Independent Review of Audiology Services in Scotland
Review report and recommendations from the Independent Review of Audiology Services in NHS Scotland. The Review was announced by the Scottish Government in January 2022 in the context of failings in the standards of care provided in the NHS Lothian Paediatrics Services.
Part of
Structure, Governance and Leadership Sub-Group
Key points
- A survey gathered views of heads of service on the structure, governance and leadership of services.
- Services were generally traditional and hierarchical in structure.
- Some services were staffed by a single audiologist.
- There was considerable variation in staffing levels between services.
- The range of services provided was generally consistent.
- Concern was expressed about service visibility.
- Audiology appears to lack clear and established governance locally.
- Most heads of service maintain a clinical role, which is likely to impact on the time they have available to lead and manage.
- Some Boards have little knowledge of what their audiology service does but events in NHS Lothian have increased awareness of the need for oversight.
Introduction
Audiology services are delivered by all of NHS Scotland’s 14 territorial Boards. In two Boards paediatric and adult services are separated. In addition, and due to a historical arrangement associated with the management of the service, Argyll and the Isles has been included as a separate service delivering audiology services in that geographical region, although it is formally part of NHS Highland.
Methodology
At the end of 2022, the Structure, Governance and Leadership Sub-Group sent the heads of service of Health Boards a questionnaire to gather information on those three themes. The questions can be found in Appendix A. The first section of the questionnaire focused on structure and the key findings are set out below.
Findings – structure
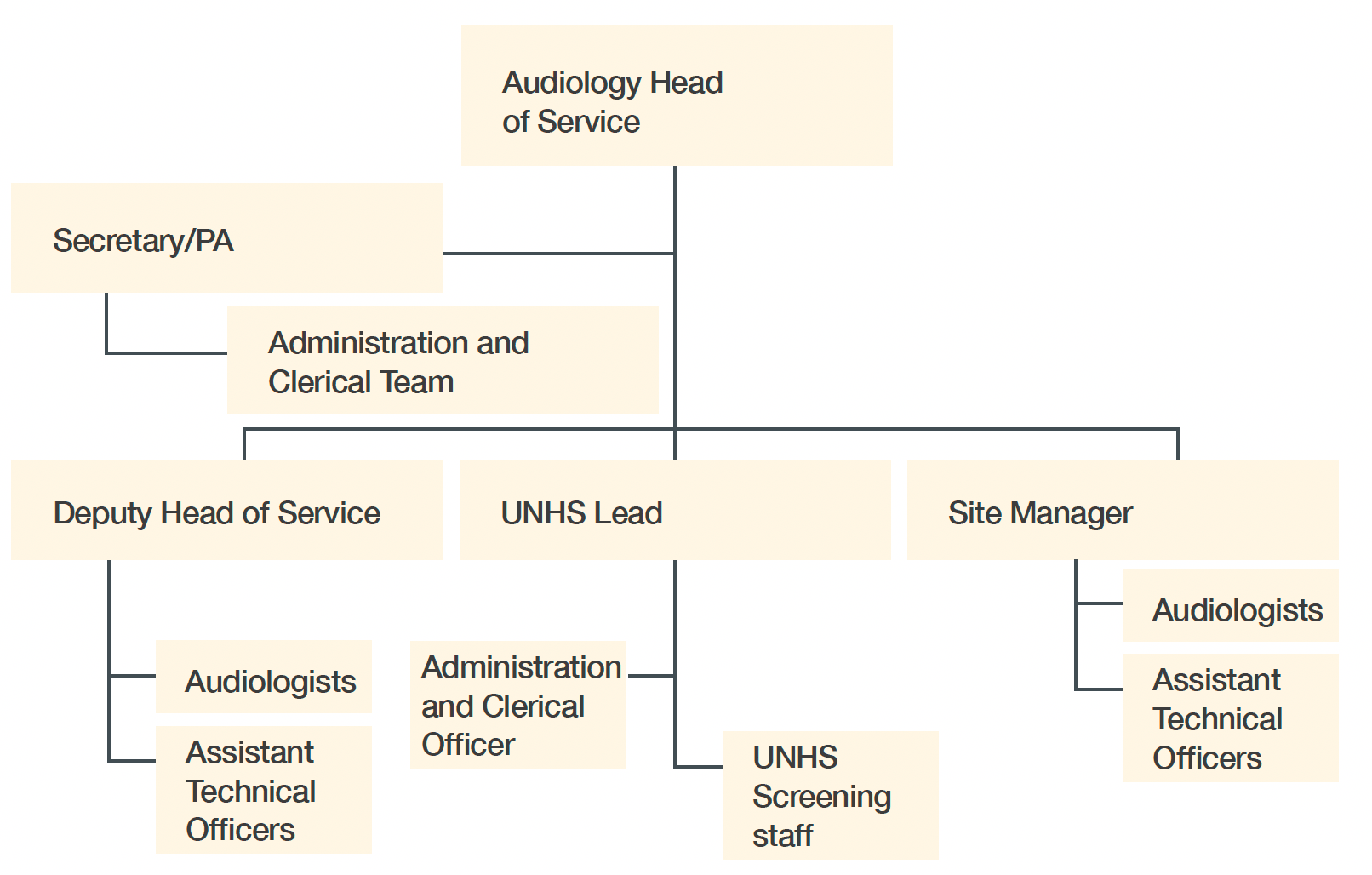
The structure of the service was, in the main, found to be fairly traditional and hierarchical. There was usually an identified head of service or, in some cases, a clinical lead as the most senior position, followed by deputy, departmental leads/chiefs and audiologists (practitioners), associate practitioners and assistant technical officers.
