Cancer prehabilitation survey: findings report
Summarises the findings from a survey of stakeholders and service providers about cancer rehabilitation and rehabilitation services in Scotland
4 Prehabilitation Findings
4.1 Attitudes and Awareness
This theme discusses attitudes among all survey respondents about the importance of prehabilitation; and their awareness of the 'Key Principles' for Cancer Prehabilitation.
4.1.1 Importance of Prehabilitation
Respondents were asked about the importance of prehabilitation interventions for people about to undergo cancer treatment. 154 out of 187 potential respondents (82% of the sample) answered this question, with findings shown in table 2.
| Importance of Prehabilitation | number of responses | % of responses to this question | % of survey respondents |
|---|---|---|---|
| 1 = Not Important At All | 0 | 0% | 0% |
| 2 | 1 | 1% | 1% |
| 3 | 9 | 6% | 5% |
| 4 | 54 | 35% | 29% |
| 5 = Crucial | 90 | 58% | 48% |
| No Response | 33 | 18% | |
| Total Responses to this Question | 154 | 100% | 100% |
Of those who answered the question, 94% selected 4 or 5, indicating that they attached high importance to prehabilitation. This finding was similar for all three cancer networks. 58% of those respondents selected 5, 'crucial', similar to the equivalent 2019 findings (47%). 18% of survey respondents did not answer this question, implying that they did not know.
4.1.2 Awareness of the 'Key Principles for Implementing Cancer Prehabilitation in Scotland'
Respondents were asked to rate their awareness of the 'Key Principles', published in April 2022. All 187 survey respondents answered this question.
- 41% of respondents selected 4 or 5 (high awareness).
- 21% of respondents selected 3 (medium awareness).
- 38% of respondents selected 2 or 1 (low awareness or not aware at all).
There was some variation among the cancer networks. For the SCAN and WoSCAN networks, over 40% of respondents selected 4 or 5 (high awareness), whereas for the NCA this figure was 33%.
Respondents with services in their local area (see Section 4.2) were more likely to have high awareness of the 'Key Principles'.
The extent to which respondents considered that the eight principles underpinned local service delivery is discussed under the themes below.
4.2 Service Availability and Resourcing
This theme discusses the availability of local prehabilitation services, changes since the start of the COVID-19 pandemic and plans to introduce new services. It also covers the key resourcing issues of staffing and funding.
4.2.1 Availability of Local Prehabilitation Activities
Respondents were asked whether any cancer prehabilitation activities were being offered in their local area.
186 out of 187 survey respondents answered this question. Around half said that prehabilitation activities were offered in their local area, as shown in Table 3.
| Prehabilitation Activities offered in local area? | Number of Responses | % of Responses to this Question |
|---|---|---|
| Yes | 95 | 51% |
| No | 28 | 15% |
| Don't Know | 63 | 34% |
| Total | 186 | 100% |
The same question was asked in the 2019 survey. 2022 findings show a small numerical and large percentage increase in the offer of local activities. Comparisons are shown in Chart 1 below.
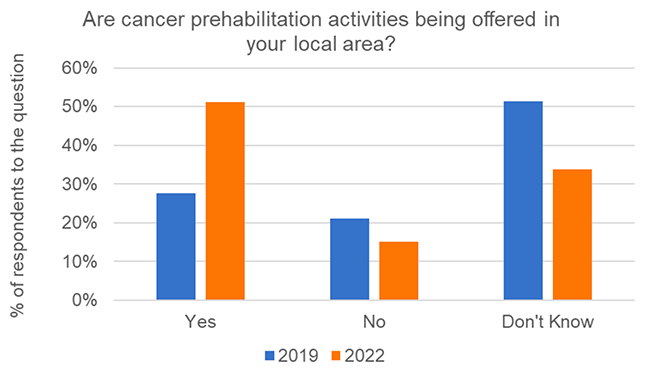
The lower percentage of those answering 'Don't know' in the 2022 survey could indicate a survey bias, with those aware of or interested in prehabilitation more likely to participate. An alternative explanation is that results might indicate an increase in awareness and/or availability of prehabilitation services since 2019. As noted in Section 1, there are limitations on comparisons between the 2019 and 2022 survey findings.
