We use cookies to collect anonymous data to help us improve your site browsing
experience.
Click 'Accept all cookies' to agree to all cookies that collect anonymous data.
To only allow the cookies that make the site work, click 'Use essential cookies only.' Visit 'Set cookie preferences' to control specific cookies.
Accessing appropriate urgent and emergency care in a safe and timely way is extremely important. This is particularly so at weekends and during the out of hours period.
Equity of access to urgent care services
People living in care homes can become unexpectedly unwell, requiring urgent care and attention. However, it is more difficult for people living in care homes to access some services that have been set up for urgent care (e.g. an urgent optometry or dental appointment, a community pharmacy or a hospital minor injuries unit). Many of the urgent care services developed as part of the GP contract, such as advanced practitioners, will only see people who are able to attend the GP surgery.
During our programme of engagement, we learned that when urgent and emergency care can be accessed in a responsive way, with consideration of ACPs and using a 'Realistic Medicine' approach, experiences were good. However, inappropriate admissions to hospital were more likely to happen where that preventative planning was not in place or professionals did not have the relevant access to an ACP.
Urgent and emergency care services perform a critical role in keeping the population healthy. People living in care homes should receive the right care, in the right place, at the right time. Care home staff are pivotal in providing this on a day-to-day basis, but there are circumstances when they may need more support to empower them to have confidence in their decisions, and there may be situations where additional services are required to meet the needs of the person.
"Urgent/emergency care can be very sporadic as residents are deemed to be in a place of safety therefore not a priority for out of hours services."
People living in care homes should have timely and equitable access to a member of the primary care multi-disciplinary team when this is required. Several HSCPs have already set up dedicated care home teams comprising of Advanced Practitioners (nurses, paramedics and physiotherapists) who can respond quickly and visit people requiring urgent unscheduled assessments, with support and advice being available from the GP by phone. The development of these local care home teams has many potential benefits and should be considered within every HSCP covering weekdays and weekends.
Supporting good communication between professional staff
Social care staff and health care staff must be able to communicate the needs of an individual in a way that is clear and concise. By implementing an SBAR (Situation, Background, Assessment, Recommendation) tool care home staff have described increased confidence in being able to focus on their observations, reflect on the person experiencing care and their care needs. Healthcare staff also found that the use of SBAR aided communication, as it provided them with the appropriate information in a concise way. It is therefore recommended that both care home staff and healthcare staff are familiar with the SBAR format when discussing urgent or emergency care and consider using a structured proforma for these conversations.
RESTORE2 is a physical deterioration and escalation tool for care homes. It is designed to support homes and health professionals to:
recognise when someone may be deteriorating or at risk of physical deterioration
act appropriately according to the person's care plan
obtain a set of physical observations to inform escalation and conversations with health professionals
speak with the most appropriate health professional in a timely way to get the right support
provide a concise escalation history to health professionals to support their professional decision making
During the COVID-19 pandemic, the development of a Care Home Assessment Tool (CHAT) was led by Technology Enabled Care, working with care homes and GP practices in Glasgow and Lanarkshire. This digital tool used the components of RESTORE 2 to enable care homes to share assessments of people who had symptoms of COVID-19 or other serious infection quickly with their GP practice.
Access to services out of hours can be challenging for care home staff and response times may be lengthy. This was echoed in the responses to our survey of care homes. There are many different ways to obtain urgent and emergency care across Scotland outwith normal working hours (out of hours services, professional lines, NHS 24 / 111, or 999), many of which do not provide an immediate service for vulnerable people living in care homes. A consistent approach is needed.
"Staff can be on the phone an hour before getting connected."
A multi-disciplinary approach of professionals working together is required. The sector has made clear their desire for direct professional to professional communication channels, such as dedicated phone lines, to ensure staff in care homes have 24/7 support in making decisions for a person who has become unwell. Having direct access to help during the out of hours period will aid seamless and timely access to health and care support and response 24/7. This is particularly important in managing symptom control for people approaching the end of life.
Providing urgent and emergency care within the care home
There are advances in near patient and point of care testing that allow medical tests and investigations to be undertaken outwith hospitals or other healthcare facilities. It is important to explore how these could be used to benefit the care of people in care homes and aid decision making regarding treatment. It is felt that simple tests such as the ability to measure oxygen saturations would be useful in the decision relating to need for hospital admission. However, this needs to be balanced with the concern of inappropriate investigations and remembering that care homes should not become clinical settings. Just because it is possible to do an investigation or test remotely, does not mean that the test should be done. Realistic Medicine principles should be considered when determining the best course of action for an individual. As part of the implementation process further exploratory work should be done to investigate this field and also how near patient and point of care testing could link in with Hospital at Home services.
