People who self-harm: rapid evidence review and survey of practitioner perspectives
This rapid evidence review and survey of practitioner perspectives investigated if self-harm can be a barrier to accessing support and services, and what measures can be taken to overcome these barriers.
Survey of Practitioner Perspectives
Methodology
As part of this research, a survey was carried out to gather practitioner perspectives on the barriers faced by individuals who self-harm when accessing support and services. The survey provides evidence to support an action from the Self-Harm Strategy and Action Plan:
“Investigating if self-harm can be a barrier to accessing support and services, and what measures can be taken to overcome these barriers” (Priority 3, Action 2.f)
The survey questions aimed to explore:
- the types of barriers individuals who self-harm face when seeking support,
- the implications of these barriers,
- issues within support services that contribute to these barriers, and
- potential solutions to overcome the barriers.
A full list of survey questions is included in Annex B.
Survey Participants
The survey targeted practitioners and service providers who support individuals who self-harm. It did not include responses from people with lived experience of self-harm, their parents, or peers.
In this report, all survey respondents are referred to as practitioners. This includes both clinical roles (such as doctors, nurses, peer practitioners, and other NHS staff) and non-clinical roles (such as administrative staff, police, educational staff, social workers, and service managers).
While the inclusion of lived experience perspectives would have offered valuable insight, engaging these groups would have required additional safeguarding and ethical protocols. As the research was conducted under the time-limited Scottish Graduate School of Social Science (SGSSS) internship scheme, it was not feasible to implement these procedures within the available timeframe.
The findings reflect the views and professional experiences of those supporting individuals who self-harm, offering an important service-level perspective on barriers to access.
Survey Design and Distribution
An initial draft of the questionnaire was developed by social researchers at the Scottish Government. This was reviewed and refined with input from a steering group comprising professionals experienced in supporting individuals who self-harm. The steering group contributed insights into the barriers faced by those they support, helping to ensure that survey questions and response options reflected practitioners’ experiences.
The final survey was distributed via email by service leads identified through Scottish Government policy networks and in consultation with the steering group. These leads, based in organisations providing self-harm and mental health support, disseminated the survey through their professional networks. This enabled distribution to a wide range of services and organisations supporting individuals who self-harm, including:
- Children and young people’s services
- Primary care
- Psychiatry and psychology
- Prison mental health services
- Social work
- Unscheduled (crisis) mental health care
- Student mental health services
- Suicide prevention services
- Community-based mental health support
Survey Administration and Response
The survey was hosted on Microsoft Forms from 8th July to 26th July 2024. A total of 479 responses were received. One response was excluded for not meeting the inclusion criteria (i.e. not a practitioner or service provider), resulting in 478 responses included in the final analysis.
Analysis
Quantitative data from multiple-choice questions were summarised using descriptive statistics.
Qualitative data from open-text responses were analysed thematically. The survey included one open-text question. An inductive thematic analysis approach was used to identify recurring patterns and themes across responses. Initial coding was carried out manually, and themes were developed through an iterative process to ensure they reflected the range of practitioner perspectives.
Main Findings
This section presents the findings from the practitioner survey. First, the quantitative data is reported, focusing on the barriers that practitioners identify as affecting the people they support who self-harm. Second, qualitative open-text feedback is explored, highlighting practitioners’ suggestions for overcoming these identified barriers.
Respondent information
Of the 478 respondents, the majority (63%) worked for the NHS. Other organisations represented included charity/non-profit organisations (15%), local government (11%), educational institutions (5%) and emergency services (5%). There were no participants who worked for private healthcare providers. Three respondents selected the 'Other' option for this question as their organisation was not listed in the survey.
The most common role among respondents was nurse, comprising one third (33%) of participants. Other notable roles included other clinical/NHS staff (12%), support workers (9%), doctors (8%), social workers (7%), service managers (7%), and police officers (5%). Additionally, sixty-nine respondents reported other roles not listed, such as psychologists, therapists, counsellors, and mental health and wellbeing practitioners. Table 1 provides details on respondents’ professions.
The largest proportion of respondents (35%) had worked in their current role for more than 10 years, while 12% had been in their role for less than 1 year.
| Respondent profession | N | % |
|---|---|---|
| Administrative staff | 3 | 1% |
| Doctor | 38 | 8% |
| Educational staff | 11 | 2% |
| Nurse | 160 | 33% |
| Other | 69 | 14% |
| Other clinical/NHS staff | 55 | 12% |
| Other emergency services staff | 1 | <1% |
| Peer practitioner | 9 | 2% |
| Police | 22 | 5% |
| Service manager | 35 | 7% |
| Social worker | 33 | 7% |
| Support worker | 42 | 9% |
| Total | 478 | 100% |
Respondents were asked to identify the population groups of individuals who self-harm that they support in their professional roles. Figure 1 illustrates that respondents supported people who self-harm across a range of different population groups. It is important to note that respondents could select more than one option to this question.