The use of the term “clinical lead” in some instances indicates that there is a lead clinician who also manages the service to an extent, with “head of service” reserved for a non-clinician/non-audiologist role occupying a senior management position. Heads of service are typically recognised as both lead clinician and operational manager of the service.
Figure 3 provides a typical example of the structure in a larger service. It is relevant to note that three of the services in Scotland are staffed by a single audiologist who is also the head of service and has few or no staff working with or for them.
Responses to the questionnaire also provided a summary of the current workforce, including vacancies – the national vacancy rate for the service runs at about 10%. Appendix B summarises the workforce across Scotland. The appendix also includes a high-level workforce plan based on work from 2002 by the professional body for audio-vestibular physicians and updated by heads of service to reflect both the current status of professionals working in audiology (an amalgamation of technicians, therapists and scientists) and the grading system for NHS terms and conditions (Agenda for Change). Based on this model, the plan suggests that the workforce is currently at about 65% of that required for a safe and effective service.
There is considerable variation in staffing levels between services when a simple ratio of staff to patients is applied, which is illustrated at Appendix C. Currently the national ratio for patients to clinical and technical staff is 20,500 patients per whole-time equivalent (WTE) member of staff. With improved staffing to the level predicted by the workforce tool, this reduces to 13,200 patients per WTE member of staff.
Generally, there is consistency in the range of services provided. A notable variation is in the grade of staff carrying out some of the listed activities. This is particularly true for hearing-aid repairs, which range from band 3 assistant technical officers to band 8 practitioner staff.
Local staffing issues are the main reason for this; however, based on findings from the questionnaire, there would appear to be situations where workforce issues mean that staff at higher grades carry out the tasks of a lower grade. This results in a “skills waste” and can affect staff morale. Ensuring that staff work to their grade will also help in establishing a more accurate picture of the workforce required in terms of skill mix. This skill mix would use assistants and associates, as well as practitioner-level audiologists, potentially in greater numbers, subject to availability/ supply.
