Alcohol Framework 2018
Updated framework setting out our national prevention aims on alcohol.
Section 2 – Outcomes
Our ambition is a Scotland where less harm is caused by alcohol.
19. As set out in the Introduction section, our approach is evidence-based and aligned with the WHO approach of placing the three prevention ‘A’s front and centre: Affordability, Availability and Attractiveness. Our approach also aligns with WHO’s new SAFER initiative[39]. In preparing the 2009 Alcohol Framework, we consulted upon the evidence base and the performance measures we should set. We produced a series of logic models which remain current and continue to underpin our work[40] (Figure 4).
Figure 4: Scotland’s Alcohol Logic Models: Logic Model 1 (strategic level)
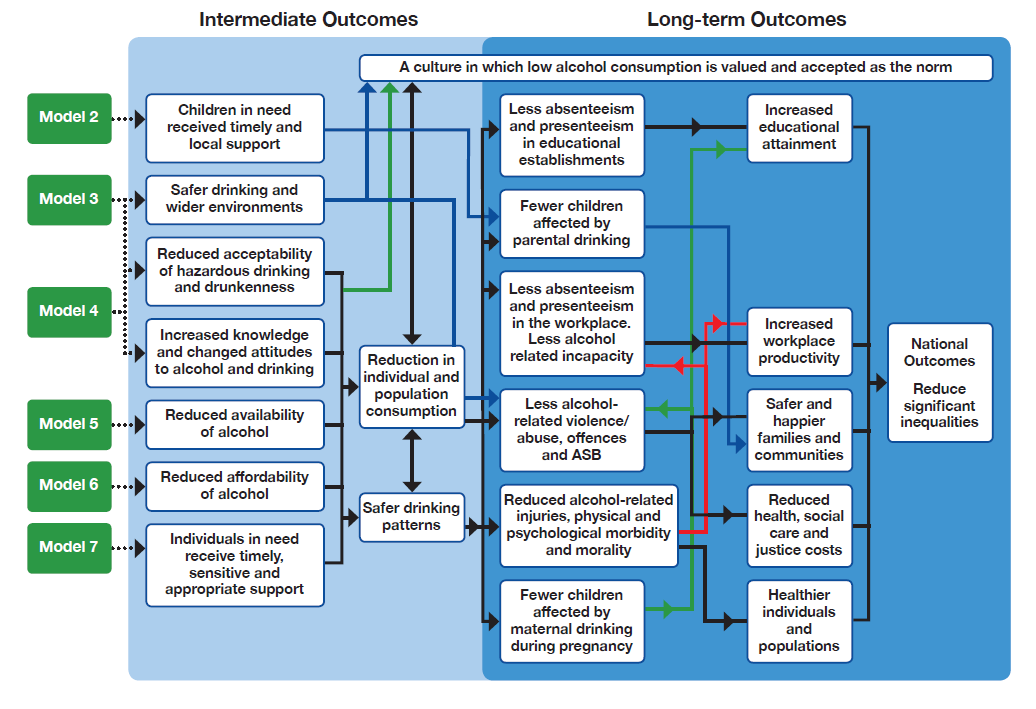
20. Our logic models set a number of intermediate and long-term outcomes. Some of these (for example, logic models 2 and 7) relate to treatment and support services, for adults and children, and they help to underpin the overarching alcohol and drugs strategy. The intermediate and long-term outcomes which underpin this Alcohol Framework are:
Intermediate outcomes
- Safer drinking and wider environments
- Reduced acceptability of hazardous drinking and drunkenness
- Increased knowledge and changed attitudes to alcohol and drinking
- Reduced availability of alcohol
- Reduced affordability of alcohol
All leading to:
- A culture in which low alcohol consumption is valued and accepted as the norm
- Reduced individual and population consumption
- Safer drinking patterns
Long-term outcomes
- Less absenteeism and presenteeism in educational establishments
- Fewer children affected by parental drinking
- Less absenteeism and presenteeism in the workplace and less alcohol-related incapacity
- Less alcohol-related violence, abuse, offences and anti-social behaviour
- Reduced alcohol-related injuries, physical and psychological morbidity and mortality
- Fewer children affected by maternal drinking during pregnancy
All leading to:
- Increased educational attainment
- Increased workplace productivity
- Safer and happier families and communities
- Reduced health, social care and justice costs
- Healthier individuals and populations
All leading to:
- Achieved National Outcomes: and National Indicators (as updated in June 2018)[41]
- Reduced inequalities
Health inequalities and young people
21. In addition, we will ensure that two consistent threads run through all our work:
(1) our actions must reduce health inequalities; and
(2) our actions must protect children and young people.