A breakdown by cancer network is shown in Table 4. WoSCAN respondents reported more local services than the other networks in both 2019 and 2022, with the NCA showing the biggest increase (numerical and percentage) in respondents with local services.
| Cancer Network | 2019 | 2022 |
|---|---|---|
| NCA | 6 | 23 |
| SCAN | 23 | 19 |
| WoSCAN | 49 | 53 |
| Total | 78 | 95 |
Respondents with locally available prehabilitation services (n = 95) were asked further questions about the availability and resourcing of those services.
4.2.2 Changes since the start of COVID-19
Respondents with local prehabilitation services were asked about changes in local activities since the start of the Covid-19 pandemic. 85 out of 95 potential respondents answered this question.
Many respondents discussed how a number of services were stopped completely, scaled back, or their progress was slowed due to the pandemic. However, they also mentioned how these activities were now resuming or increasing. Some new services were highlighted as positive developments even if they were starting on a small scale or as pilot projects. Examples of new services included:
- A new service for lung cancer patients, which was delayed by the pandemic.
- A new dietitian post for gynaecological cancers.
- Funded psychological support allocated to Maggie's who deliver it to urology patients.
- A funded dedicated physiotherapy service.
- A new small-scale service for people with advanced lung cancer.
- A new link with a local authority leisure service to establish a pathway.
4.2.3 Delivery Mode
Following the onset of the COVID-19 pandemic, many services switched from face to face to phone or video appointments as appropriate. This experience informed the resumption of some services in hybrid / blended delivery modes. Respondents commented positively that the use of video increased access for some groups, for example those living in remote or rural areas. However, it was also acknowledged that video is not appropriate for others, such as some older people, those who are digitally excluded, or people whose suitability for exercise programmes needs to be assessed in person. Respondents believed that face to face services would still be needed for some groups such as these.
4.2.4 Staffing
Respondents were asked what staff or volunteers were involved in the delivery of prehabilitation activities in their local area. 90 out of 95 potential respondents answered as shown in Table 5.
| Staff / Volunteer Role | % of Respondents to this Question who selected this option |
|---|---|
| Nurse | 61% |
| Dietitian | 51% |
| Physiotherapist | 47% |
| Clinical Psychologist | 32% |
| Fitness Instructor (Local Authority/Move More etc.) | 28% |
| Occupational Therapist | 20% |
| Volunteer/Buddy/Peer Supporter | 19% |
| Counsellor | 13% |
| NHS Technical Instructor/Support Worker | 8% |
Nurses, dietitians, and physiotherapists were the staff roles most likely to be identified by respondents as involved in the delivery of activities.
Compared with 2019, the most notable increases were in the proportion of respondents selecting:
- Dietitian (from 30% in 2019 to 51%).
- Clinical Psychologist (from 11% in 2019 to 32%).
- Counsellor (from 2.5% in 2019 to 13%).
- Fitness Instructor (from 20% in 2019 to 28%).
There was a smaller increase in mentions of Physiotherapist (from 43% in 2019 to 47%).
Of 'Other' roles, Maggie's staff were mentioned most frequently.
Involvement of staff delivering all three prehabilitation modes was reported by 19% of respondents, as shown in Table 6. Many also responded that a nurse and other staff were involved too.
| Prehabilitation Modes | % of Respondents to this Question |
|---|---|
| Physical Fitness: Physiotherapist and/or Fitness Instructor | 65% |
| Nutrition: Dietitian | 51% |
| Psychological Support: Clinical Psychologist and/or Counsellor | 35% |
| Responses showing staff from all 3 modes | 19% |
Qualitative findings from open questions highlighted staffing as a major theme. Staff shortages, heavy workload, and pressures on existing staff; and challenges in attracting and retaining staff, both in general and for temporary prehabilitation projects, were cited as barriers to supporting prehabilitation. Some respondents suggested that designated staffing for prehabilitation work was needed.
