My Health, My Care, My Home - healthcare framework for adults living in care homes
Framework providing a series of recommendations that aims to transform the healthcare for people living in care homes.
2. The Multi-Disciplinary Team
A multi-disciplinary approach allows people to benefit from the combined skills and expertise of health and social care professionals who are working together to optimise health and care outcomes.
A constant desire emanating from our programme of engagement is the need to adopt a multi-disciplinary team (MDT) approach to healthcare.
This is where a group of healthcare and social care professionals, who are members of different disciplines, with different skills and expertise (e.g. care workers, social workers, podiatrists, dentists, nurses and doctors), work together to enable the best outcome for the person living in the care home.
The MDT
There are many different individuals and professionals who support the health and wellbeing of an individual living in a care home, and these can be represented by concentric wheels around the person (figure 3).
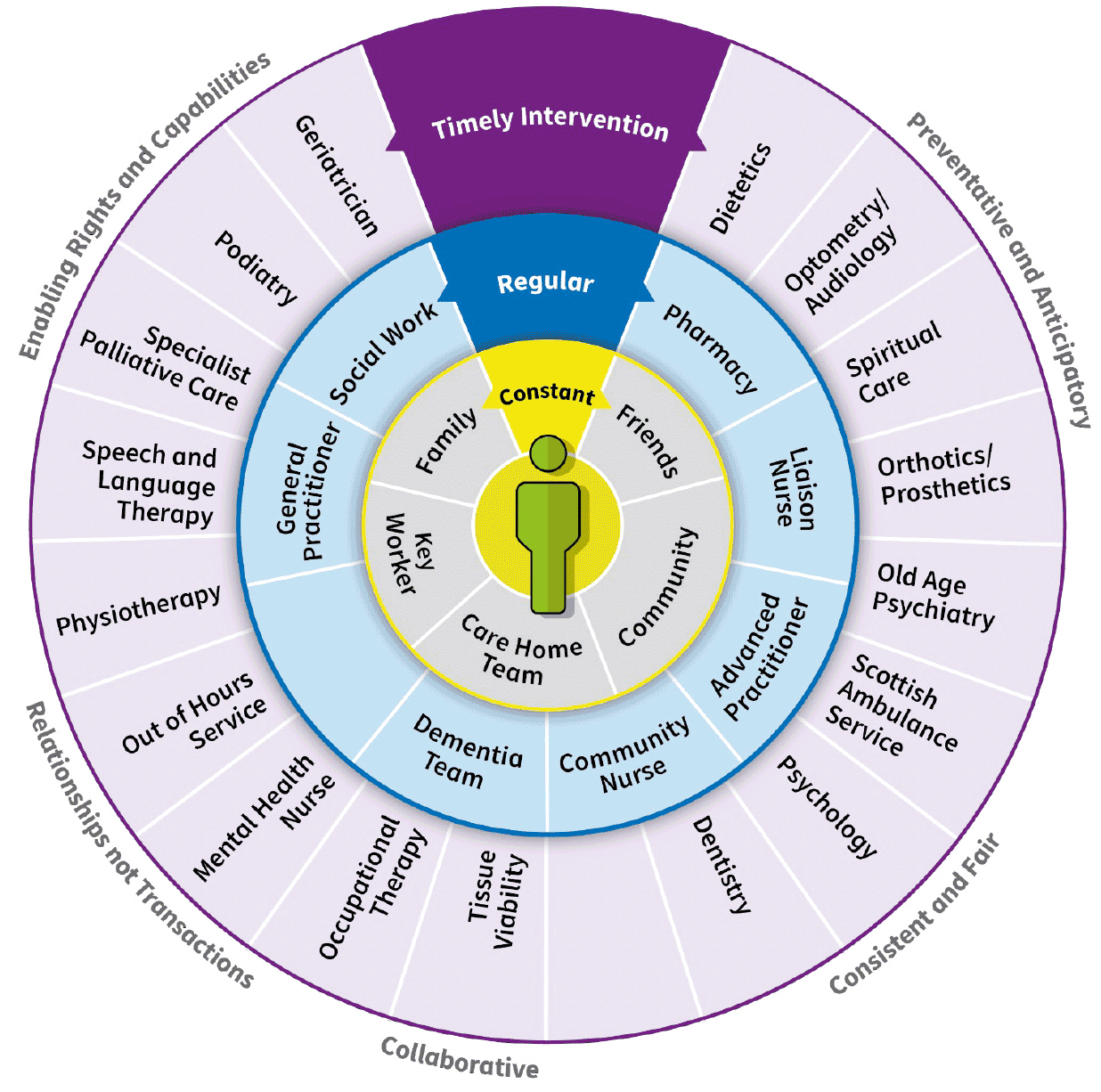
The people that will normally have the largest impact on health and wellbeing, and who are likely to be a constant presence in the life of the individual in a care home, are listed in the inner wheel. These include friends and family, the community and the care home team. All members of the care home team have an important role in promoting a person's health and wellbeing; for example, catering staff supporting nutritional care, domestic staff engaging in day-to-day conversation and promoting mental wellbeing, and gardening staff who can promote outdoor physical activity by creating a safe and stimulating outdoor environment. There is a particularly important role for the registered nurse within this team. They possess an in-depth knowledge of long term health conditions associated with ageing and skills in the management of complex multiple morbidities and frailty.
