The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment Regulations 2022 and The Health Protection (Coronavirus) (Requirements) (Scotland) Amendment (No. 2) Regulations 2022: equality impact assessment
This equality impact assessment (EQIA) is to analyse the potential impacts for each protected characteristic under the Equality Act 2010 of amending the definition of fully vaccinated to include the requirement for a booster if a primary course of MHRA vaccine was over 120 days ago and amend the definition of late night venue.
Race
Background
Minority ethnic (ME) people in Scotland experience significant health inequalities. Prevalence of some health conditions are higher for some ethnic groups, such as Type 2 diabetes and coronary heart/cardiovascular disease among people of South Asian and African descent. In 2011, despite having a much younger age profile, 37% of Gypsy/Travellers reported having long-term health conditions compared to 30% of the population as a whole.[165]
Gypsy/Travellers in Scotland, compared to the population as a whole, are more likely to report a long-term health problem or disability and were more likely to report bad or very bad general health.[166] Reducing the spread of coronavirus should therefore have a positive impact on protecting these communities from health harms.
Inequalities are also socioeconomic. Relative poverty, which affected 23% of households in Scotland in 2019, rose to 38% and 39% in Black and Asian households respectively.[167] The gap in employment rates for working age minority ethnic people, relative to the white population, was 22% for women and 9.5% in men, and Pakistani and Bangladeshi workers had the lowest median hourly pay and were also the least likely to work from home in the UK.[168]
Estimates show that low earners were 7 times more likely than high earners to have worked in a sector that has shut down as a result of the lockdown, and those with customer facing roles are likely to have seen reductions in earnings or face job losses as they are less able to work from home.[169]
The pandemic has exacerbated existing health and wider inequalities. Analysis of hospitalisations and more severe outcomes due to COVID-19 up to 30 September 2021 point to continued evidence of increased risks in most ethnic minority groups relative to the White group. Rates of hospitalisation or death were estimated to be around 4-fold higher in Pakistani and Mixed groups, and around 2-fold higher in Indian, Other Asian, Caribbean or Black, and African groups. Deaths amongst people in the South Asian ethnic group during wave 1 were almost twice as likely to involve COVID-19 as deaths in the White ethnic group, after accounting for age group, sex, area-level deprivation and urban rural classifications. This increased to 3.78 times and 3.55 times more likely for wave 2 and wave 3 respectively. A similar pattern was seen for the Black/Caribbean/African group compared to the white group with an increased risk of 1.47 times, 2.03 times and 3.33 times more likely to die of COVID-19 for wave 1, 2 and 3 respectively.[170]
Differential impacts
Positive impacts
If the policy objective to reduce the risk of transmission is achieved, Covid Status Certification could benefit minority ethnic communities, as they are at a higher risk of poorer health outcomes if they contract the virus.
A panel study with more than 70,000 participants across the UK undertaken by University College London suggests that minority ethnic people describe higher levels of loneliness than their White counterparts.[171] Therefore, if the policy objective to allow higher risk settings to continue to operate as an alternative to closure or more restrictive measures is achieved, Covid Status Certification could benefit minority ethnic groups by facilitating socialisation.
People from certain ethnicities, for many different complex and nuanced reasons, are less likely to take up the vaccine. Testing will act as a mitigation and will allow those who have not been fully vaccinated to access the regulated settings.
Negative impacts
Lower vaccine uptake among ME communities is a result of a combination of factors including misinformation, mistrust, socioeconomic barriers, and delivery that does not meet accessibility needs. For example, some Gypsy/Travellers are often not in an area long enough to engage with health services to be fully vaccinated. In this circumstance testing could act as a mitigation for Gypsy/Travellers, who are more likely to have an address on their GP records (where paper vaccine Certification is sent to) different to the one where they currently reside. A test result could be registered on the GOV.UK website and the SMS or email used to access a regulated setting.
Looking at ethnicity, the uptake of the first dose by most ethnic groups is lower than the White group for all age cohorts.
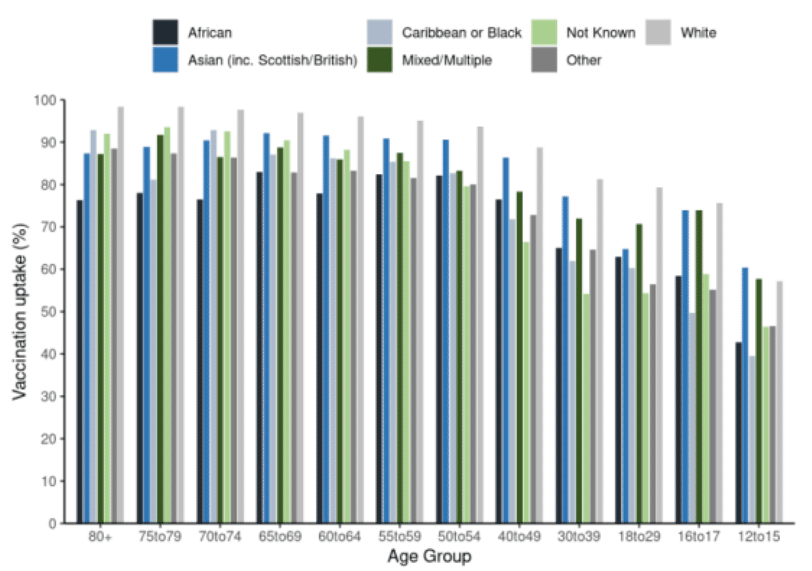
% uptake of first dose of Covid-19 vaccination as at 23 November 2021, by age group and ethnic group. (Source: Public Health Scotland).