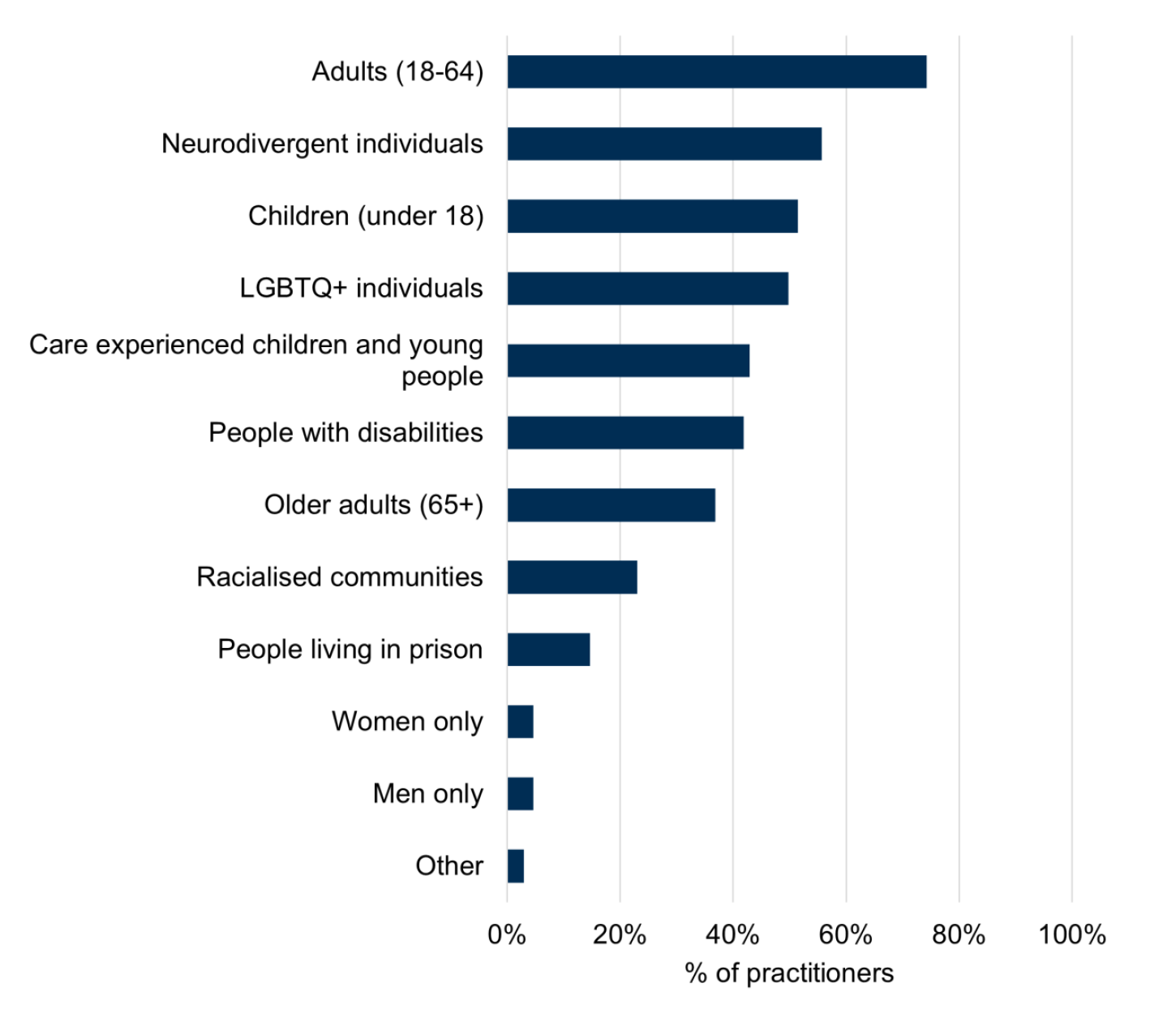
Base: n = 478
Most respondents[6] stated that they worked with adults aged 18-64 (74%). Just over half (51%) of respondents said that they supported children (under 18). 43% of respondents supported care experienced children and young people. 37% of respondents reported supporting older adults aged 65 and above. Over half (56%) of respondents said they supported neurodiverse individuals, while 42% of respondents supported people with disabilities. LGBTQ+ individuals were supported by half (50%) of the practitioners. Each of the remaining population groups were each supported by under a quarter of respondents.
Practitioner Perspectives on Barriers to Accessing Support or Services for Self-Harm
Respondents were asked “Have individuals who you support who self-harm reported experiencing barriers to accessing support or services?”. A total of 354 respondents (74%) answered “yes” and these respondents went on to answer a series of multiple-choice questions regarding the barriers and subsequent implications[7]. The remaining 124 respondents (26%) were branched to a final open-text question on how to improve access to services and support for individuals who self-harm.
A key aim of the survey was to identify barriers that people who self-harm may experience when accessing a range of types of support and services. To explore this, practitioners were asked about barriers encountered across a broad range of services used by the people they support who self-harm. Figure 2 illustrates that, according to these practitioners, barriers are not limited to mental health services but may also be experienced across a wide range of support and services.
Of the 354 respondents, 316 (89%) reported that people they support who self-harm have experienced barriers to accessing mental health services. Barriers were also reported in other health services, for example counselling (64%), out of hours (45%), physical healthcare services (31%) and addiction services (27%). However, barriers to access were not limited to only health services. Notably, every listed service received responses from at least 16% of practitioners.
The findings indicated that there are also barriers to accessing education (24%), emergency services (24%), housing support (29%), employment support (16%), financial support (21%), and educational support (20%). In the open-text “Other” responses, 10 respondents highlighted barriers to accessing other services, such as GPs and psychology services.
A cluster analysis[8] was conducted to explore potential patterns between profession type and the services where barriers to access were reported. Distinct clusters were identified for mental health services across all professions, indicating that barriers to accessing these services were consistently reported regardless of professional background. However, no clear clusters or associations were found for other services, suggesting that reported barriers in those areas may be more variable or context specific.

Base: n = 354
Individual, Service and Structural Barriers
Respondents were asked about the individual, service, and structural barriers faced by the people they supported when accessing services.
- Individual barriers are personal and social factors within or close to the individual that may affect their willingness or ability to seek support.
- Service barriers are obstacles within the design, delivery, and accessibility of support services that can limit access.
- Structural barriers are systemic or environmental factors, such as financial or logistical issues, that create practical difficulties in accessing services.
As shown in Figure 3, the most prevalent individual barriers faced by individuals who self-harm, as reported by practitioners, are fear of stigma, discrimination, or judgement from service providers (65%) and self-stigma (64%). Other individual barriers reported by practitioners include family or cultural beliefs (42%), concerns about receiving a psychiatric diagnosis or misdiagnosis (40%), and concerns about confidentiality or data sharing (30%).
In the open-text “Other” responses, additional barriers mentioned by respondents included the impact of mental health conditions, which respondents said could increase feelings of anxiety or reduce motivation to attend appointments.
