Self-harm strategy and action plan: mid-term report
Overview of the activity and achievements in the first 18 months since November 2023 of implementation of the Self-Harm Strategy and Action Plan. It highlights where progress has been made across the action plan, key learning and next steps
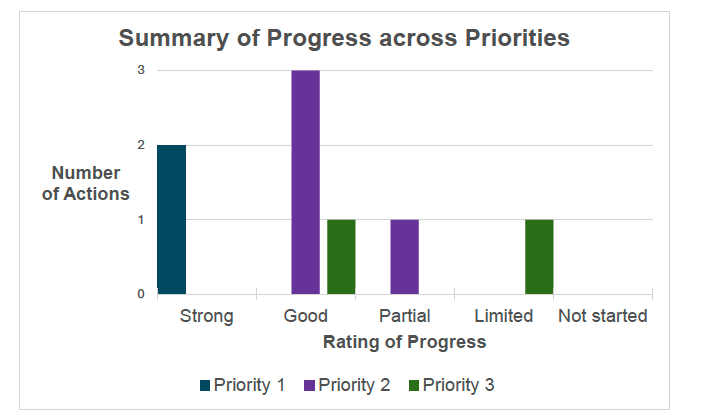
Progress in Delivering our Action Plan & Outcomes
This section of the report details the progress we have made across the action plan, by each priority area, showing the key actions and progress towards the respective short-term outcomes. A full explanation of the detailed actions can be found in the Action Plan section of the Self-Harm Strategy. The ratings below are self-assessment ratings shaped further by the SHAPE and Data and Evidence Groups. They are based on where there has been significant progress at the current point of time for the Action Plan. We recognise that there are still many challenging areas to be addressed including the prevalence of stigma across health and care settings and in availability of data.
Priority 1: Continue to expand and deepen knowledge and compassionate understanding of self-harm and tackle stigma and discrimination.
Number of actions: 2
Action 1.1 progress: Strong
Action 1.2 progress: Strong
(Action 2.1 also contributes to this Priority)
Priority 2: Continue to build person-centred support and services across Scotland to meet the needs of people affected by self-harm.
Number of actions: 4
Action 2.1 progress: Good
Action 2.2 progress: Good
Action 2.3 progress: Partial
Action 2.4 progress: Good
Priority 3: Review, improve and share data and evidence to drive improvements in support and service responses for people who have self-harmed or are at risk of doing so.
Number of actions: 2
Action 3.1 progress: Good
Action 3.2 progress: Limited
Below outlines the priorities for the Self-Harm Action Plan, their Short Term Outcomes and the main actions associated with each
Priority 1: Continue to expand and deepen knowledge and compassionate understanding of self-harm and tackle stigma and discrimination.
Short-Term Outcome 1: There is increased provision and uptake of resources, support and learning opportunities about self-harm for people, communities, and settings to help develop greater knowledge, awareness and compassionate understanding of self-harm.
Action 1.1: Provide learning for people, communities, services and healthcare settings using existing networks and building upon the bespoke self-harm resources already created which align with Trauma Informed and Time, Space, Compassion approaches.
Short-Term Outcome 2: Resources, support and learning opportunities are targeted and tailored to meet the needs of key professional groups and sectors.
Action 1.2 Explore further opportunities to include safe and evidence-based self-harm learning content and materials.
Short-Term Outcome 3: More resources, support and learning opportunities are co-designed with people with lived experience and key partners, to ensure they meet the needs of marginalised communities and groups at higher risk of self-harm.
Action 2.1 Work with key partners, including with people with diverse lived experience, to tailor and disseminate national resources and support to ensure they effectively reach communities who are at higher risk of self-harm. This work will support local approaches and seek to tackle stigma and discriminatory practices.
(this action builds on work in Priority 2 but also contributes strongly to Short Term Outcome 3)
Priority 2: Continue to build person-centred support and services across Scotland to meet the needs of people affected by self-harm.
Short-Term Outcome 4: Increased availability and promotion of bespoke self-harm support, including online and peer support.
Action 2.2 Share and encourage uptake of self-harm resources and support, including online and peer support. We will give specific consideration to people who support someone who self-harms, in whatever their role.
Short-Term Outcome 5: More existing services and settings will offer and deliver effective, compassionate and non- stigmatising self-harm support.
Action 2.3. Continue to build compassionate responses for people accessing clinical services (including as part of assessment and treatment).
Short-Term Outcome 6: Increased collaboration, sharing of best practice and learning to support continuous improvement in existing and new services.
Action 2.4. Encouraging all partners including people with lived experience, to work together to provide person-centred and compassionate care with a focus on recovery.
Priority 3: Review, improve and share data and evidence to drive improvements in support and service responses for people who have self-harmed or are at risk of doing so.
Short-Term Outcome 7: Currently available data, data gaps and limitations on self-harm are identified and reviewed across a broad range of settings, including those where risks of self-harm may be highest.
Action 3.1. Identify what data (including equalities data) is routinely collected on self-harm across a range of settings (e.g. primary care, secondary care, unscheduled care, social care, justice and education) and identify what is missing and seek ways to improve
Short-Term Outcome 8: Increased availability and promotion of emerging self-harm research.
Action 3.2. Take steps to gather existing and new data and evidence on self-harm to improve support and service responses for people.
Priority 1
Priority 1: Continue to expand and deepen knowledge and compassionate understanding of self-harm and tackle stigma and discrimination
Short term outcomes (initial 18 months)
- 1: There is increased provision and uptake of resources, support and learning opportunities about self-harm for people, communities, and settings to help develop greater knowledge, awareness and compassionate understanding of self-harm
- 2: Resources, support and learning opportunities are targeted and tailored to meet the needs of key professional groups and sectors.