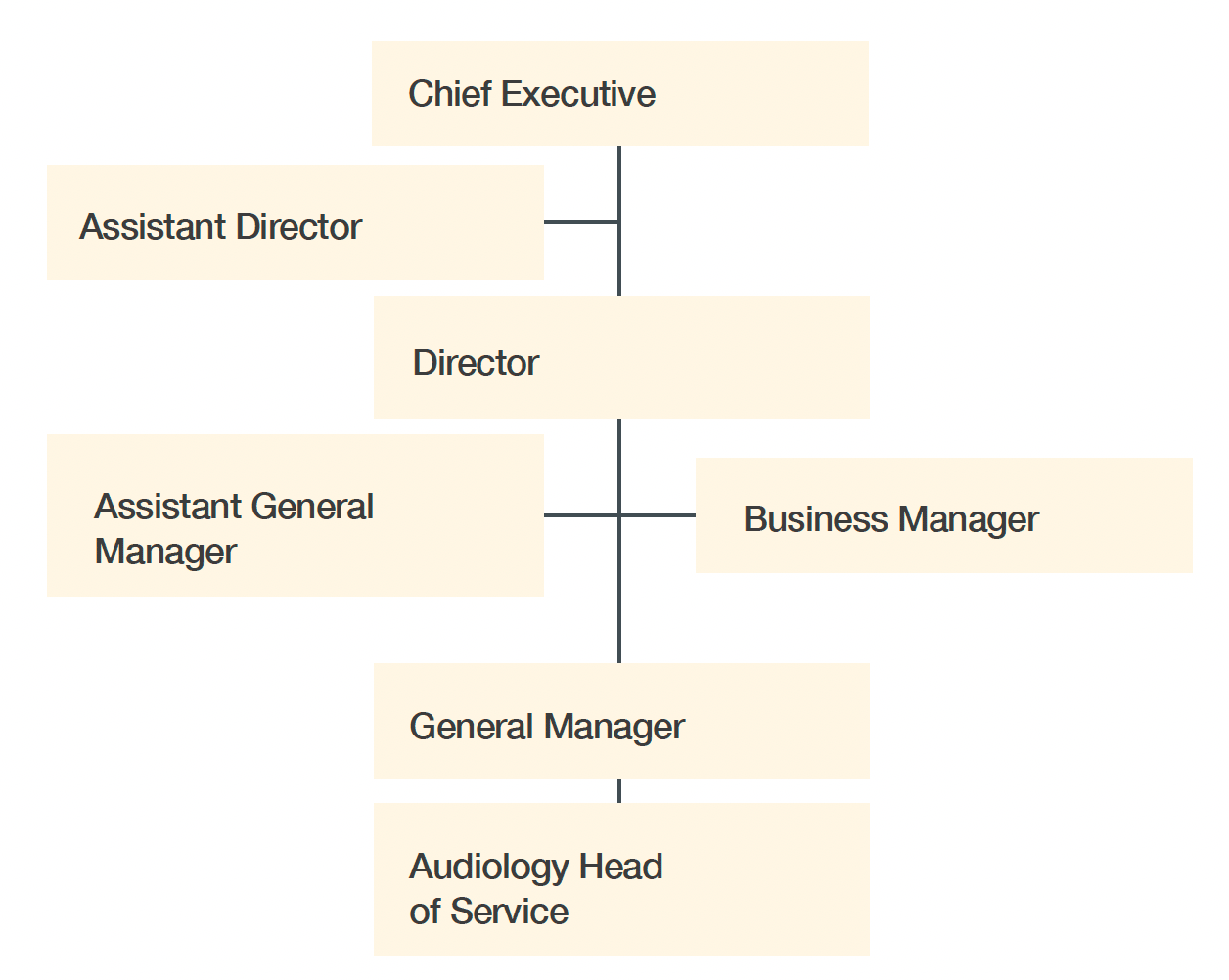
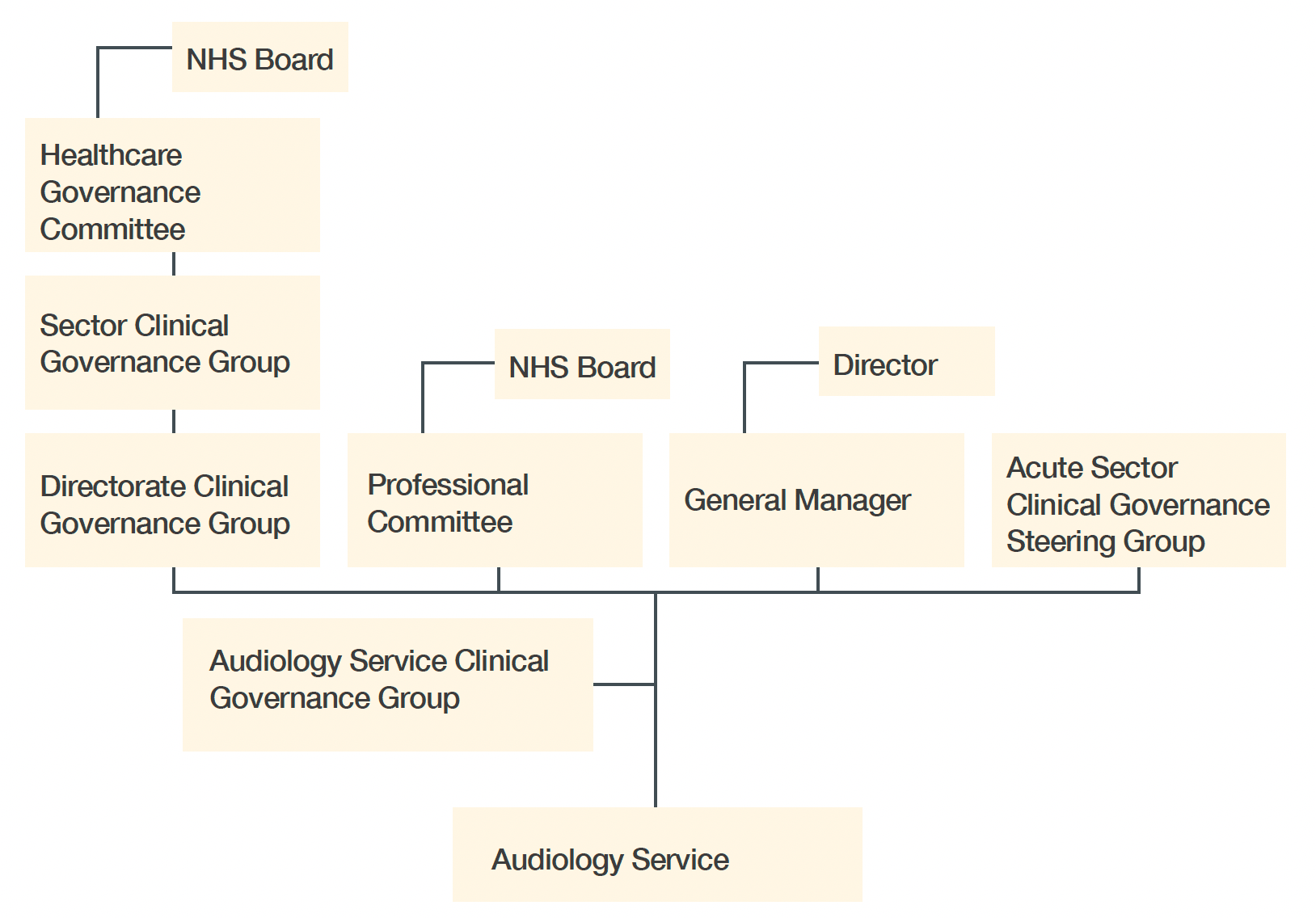
Responses to the questionnaire provided a picture of how services were organised at local level (Figure 4). The questionnaire asked for detail about where the service sits within the internal structure and, from a governance perspective, within the Health Board (Figure 5). At present, all services sit within the acute setting in each Health Board, although audiology can be found under a range of different directorates within acute services.
Several responses indicated that work was underway to look at the local structure and where audiology sat and that this was a direct response to the findings from the NHS Lothian BAA report on paediatric audiology. The review of structure was also directly linked to a concern that the clinical governance route for the service may not be clear and robust and that this should be properly established.