Respondents also mentioned pressures on broader health services, such as long waiting lists and insufficient clinical space, which made services difficult for people to access. Services were said to be reactive and focused on crisis management, rather than on prevention and prehabilitation.
4.2.5 Funding
Respondents were asked what type of funding their prehabilitation activities received. 94 out of 95 potential respondents answered that question as shown in Table 7.
| Type of Funding | Number of Responses | % of Responses to this Question |
|---|---|---|
| Permanent funding | 2 | 2% |
| Temporary funding | 37 | 39% |
| I don't know about funding | 40 | 43% |
| No funding | 15 | 16% |
| Total | 94 | 100% |
Compared with the 2019 findings, the percentage of permanent funding shows a notable decrease, down from 16% to 2% (2 responses). Review of those 2 responses showed that, in both cases, the permanent funding was for specific services which were not part of a comprehensive prehabilitation programme.
There has been a considerable increase in temporary funding (from 17.5% in 2019 to 39%). 65% of respondents with temporary funding stated that it was expected to end in 2022 or 2023 or had ended already.
The proportions with no funding and who did not know were similar to those in 2019.
Funding and resources, including staffing, were strong interrelated themes in response to open questions in this survey, as also reflected in the 2019 survey. Respondents discussed the need for dedicated and permanent funding to develop sustainable prehabilitation services.
Potential influences on future resourcing of prehabilitation, both funding and staffing, could include senior leadership and buy-in for prehabilitation (discussed in Section 4.3), and the availability of evidence about the outcomes of prehabilitation (see Section 4.6).
4.2.6 Introduction of New Prehabilitation Activities
All survey respondents were asked about plans to introduce or add to local prehabilitation activities. 27% of those who answered this question said there were such plans but two thirds did not know. Details are shown in Table 8.
| Plans to introduce / add to local activities? | Number of Responses | % of Responses to this Question |
|---|---|---|
| Yes | 50 | 27% |
| No | 12 | 7% |
| Don't Know | 122 | 66% |
| Total Responses to this Question | 184 | 100% |
There was some variation across cancer networks. NCA respondents were most likely to be aware of plans to introduce or add to local activities (31%), with SCAN respondents least likely (23%). The proportion for WoSCAN was 27%.
4.3 Service Delivery and Pathways
Respondents with locally available prehabilitation services (n = 95) reflected on specific aspects of prehabilitation service delivery in their area, where improvement could enhance the future effectiveness of local services. Some of the 'Key Principles' are used to frame the discussion about those findings.
4.3.1 Local Delivery underpinned by 'Key Principles for Implementing Cancer Prehabilitation'
Respondents were presented with a series of statements about the eight 'Key Principles' and asked to what extent they agreed that each principle underpinned the delivery of prehabilitation activities in their local area. For each statement, 94 or 95 out of 95 potential respondents answered the question.
The highest level of agreement was with the statement "Prehabilitation activities are multi-modal including exercise/activity, nutrition and psychological support", with 61% of respondents agreeing (including strong agreement).
About half of respondents agreed with the 4 statements below.
- "Prehabilitation activities start as early as possible and in advance of any cancer treatment" (46% agreed).
- "Prehabilitation activities run in parallel with usual decision-making processes so it does not have an adverse effect on cancer waiting times nor delay the start of treatment" (55% agreed).
- "Prehabilitation activities are part of the rehabilitation continuum" (45% agreed).
- "Completion of prehabilitation screening should be recorded at cancer multidisciplinary team alongside performance status" (47% agreed)".
Three statements had fairly low levels of agreement. These were:
- "All patients are screened to determine the level of prehabilitation required (universal, targeted, specialist)" (23% agreed).
- "All patients (receiving universal, targeted and specialist interventions) have a co-produced personalised prehabilitation care plan" (21% agreed).
- "Validated tools are used for individualised assessment, care planning and outcomes measurement when patients are receiving targeted and specialist interventions" (16% agreed).
Some of these principles are used to frame the discussion below about specific aspects of service delivery.