- 3: More resources, support and learning opportunities are co-designed with people with lived experience and key partners, to ensure they meet the needs of marginalised communities and groups at higher risk of self-harm.
Short-term Outcome 1:
There is increased provision and uptake of resources, support and learning opportunities about self-harm for people communities and settings to help develop greater knowledge, awareness and compassionate understanding of self-harm.
Primary Actions:
1.1. Provide learning for people, communities, services and healthcare settings using existing networks and building upon the bespoke self-harm resources already created which align with Trauma Informed and Time, Space, Compassion approaches. Our learning priorities will:
a) Provide information and increase compassionate understanding about self-harm.
b) Dispel myths about self-harm.
c) Challenge stigma and discriminatory practices.
d) Increase compassion and confidence in responding and supporting someone who has self-harmed in a non-judgemental way.
e) Share information about online aspects of self-harm including the role and influence of online platforms in the lives of those who self-harm, supports available, unique risks posed, and ways to manage risk.
f) Promote the uptake of wellbeing support for people who care for someone who has self-harmed.
Achievements so far:
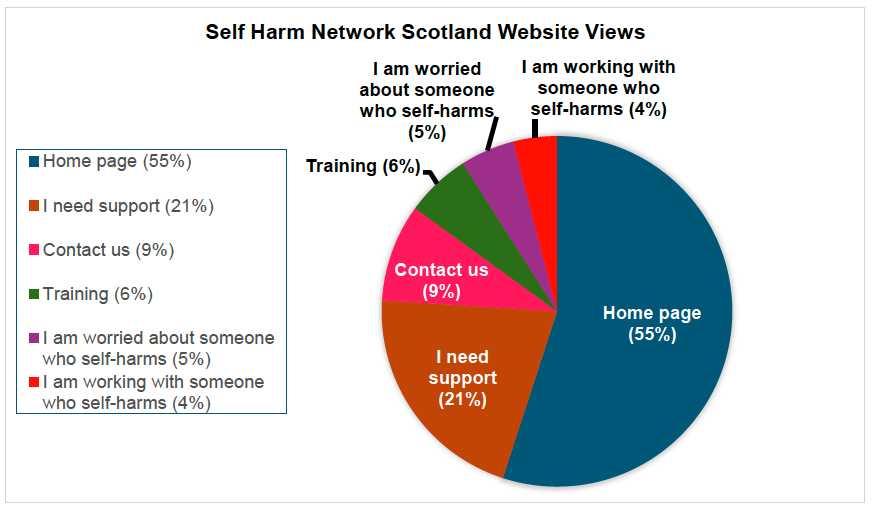
- The SHNS Website launched in March 2023 and serves as a central access point for information, support, and training related to self-harm. In the first 18 months of the strategy implementation, the website has received 278,023 page views from 26,727 individual users. The website also offers a range of tools designed to help people better understand their self-harm and explore various strategies and techniques for managing it. Over the past 18 months, tools to support with managing self-harm have been downloaded 860 times.
- SHNS have also produced 17 videos of Peer Practitioners discussing a range of topics that aim to increase understanding of self-harm by tackling some assumptions and stereotypes and explain more about the support available from SHNS.
- The SHNS Self-Harm Awareness Training is designed to enhance participants’ understanding of self-harm and to equip them with the knowledge, skills, and confidence to offer a compassionate and informed response. Over the past 18 months, 276 training sessions have been delivered to 3,380 people in both national and local organisations. To date, SHNS have trained locality organisations in 25 out of 32 local authorities across Scotland as well as through a number of health boards including rural and island areas of NHS Highland and NHS Orkney. Participants have represented a wide range of professional backgrounds, including:
- Education, and child and family support
- Social Work
- Primary and secondary healthcare
- Mental health services and support
- Victim and counselling support services
- Carer and disability support
- Housing support
- SHNS’s training package has been developed using a range of resources, feedback, and research, including Penumbra’s existing materials, NHS GGC’s ‘What’s the Harm?’ course, Time, Space, Compassion and lived experience insights. The programme has been regularly evaluated and refined based on participant feedback. SHNS have also worked with the British Deaf Association and the National Autistic Society to improve accessibility and including adding more visual content. All materials are kept up to date with national research and policy, and are fully referenced to ensure transparency and academic integrity.
- Training evaluation found that 97% of training participants who completed the end of training feedback (46% of all training attendees) agreed or strongly agreed that they feel more able to compassionately respond to a person who is self-harming and 96% had increased understanding of the stigma associated with self-harm. This aligns with the overall vision of the Strategy, that people who have self-harmed, or are thinking of self-harming, received compassionate, recovery focused support, without fear of stigma or discrimination.
- Further data from the training participants who completed the end of training survey showed participants felt they had increased understanding of:
- Different types of self-harm (99%)
- Self-harm as a coping strategy (98%)
- Where help and support exists for people who self-harm (99%)
- Underlying causes of self-harm (97%)
- Functions of self-harm (98%)
Spotlight on Island Areas
Engaging and Equipping Island areas
SHNS trainers spent 4 days on Orkney delivering 4-full-day training sessions to 48 participants from 15 organisations, an information session for 5 parents, and provided a drop-in session at a youth café which was attended by 7 young people.