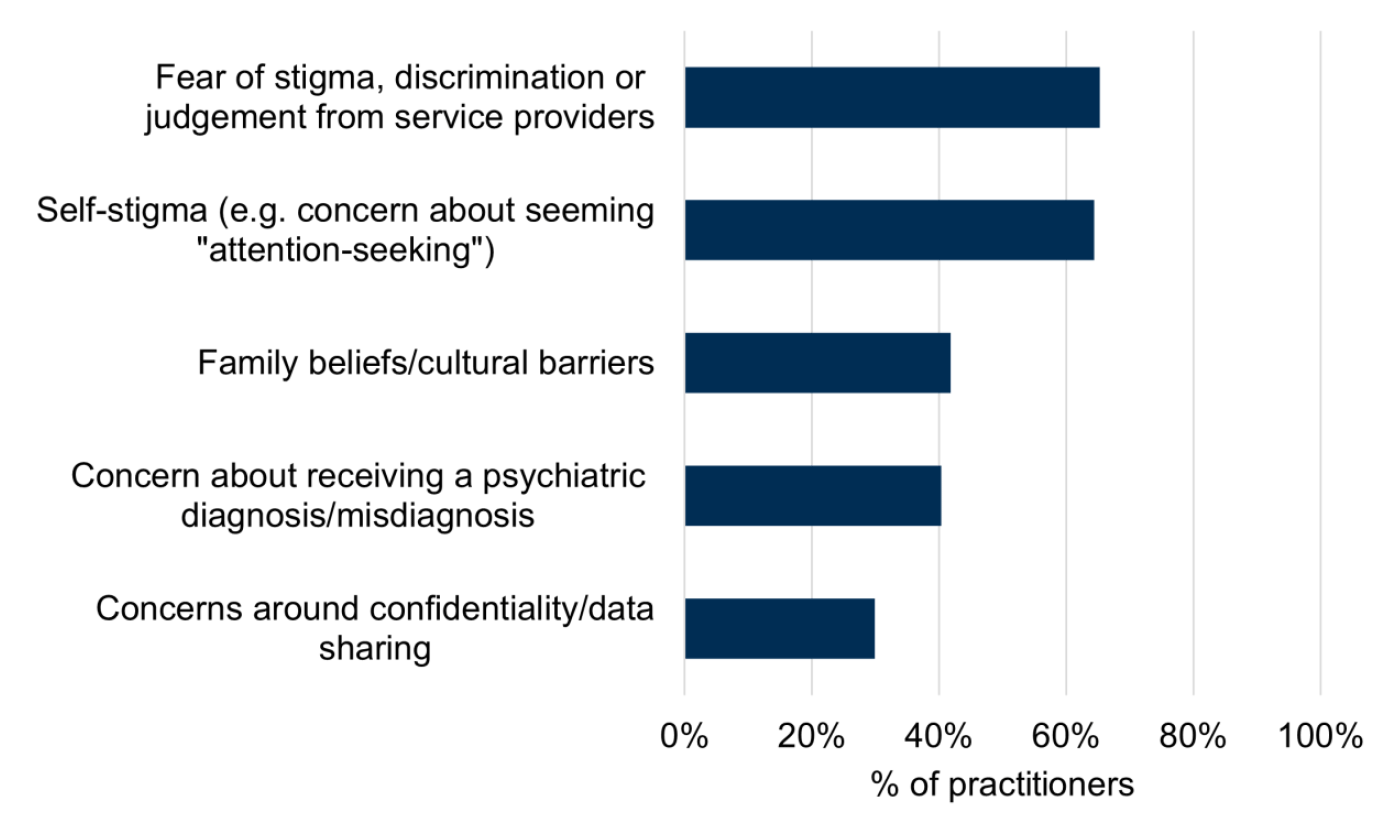
Base: n = 354
Respondents were also asked about any service-related barriers experienced by people they supported. Figure 4 shows that long waiting times (84%) were the biggest service-related barriers faced by people who self-harm according to practitioners, followed by negative past experiences accessing support (79%).
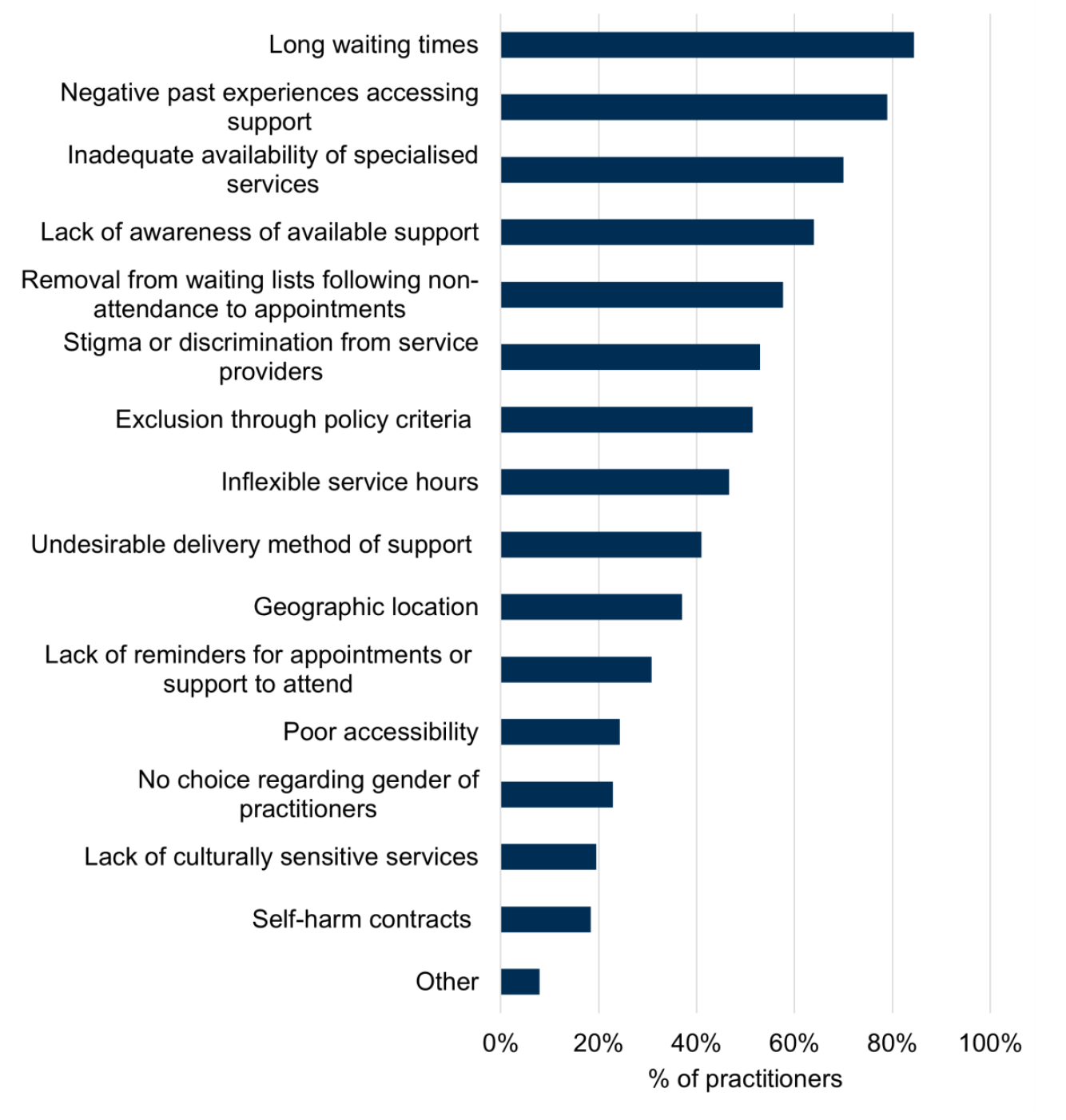
Base: n = 354
Inadequate availability of specialised services (70%), lack of awareness of available support (64%) and removal from waiting lists following non-attendance to appointments (58%) were also listed among the most common service barriers. The proportion of practitioners reporting barriers varied widely, from 84% for most commonly reported barrier to 19% for the least, highlighting the diversity of practitioners’ experiences and perspectives.