Survey data from UK-wide research suggests that, in comparison to White British and White Irish participants, Black African and Mixed Black African health and social care workers were less likely to have been offered a vaccine, and much more likely to have declined vaccination if offered. Reasons for doing so among Black African participants included distrust in Covid-19 vaccinations, healthcare providers and policymakers.[172] Uptake by the White Polish community is also comparatively much lower.[173] Therefore Covid Status Certification could negatively impact ME communities if they are denied access to the regulated settings due as they have not been vaccinated.
As at 28 September 2021, in those aged 18 and over, dose 1 vaccine uptake is highest in White ethnic groups (89%) and lowest in the Caribbean or Black ethnic groups (68%). For dose 2 this is 84% and 60% respectively. For dose 2 the lowest uptake is in African ethnic groups (59%).[174]
SAGE have reported, with high confidence, that Black African and Black Caribbean groups are less likely to be vaccinated (50%) compared to White groups (70%). Survey data from the UK Household Longitudinal study shows overall high levels of willingness (82%) to take up the COVID-19 vaccine. However, marked differences existed by ethnicity, with Black ethnic groups the most likely to be COVID-19 vaccine hesitant followed by the Pakistani/Bangladeshi group. Other White ethnic groups (which includes Eastern European communities) also had higher levels of COVID-19 vaccine hesitancy than White UK/White Irish ethnicity.[175]
Stakeholders raised concerns that the introduction of Covid Status Certification could exacerbate vaccine hesitancy and thus undermine one of our initial policy objectives. They felt that Covid Status Certification is unlikely to incentivise asylum seekers, refugees or migrants to take up the vaccine as they do not often frequent the settings in scope. Stakeholders also felt that as parents and guardians are influential figures in children's lives, children may hold the same sentiments as their parents, and may also become less likely to take up the vaccine.
Engagement with external stakeholders suggests that there is potentially perceived stigma attached to being tested depending on a person's cultural background. Early feedback suggested that with the online booking system being the primary route to testing, it was felt that this excludes people who do not fully understand written English and/or who do not have internet access. Feedback also suggests that the information provided as part of this portal is complex and people have to read through a lot of guidance and click through a number of links before they can book a test. This could create a barrier to those with lower literacy levels.
However, research shows that those from Gypsy / Traveller communities may have lower levels of literacy which could create a barrier to understanding advice and information on access to testing.[176]
Covid Status Certification could also impact migrants. Research suggests that the majority of documented migrants that are recent entrants to the UK do not register with a GP, despite relatively easy access to primary healthcare.[177] Undocumented migrants, refugees and asylum seekers are even less likely to register in primary care services.[178] Stakeholders identified that a reason for this is fear that their data will be shared with the Home Office, which could impact on their migration status. This is based on prior experience of health data being shared by the NHS with the Home Office.[179] [180]
We know people from lower socio-economic backgrounds are more likely to be digitally excluded. For example, 82% of households in the 20% most deprived areas in Scotland had internet access at home compared with 96% of households in the 20% least deprived areas.[181] We also know that relative poverty impacts ME people far more than White people and so minority ethnic communities are more likely to be digitally excluded. Paper certificates are available as an alternative, together with support and guidance. Whilst this is a sound option, it may still present some challenges. For example, as a security measure, the paper Certificate is posted to the address held by the GP. This could impact some groups, such as some Gypsy/Travellers, who may not have a fixed address.
Those in Scotland who have been vaccinated abroad with a vaccine that has not been approved by the MHRA may be negatively impacted by the scheme if they are unable to access spaces were Covid Status Certification is required. This may include those visiting Scotland, or residents, such as international students. Stakeholders have informed us that an estimated 23,000 international students, including 13,000 Chinese students, could have had a non-MHRA vaccine. This could impact on people's ability to participate in society. For those whose vaccine is not recognised by the MHRA, testing would be an alternative option which would allow them to access the regulated settings.
In terms of the App, as previously explained under the Gender Reassignment section, facial recognition software has been found to contain racial and gender biases. This may mean that a higher number of minority ethnic people, especially women, registering for the App could encounter more difficulties verifying their identity than white people.[182] Stakeholders also highlighted that migrants, asylum seekers and refugees, are less likely to have ID, and as such may be unable to use the App. ID is not needed to register a test result and so an SMS or email confirmation could be used to access the regulated setting.
There is also the possibility that Covid Status Certification could be used beyond the intended purposes and employers could require proof of vaccination as a condition of employment. People from ethnic minorities are disproportionately represented in industries where working from home is not feasible, and may therefore be more impacted if employers enforce this requirement.[183] The businesses not covered by Covid Status Certification and operating certification voluntarily should consider asking for a record of a negative test as an alternative to a record of vaccination. However as a LFD test result is only valid for 24 hours, testing every day could be burdensome. Businesses which are not covered by the Government's scheme are required to meet their obligations under all relevant law including data protection, the Equality Act and Human rights. For more information see the Equality and Human Rights Commission Guidance for Employers.
As with anything where documentation affords access to certain spaces, services or products, there is the potential that unconscious bias could cause enforcement of Covid Status Certificate to be administered in a discriminatory manner. There are more subtle ways that unconscious bias could be enacted, as for example while taking all reasonable measures to enforce Certification, employees may spot check people from minority ethnic groups far more than white people. While people may still ultimately gain access to the setting if they have Certification, the experience of feeling singled out could still cause distress, a loss of time, distrust in the scheme, and anxiety about future use.
Concerns regarding discrimination are apparent in public polling: minority ethnic people report 18% more concern than White respondents that they would be discriminated against through vaccine passports, and 54% of all surveyed people think it is likely that vaccine passports would lead to discrimination against marginalised groups.[184] There is also anecdotal evidence that this has occurred and that ME attendees have been asked for Covid Status Certification more frequently than White attendees.