“Really excellent training. [Trainer] was excellent- informative, friendly and approachable. Her real-life examples really brought the material to life in an understandable way. Although I already had a decent knowledge of self-harm, I feel like the training has broadened and deepened my understanding significantly. Thank you! Would highly recommend it to other professionals.”
Following on from the success of the training in Orkney, SHNS have since had training requests from both the Shetlands and the Western Isles, and the training team will be travelling to Shetland to deliver 3 full days of training in autumn 2025.
Short-term Outcome 2:
Resources, Support and Learning Opportunities are targeted and tailored to meet the needs of key professional groups and sectors
Primary Actions:
1.2. Explore further opportunities to include safe and evidence-based self-harm learning content and materials in:
a) Core training and continuous professional development for key professional groups.
b) Schools and further and higher education.
c) Parenting and family support programmes and resources.
Achievements so far:
- In the first 18 months of the strategy implementation, the implementation team - comprising the Scottish Government, COSLA, and SHNS - has undertaken extensive work to raise awareness of self-harm and disseminate key resources. This engagement has sought to ensure that a variety of professional groupings, working across a range of community and service settings, have access to support to increase their understanding of self-harm - enabling them to offer more compassionate responses. This intensive awareness-raising work recognises the multiple opportunities professionals across a range of sectors and settings have to support someone affected by self-harm. This work has included presentations and contributions to a wide range of conferences and professional networks spanning Social Work, Education, Children and Young People and other areas.
- We have reached over 160 professionals through the Provider Network, a national network of individuals who have an interest in or deliver services supporting people affected by self-harm. Hosted by Self-Harm Network Scotland, the Provider Network has grown from a core group meeting quarterly to an events-based network with national reach. Recent events have focused on ‘Looking after yourself when supporting people who self-harm,’ and evaluations show that 91% of attendees who completed feedback (43% of attendees) agreed or strongly agreed that they feel more equipped to look after themselves while supporting others.
- SHNS has developed a set of professional wellbeing resources specifically for professionals supporting people who self-harm. The dedicated webpage I am working with someone who self-harms has been viewed 2971 times in the past 18 months.
- The Scottish Government took proactive steps to inform and re-assure the self-harm support community about the implications of the new offence in the Online Safety Act via a Ministerial Letter in January 2024.
- To provide support across unscheduled and primary care, Resources for Mental Health in Unscheduled Care Services and Mental Health and Wellbeing in Primary Care Services were published in December 2024 providing a directory of additional sources of help, training and support relating to self-harm.
- Co-produced by NHS Education for Scotland (NES) and Public Health Scotland (PHS), the Ask, Tell, Respond (ATR) education resources support the implementation of Scotland’s Public Health Priorities for Mental Health by helping staff across sectors develop skills to prevent mental ill health, self-harm, and suicide.
Between 28 November 2023 and 28 May 2025, 4,654 learners completed the adult Ask, Tell Respond eLearning module, while 864 completed the module focused on promoting mental health and preventing self-harm and suicide in children and young people. These informed level resources are accessed by staff across health, social care, the third and independent sectors, and are also in use by staff and students in 14 higher education institutions and 7 further education colleges in Scotland. NES is continuing to work with education providers to test uptake and engagement with both the adult and children and young people’s modules.
At the Skilled level NES offer Learning Byte 4, which focuses on supporting a person at risk of self-harm. This resource was accessed and downloaded 2,899 times in the first 18 months of the strategy implementation. In the same period, the Skilled Level Facilitation Resource was taken up by 17 organisations across seven NHS Boards and one local authority area. Facilitators delivering this content locally are supported through a national facilitator network hosted by NES and PHS.
- NHS Education Scotland (NES) has also worked with the University of the West of Scotland to embed self-harm education throughout its three-year BSc Adult and Mental Health Nursing programmes.
- Within schools and further and higher education, there has been a range of information disseminated, and events held to share information, learning and materials about self-harm. This includes active work with relevant professional associations working with young people, and engagement with staff and young people across a variety of educational settings including schools, colleges and universities. As part of the partnership between Breathing Space, University of Strathclyde and Glasgow University, SHNS’s sticker campaign successfully reached over 30 colleges and universities in Scotland, sparking new conversations around self-harm. Feedback from with professionals to date has indicated that resources made available through the strategy are helpful in supporting their practice.
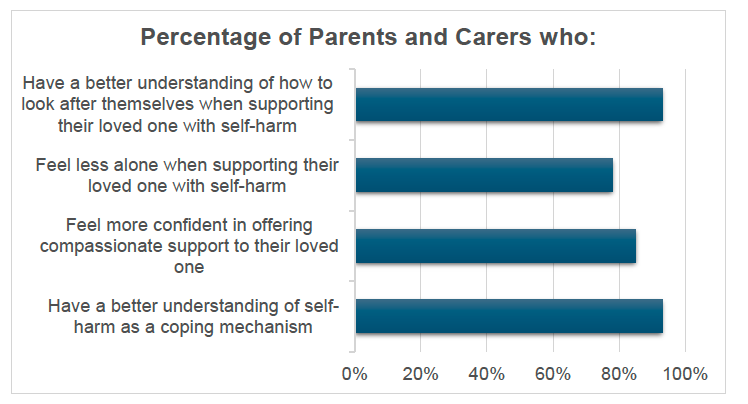
- For parents and carers, the SHNS Loved Ones Support groups were launched in April 2024 to provide information and support to people who support someone who is self-harming. Since its launch, six groups have been run with 48 people signing up and 25 attending all four sessions. Evaluation of the group showed that parents and carers felt better placed to support and manage when caring for someone who self-harms.“I learned so much from the sessions and from the others in the group. The opportunity to talk to other people (parents especially) going through the same experiences with their loved ones was so validating, heart-warming and helpful...Our relationship has grown closer as a result of the information I learned…”
“I learned so much from the sessions and from the others in the group. The opportunity to talk to other people (parents especially) going through the same experiences with their loved ones was so validating, heart-warming and helpful...Our relationship has grown closer as a result of the information I learned…” Loved Ones Participant
- There have been self-harm support information and resources disseminated with a range of parenting organisations including Parentclub, Parenting Across Scotland, and Connect. In addition, SHNS has delivered awareness sessions for parents, carers and loved ones in collaboration with a number of local organisations including those supporting transgender, autistic, deaf and care experienced children and young people.