Responses indicate that the following service barriers are also encountered by individuals accessing support who self-harm: inflexible service hours (47%), stigma or discrimination from service provider (53%); exclusion through policy criteria (51%), lack of culturally sensitive services (19%), poor accessibility (24%), no choice regarding gender of practitioners (23%), undesirable delivery method of support (41%), geographic location (37%) and lack of reminders for appointments or support to attend (31%).
Self-harm contracts, which involve individuals having to sign an agreement stating that they will not engage in self-harm during treatment, were reported by the smallest proportion of practitioners (18%), aside from the “Other” category (8%). Of those who responded “Other”, they cited additional service barriers including a lack of staff understanding on self-harm and a lack of service provision.
Over half of respondents stated that people they support who self-harm have experienced the following structural barriers when accessing services or support; financial barriers (such as cost of accessing service or cost of transport) (59%), lack of transport to attend appointments (58%) and digital barriers (such as being unable to interact with online services due to lack of access to technology) (52%). Additionally, 40% of respondents indicated that caregivers being unable to bring children or dependents to appointments was a barrier to accessing support.
Implications of Barriers to Accessing Support and Services
Following on from asking respondents about the barriers faced by individuals who self-harm, they were asked about the implications these barriers can have on mental and physical health, as well as any social implications.
Respondents recognised numerous potential mental health implications for individuals who self-harm when they face barriers to accessing support or services. The most frequent mental health implications reported by respondents were an increase in feelings of hopelessness and helplessness (90% of respondents), increased severity or frequency of self-harm (89%) and difficulty engaging with alternative coping strategies (83%).
Additional mental health consequences reported include increased risk of suicidal ideation (81%), ongoing, unmet mental health needs (81%), increased social isolation (79%), worsening underlying mental health condition (77%), enduring self-stigmatisation (58%), and receiving a potentially unwanted diagnosis (45%).
Practitioners acknowledged a variety of potential physical health implications people who self-harm may face as a result of barriers to accessing support. These implications included an increased risk of physical injury or related complications (89%), not seeking help for physical health concerns due to anticipated stigma (75%), and the neglect of physical health needs unrelated to self-harm (73%). Respondents also reported that individuals they support with self-harm are likely to experience potential increased substance use or dependency (67%) and chronic pain (44%) when facing barriers to accessing support and services.
Respondents also recognised a range of social implications for individuals who self-harm when facing barriers to accessing support. These included strained relationships with friends or family (89%), disengagement with support (both formal and informal) (84%) and difficulty in maintaining employment or education (78%). Practitioners also recognised that barriers to support have caused people to avoid re-presenting for treatment due to negative past experiences (76%), decreased their ability to engage in daily activities (71%), increased financial stress (44%), experiencing housing instability (40%) and facing legal issues (32%).
Systemic Issues Impacting Support Services
Respondents were asked whether they have observed any systemic issues impacting support services that contribute to barriers for individuals who self-harm.
Out of the 374 respondents to this question, only two practitioners believed that there were no systemic issues contributing to barriers to support. The most prevalent systemic issue reported was insufficient funding and resources, with 83% of respondents listing this. Other systemic issues include lack of communication between services (74%), burnout among service providers (67%), challenges in transitioning between services (e.g. child to adult services) (66%), rigid service criteria and eligibility requirements (64%), insufficient knowledge or training in self-harm (51%) and a lack of cultural inclusivity and sensitivity (27%).
Summary of Barriers
The survey findings revealed that individuals who self-harm may experience a variety of barriers to accessing a range of different services. Respondents reported that people they support can face barriers to not only mental health services, but services such as addiction, physical healthcare, housing support, financial support, emergency support, and educational support services.
The reported barriers were diverse and multifaceted, with most types listed in the survey being widely acknowledged by respondents as challenges faced by individuals who self-harm. These barriers ranged from negative past experiences when seeking support to long waiting times and financial constraints. Respondents also highlighted various implications of these barriers, including strained relationships with friends or family, an increased risk of physical injury or complications, and heightened feelings of hopelessness or helplessness.
Practitioner Perspectives on Overcoming Barriers to Accessing Services and Support for Individuals Who Self-Harm
Respondents were asked to answer an open-text question on “What can be done to overcome barriers to accessing support for individuals who self-harm?”. Of the 478 respondents, 33 did not provide an answer to this question.
Overall, 93% of respondents were able to identify potential solutions for overcoming barriers to accessing services and support. The qualitative responses also provided valuable insights into various barriers and their impact on individuals who self-harm.
Respondents described what could be done to overcome barriers to accessing support across a range of areas, including improving service provision and accessibility, adopting appropriate approaches to self-harm support, improving service criteria and referral processes, improving understanding, training and education on self-harm, and greater funding into self-harm support and services.
Improving Service Provision and Accessibility
Respondents stated that there needed to be greater provision and availability of self-harm support and services, improved accessibility and signposting to support, and a reduction in waiting times.
Improving Provision of Services
Improving the provision of services to support individuals who self-harm was a key suggestion from respondents. They expressed concern around a perceived lack of services and support options available for individuals who self-harm, with one respondent describing this lack of options as “incredibly destructive and dangerous.” In addition, others felt that there was a lack of staff with specialised self-harm expertise within current mental health services. Many respondents said they would welcome more specialised, dedicated self-harm services throughout Scotland.
Another key suggestion was to create more informal support options outside of NHS care. These could include drop-in centres, community crisis houses, and third-sector services that offer holistic care, as well as online resources to increase accessibility. Safe spaces for individuals who self-harm, modelled on existing services for substance users, which provide non-judgemental support, were also suggested.
To ensure more immediate access to support, embedding mental health, trauma-informed, and self-harm specialist staff in primary care settings, hospitals, and schools was recommended. These embedded workers were seen as a crucial first point of contact for individuals in distress. Respondents also emphasised the need for dedicated therapy and counselling services. Additionally, the need for specialist services tailored to the neurodiverse population was highlighted, ensuring that care is accessible and appropriate for all individuals.