Findings – governance
This section looks at the key findings from the survey responses to the questions about governance.
Responses show that heads of service are consistent in their concern around service visibility and where audiology sits within the Health Board. This in turn leaves a degree of uncertainty regarding the governance position of the service and how it fits with the governance structure of the Board. There is a clear lack of understanding of what good governance is and means, and a strong feeling that audiology has, to a degree, operated within its own bubble. It has not truly been accountable in the sense that it has not been properly connected to the formal governance structures within each Board.
Governance structure: Responses showed that governance as a whole is not clearly understood within the service itself; and while the heads of service have some understanding of its concept, it does not appear that the service currently benefits from clear and established governance within its local organisation. As a result, it should be expected that the governance processes of the organisation may not be adhered to. This is not due to a deliberate lack of compliance or effort on the part of the service. Rather, it appears to be related to the service growing and developing in isolation and not being part of the governance system. Nor is it being held to account by any form of regular assurance reports or measures, except when things go wrong.
Audiology has not traditionally presented as a high-risk area. This may explain the general lack of understanding and focus, and the less-than-clear processes that some services describe with regard to where they fit locally.
The national structures and their governance must also be considered and these are described earlier in the report.
Although not part of the scope of the Review, the service itself has been engaged in conversation with policy colleagues in the Scottish Government regarding an earlier government commitment to move audiology from the acute sector to the primary care sector. This should be borne in mind when considering implementation of the Review recommendations.
Budgetary and human resources issues: In most cases, budgetary and human resource management sit with the head of service with support from human resources and finance teams, and senior management where appropriate and necessary.
The breadth of people-management roles is wide and in most cases includes performance and capability management of staff, recruitment and attendance management, as well as personal development planning and reviewing.
Heads of service will be guided by local policy, which is aligning increasingly with national policy, due to the implementation and ongoing development of “Once for Scotland” (14) human resource policies. Personal development of staff, their training requirements related to role and the needs of the service were noted to be “variable”. Possible reasons for this could be limited or an absence of training budgets, and lack of insight from the head of service regarding the need for specific training.
Waiting times reporting, service performance: Responses to the questionnaire indicated that the monitoring and reporting of waiting times and the performance in general of the service were variable. Some of this was linked to how information is or may be accessed and where the systems with this information are situated. In some cases, the head of service is responsible for developing and running reports and presenting data on waiting times, while elsewhere these tasks are carried out by other parties. Consistency in what and how data is recorded, as well as how it is reported, have been longstanding concerns within the profession. At times, this has made it very difficult to determine what services are doing and to compare them.
Governance links and responsibilities between service and government: These are not clear or well understood, and work to develop a clear pathway and understanding is required. The Welsh model for external governance arrangements for audiology services, along with the development of an Audiology Services Advisory Group in Wales, is described in Appendix D and should be considered as one option for clarifying links and responsibilities.
Multi-agency working arrangements: There were many examples of formal and informal working arrangements between services and other agencies. In many cases, these were undertaken on the basis that either the parties have been working in that manner for many years or that the arrangement is understood and governed by “common sense”. Equally, services reported that in some situations there are formal service-level agreements in place, particularly where some element of work has been commissioned and where there is an exchange of goods, services or payment for those goods or services. These service-level agreements appear to be a mix of local or more formal. Formal, documented arrangements seem to be in place to help mitigate risk. Where arrangements are informal, it is likely that in some instances there is the possibility of significant risk, depending on the nature of the agreement.
There is good evidence of staff within most services taking on positions and roles external to their organisation. These include teaching and training roles and chairing national groups.
Information governance and data management: The use of patient management systems in audiology has highlighted that within the next year all services in NHS Scotland will be using the same main audiology IT system. This offers the potential for standardisation of data definitions and of ways data is collected and used. There is concern, however, that standardisation could still be problematic given that not all services are currently on the same version of the system.