Short-term Outcome 3:
More resources, support and learning opportunities are co-designed with people with lived experience and key partners, to ensure they meet the needs of marginalised communities and groups at higher risk of self-harm.
Primary Action:
2.1 Work with key partners, including with people with diverse lived experience, to tailor and disseminate national resources and support to ensure they effectively reach communities who are at higher risk of self-harm. This work will support local approaches and seek to tackle stigma and discriminatory practices. There will be an initial focus on:
a) Children, young people and families, including care experienced children and young people.
b) Marginalised groups where self-harm may be more prevalent, initially LGBT+ and neurodivergent people.
c) People who may face additional barriers to getting the help they need. For example, people experiencing trauma and those with severe and enduring mental illness.
d) People in higher risk settings, (such as, care experienced children and young people, people in prisons, or those experiencing homelessness).
(this action sits under priority 2 but contributes strongly to Outcome 3. We have placed it in this section and also included it under priority 2 for our overall assessment, representing the relational and complex nature of this work)
Achievements so far:
Dissemination work includes:
- COSLA hosted a session for the Local Government Promise Leads Network, focused on mental health and wellbeing of those with care experience, sharing information on available self-harm resources and support.
- SHNS have been working collaboratively with a wide range of settings, organisations and groups to test and tailor resources, ensuring they are responsive to the specific needs of diverse populations. Below are a number of illustrative (but not exhaustive) examples of this work:
- Attended a drop in session at the Orkney Blide Trust youth group to understand the experiences of young people living in an island community and to help shape the design of future services and supports.
- Delivered a training session to staff at the Kibble Education and Care Centre and plans to continue to work in partnership with Kibble and other organisations in the secure care settings to continue to embed a compassionate response to self-harm.
- Working with Hope for Autism and the National Autistic Society (NAS), to tailor learning resources to meet the needs of autistic people who self-harm.
- SHNS also hosted a stall at the 2024 Young Carers Festival, sharing information and resources with those in attendance, and provided a drop-in session at the University of the Highlands and Islands.
- Worked in partnership with the British Deaf Association (BDA) to create a British Sign Language (BSL) hub on the SHNS website. The hub contains videos of all SHNS website resources which have been translated into BSL (17 videos in total), and these have been viewed over 1,200 times. SHNS has delivered multiple training sessions to a range of BDA stakeholders during the partnership and have also delivered a session with the Deaf Roots & Pride Transitions team.
- Worked with key professional groups to tailor their training to ensure it meets the specific needs of staff and service users within specific settings. This includes tailoring training with The Scottish Prison Service and the Scottish Ambulance Service.
- Developed a partnership with a local veterans’ centre, attending weekly sessions which helped reduce stigma, leading to stronger trust and increased willingness to seek support.
- Developed a relationship with Dumbarton Rock Recovery Group which supports in substance use recovery, and began attending their recovery cafe twice a month when capacity allowed.
Spotlight on Engaging in High-Risk Settings
Scottish Prison Service (SPS)
SHNS and SPS are working collaboratively to develop a training package which can be rolled out to SPS staff. As with all SHNS training, it is intended to provide staff with the confidence, knowledge, resources and tools that equip them to provide a compassionate response to people care who are self-harming.
The unique environment and context of prison settings means that the standard SHNS training requires tailoring to ensure the learning approach and resources are relevant, effective and can be operationalised in a prison environment. To achieve this SHNS have been working with a focus group of prison staff from across the SPS estate, the team have developed bespoke training slides, trainer manuals, SPS-specific case studies, and will include a recovery video featuring a person with lived experience of self-harm in a prison setting.
Priority 2
Priority 2: Continue to build person-centered support and services across Scotland to meet the needs of people affected by self-harm.
Short term outcomes (initial 18 months)
- 4: Increased availability and promotion of bespoke self-harm support, including online and peer support.
- 5: More existing services and settings will offer and deliver effective, compassionate and non-stigmatising self-harm support.
- 6: Increased collaboration, sharing of best practice and learning to support continuous improvement in existing and new services.
Short-term Outcome 4:
Increased availability and promotion of bespoke self-harm support, including online and peer support.
Primary Actions:
2.2 Share and encourage uptake of self-harm resources and support, including online and peer support. We will give specific consideration to people who support someone who self-harms, in whatever their role, with an initial focus on:
a) Informal support networks including friends and family members such as parents and carers, and partners.
b) Staff and volunteers who are likely to provide self-harm support to someone though the course of their work.