Respondents frequently stated that improvements should be made to ensure that individuals who self-harm have more regular appointments and in-depth discussions with service providers, such as their mental health team. It was believed that having longer and more intensive sessions would help to understand the deeper causes of self-harm, rather than focusing soley on coping mechanisms.
The lack of service provision for individuals who self-harm observed by some of the respondents was said to have negative implications for individuals they support. One respondent described how, due to limited availability, healthcare providers have recommended that individuals who self-harm enrol in college courses in order to access mental health support.
“As a Further Education establishment, we are also aware that individuals who self-harm have enrolled onto courses in order to access the college's own counselling and wellbeing services after experiencing difficulty or delays in accessing the help they need from the NHS and local authorities. Indeed, anecdotally we are being told that people are actively being directed to colleges from other would-be providers to access these services” (Service Manager)
Reducing Waiting times
Waiting times were viewed as a significant barrier to accessing services. When individuals who self-harm experience long waiting times, it was said to contribute to a loss of hope about getting the support they needed. A prevalent view among respondents was that quicker access to support was critical, particularly when individuals who self-harm experienced a crisis. In addition, a few respondents highlighted that if self-harm is not considered “severe” by services then an individual may be placed on a long waiting list which could lessen the effectiveness of support once received.
“Self-harm doesn’t fall under urgent criteria unless it is severe therefore young people are waiting 2-3 years to be seen. [Needs] Better tier 2[9] supports to help with self-harm while waiting on specialised support” (Nurse)
“Accessing services should be available at the point of crisis and those experiencing self-harm should not have to wait for appointments which can often take weeks or even months to be seen” (Social worker)
A more rapid response approach was suggested so that appropriate support is available for those who self-harm at the right time. An NHS nurse noted that their service provides self-referrals and same-day appointments if required, which they reported on positively and felt would help.
Improving Accessibility to Services
Respondents were concerned that restrictive and inflexible service hours acted as a barrier to accessing support in individuals who self-harm. For example, services which were only available on weekdays from 9am to 5pm. This availability was considered potentially damaging by several respondents due to self-harm often occurring out with these hours, with one respondent explaining:
“Mental health professionals available for non-hospital-based crisis services outside of 9-5, when most crises actually happen. Sticking to 9-5 is a disgrace that results in deaths, to be quite frank.” (Psychologist)
The issue of restrictive hours was raised by a few respondents when discussing non-crisis services such as CAMHS and community mental health teams. For example, if somebody was to present late on a Friday to a community mental health team there would be time pressures to refer the individual to another service before the weekend to ensure their safety.
Many respondents suggested that, to effectively support individuals who self-harm, services and support should also be available outside of regular hours or 24/7. Suggestions included 24-hour hubs where individuals can call and receive support or out of hours services they can attend in times of crisis. Although respondents acknowledged the availability of out-of-hours services, such as NHS 24, one respondent noted that calling NHS 24 for self-harm may lead to police being sent to the individual’s home. This was reported to be intimidating for young people and may deter them from accessing the service. One respondent provided a more positive example of successful out-of-hours support, which was from Scottish Action on Mental Health (SAMH) Sam’s Café[10] which is a drop-in service where there is no wrong time or place for individuals who self-harm to ask for help.
As well as having more services with flexible hours, being able to reach and access services across multiple formats was considered beneficial. For example, offering individuals who self-harm appointments via telephone, online video, and face to face, including home or school appointment options. Additionally, utilising texts to send appointment reminders to help with non-attendance or offer a 24/7 text-based chat option. While digital healthcare options were recommended, it was also acknowledged that improved access to digital technologies is essential for people who self-harm and also experience digital exclusion, in order for them to effectively benefit from these services.
Several respondents felt individuals living in remote and rural areas should have greater access to support and services for self-harm. This included improved out of hours services and self-harm trained staff within services in remote and rural locations. A nurse highlighted that they currently only had one self-harm service that can provide support to individuals in their council area stating that it “results in a postcode lottery for treatment.”
Transport links were a particular challenge for those in remote and rural communities, with respondents reporting that there may be several hours between bus services to attend an appointment and the return bus to their home. Financial support such as free transport to attend appointments was recommended in these situations. However, others said that public transport can act as a barrier due to anxiety, low self-esteem and finding the experience overwhelming. In these cases, improved digital healthcare options or more local services to reduce the need for travel would be beneficial.
Other accessibility issues identified by respondents included the ability to access NHS services anonymously, user friendly forms or pathways for support, patients having stable accommodation, services proactively encouraging individuals to attend, interpreters available within services, having services tailored towards different genders and cultures, and support options for single parents who cannot attend with their children.
Improving Signposting to Available Support
Many respondents said that there should be improvements in signposting and awareness of what resources are available for individuals who self-harm. A few highlighted that the people they were supporting were sometimes unaware of what services were available or who to ask for help. A suggested solution to the lack of awareness was to provide a one-stop resource that individuals who self-harm can access to identify available support. Respondents thought this could also be beneficial for service providers who support individuals who self-harm and may be unsure where to direct or refer someone to.
“Improved awareness amongst professionals/service providers about what can be accessed, whom it is for, and where & how it can be accessed. There can also sometimes be too many options (or things that look like they might be options) which can make it challenging for practitioners and those they support to know what is the right service or resource at the right time.” (Other clinical/NHS staff)
“They [people who self-harm] often don't know how to find help and there should be a simple 'Fridge Door' where there can go to look for whatever service they need at that time (where do you go to find the note or telephone number you need - the Fridge Door).” (Police)
Respondents also recommended that signposting and resources should be accessible and visible to individuals who self-harm, with information displayed in public places such as GP surgeries, libraries, community centres, pubs, and cafes.
Summary
A key suggestion to overcome barriers to accessing support and services was to develop more specialist and dedicated self-harm support options. Respondents offered a wide range of suggestions, from drop-in centres to self-harm trained staff being embedded into GPs and schools. Respondents also felt that it should be easier for people who self-harm to access services by extending opening hours and offering appointments in multiple formats. Additionally, clearer signposting to resources was identified as a strategy for increasing awareness of available support for individuals who self-harm. Finally, respondents believed that waiting times should be reduced to ensure people who self-harm receive effective support, particularly during a crisis.
Improving the Types of Approaches to Self-Harm Support
Respondents offered several suggestions on the approaches mental health and self-harm services should adopt when supporting individuals who self-harm. Overall, they believed a holistic approach was essential, recognising the many contributing factors that may lead to self-harm. Respondents also emphasised the importance of understanding the person as a whole, treating them with compassion, and co-creating a care plan that suited their needs.