4.3.2 Referrals
Respondents were asked if they personally referred people to prehabilitation activities and how routinely they did so. 95 out of 95 potential respondents answered, with a breakdown of responses in Table 9.
| Referral to Prehabilitation Activities? | Number of Responses | % of Responses to this Question |
|---|---|---|
| Yes | 35 | 37% |
| No | 38 | 40% |
| I provide prehabilitation services | 22 | 23% |
| Total Responses to this Question | 95 | 100% |
60% of respondents reported that they either referred to or provided prehabilitation services. These findings are similar to the 2019 survey (which included a 'not applicable' response option).
34 out of 35 potential respondents (those who answered Yes) also answered the follow-up question about how routinely they refer people.
- 41% selected 4 or 5 (more likely to or always refer).
- 38% selected 3 (medium likelihood of referring).
- 21% selected 1 or 2 (less likely to refer).
Qualitative findings from the open questions highlighted the timeliness of referrals as a key issue, which had already emerged in the 2019 survey. This links to the 'Key Principles' that "Prehabilitation activities start as early as possible and in advance of any cancer treatment;" and that "Prehabilitation activities run in parallel with usual decision-making processes, so it does not have an adverse effect on cancer waiting times nor delay the start of treatment."
While it was acknowledged that waiting lists offered an opportunity for prehabilitation interventions, more commonly respondents commented that referrals were not made automatically or were made late. Since treatment should not be delayed and taking into account waiting time targets, this meant that there was often insufficient time to provide prehabilitation interventions before treatment. The need for earlier screening, identification and offer of prehabilitation was highlighted, as well as appropriate referral to universal, targeted and specialist services.
Respondents were asked to share their thoughts on how local pathways could be changed to support prehabilitation. Some stated that prehabilitation services were integrated in patient pathways, with staff routinely screening and referring or signposting patients to appropriate services. Others reported that their local services were not working in this way, with comments that referrals were not always timely. It was suggested that the Single Point of Contact approach, pathway navigators and cancer support workers could support this process.
4.3.3 Screening, assessment and care planning
Respondents were asked if their local prehabilitation service was screening or triaging patients for perceived risk associated with each of the three modes of Nutrition, Physical Activity and Psychological Need. This links to the 'Key Principles' that "All patients are screened to determine the level of prehabilitation required (universal, targeted, specialist);" that "Validated tools are used for individualised assessment, care planning and outcomes measurement when patients are receiving targeted and specialist interventions; and that "All patients (receiving universal, targeted and specialist interventions) have a co-produced personalised prehabilitation care plan."
Of the 95 respondents with local services, 71% responded that their service screened for one or more of the three modes. For each separate mode, just under half of respondents indicated that patients were screened or triaged. Details are shown in Table 10.
| Screening or triaging patients for perceived risk associated with: | % responding 'Yes' |
|---|---|
| Nutrition | 44% |
| Physical Activity / Exercise | 46% |
| Psychological Need | 43% |
| Any mode (n = 67 respondents) | 71% |
| None of the modes (n = 28 respondents) | 29% |
A breakdown of the 67 respondents whose service was screening for any of the three modes is shown in Table 11. Half of those respondents said that their local service was screening for all three modes, representing 22% of respondents with local services.
| Service screening for: | Number of Respondents | % of Total | % of respondents with a local service |
|---|---|---|---|
| all 3 modes | 21 | 50% | 22% |
| 2 modes | 16 | 31% | 17% |
| 1 mode | 30 | 19% | 31% |
| Total | 67 | 100% | 71% |
In response to open questions, respondents highlighted the need for the involvement of all three modes in prehabilitation services. This links to the 'Key Principle' that "Prehabilitation activities are multi-modal including exercise/activity, nutrition and psychological support." Although responses to some questions suggested that multi-modal interventions were relatively common, some respondents commented that existing interventions did not involve all three modes or that these were not linked to each other.
Respondents whose service was undertaking screening were invited to describe how it was doing this; they responded as follows.
Nutrition
Common approaches to screening included using MUST (Malnutrition Universal Screening Tool), or assessments of weight or appetite change. Less common tools mentioned included the 'Eat Well Age Well' tool for non-clinicians and a frailty screening tool. Respondents reported that screening most often took place through an assessment but that this could be over the phone or during a discussion. Professions highlighted as involved in the screening included Clinical Nurse Specialists, GPs, Physiotherapists and Dietitians. Referrals mostly went to community or specialist dietitians for onward treatment.