Achievements so far:
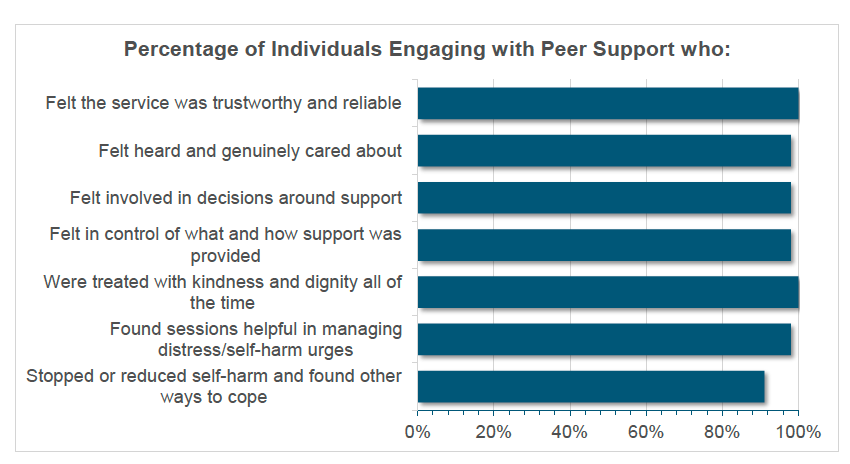
- SHNS Peer Support service offers flexible, person-centred, and non-judgemental support that is grounded in recovery principles and delivered by peer practitioners with lived experience. Typically, supported people engage in 7 to 8 one-hour sessions, during which their own goals, values, and definitions of progress are central to the support process. Rather than focusing solely on reducing self-harm, the service supports individuals to explore and understand their experiences, such as the functions and cycles of self-harm and to develop tools that promote wellbeing, safety, and alternative coping strategies. Effectiveness is not narrowly defined by the cessation of self-harm, but instead by what matters most to the individual. This may include outcomes like improved emotional regulation, increased self-awareness, or strengthened support networks. Further insights into how supported individuals experience and evaluate the service can be found in Figure 4.
- In the first 18 months of the strategy implementation:
- 491 referrals to one-to-one peer support were received by SHNS
- 369 people accessed one to one peer support
- 2,988 support sessions were delivered
- SHNS Live Chat support is available from 6pm-10pm, 7 days a week providing immediate support to people who self-harm. As such this support is available outside the normal operating hours of many statutory support services. During the chat the team of peer practitioners and volunteers will support people to manage their current distress, discuss issues around their self-harm, explore alternative coping strategies and discuss how to access support in other services where that is needed.
- In the first 18 months of the strategy implementation:
- 1,790 people accessed the Live Chat
- 833 people engaged in a support conversation
- 88% of people who completed end of chat feedback (33%) rated the support very or somewhat helpful
- Self-Harm Network Scotland use a variety of social media platforms to raise awareness of the service and to decrease stigma around self-harm. Additionally, a recent ad campaign reached 14,000 people, with 22,631 total views and in the two months following the ad, referrals increased by 29%.
Spotlight on Peer Support
Using the Live Chat and one-to-one support: B’s recovery story
- I first started using the SHNS online Live Chat - I knew I needed help, but I was still scared to ask. Using the online chat and speaking to someone helped me every time that I felt I was about to relapse. I finally realised I needed help, and I completely wanted to stop self-harming. I started my support session with the loveliest lady ever. She made me feel welcomed, supported and not judged. Whenever I’ve opened up to someone in the past, they have used it against me, which meant that I was very wary to opening up again. But when I did, I felt beyond amazing.
- The support from Penumbra has been amazing, my self-confidence has gone up so much (which is something I’ve really struggled with), I haven’t relapsed in 100 days – that’s over 3 months! My attitude towards things has changed. I’m actually looking after myself which I’m not used to doing.
Understanding more about my self-harm: Claire’s recovery story
- Now, I understand so much more about self-harm and ways to distract myself. Susan also helped me to understand why I was self-harming and showed me alternative coping strategies. My favourite is reading the affirmations I made. The support has made me feel relieved that I had someone who I could talk to that understands me.
- I have reduced my self-harm more than I ever thought possible. I don’t even remember the last time I self-harmed. I feel like I am more confident and less embarrassed when talking to others, so it has really improved my confidence.
Using my own lived experience- Peer Practitioner perspective
- It helps them [supported people] to worry less about being judged negatively for their self-harm. I often also hear a sense of relief from people I am supporting that someone else ‘gets it’ – it’s a normalising of experiences that they previously felt they were alone in having. There is also an element of hope in seeing that people can and do overcome these difficult things. (Peer practitioner)
- Using my lived experience for me feels like I have been able to use some of my worst times to hopefully support others. It’s not that those times were ‘worth’ it but that is what life is, lots of experiences, good and bad, and I am glad to have a purpose for the not-so-great ones. (Live Chat volunteer)
Short-term Outcome 5:
More existing services and settings will offer and deliver effective, compassionate and non-stigmatising self-harm support.
Primary Action:
2.3. Continue to build compassionate responses for people accessing clinical services (including as part of assessment and treatment). This will include:
a) Working with first responders, for example emergency services and unscheduled care, and staff working in other healthcare settings such as, primary care, mental health services, liaison psychiatry, and the Child and Adolescent Mental Health Service (CAMHS).
b) Providing evidence and support to services to embed the National Institute for Health and Care Excellence (NICE) and The National Confidential Inquiry into Suicide and Safety in Mental Health (NCISH) self-harm guidelines and recommendations, relevant to the Scottish context. This could include psychosocial assessments, safety planning, provision of psychosocial interventions and psychological therapies in line with the Psychological Therapies Matrix. This will ensure that people in suicidal crisis are identified early and provided with appropriate support.
c) Providing specialist support and interventions for those with severe and enduring mental illness and more complex needs, through interface services such as liaison psychiatry.
d) Investigating opportunities to improve post self-harm care to address medical and broader health and wellbeing needs resulting from self-harm.