Person-Centred Approach
Adopting a person-centred approach to supporting individuals who self-harm was generally viewed as good practice for services. Respondents stated that effective and appropriate support came from understanding why someone may be self-harming and tailoring support to an individual’s needs. Some believed that third sector organisations tended to have more service user and needs led support, while NHS support was viewed as more prescriptive because it applied similar intervention methods to all. One respondent described NHS mental health support as a “revolving door”. Group-based interventions were described as sometimes failing to account for an individual’s past experiences, meaning individuals who self-harm may discontinue with support. A service manager reported how an individual they supported attended a group-based intervention where:
“Someone spoke openly about how they attack people which triggered others who had experienced domestic abuse. The result, this person did not feel comfortable to complete the course and as a result was discharged from support.” (Service Manager)
Co-creating care plans was recommended as an effective way to tailor support to an individual’s needs. This approach requires staff to build a trusting relationship with the individual, supporting them to identify and understand their self-harm, explore coping strategies, and collaboratively develop a plan that works for them. Respondents considered continuity of care with the same practitioner important for this, in particular because of the value of building a therapeutic relationship can have when receiving care.
“I feel we all have a duty of care to patients who are in [need of] mental health [support]. And I think employees should be taking the time to explore the reasons as to why self-harm occurs, rather than disrupting the therapeutic relationship, because 'it's not our remit to manage self-harm,' and directing patients back to the clinic to speak to someone to whom they have never met before.” (Nurse)
A trauma informed approach within mental health services, including when caring for those who self-harm, was also advocated by a few respondents. These respondents also noted that self-harm should be considered as part of a wider context, including if an individual has experienced trauma and adverse childhood experiences.
Harm Reduction Approach
Several respondents believed there should be more of an uptake and embrace of helping people with harm reduction and safer alternative coping strategies. Advocating a harm reduction approach, rather than abstinence from self-harm, was viewed by some as a potential way to support people with the initial engagement process and help to open up discussions around alternative coping strategies. In addition, this type of approach was suggested as being particularly helpful in more closed settings such as prisons.
Early Intervention
Supporting early intervention was recommended by a few respondents to help identify and support individuals who may be at risk of self-harming before the behaviour escalates or reoccurs. It was felt that much of the support currently available for people who self-harm is crisis management, often requiring emergency service staff to provide the support. This was viewed as potentially leading to a cycle of self-harming behaviours and that early intervention is a more effective approach. A social worker described how people who self-harm can fall into a cycle of contact with the same services:
“service user self-harms - police contacted - police take to hospital - CAMHS/MH services assess then discharge to community - client self-harms - police take to hospital etc etc...…Early intervention is often a better approach, however this requires funding.” (Social Worker)
Early intervention was deemed particularly important for children and young people. For example, where teachers are trained in mental health and self-harm, or specialists are embedded within a school setting. This approach was said to have two main benefits: enabling staff to identify early if someone was self-harming or at risk and provide appropriate support, while also functioning at a preventative level by teaching children coping skills and resilience from an early age.
Reducing Experiences of Stigma
Stigma was considered a major barrier to accessing services for people who self-harm. Respondents therefore welcomed any efforts aimed at reducing self-harm stigma across services and wider society. It was felt that the current stigma around self-harm can perpetuate self-stigma and discourage individuals from seeking support.
“Stigma and bias in professionals is, in my opinion, the largest barrier to accessing support for an individual who self-harms. This must be eradicated at all levels to reduce barriers to access.” (Senior Practitioner)
“After all, many of those who self-harm feel rejected, unwanted, misunderstood etc. It doesn't help if the service that is supposed to support them perpetuates those impressions.” (Social Worker)
Respondents said that individuals they supported easily recognised stigma and judgement coming from service providers. Examples included viewing self-harm as attention seeking, having negative reactions to disclosing self-harm, viewing self-harm as only a behaviour resulting from a mental health condition or addiction, and disregarding their self-harm as not “serious enough” to receive support. These responses from service providers can mean individuals who self-harm may step away from seeking support or worsen their self-harming behaviours.
“I have had many young people come to a tier 3 service [specialised mental health services] feeling more anxious explaining to me that they just wanted support and to talk to their chosen 'safe person' however, that safe person's reaction of alarm/fear and automatic responses, such as telling parents/carers or referrals to tier 3 services as they feel unprepared or not able to manage self-harm, result in the young person feeling 'rejected,' 'shame,' 'embarrassment' and 'lack of trust' to name a few feelings/emotions described by the young people I work with.” (Nurse)
“Many of the people are concerned about being turned away from psychiatric services due to their self-harm not being considered serious enough, this tends to lead them to feel pressure to increase/worsen their self-harm behaviour in order to justify their need for psychiatric support services.” (Mental Health and Wellbeing Practitioner)
Some respondents expressed the view that “changing the culture of blame to a culture of support“ within services is required to overcome and reduce stigma. This cultural change within services could be supported by improved training for staff on how they respond to self-harm and taking a compassionate approach.
Many respondents thought that ensuring individuals who self-harmed were treated with compassion and felt listened to was vital for overcoming barriers to support. An example of this was described as a service which creates a non-judgemental environment where individuals who self-harm are listened to with compassion, empathy and acceptance. A few respondents highlighted the importance of individuals who self-harm feeling listened to during the first point of contact with services. This was said to help build trust in the support and meant they could start to foster positive therapeutic relationships with the service provider.
A reduction in stigma could also be aided by educating the public on self-harm, according to respondents. For example, it could help normalise the conversation around self-harm and encourage people to feel more comfortable seeking support. Likewise, respondents proposed that if parents felt they understood more about self-harm they may feel more confident and empowered to support their child, as well as reducing the risk of potential negative reactions to a disclosure of self-harm.
Summary
Respondents provided examples of different types of approaches to supporting individuals who self-harm. At the centre of these suggestions was for service providers to take a person-centred approach by understanding the needs of the individual who self-harmed, as well as treating them with compassion to reduce stigma.
Improve Service Eligibility Criteria and Referral Processes
Respondents argued that service criteria for accessing support should be less restrictive, and that referral processes between services could be improved.
Less Restrictive Service Eligibility Criteria
A major service barrier cited by the respondents was criteria being too narrow and restrictive for individuals who self-harm to access support. Respondents explained that restrictive criteria can leave a gap in services available for people who self-harm. They described how people they supported had their access to a range of different services denied due to their self-harm including statutory services, daytime and out of hours, psychological therapies, counselling, pain management services, physical health screening, and alcohol or drug services. Ultimately, it was felt by many that the exclusionary criteria for those who self-harm can worsen their situation, are discriminatory and leaves people with limited options and inequitable care.