Nurses working in care homes require leadership skills and will often have management responsibilities for others within the care team. They are also a key link with the professionals working within the middle and outer wheels.
The people listed in the middle wheel may not be involved on a daily basis, but will often be providing regular healthcare advice and reviews over many weeks, months and sometimes years. They will work closely with those in the inner wheel. Those in this wheel may change depending on the needs of the individual. For example, someone recovering from an illness or injury may require a proactive rehabilitative or enablement approach led by a physiotherapist or an occupational therapist. The role of advanced practitioners within the middle wheel, providing regular professional input is increasing. These advanced practitioners may be specialist nurses or Allied Health Professionals. Social workers hold legal duties under the Social Work (Scotland) Act 1968 to assess needs and make arrangements for care and support. They have an important role in 'protection and monitoring', and also provide assessment of needs and finance when making arrangements for people to go into care homes. Approaches based on human-rights enabling and person-centred strengths should drive the support delivered, but also challenge it where it is not. Social workers have a statutory duty to ensure this happens.
The outer wheel represents a range of other health and care professionals who will provide proactive timely interventions to support the individual. This may be through offering advice and guidance to those in the inner or middle wheel.
It is likely that the individual will not require input from everyone within these concentric wheels, and for some people there will be more focused involvement than for others.
The blank boxes within the diagram signify that other professionals who are not listed, may become part of the MDT for an individual, and that professionals may move between the outer and inner wheels.
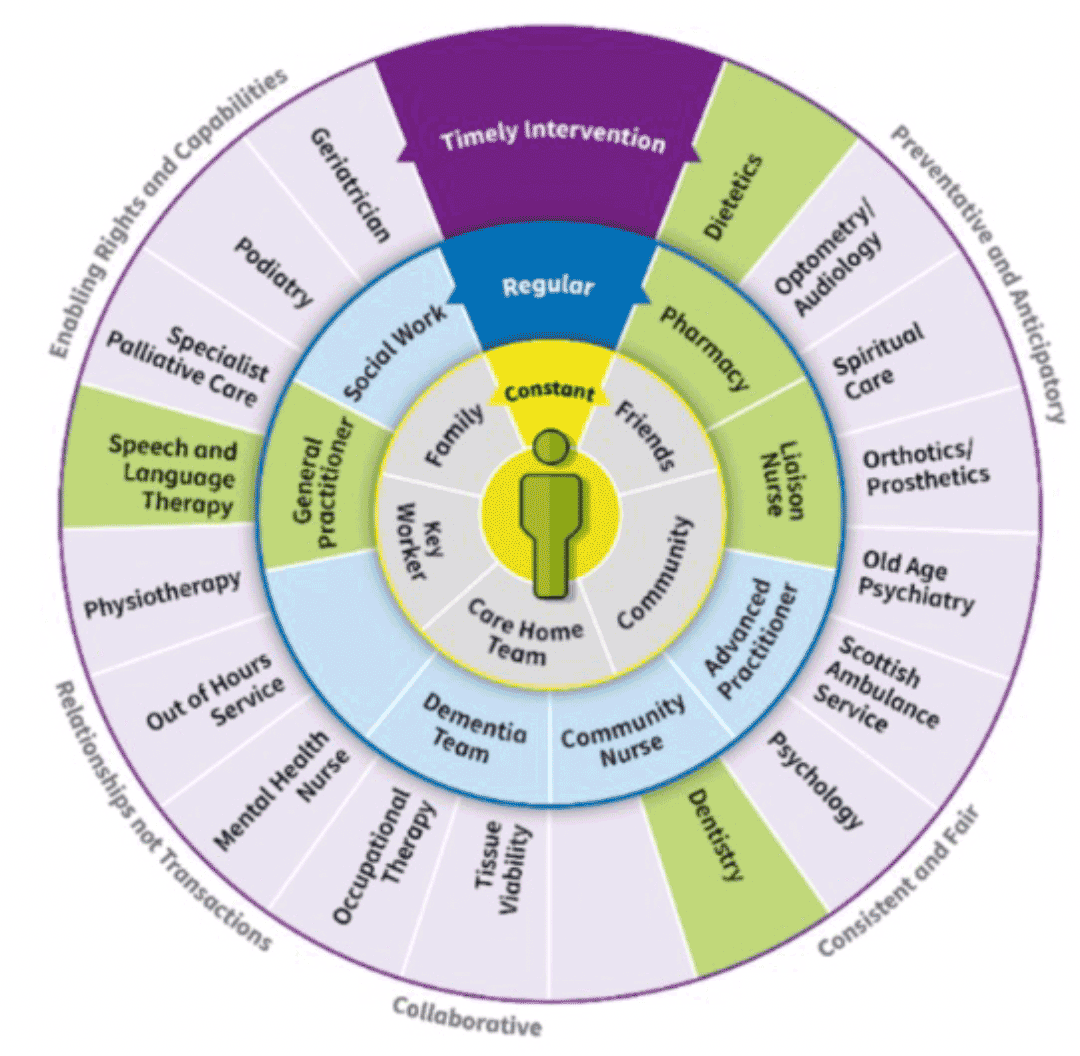
Someone living in a care home may need the time-limited and focused support from specific members of the MDT. For example, someone with swallowing problems may require increased input from those professionals highlighted in green within figure 4.