Achievements so far:
- Through the Mental Health Unscheduled Care Network, Scottish Government has completed a national review of Psychiatric Emergency Plans (PEPs) to consider how they should be used across Scotland. This has included specific focussed work on improving compassionate responses to self-harm. PEPs are local protocols designed to guide the immediate response of services when a person is at risk of detention, ensuring timely, coordinated, and effective care. In response to the review, the Scottish Government, supported by the Network and the Working Group, are developing national PEP guidance and a template to improve national consistency, make plans easier to use, clearly define local roles and responsibilities, and processes. The guidance is intended to include specific measures to strengthen multi-agency working in situations where someone has self-harmed and may be at risk of detention. Input from people with lived experience is being actively sought to ensure the guidance is appropriate, and person-centred. Further engagement with wider stakeholders on the draft national guidance and national template will also take place prior to publication. To improve the response to mental health distress and crisis—and to strengthen how services and emergency responders work together—the Scottish Government and national partners have set out a clear framework for action.
- In February 2025, the Scottish Government published the Framework for Collaboration to Improve Mental Health Distress and Crisis Response, and the Mental Health and Policing Partnership Delivery Group published a cross-sector Collaborative Commitment Plan. These plans include specific reference to self-harm and build on the progress of the Mental Health Unscheduled Care Programme, supporting services to work more effectively across boundaries and deliver a more coordinated, compassionate response to people in distress
- Scottish Government have worked as part of a national partnership team, led by Suicide Prevention Scotland, collaborating with several Health Boards to support the implementation of guidelines from NICE and NCISH to improve the assessment and care of people who self-harm and family and carer involvement. We have contributed evidence and content on self-harm to the programme of awareness raising sessions on the guidelines. Sessions have been delivered to a range of key professional groups, including the Royal College of Psychiatrists’ Scottish Liaison Psychiatry Network, Mental Health Nursing Leads, the Mental Health Unscheduled Care Network, and the Heads of Psychology Group.
Short-term Outcome 6:
Increased collaboration, sharing of best practice and learning to support continuous improvement in existing and new services.
Primary Actions:
2.4 Encouraging all partners including people with lived experience, to work together to provide person-centred and compassionate care with a focus on recovery. To achieve this we will:
a) Develop a professional ‘self-harm community of support’ that provides opportunities to make connections, share good practice and learning between communities, various settings and healthcare services. This will include hosting a self-harm conference and taking action to grow the existing self-harm network.
b) Encourage cross-sector communication and collaboration between support organisations and service partners. This includes with services and settings that support people who engage in other forms of health-harming behaviours (that might be considered self-harm) for example, eating disorders, substance use, alcohol use and gambling.
c) Use Getting It Right for Every Child (GIRFEC) and Getting it Right for Everyone (GIRFE) tools to support multi-agency approaches, where relevant.
d) Identify and open up opportunities for practitioners to inform relevant national and local policies to strengthen links and share learning and good practice.
Achievements so far:
- The Provider Network has been established, this is a national network of professionals who have an interest in, or deliver services that support, people who may be affected by self-harm. The network comprises third sector and statutory organisations which provide a range of support in the community, including to people at highest risk of self-harm. The aims of the network are to:
- establish relationships and identify opportunities to deepen understanding of self-harm, reduce stigma, discrimination and promote compassionate responses.
- plan and deliver self-harm awareness events, regional and national conferences.
- work with Scottish Government, COSLA and relevant professional associations to raise awareness with networks within schools, educational establishments, third sector, NHS services, and other organisations working with children, young people and adults to deepen understanding, reduce stigma and improve responses to self-harm.
- share learning, data and evidence, effective approaches, resources and tools with provider organisations, primary care, people working in unscheduled care so that compassionate responses are provided to people who self-harm.
- As part of the work to support implementation of NICE and NCISH guidelines we have worked alongside Suicide Prevention Scotland to develop a shared evidence bank. We have also worked together to deepen our collective understanding of how intersectional inequalities - such as discrimination, stigma, marginalisation, and barriers to healthcare – have an impact on risk, care and recovery for people impacted by suicidality or self-harm. As part of this work, we also supported delivery of a series of thematic learning sessions, including:
- A session with the Mental Welfare Commission’s lived experience team on effective involvement of families and carers;
- A workshop with See Me on intersectional stigma and discrimination in mental health;
- A presentation by Professor Nav Kapur (NCISH) on current trends and evidence in psychosocial assessment and risk management;
- A session with Dr Dan Warrender (Abertay University) on lived experience and ethical practice in supporting individuals and their families, where there is a diagnosis of Borderline Personality Disorder;
- Learning exchanges with English NHS Trusts leading in this area of practice improvement.
- Work is underway to share self-harm information and support with partners who are working to support people who engage in other health harming behaviours that may also be considered forms of self-harm. This includes collaborative efforts with stakeholders across working on drug and alcohol, eating disorders, and gambling policies.} SHNS has also been actively sharing information about self-harm, and the resources, tools and support that are available to people affected by self-harm through presenting to GamCare and attending a Scottish Drug Forums emerging practice event. Furthermore, SHNS has delivered Self-Harm Awareness training to North West Recovery Communities and Scottish Families Affected by Alcohol and Drugs.