Physical Activity / Exercise
Many responses mentioned consultations or assessments as a means of undertaking physical activity screening. These often included validated tools or objective measures, such as the DASI (Duke Activity Status Index) functional capacity calculator, BMI (Body Mass Index), frailty scores. Clinical Nurse Specialists and Physiotherapists were commonly mentioned as carrying out the screening although other professions were also noted, including Consultants, GPs, and Occupational Therapists. The outcome of screening often involved referral to a physical activity service, which might be provided by the third sector (e.g., Move More) or a local authority.
Psychological Need
Screening processes were described for low mood, anxiety or depression, or for support needs. These were typically undertaken using a clinical assessment or health needs assessment, involving tools like the EQ-5D (Health-Related Quality of Life). However, a couple of responses mentioned that screening for psychological support is part of a broader, holistic assessment of support needs. More conversational or informal assessments were noted by a few respondents.
In many examples given, respondents used the terms screening and assessment interchangeably, although they are different processes with different purposes. No detail was provided about care planning.
4.3.4 Rehabilitation Continuum
This sub-theme links to the 'Key Principle' that "Prehabilitation activities are part of the rehabilitation continuum." 62 respondents had both local prehabilitation and rehabilitation services, representing around two thirds of respondents with either local service. Analysis of responses from this group showed that around half agreed that this principle underpinned their local services. However most did not describe how their local continuum worked in practice, so the extent to which their patients moved along a seamless pathway was not clear. This could be because of respondents' limited awareness or because the survey did not ask about the rehabilitation continuum explicitly. Some responses suggested that a continuum was in place to some extent, but in some cases this applied only to one prehabilitation mode. A few respondents who did describe service delivery throughout the cancer journey were mainly from third sector organisations which provided both prehabilitation and rehabilitation services. Some respondents highlighted the need for improvement in this area.
4.3.5 Leadership and Management
Leadership and management were mentioned in relation to how local pathways could be changed to support prehabilitation. Some respondents discussed the need for senior-level leadership and buy-in for prehabilitation in principle, setting the tone for less senior staff. This issue could also link to the service availability and resourcing theme (see Section 4.2), if senior-level buy-in led to the provision of longer-term funding and sustainable staffing.
Other respondents emphasised the need for local management and co-ordination of the practical aspects of service delivery.
4.3.6 Consistent Programmes and Guidance
Some respondents highlighted the need for consistent programmes and guidance, in line with the 2019 survey. A few respondents suggested developing a formalised prehabilitation intervention and guidance for a consistent local offer by all prehabilitation services.
While many of the above themes show similarities with findings from the 2019 survey, they also reflect challenges in the NHS and cancer services landscape which have arisen since then. Particular challenges arising from and following the COVID-19 pandemic include broader pressure on health services including staff shortages and long waiting lists, as discussed in Section 4.2.
4.4 Access to Services
Respondents with local prehabilitation services (n = 95) discussed the location of and access to prehabilitation services; and the need for equitable access to services.
4.4.1 Access to Services
Location of intervention: it was suggested both that services should be based in hospitals to facilitate patient access at initial referral, and that services should be available in community facilities which would be more accessible to patients receiving interventions. The need to address geographical inequalities was also mentioned in the context of the location of interventions and availability of transport.
Patient access: some respondents commented on the general need to improve access to services for patients and their families, by increasing their awareness about prehabilitation and by making access easier and more flexible.
4.4.2 Equity and Inequalities
Respondents commented on the challenge of providing services across remote and rural areas, and for island residents. The need to provide equitable services for all tumour groups was also highlighted. Respondents also thought socio-economic inequalities needed to be addressed, in terms of the likelihood of people engaging with services and the affordability of some services, such as exercise sessions.
As discussed in Section 4.2, some respondents highlighted the need to consider the potential impact of service delivery mode on equity of access. They noted that video consultations are not appropriate for some groups, such as people who are digitally excluded, who might also be experiencing other inequalities.