Alternatives to hospital admission including community facing specialty teams (e.g. hospital@home) should be considered to allow individuals to receive hospital level care within the care home when appropriate. All health boards should develop Hospital@Home type services that enable people living in care homes to receive hospital-level care within the care home.
Hospital at Home (H@H)
H@H is a short-term, targeted intervention that provides a level of acute hospital care in an individual's own home which is equivalent to that provided within a hospital. A hospital specialist acts as senior decision maker and responsible medical officer, sometimes with the help of other grades of medical staff. Care is delivered by multi-disciplinary teams of healthcare professionals complying with current acute standards of care. It complements other community-based health and care initiatives which support patients to remain in their own homes. It provides a different level of interventions, such as access to intravenous fluids and oxygen. It has been in existence in a number of countries across the world for 25 years. The first hospital at home service was introduced in Scotland in 2011.
HIS have established a programme to support the implementation of H@H, including work with a mixture of NHS boards and Health and Social Care Partnerships. A total of 20 HSCP areas across the country are supported.
The programme includes a system to share learning and good practice, building on the experience of the established services in NHS Lanarkshire, NHS Fife and NHS Lothian. It tends to work best when it is part of an integrated acute and community-based service model to meet local population need.
The Urgent and Unscheduled Care Team are leading on the development of virtual capacity pathways with a number of stakeholders. Outpatient Parenteral Antimicrobial Therapy (OPAT) and Respiratory pathways are currently in place with others in the development phase.
Treating urgent medical conditions within the care home will often require prompt access to appropriate medication. The relationship between care homes and pharmacy services is varied across the country. One of the main challenges the sector faces is how medicines can be obtained out of hours. Visiting out of hours GPs only carry a limited supply of medicines, and care homes are not permitted to hold stocks of prescription-only drugs unless they are for a specific named individual. It is a constant challenge for staff to access medicine when their local pharmacy is closed. This can sometimes lead to attendances / admission to hospital if medication is not available. During the pandemic, temporary changes in legislation were allowed for care homes to repurpose medicines for another person if they had stocks in the care home. Further work is required within this area.
Hospital transfers and admissions
People living in care homes are at risk of developing delirium and deconditioning from an admission to hospital. A shared decision should be made about whether transfer to hospital is appropriate, taking into account the individual's care plan, carer and relatives' wishes and clinical assessment. However, people should never be denied admission to hospital solely on account of living in a care home.
There are often delays in transferring people living in care homes to and from hospitals, often as a result of wider system pressures. It is important that ambulance staff and other stakeholders work closely together, optimise safe travel routes and utilise all options of transport available.
Upon arrival at hospital it is vital that people living in care homes have equitable access to specialist care and they should, wherever possible, be assessed by a senior clinical decision maker. We know that older people living in care homes are often frail, and unless clinically inappropriate (e.g. if they have an acute stroke), their care should be in a specialist area for frail, older adults. They should have early access to comprehensive geriatric assessment, with nurses and AHPs trained and experienced in caring for this vulnerable group. This can enable faster recovery and earlier discharge back to the care home.