- SHNS has also been actively sharing information about self-harm, and the resources, tools and support that are available to people affected by self-harm through presenting to GamCare and attending a Scottish Drug Forums emerging practice event. Furthermore, SHNS has delivered Self-Harm Awareness training to North West Recovery Communities and Scottish Families Affected by Alcohol and Drugs.
Priority 3
Priority 3: Review, improve and share data and evidence to drive improvements in support and service responses for people who have self-harmed or are at risk of doing so.
Short term outcomes (initial 18 months)
- 7: Currently available data, data gaps and limitations on self-harm are identified and reviewed across a broad range of settings, including those where risks of self-harm may be highest.
- 8: Increased availability and promotion of emerging self-harm research.
Short-term Outcome 7:
Currently available data, data gaps and limitations on self-harm are identified and reviewed across a broad range of settings, including those where risks of self-harm may be highest.
Primary Actions:
3.1. Identify what data (including equalities data) is routinely collected on self-harm across a range of settings (e.g. primary care, secondary care, unscheduled care, social care, justice and education) and identify what is missing and seek ways to improve this: This could include:
a) Scrutinising the quality and relevance of the data collected.
b) Establishing how this data is currently being used and whether there is transferable learning that can be used for other settings.
c) Identifying what data and evidence is missing about self-harm and seek ways to improve.
Achievements so far:
- To better understand the available qualitative evidence from a lived experienced perspective, a meta-ethnographic study was completed by the University of Edinburgh. This has improved our understanding around the context of self-harm data by reviewing qualitative evidence from the UK. This study found that:
- Self-harm can have wide-ranging and long-term effects on people’s lives: relationships, employment, and sense of self
- Self-harm methods, meanings and experiences are nuanced and diverse. This underscores the importance of avoiding assumptions about what self-harm ‘looks like’, who self-harms, and why they may do so.
- There are complex and varied reasons behind self-harm (including how far self-harm is – and is not – related to suicide)
- Non-judgemental, person-led support can help, especially were this recognises that ‘recovery’ can have different meanings for different people
- There is a lack of qualitative evidence/data for younger people (16 and below), older adults, individuals from disadvantaged communities and for people from racialised minority groups
- Experiences of accessing self-harm information online were mixed, and could be both helpful and harmful.
- To further broaden understanding around the quality of available data, Public Health Scotland undertook a review of its self-harm related data. This included assessing its completeness, quality and potential applications. Although the health service data on self-harm faces a number of issues which means presenting a national picture of incidence and/or prevalence is challenging, the review provided:
- an overview of previous investigations and the current status of numerous data sources, including A&E, acute and psychiatric hospital admissions, Distress Brief Interventions and the Child, Adolescent and Psychological Therapies National Dataset.
- potential data developments, as well as information on approaches to self-harm data analysis outside of Scotland.
The work concluded that improving self-harm data will require careful consideration across a number of factors. The Data and Evidence Group will continue to support PHS to identify and implement improvements over course of this strategy.
- To help support access to quality data, Public Health Scotland (PHS) has developed a pilot online evidence and gap map (EGM) on the subject of self-harm in children and young people, including what is known about risks and protective factors associated with self-harm; and what interventions or policies could work for secondary prevention.
The map provides an interactive, visual representation of evidence – and highlights what evidence exists and gaps which require further research. This map increases access to quality research around self-harm, supporting professionals to explore the landscape.
In the early stages of the EGM development, Public Health Scotland used the associated rapid review of review-level evidence to publish an evidence briefing on factors associated with self-harm in childhood, based on 15 included reviews. This literature review is supporting policies and practice when considering preventative responses to self-harm in childhood.
The evidence synthesised in the briefing:
- suggested the need for self-harm prevention policies focused on supporting healthier familial and peer relationships for children, and
- concluded that understanding individual risk factors could provide direction for prioritising service development aimed at primary or secondary prevention rather than harm reduction.
Spotlight on Lived Experience Data
Professor Amy Chandler (University of Edinburgh) and Ms Lisa Quigley conducted a meta ethnography of peer-reviewed qualitative research in the UK. The review asked:
1. How do people who self-harm make sense of self-harm (functions and meanings)?
2. How is self-harm related to other social factors in qualitative literature?
3. What experiences do people who self-harm report with services?
4. What messages does this work pose for the self-harm strategy in Scotland?
Theme 1: Context and Culture
Studies reviewed commonly connected experiences of self-harm to a range of contextual and cultural factors. This included experiences of:
- The negative impacts of the characterisation of self-harm as being a practice engaged in by ‘young women’.
- The role of social media in understanding self-harm experiences.
- Portrayal of self-harm in relation to victimisation; and
- Self-harm in relation to particular institutions (prisons, schools, residential units).
Theme 2: Narrating the unspeakable
Participants across the reviewed studies articulated challenges with talking about, explaining and understanding self-harm. Several different, and sometimes contradictory, ‘functions’ of self-harm were shared including:
- Compulsion and control – these functions could co-occur for participants.
- Self-harm was described in relation to suicide – both as part of a ‘suicidal practice’ but also, often, as a way of avoiding or postponing suicide.
- Description of self-harm as both dramatic and mundane; and
- Bodily aspects of self-harm, with sensations being important to understanding ‘why’ self-harm was practiced.
Theme 3: Changed landscapes
This theme addressed the ways that self-harm contributed to changes in the lives of those who had self-harmed. This incorporated changed relationships, changed relationships to the self, and altered future trajectories, especially employment:
- Scars, stigma and shame – including impacts that visible evidence of self-harm had on their relationships with others.