4.5 Communication and Collaboration
Respondents with local prehabilitation services (n = 95) reflected on communication and collaboration between services, including with regard to their local MDT and with local third sector projects.
4.5.1 Multidisciplinary Team (MDT) Engagement
This sub-theme links to the 'Key Principle' that "Completion of prehabilitation screening should be recorded at multidisciplinary team alongside performance status." Findings which contributed included responses to a question about how closely staff providing prehabilitation worked within the care team and patient pathway, for example in an MDT.
Around 40% of respondents to this question explicitly mentioned or alluded to the MDT, though not specifically to MDT meetings. Around half of those discussed prehabilitation services integrated within the local MDT or working closely with it. The other half commented on services not being part of the MDT and not linked into it.
Some respondents described MDT involvement as an important enabler of an effective pathway. Respondents cited the need for improved MDT awareness and understanding of prehabilitation; improved communication between service providers; and improved MDT links with third sector services. A few respondents commented that their local MDT was not comprehensive in terms of including all key professions and all three prehabilitation modes.
Where prehabilitation falls outside MDTs or is spread across services, there were some positive comments about communication and collaboration, but others that there was need for improvement. Respondents reflected on the need for improved communication among staff, including between primary and secondary care and with third sector and local authority service providers. The importance of improving staff understanding of the benefits of prehabilitation was also highlighted. They also mentioned the need for improved communication with patients, including about how prehabilitation could benefit them.
4.5.2 Collaboration with Third Sector Organisations
Several respondents mentioned specific third sector projects, mainly the Maggie's pilot projects and Macmillan/ICJ projects. NHS respondents in particular highlighted partnership working with such projects as a potential enabler of effective prehabilitation. However awareness of these projects and working relationships with them varied. While a few respondents mentioned a close working relationship, most suggested a more distant working relationship. They stated or implied that local prehabilitation was something separate undertaken by Maggie's and that the MDT was not involved.
4.6 Monitoring, Evaluation and Outcome Measurement
Respondents with local prehabilitation services (n = 95) were asked how patient uptake, adherence and experience were monitored; and how patient outcome measures were used to determine the effectiveness of those services.
4.6.1 Monitoring and Evaluation
Many respondents were uncertain about whether and how monitoring was undertaken. Monitoring processes mentioned included recording patient referrals, uptake and attendance; and feedback forms or questionnaires.
Patient uptake.
Monitoring processes described often involved recording patient referrals and uptake on a database (e.g., a spreadsheet or software system). A couple of responses mentioned monitoring demographic information and patient impact or outcomes. Few mentioned how the data were used. Some responses highlighted regular reporting of the data, which appeared to be for local monitoring purposes.
Patient adherence.
There was a lot of uncertainty about whether patient adherence was monitored within local programmes. Several respondents reported on activities which were stand-alone sessions and so this was not applicable. Others commented that monitoring was undertaken by Maggie's projects. Where data were recorded this was primarily in the form of statistics such as attendance figures. A few respondents mentioned more qualitative information such as feedback or diary information being used.
Patient experience.
Many respondents were unsure about whether or how patient experience was monitored. For those that did provide information, feedback forms or a questionnaire or survey was a common approach. These were offered at the end of an intervention, at a specific point (e.g., after surgery), or at multiple points. A few mentioned collecting information informally. Case studies, stories and focus groups were also mentioned but less often as ways of monitoring patient experience.
4.6.2 Outcome Measurement
This links to the 'Key Principle' that "Validated tools are used for individualised assessment, care planning and outcomes measurement when patients are receiving targeted and specialist interventions."
Respondents were asked if outcome measures were being used to determine the effectiveness of their prehabilitation activities. 90 out of 95 potential respondents answered, as shown in Table 12.
| Use of Outcome Measures? | Number of Responses | % of Responses to this Question |
|---|---|---|
| Yes | 33 | 35% |
| No | 14 | 15% |
| Don't know | 41 | 43% |
| Not applicable | 7 | 7% |
| Total Responses to the Question | 95 | 100% |
The proportion answering 'Yes' (35%) was lower than the 2019 finding (55%).