It should be clear to the key worker and care home team how to access all members of the MDT, with a clear understanding of how and when to obtain help. Professional to professional support should be available without having to go through the GP, whenever it is clinically appropriate to do so.
MDT meetings
The MDT must take a proactive and anticipatory approach to the care of those living within the care home. To enable this to happen there should be regular meetings and good communication between those professionals providing constant and regular input (the inner two wheels in figures 3 and 4) and the person living in the care home. Other professionals highlighted as part of a person's care team (for example those in green in figure 4) should be invited to contribute to MDT meetings as and when required. This could be in person, or by providing a report or update ahead of the MDT meeting. Allied Health Professionals can make a significant contribution to discussions by shifting the focus onto prevention, rehabilitation and reablement. These MDT meetings will allow professionals to share information, discuss and plan care for the individual. All members of the team (including families and the person) will have the opportunity to highlight people that should be discussed at the MDT meeting.
For practical reasons meetings may take place virtually using video technology, and should happen as frequently as is necessary. However, this is likely to be dependent on the person and/or the care home. Smaller care homes may wish meetings to take place monthly whereas larger care homes may need to meet more frequently. The 2018 General Medical Services (GMS) contract describes how GPs should provide senior clinical leadership to the MDT, and so with the implementation of Primary Care Improvement Plans, it is a strong recommendation that there is GP representation at these meetings.
MDT meetings will require some administrative support to ensure that they take place and that the appropriate people are invited. This role should be co-ordinated between the HSCP and the care home. Discussions during these meetings should be led by the most appropriate members of the MDT. During any subsequent planned review, people living in care homes should have the opportunity to involve a family member or any legally appointed welfare guardian or attorney. If required, Chief Social Work Officers can act as legal welfare guardians, making decisions (Adults with Incapacity (Scotland) Act 2000) if there are no other suitable people in a person's life to undertake this role.
As MDTs form and develop, opportunities for shared learning should be explored to develop the knowledge, skills and experience required to provide the best possible care.
Some health boards are already looking at this multi-disciplinary way of working. NHS Tayside have developed a set of principles for developing the MDT and for how General Practice should work with care homes.
Communication between different agencies needs to be improved for a co-ordinated and enhanced MDT approach to work. There must be better access to relevant care and clinical information, with sharing of relevant assessments, care plans and treatment decisions. This theme is explored more in the Data, Digital and Technology section.
Alignment of GP practices with care homes
Some care homes look after people who are registered across multiple GP practices, and similarly some GP practices look after people residing in multiple different care homes. This can be challenging for all involved.
Care home staff and community MDTs report difficulties when dealing with several GP practices who each have different ways for requesting advice, visits and prescriptions. It is also inefficient for staff in the same GP practice to visit multiple care homes on the same day. There is evidence of better outcomes (better satisfaction amongst all professionals, fewer medication-related problems, reduced inappropriate admissions to hospital, agreement over the optimal healthcare management plan) when care homes are either aligned or work more closely with specific GP practices. Optimal NHS service delivery to care homes
It is a strong recommendation that each care home should be linked with a named GP practice that will play a lead role with that home. This will allow closer and stronger working relationships to develop between the GP practice team and the care home. It will also provide clarity over which GP practice should be supporting the MDT.
"We are lucky as our district nursing teams and GP practice work excellently alongside us to benefit the resident."