- Navigating the world following self-harm - again addressing responses to self-harm from others but especially attending to future-orientations and employment.
- ‘Recovery’ and self-harm cessation - competing accounts pose challenges for many approaches to treating and responding to self-harm in policy and practice; and
- Accounts of care for self-harm - participants reported experiences with ‘care’ that were perceived as harmful or, at best, unhelpful. Approaches that were described as more helpful centred on a non-judgemental approach that was open to diverse meanings and led by the individual who self-harmed.
Short-term Outcome 8
Increased availability and promotion of emerging self-harm research.
Primary Actions:
3.2. Take steps to gather existing and new data and evidence on self-harm to improve support and service responses for people. This could include:
a) Identifying existing and new research and learning on self-harm, ensuring this is shared and incorporated into support and service practice, where relevant.
b) Exploring early intervention approaches and investigating what support would be beneficial to people considering self-harm, (i.e., to prevent first episode of self-harm or reduce repetition of self-harm).
c) Continuing to identify what factors put people at increased risk of self-harm and what can be done to mitigate against risks and increase help-seeking with a specific focus on racialised and other marginalised communities.
d) Continuing to improve understanding of self-harm within the digital landscape, including how online platforms are accessed as a means of support and their role in the lives of those who self-harm. Build awareness of their potential to increase risk, and of the mechanisms driving harmful impacts. Monitor the use and impact of the Online Safety Act 2023 offence of encouraging or assisting self-harm as a means to keep people safe from harm.
e) Using learning from the Self-Harm Network Scotland to inform developments in peer and online support.
f) Investigating if self-harm can be a barrier to accessing support and services and what measures can be taken to overcome these barriers.
Achievements so far:
- The Scottish Government’s Mental Health Analytical team conducted a rapid evidence review and survey of practitioner perspectives to investigate if self-harm can be a barrier to accessing support and services, and what measures can be taken to overcome these barriers. The evidence review examined barriers and facilitators to accessing and engaging with self-harm support, while the survey gathered insights from practitioners about barriers to a broader range of services. The research found that people who self-harm often face multiple barriers when trying to access and engage with support, including stigma, fear of judgment, restrictive service eligibility criteria, and long waiting times. Importantly, the findings highlight that these barriers apply not only to mental health care, but also to wider support and services such as housing or financial services. Despite these challenges, the research also identified several facilitators that can improve access and engagement. These include person-centred, compassionate approaches and more inclusive eligibility criteria.
- Work led by NHS Greater Glasgow and Clyde (see spotlight) has strengthened our understanding of good and emerging practice in responding to self-harm. This work has broadened awareness among professionals working both directly and indirectly with self-harm by exploring how young people typically present to services and highlighting the complex links with issues such as social media use.
- National data provides a degree of insight into where and how many children and young people are accessing available supports and services to seek support with self-harm. This includes agreed annual data collection on school counselling and community-based support. For example, data on community supports and services for children, young people and families and school counselling from July 2023 to March 2024 was published 30/6/25 This indicates that across this period 2,337 children and young people sought support for self-harm through school counselling and 1927 individuals sought self- harm support through community-based supports and services. Whilst providing a useful insight into the range of issues young people seek support for this data does not provide information on self-harm beyond this.
- Local approaches to collect and utilise data on self-harm are also undertaken in order to understand and meet local need. For example, between 2020 and 2025 Shine mental health surveys have been utilised in 6 local authority areas to provide a better understanding of self-harm locally.
- SHNS shares learning through its annual impact report, which is published on its website and promoted through targeted communications, including bite-sized extracts highlighting key findings. This is supported by partners such as the Scottish Recovery Network, who help amplify the report through social media. Key insights are also shared directly with the provider network to support service development.
Spotlight on Greater Glasgow and Clyde
A programme of work was completed in NHS Greater Glasgow & Clyde which has increased our understanding of self-harm in relation to social media, patient journeys and health needs. This included:
- A review of the literature on Social media - its use and impact on mental health and wellbeing on young people, with a focus on self-harm and suicidality. It provides an update on the state of knowledge about social media usage and shares insights into its potential for both harm and good.
- Using the Child and Adolescent Patient Tracking and Notification (CAPTN) Dataset and local data to investigate the profile of young people who have suicidal thoughts or who self-harm and are referred to CAMHS, and their patient journeys in CAMHS. The study found young people being referred regarding self-harm from age 12, peaking between 14 and 15 years old, with females in the large majority. The review identified four ‘types’ of patient journey from 1) referred but did not attend themselves (although a caregiver may attend), 2) young person seen once, 3) seen over a significant period, or 4) seen over a very significant period. These four types of journeys underscore the need for support and assessment that is tailored to the needs of young people and their caregivers.
- A Health Needs Analysis was conducted in relation to self-harm in children and young people in NHS Greater Glasgow and Clyde. This work sought to assess the needs of children and young people who self-harm in NHSGGC. Through a combination of information sources including: surveys, service data, academic literature, interviews and focus groups of teachers and mental health workers, the report builds a picture of self-harm as a common, impactful and likely increasing issue amongst our young population.
- An exploratory project to investigate the lived experience of young people with experience of self-harm using social media. It involved a series of focus groups with young people aged 16-23. The report provides novel insights into the complex and nuanced relationship between social media use and self-harm among young people. This will help to support organisations and professionals in having a deeper understanding of the interplay between self-harm and social media usage.
Contact
Email: Harriet.Waugh@gov.scot