Accurate reporting will require that the same or very similar versions of the system are in use across Scotland. In addition to the main audiology system, there are currently two different systems in use for collecting data from newborn hearing screening, so similar issues and concerns are likely. It is also significant that while the main audiology IT system has the capability for running a standalone audiology service, integration with larger hospital systems is often required due to local working practices. In some instances, this has been done with reasonable success but at the other extreme there is no integration. At times this leads to double data entry, which can lead to errors and difficulties.
Record keeping: Formal documentation is another area where variation in processes and procedures has been identified. The service has experience of developing documentation to support the delivery of a quality assurance programme. In many cases, however, this requires updating and should be carried out as part of a general programme of work, to ensure that the service and its operation is suitably supported.
Findings – leadership
The survey asked about leadership, leadership development and formal qualifications in this area. Below is a summary of key findings relating to these areas.
Responses showed that the majority of heads of service can demonstrate external leadership training and development, with some holding a qualification. However, it is acknowledged that this is not a measure of the effectiveness of either the training or the individual. In Health Boards where services do not have a strategic lead and where the head of service role is focused on being a senior clinician, there is little or no development in this area, nor is there access to leadership training programmes. It is noted that most heads of service retain a significant clinical role (often 50% or more), which is likely to impact on the time they have available to lead and manage the service.
This also applies more generally to the lack of opportunities for staff at band 6 and band 7 levels to undertake formal leadership development. Few of the responses highlighted leadership training for those at band 6 and below. The implication of this is that leadership is not recognised as an important part of a professional’s development until they are in a senior role and that before they reach this level, they are not required to undertake activities that could be seen as requiring leadership skills.
Staff at band 6 level and sometimes lower often have responsibility for an area of clinical service, the review of junior staff, and the supervision and training of junior staff and students. Leadership is part of a suite of skills that individuals working in this capacity should be developing and they should have ongoing support and encouragement to do so.
Responses to the theme of opportunities and processes for staff and others to contribute ideas and suggestions, as well as raising concerns about the operation of the service, were varied. Use of staff meetings, one-to-one conversations (typically performance development reviews), “open door” approaches and even the potential to use the national whistleblowing policy were highlighted as methods of input and influence. Similar approaches were provided for raising ideas and concerns regarding clinical practice. Services where there was no strategic lead were more concerned with professional issues than operational issues.
There is evidence of networks and other resources being used to develop and improve services. For example, staff participate, or have participated in the past, in a national tinnitus group for NHS professionals, a balance group and a paediatric group – sub-groups of the Scottish Audiology Heads of Service Group, which set these up several years ago. Unfortunately, the groups were paused during the pandemic and, with the exception of the tinnitus group, are yet to restart. There has been an increase in the use of webinars and meetings, often industry or professional body-driven, that encourage discussion and sharing of ideas and practice across a wide area – often beyond the boundaries of NHS Scotland. Use of these approaches has, to a degree, become the norm, but it is difficult to gauge their impact in terms of the development and improvement of services.
Summary
Formally, there is a clear understanding of the structure of the service, reporting lines and responsibilities, as highlighted within the findings from the “structure” section of the questionnaire. But there is serious concern that this misses the point that governance, and ultimately accountability, is less well understood; more worryingly, that systems are not in place to ensure and assure the service, Board and beyond, that there is ongoing review and audit of practice and care to provide a solid and robust picture of how well the service is running.
After the events in NHS Lothian, awareness of the need for oversight has increased and this is now better understood within the service. However, there is also a lack of clarity regarding external oversight and where responsibility for it lies.
Use of standardised approaches such as quality standards, adherence to national/professional standards for practice and other referenceable methods of working are not in place within NHS Scotland’s audiology service – and they need to be. There is a very strong message from the service itself that better national oversight and measurement, and in particular service quality, are required. These must be led from the front and not left to chance. Such leadership would be welcome at Board level, where responses to the questionnaire show that in some cases Boards have little knowledge of what their audiology service does.
Recommendations 5 to 18 are especially relevant to the work of this Sub-Group.