| reduce alcohol harm | |
|---|---|
| reduce health inequalities | protect children and young people |
Our actions will work towards reducing health inequalities:
22. There is a stark social gradient to alcohol-related harm and, whilst we have seen some improvements in alcohol-related health inequalities in recent years, deaths are nearly seven times higher in the most deprived decile compared to the least deprived decile, and hospital admissions are nearly nine times higher in the most deprived decile compared to the least deprived.
23. These statistics are unacceptable for any modern nation, and especially so given our strong ambitions to create a fairer country with opportunities for all, regardless of socio-economic background. Tackling alcohol-related harm – in itself – has the potential to help address Scotland’s wider health inequalities.
24. Our actions must always work together to reduce health inequalities. In particular, work on minimum unit pricing, engaging in licensing, Alcohol Brief Interventions, positive alternative opportunities and safer communities and preventing alcohol-related violence and crime have substantive equity dimensions.
Our actions will protect children and young people:
25. Children’s wellbeing sits at the heart of the Scottish Government’s approach to Getting it right for every child (GIRFEC)[42]. By understanding the quality of children’s and young people’s wellbeing through eight indicators: Safe, Healthy, Achieving, Nurtured, Active, Respected, Responsible and Included (SHANARRI), we offer a common language showing how we aim to improve outcomes for our children and young people. Through GIRFEC, we are determined that every child should be able to reach their full potential as an individual. In considering our approach to public health policies, it is incumbent upon us to do all we can to support children’s health in positive ways, including taking preventative action at the national level where that is warranted.
26. Children’s rights are enshrined in the United Nations Convention on the Rights of the Child (UNCRC)[43]. In Scotland, Ministers have a duty under the Children and Young People (Scotland) Act 2014[44] to keep under consideration whether there are any steps they could take to give further effect in Scotland to the UNCRC. The Act also requires Scottish Ministers to report to Parliament every three years on progress made in meeting these new duties, and on their plans for the following three-year period. The first report is planned for 2018.
27. Alcohol is an age-restricted product for good reason. The scientific evidence is clear that an alcohol-free childhood is the healthiest and best option. Children and young people are particularly vulnerable to the effects of alcohol. The earlier a young person begins to drink alcohol, the more likely they are to drink in ways that can be risky later in life. Underage drinking can cause short and long term harm to health, as well as put young people in dangerous situations. We must continue to take forward actions to prevent children and young people from gaining access to alcohol and therefore putting themselves in risky situations.
28. Children’s right to be kept safe from alcohol harm includes the damage caused by parental or other familial drinking. The move towards most drinking being done in the home means children and young people are much more likely to be around alcohol and to witness adults’ drinking, and potentially be exposed to its harmful effects[45]. This is even where drinking is within the lower-risk guidelines, showing that we should not assume that negative impacts of parental drinking are only associated with higher levels of consumption.
29. Policy can sometimes seem to place children and young people in something of a vacuum, thinking about them only in specific contexts or settings such as within schools. In reality, of course, children and young people are central to their families, their peer groups, their local ‘places’ and their wider communities.
30. Our actions must always protect children and young people. In particular, work on preventing underage drinking, marketing and advertising, education in schools, positive alternative opportunities and safer communities and preventing alcohol-related violence and crime all aim to protect children and young people.
31. In taking actions to protect children and young people we must ensure that measures are developed with them and not imposed upon them. As Article 12 of the UNCRC makes clear, children and young people, who are capable of forming a view, should be allowed to express their views on matters affecting them. We take this very seriously and utilise the Child Rights and Wellbeing Impact Assessment (CRWIA) in ensuring that our policies, measures and legislation protect and promote the rights and wellbeing of children and young people. In developing preventative approaches to alcohol harm, we will encourage young people to participate and influence the development of our policies at the earliest stage.
Action 1: we will put the voices of children and young people at the heart of developing preventative measures on alcohol. This will involve encouraging and seeking the views of children and young people.
Contact
Email: Alison Ferguson