Acute and Emergency Care
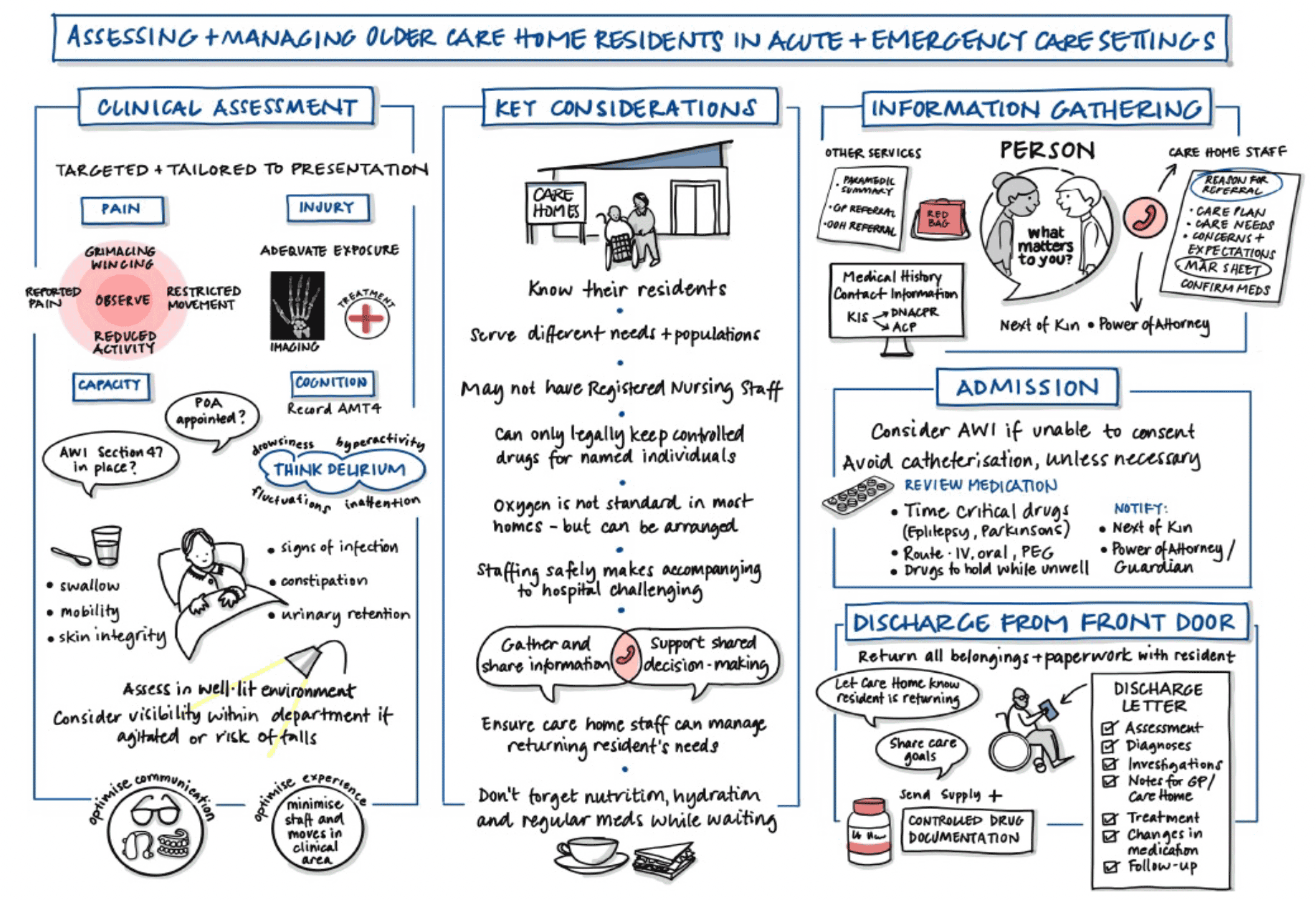
It is recognised that when care home patients are admitted to hospital they are at risk of adverse events. It is important that the hospital team are aware of the wealth of information that would be available from the carers usually looking after them and that there are ways to mitigate the risk of adverse events. The following infographic is available to download from the Scottish Government website, and was developed to assist in assessing and managing older adults being admitted from their care home.
Figure 6: Looking after people from a care home infographic
Timely access to someone's health records is also vital. The Key Information Summary (KIS) and ACP information should be readily available to all parts of the system. On transfer back to the care home, clinical information and outcomes should be shared with the care home to allow the care home records to be updated. Sharing details of any previous discussions and decisions regarding capacity and DNACPR (Do Not Attempt Cardio Pulmonary Resuscitation) can be helpful both for people being admitted but also on discharge back to the care home.
There is currently no national data on the frequency by which people living in care homes use urgent and emergency care. NHS 24 have put measures in place to fulfil the desire for this metric by asking callers if they are calling from a care home.
Recommendations
5.1 Support and empower care home staff by providing and encouraging participation in training opportunities and enabling all staff to have the tools to assess and communicate in acute and emergency situations using the SBAR format.
5.2 People living in care homes should have timely access to members of their MDT, 24/7 when urgent or unscheduled care is required.
5.3 HSCPs should consider developing dedicated community healthcare teams comprising advanced practitioners who can respond quickly and visit people in care homes requiring urgent unscheduled assessments, with support and advice being easily available from the GP by phone. These services should cover both weekdays and weekends.
5.4 Both care home staff and healthcare staff should be familiar with the SBAR format when discussing urgent or emergency care, and consider using a structured proforma for these conversations.
5.5 Care home staff should be able to contact healthcare professionals during an urgent or emergency situation in a consistent and timely manner – this includes exploring possibilities for dedicated professional to professional communication channels.
5.6 Scoping work should take place to explore the use of near patient and point of care testing within care homes, taking into account Realistic Medicine principles.
5.7 Health boards should develop Hospital@Home services that support people living in care homes to receive hospital-level care within the care home.
5.8 Further work is required across Scotland to improve the accessibility and provision of medicines during an urgent situation. This includes exploring mechanisms to enable care homes to hold a stock of certain drugs within the home.
5.9 People living in care homes should never be denied admission to hospital solely on the basis of living in a care home, and at point of admission older people should be assessed by a senior clinical decision maker with experience in caring for frail older adults.
5.10 Timely and safe transfers to and from hospital for older people in care homes should be optimised.
5.11 Digital access to an individual's health records, and clinical outcomes should be timely and accessible to all parts of the system.