Rigid eligibility criteria can also mean that if an individual self-harms while they are receiving care they may be withdrawn from that service. It was felt that removing an individual from a service because of self-harm can be detrimental to their recovery. For example, if self-harm escalates, some therapists or counsellors may redirect patients back to their GP clinic, due to restrictive service criteria. By refusing access to psychological therapies while self-harming, it meant that nurses may be left to manage the self-harm without a proper understanding and support for the underlying issues.
Others suggested that services may have rigid criteria because they feel they do not have the expertise to support individuals who self-harm or to manage waiting times due to a lack of resources. Respondents noted that some services refuse to admit individuals who self-harm if they also have a diagnosis of personality disorder. Another respondent highlighted that some service criteria can limit older adults from getting support.
“I work with Older Adults. Older adults are frequently discriminated against as many support services, including NHS, have an age cut off at 65yrs. My patients cannot access Mental Health Assessment units in the way "younger" adults can. Very many community services are similar and will cite "comorbidities" as the reason. This needs to change.” (Nurse)
A few respondents also raised concerns that services had a policy of removing patients from the service if they did not attend an appointment. Respondents emphasised that efforts should be made to visit the patient’s home, find out why they have not attended and offer follow up appointments.
“People with low mood, poor mental health, neurodiversity are not always able to reach out or be organised to attend appointments, or perhaps missed one by accident and feel anxious about going to the next one as they will be asked why they forgot/missed the last one. At the scene of an accident, you go to the quiet casualty first, you know the one shouting out is alive and breathing, the quiet one could be in worse shape if not making a noise. Why is this not an approach we think of when service users go quiet/don't attend appointments and we know they have mental health support needs?” (Support Worker)
Many respondents recommended implementing a lower threshold for care, broadening acceptance criteria for services, and recognising self-harm as a treatable symptom rather than a barrier or a reason for exclusion. Where individuals who self-harm were refused due to service criteria, they felt that signposting to alternative services that would not exclude on the basis of self-harm would be valuable.
“Services being encouraged to be more inclusive in their acceptance criteria. Better discussion between services around individuals who are at risk of falling through gaps caused by service referral criteria. At present there are far too many occasions where we are encouraged (by policy and by the interpretation of policy by managers) to think and explain why we can't see someone than to consider maybe we can and should see someone” (Doctor)
Improving Referral Processes
Respondents advocated for a faster and clearer referral process between services for individuals who self-harm. They highlighted that delays in treatment or support are particularly challenging, especially when individuals are referred only to be placed at the end of another waiting list if they do not meet the criteria of the service they were initially directed to. Additionally, limited referral options can be problematic, particularly for those with trauma histories or specific diagnoses.
“We don’t have easy access to refer patients for evidence-based treatments that help those who self-harm with a background of trauma or diagnosis of personality disorder. This patient group do not have appropriate support or access to treatment.” (Nurse)
Furthermore, improved referral pathways are especially important for individuals with co-occurring mental health and substance use issues, which are often interconnected. These individuals can experience being passed between services, as they may not be accepted until one of their needs is resolved.
“Often a person with multiple issues, drug use impacting on mental health (or vice versa), where there are additional knock-on effects re housing / financial / more vulnerable to cuckooing etc. they are often directed to one service who advises they have to get one of their issues sorted before they will look into others. The problem is that the issues are interconnected, and a one issue one service approach doesn't work.” (Police)
Many respondents advocated for a "no wrong door policy," where if an individual does not meet the criteria for one service, they are still guided to an appropriate service at the point of contact. This approach was said to require improved coordination between mental health services but could prevent individuals from being passed between services and ultimately save resources in the long term.
“First point of contact with mental health or addiction services must be the single gateway to whichever mental health service is appropriate so that people are internally supported to access the right service rather than the appalling circus of staff resource being consumed by policing boundaries and rejecting referrals rather than serving the needs of patients.” (Doctor)
More joined-up working between services was seen as essential to improving referrals. Respondents suggested a multidisciplinary approach, where service providers, charities, the NHS, and other organisations collaborate to ensure individuals receive the support they need, rather than being passed between services or being unable to access care. Improving communication between services could assist with this. For instance, one respondent said that more shadowing days, where staff visit other services to better understand what each service offered, could ensure that referrals are more appropriate. In addition, having one IT system that integrates all relevant information was proposed as a way to support referrals.
Better transitions between services, such as from CAMHS to adult services, during geographical moves or better links with services to prison health care for those who cycle in and out of custody, were also suggested as areas of improvement. While some respondents recommended introducing self-referrals as another way to streamline the referral process.
Summary
Many respondents suggested that there should be a lower threshold for care and wider acceptance criteria into services. They believed that current restrictive service criteria means that individuals who self-harm can fall between the gaps of support. In addition, respondents recommended an improved referral process that adopts a “no wrong door” policy so that people who self-harm can be guided to appropriate support at the point of contact.
Improving Understanding, Training and Education on Self-Harm
The most common recommendation that respondents suggested to overcome barriers to accessing services was to improve training and understanding on self-harm. This included increases in the provision of training available across professions and suggestions on the content of the training itself. It was suggested that if practitioners across different professions had a greater understanding of self-harm, individuals who self-harm could feel more supported within the wider community, rather than relying solely on specialist services.
Improving Practitioners’ Understanding of Self-Harm
Respondents believed there was a need for a greater understanding about self-harm. It was viewed that if service providers understood the behaviour more it would make them better equipped to support individuals in a compassionate and non-stigmatising way. Service providers having an improved understanding about why people self-harm could make them more approachable for people wishing to access services, enabling them to ask the right questions and refer appropriately, if needed. Some viewed understanding the processes leading to self-harm as essential to providing support, noting that these processes were often systemic and rooted in histories of trauma and adverse childhood experiences.
