decriminalising drugs for personal use would help and support people rather than criminalise and stigmatise them; freeing individuals from the fear of accessing treatment and support, reducing drug related harms and, ultimately, improving lives.
In addition to these critical public health benefits, people who use drugs would no longer be channelled into the criminal justice system, reducing the costs to the justice system. Decriminalisation could result in fewer people being imprisoned[80] and free up law enforcement resources to address other priorities.
Decriminalisation is no longer as radical a proposal as it was. In fact, thirty countries around the world have now recognised the harm caused by criminalisation and moved to change their drug laws, in different ways and with varying levels of effectiveness.[81] In 2018, the UN Chief Executives Board, which includes the head of every UN agency agreed the first ‘UN common position supporting the implementation of the international drug control policy through effective inter-agency collaboration’. The common position committed “to promote alternatives to conviction and punishment in appropriate cases, including the decriminalization of drug possession for personal use, and to promote the principle of proportionality, to address prison overcrowding and overincarceration by people accused of drug crimes”.[82]
While there are many factors that have an impact on drug use and substance issues – including social, cultural and economic factors – evidence indicates that decriminalisation directs more people into treatment, reduces criminal justice costs, and reduces the negative impact that a criminal conviction can have on a person who uses drugs.[83] While the research base is complex, limited and growing rapidly, the majority of studies on decriminalisation have found that people’s usage tends to remain the same[84] and in cases where usage does increase, the change is generally small and may be limited to adults rather than young people.[85]
Portugal is often cited as a potential model of decriminalisation. In 2001, it changed its drugs policy with the aim of fighting the health problem, not the patients. It implemented decriminalisation as part of a wider harm reduction and treatment policy package; not only changing the law but investing in prevention, social education, treatment and rehabilitation.[86]
In calling for decriminalisation for personal use, we recognise that it would not solve our drug crisis by itself. But it could provide a framework within which we can better pursue our existing policies to help, treat and support people rather than criminalise, stigmatise and fail them. In implementing any policy we will learn from other countries to ensure we legislate in a way that optimises public health benefits, while minimising any unintended consequences.
Potential for Strict Regulated Supply
Decriminalisation for personal supply, as with prohibition, provides no additional control over the market and essentially continues to leave it in the hands of organised crime. It continues to provide revenue to fund other illegal activity, further driving violence and crime in our communities. It also accepts that there can be no quality or safety controls on the substances people are consuming, something we simply wouldn’t accept with other, legal and regulated harmful products like alcohol or tobacco.
While we do not currently advocate for this policy, implementing a more evidence-based approach to drugs policy could be the basis for considering the potential of introducing regulated markets for the reduction of harm and the safe control of substances. This could be supported by a Citizens’ Assembly to consider the evidence and give a perspective from a representative sample of the public. This would enable a mature, informed conversation about the level of regulation and control that we as a society are comfortable with for substances, based on an expert assessment of their relative harms.
A debate of this kind could consider the many ways in which substances could be regulated, including licensed sales, expanded pharmacy provision or state run monopolies and the means for achieving this. Which measures are most appropriate for which drug should be determined by the evidence. A considered, methodical and cautious approach would be essential. In Canada’s regulated cannabis market a staged approach was taken, introducing new products slowly over time.[87] Starting with strict regulation allows for the possibility for later easing, if and when evidence and evaluation proves that it is safe to do so.
Other themes to explore include what can be learned from regulatory measures in existing markets of legal substances. These could include age restrictions and laws to prevent driving under the influence, requiring strict enforcement to prevent harms. Measures like price controls, proven effective with Minimum Unit Pricing for alcohol[88],[89], regulation of advertising, branding and sponsorship, and providing consumers with accurate information on the effects, preparation, storage, side effects, risks and where to access support.[90],[91] Legislation would of course be needed to control and monitor the production, supply, sale and consumption of newly regulated substances.
The war on drugs and the UK’s approach has disproportionately criminalised minority ethnic communities and those from disadvantaged backgrounds.[92] If the decision was made to move towards strict regulated supply then a debate could examine steps to redress the harms of punitive prohibition, potentially including measures to expunge relevant criminal convictions.
Conclusion
The overarching ambition of the Scottish Government National Mission is to reduce deaths and improve lives. Our objective is that no person finds themselves dependent on substances, but that if they do, they should be supported and not criminalised for that health condition. These objectives will continue to drive our drugs policy regardless of the legal framework in which we operate and we will work tirelessly to reduce drugs harms within the powers devolved to Scotland. There is much more we can and will do to reduce deaths and improve lives within those powers.
In addition to that essential work, this paper argues for a new way of developing our drug laws, one which is based on evidence, the experience of those on the front lines, as well as those with lived, living and family experience, and that involves citizens in its development. It sets out a caring and compassionate approach to our drug laws, which is grounded in human rights and would allow for the provision of safe, evidence-based harm reduction services. It also argues for transition towards decriminalisation for personal use, which we argue would enhance our National Mission on drug deaths, removing legal barriers that currently restrict progress. In the future, an evidence-based approach could even support a national conversation about whether Scotland could consider strictly regulated drugs markets that were evidence-based, cautious and led by our overarching principles.
A fairer, safer and healthier country must care about all its citizens and be inclusive of those with health conditions such as drug dependence. Future generations, our children and grandchildren, have a right to health and happiness. They have the right to live in a country where they are helped and supported, not stigmatised and punished for their health conditions.
These proposals present an opportunity to do something different, something bold, progressive and evidence-based which would make a real difference to people’s lives. They build on the international evidence, and set out a policy based on human rights, that prioritises interventions that will work.
Independence or further devolution would provide the opportunity to implement these policies, but these changes are not dependent on constitutional changes. We stand ready to engage with the UK Government on meaningful drug law reform to improve the lives of people who use drugs, their families and our communities.