Respondents highlighted a wide range of measures, similar to those mentioned in the 2019 survey. They included objective measures such as of muscle strength and Body Mass Index (BMI); patient-reported outcome measures and service-level outcomes. Some measures mentioned by respondents would be regarded as process measures or screening tools.
For Physical Activity / Fitness, the most frequent mentions were of Sit to Stand assessments, measures of grip strength and the self-reported GLTEQ (Godin Leisure-Time Exercise Questionnaire).
For Nutrition, measures mentioned included oral nutritional supplement usage, feed usage and dietetic care duration.
For Psychological Status, several measures were mentioned by one or two respondents. CORE-10 (Clinical Outcomes in Routine Evaluation) and MYCAW (Measure Yourself: Concerns & Wellbeing) were each mentioned twice.
Patient-reported outcome measures such as the multi-dimensional EQ-5D (Health-Related Quality of Life) were also mentioned, as was patient feedback on satisfaction with services and on quality of life.
Some respondents acknowledged the general need for better monitoring, evaluation, and outcome measurement to demonstrate the benefits of prehabilitation.
Outcome measurement could link to the service availability and resourcing theme (Section 4.2). Evidence that prehabilitation leads to positive outcomes could help make the case for longer-term funding and sustainable staffing.
4.7 Prehabilitation 'Key Principles': Summary of Findings
This section discusses, for each of the 'Key Principles', findings from the survey question about the extent to which the principle underpinned delivery of local prehabilitation activities. This question was available to all survey respondents, with and without local services. This section also draws on relevant qualitative findings derived from responses to open questions by respondents with local services.
4.7.1 Prehabilitation should start as early as possible and in advance of any cancer treatment
Around half of respondents agreed or strongly agreed that this principle underpinned local activities. However many respondents commented that broader system pressures and staffing shortages could delay the start of prehabilitation.
4.7.2 Prehabilitation should run in parallel with usual decision-making processes, so it does not have an adverse effect on cancer waiting times nor delay the start of treatment
Around half of respondents agreed or strongly agreed that this principle underpinned local services. Several respondents commented that referrals were not made automatically or were made late, which meant that there was often insufficient time to provide prehabilitation interventions before treatment.
4.7.3 Prehabilitation should be part of the rehabilitation continuum
Around half of respondents agreed or strongly agreed that this was the case in their local area. However most respondents with local services did not describe how their local continuum worked in practice, so it was not clear whether it worked seamlessly for patients. Some respondents highlighted the need for improvement in this area.
4.7.4 Prehabilitation should be multi-modal including exercise/activity, nutrition, and psychological support
There were mixed findings on this issue. Around 60% of all respondents agreed or strongly agreed that this was happening in their local area. It appeared that this situation had improved since 2019, with increased involvement of staff groups which delivered the three prehabilitation modes.
Of the 95 respondents with local prehabilitation services, 71% responded that their local service screened for one or more of the three modes. Of those respondents, half said their service was screening for all three modes, which represented 22% of respondents with local services. Some qualitative findings suggested that existing services did not involve all three modes or that these were not linked to each other.
4.7.5 All patients should be screened to determine the level of prehabilitation required (universal, targeted, specialist)
Only a minority of respondents (23%) agreed or strongly agreed that this principle underpinned local services. Respondents acknowledged the importance of early screening and identification of patient needs.
4.7.6 Completion of prehabilitation screening should be recorded at MDT alongside performance status
Around half of respondents agreed or strongly agreed that prehabilitation screening was recorded at their local MDT. Respondents highlighted the MDT as an important enabler of effective prehabilitation services, but there were mixed views on the extent to which such services were integrated or working closely with local MDTs.
4.7.7 Targeted and specialist interventions demand the use of validated tools for individualised assessment, care planning and outcomes measurement
Only 16% of respondents agreed or strongly agreed that this principle underpinned local services.
4.7.8 All patients should have a co-produced personalised prehabilitation care plan
Only a fifth of respondents agreed or strongly agreed that this principle was a reality for local patients.
Contact
Email: socialresearch@gov.scot