“We need a deeper and richer response to the underlying drivers to self-harm - the function of it. We need to reach the warded off and intolerable feelings below the self-harm behaviours. Otherwise, we are just superficially firefighting, patching up endlessly and never reaching the root of the issue” (Other clinical/NHS staff)
Many believed that an area where practitioners should have a greater understanding is of the multiple forms of self-harm that an individual may engage in. By having a broader understanding of this, it could help with early identification for those who support people who self-harm, both professionally and personally. A support worker noted the different forms of self-harm they have observed:
“I haven't witnessed self-harm as people hurting themselves by cutting or burning, it's more, not eating, drinking alcohol in excess, not looking after their personal care, and living in isolation, scared or unsure whether to mix with others and be seen in public” (Support Worker)
There were several respondents who wanted improved understanding on what they viewed as common misconceptions about self-harm. Firstly, respondents emphasised that service providers should recognise that self-harm does not always indicate a mental health condition. Secondly, they highlighted the need for greater understanding that self-harm is not always an intention to end one’s life but can instead serve as a coping mechanism. Thirdly, some respondents called for increased awareness that self-harm is not an act of attention-seeking. Lastly, they stressed that the severity of self-harm does not necessarily reflect the severity of an individual’s distress. This can be particularly problematic if someone’s self-harm is not considered severe enough to access a service, potentially encouraging individuals to escalate their self-harming behaviour in order to gain access.
Self-Harm Training for Practitioners
Several respondents believed that training and education on self-harm should be made available to all professionals across social care, health and education sectors. It was considered important that all professionals understood how best to work with those who self-harm and on how their behaviour may affect the people they support.
“Training on how to manage self-harm doesn't exist currently, even if you are a psychologist which I am. Training on emotion regulation should be given to all mental health professionals.” (Psychologist)
Other respondents gave specific examples of areas where they viewed training to be needed, including within emergency departments, physical healthcare services, and schools and education. Respondents stated that improved training and understanding of self-harm within emergency departments and from first responders was important. In particular, educating staff on taking a compassionate approach was considered a way to reduce stigma and negative reactions to self-harm. Additionally, it was suggested that emergency department staff would be better equipped to support an individual who had self-harmed if they had an improved understanding of the underlying causes and awareness of available services and referral options.
“Having better training to understand self-harm among police and other emergency services would be beneficial to workers and individuals who self-harm. Police Scotland clearly do not want to be dealing with the NHS's workload but in reality they do and should be better at dealing with persons in crisis generally and have more specific training to deal with self-harm in a sympathetic manner.” (Police)
Similar to perspectives on emergency department staff, there were a few respondents who believed that physical healthcare staff working could benefit from training on self-harm. It was suggested that training could help these staff understand how negative reactions to an individual’s self-harm may impact on the patient and help to build a more compassionate response. In addition, respondents said staff working in physical healthcare should understand that self-harm is not solely the responsibility of mental health services, and that physical injuries require treatment.
“Training for non-mental health professionals in relation to attitudes towards self-harm, and understanding of self-harm. In my experience, young people have been sent away from physical health settings after engaging in self-harm because 'it's a mental health problem', however the resulting injuries from engaging in self-harm still require physical explorations due to risk of infection. (Nurse)
Within schools, there were a few suggestions of where specific self-harm training could be valuable. For example, training for teachers on understanding self-harm. This was suggested because teachers may be one of the first to become aware of children and young people self-harming. It was recommended by a few respondents that embedding mental health into the school curriculum could enable children to learn basic skills and resilience. Suicide prevention training initiatives such as SafeTALK[11] or ASIST[12] were also suggested in school settings.
Respondents also said that training could be improved within prisons, where it was recommended that staff should be trained on the basics of mental health nursing and support the work of mental health services in prisons. In addition, some suggested training for mental health staff supporting individuals who self-harm on adapting materials for individuals with learning disabilities or autism.
Summary
Respondents believed that it was vital for practitioners supporting individuals who self-harm to have a greater understanding of the behaviour and the multiple forms of self-harm individuals may engage in. In addition, it was considered important to educate staff on several misconceptions about self-harm such as the view it is attention seeking. In doing so, respondents felt practitioners would be better equipped to support individuals in a compassionate and non-stigmatising way. To achieve this, they suggested staff training across a range of services that may support individuals who self-harm.
Funding and Resources
It is important to note that many respondents recognised that their recommendations to overcome barriers to access support for people who self-harm were reliant on funding and resources. This was the second most commonly cited issue by respondents.
Respondents cited needing funding to ensure services are adequately resourced to support individuals appropriately. A variety of different specific reasons were given for needing increased funding. Including for the development of new services, recruiting staff, improving staff capacity and ensuring that staff are appropriately trained to support individuals who self-harm. Increased funding was also cited as way to help reduce waiting times or provide outreach support for people who are on long waiting lists. In addition, more funding could be used to adopt a person-centred approach to self-harm support where staff have the capacity to co-create plans and address the underlying causes of self-harm.
Overall, there was a sense among respondents that many services are working at crisis points due to a lack of resources and personnel. As a result, individuals who self-harm may not receive the support they need, refrain from initially seeking support, or their self-harming behaviour may escalate. On the other hand, staff were reported to feel overstretched and burnt out. This can be exacerbated by staff absences and retention issues, meaning new staff could enter a workplace where there is a lack of experience. Practitioners across different professions highlighted issues associated with a lack of resources and funding in the following quotes:
“I think the whole system needs reviewed independently and overhauled from top to bottom. Services are chronically understaffed and overstretched resulting in obscene wait times for even initial contact which puts many off even starting the process.” (Police)
“The demand on services means that Community Mental Health Teams are just not fit for purpose. They themselves are now acting like crisis services, and unable to attend to planned, routine interventions. High risk behaviour is prioritised and therefore often for people, reinforced. "I had to try to kill myself before I got seen". I have heard this numerous times.” (Other clinical/NHS staff)
“All the issues - long waiting lists, lack of provision, having to disengage from people who do not attend appointments stem from a real lack of resourcing. Everything comes from there and leads to burnout of staff, feelings of hopelessness and helplessness and so on. The training is good and is enlightening for professionals, but the lack of time and resources means it cannot be implemented effectively.” (Social Worker)
Summary
Respondents recognised that most recommendations to overcome barriers to access support for people who self-harm were reliant on funding and resources. There was a prevalent view among respondents that many services are working at crisis points due to a lack of resources and personnel. Therefore, they felt that more funding to address these issues was required to ensure services are adequately resourced to support individuals who self-harm.
Conclusion
In conclusion, the survey with practitioners who support people who self-harm identified that there are barriers to accessing support across a range of services. These barriers are the result of different individual, service and structural issues and can lead to an array of different mental, physical and social implications for people who self-harm.
Despite the multitude of barriers identified, almost all respondents described what could be done to overcome barriers to accessing support across a range of areas, including improving service provision and accessibility, adopting person-centred and compassionate approaches, improving service criteria and referral processes, improving understanding, training and education on self-harm, and providing greater funding into self-harm support and services.
Contact
Email: socialresearch@gov.scot