HSCPs should work within localities to have, wherever possible, a single lead GP practice, working in close partnership within an extended MDT for each care home. Very large care homes may require input from more than one GP practice. Where there are exceptional circumstances making linkage of care home and GP practice impossible, HSCPs should work with the local care homes and GP practices to establish safe and reliable alternative arrangements that enable effective MDT working.
There may be someone living in the care home who chooses to remain registered with a GP practice which is not the lead practice for that home, but is still within the practice boundary. This request should be accommodated whenever possible, but the individual should be aware of the advantages of being registered with the lead GP practice for their care home and that they are able to make a decision that best suits their needs.
Most health boards in Scotland offer GP practices 'local enhanced services' (LES) in relation to care homes. These provide additional funding to supplement services already offered within the core GP contract. GP practices can decide whether or not to participate in a LES. Many of the LES relating to care homes have not been revised since the introduction of the GP contract in 2018. Health Boards should review their existing LES that relate to care homes and revise them in line with the aspirations of the 2018 GP contract and the ambitions of this framework.
Specialist provision for those with the most complex care needs
Care home staff have a wealth of experience and expertise in caring for frail older people, people living with dementia and within palliative and end of life care. However, there should still be clear pathways to access and obtain support from specialist services. There should be a proactive system in place for reviewing people living with the most complex of healthcare needs.
Some care homes have established dedicated facilities for people living with very specific and complex health conditions (e.g. homes for people with advanced Huntington's disease or severe brain injury). The healthcare needs of these people go beyond the scope of General Practice, and so HSCPs have a responsibility to ensure that there is the appropriate specialist provision available when commissioning such services from the care home sector. These specialist services must maintain close links with the care home and be responsive to the specialist needs of the unit, as well as with the GP practice and MDT. This includes having clear contact details, referral routes and communication channels for when specialist advice and support is required.
Getting It Right For Everyone (GIRFE)
The Scottish Government's National Care Service consultation consulted on a National Practice Model: Getting It Right For Everyone. A proposed multi-agency approach of support and services from young adulthood to end of life care.
GIRFE will help define the adult's journey through individualised support and services, and will respect the role that everyone involved has in providing support planning and support. Too often, adults and their families are excluded from assessment and support processes by complex bureaucracy.
GIRFE is about providing an easier way to access help and support when it is needed – placing the person at the centre of the decision-making process to achieve the best outcomes, with a joined-up, coherent and consistent multi-agency approach regardless of the support needed at any stage of life.
Principles:
- Focused on individual care needs
ensures that every person is at the centre of informed multi-disciplinary decision making and the support available to them.
- People treated as equal partners
share decisions about treatment options so people are supported to make an informed choice about what's right for them.
- Based on an understanding of the wellbeing of individuals
adopts a person centred approach to ensure that a person's needs are taken into account while acknowledging that their needs will vary over time.
- Based on early intervention
aims to ensure individual needs are identified through meaningful and ongoing conversation, and appropriate support provided, as early as possible.
- Requires joined-up working/information sharing
is about people and their care teams working together in a co-ordinated way to meet specific needs, provide care they really value and improve their wellbeing.
- Requires an evidence-based approach,
where professional judgment, the best available evidence and people's preferences converge to ensure we provide better value care for the people we care for and for the system, and in turn help to reduce waste and potential harm.
- Based on a human rights approach
about ensuring that both the standards and the principles of human rights are integrated into policymaking as well as the day-to-day running of organisations. Everyone has the right to be involved in decisions about their treatment and care.
Recommendations
2.1 Regular MDT meetings (face-to-face, virtual or hybrid) should take place involving the care home team, the GP practice and relevant other professionals to co-ordinate and plan healthcare.
2.2 The administration and support of MDT meetings should be co-ordinated between the HSCP and the care home.
2.3 People living in care homes should have the opportunity to involve a family member or any legally appointed welfare guardian or attorney during consultations with members of the MDT.
2.4 As MDTs form and develop, opportunities for shared learning should be explored, to develop the knowledge, skills and experience required to provide the best possible care.
2.5 Wherever possible, each care home should be linked with a named GP practice that will play a lead role with that home. Where this is not possible, HSCPs should work with the local care homes and GP practices to establish safe and reliable alternative arrangements that enable effective MDT working.
2.6 People living in care homes should be made aware of the benefits of being registered with the GP practice that is linked to the care home that they live in, however they should not be forced to change GP practice.
2.7 Health Boards should review Local Enhanced Services (LES) that relate to care homes and revise them in line with the aspirations of the 2018 GP contract and the ambitions of this framework.
2.8 HSCPs must ensure that there is access to appropriate specialist provision when commissioning with the care home sector to provide specific services for people with highly complex care needs.
2.9 Care home teams must be provided with contact details and referral routes for all members of the MDT. Where these are not clear, the HSCP should work with the care home to obtain these.