Suicide Bereavement Support Service: evaluation report - year 2
This report covers Year 2 of the multi-year evaluation of the Suicide Bereavement Support Service (SBSS). It draws on two years of the evaluation to date while also providing additional learning and evidence on experiences and outcomes.
5. Experience and outcomes for people supported by the service
In this chapter, we discuss the experiences of the support people have received from the SBSS and the difference it has made.
The findings are drawn from interviews with 42 people supported by the service over the evaluation period. Just under half (19) have engaged in a single interview, 17 engaged in two separate interviews, and six participated in three interviews, each taking place between four and six months apart. This has provided insight into short and longer-term experiences and outcomes.
The chapter is organised under the following headings:
- 5.1 Accessing the service.
- 5.2 Reasons for accessing the service.
- 5.3 Experience of support.
- 5.4 Impact.
- 5.5 Strengths and areas for improvement.
5.1 Accessing the service
In this section, we discuss how people accessed the service, their first contact with the service, and whether access came at the right time for them.
Pathways into the service
People were referred to the service through a formal referral process by an organisation or service, with various examples provided, or self-referred by contacting the service directly. Those referred to the service confirmed they were given enough information to decide about a referral. Some recalled that the service had been described to them as specifically for people who had been bereaved by suicide. Others could not recall what had been explained to them about the service.
A few people also described referrals to other organisations, which led to them accessing the SBSS. For example, one person who is a carer for their partner said her GP had referred her to an organisation that supports carers, and that organisation made them aware of the SBSS. Several of those who self-referred explained that they had learned about the service in different ways, either through conversations with friends, family or colleagues. Others came across it in the local press or online, doing their own searches or through social media. A few people found out about it when they revisited leaflets left with them by Police Scotland. In these instances, none could recall discussing the opportunity to be referred to the service.
“Well, it was actually from leaflets that had been lying for a while, and there were actually quite a lot of leaflets that the police gave us right afterwards, and I was just looking through them one day and came across some numbers to phone.”
For those who self-referred, the most reported area for improvement with the service was its visibility and awareness, particularly among the general public.
“So the only thing that I'd say needs improved is I didn't know about the service. It was the lady from Petal [another support organisation] that told me.”
A few people described hesitancy or difficulty in taking that first step to contact the service. At that time, they explained that they did not know what they wanted to say or what they were looking for. One person described having the contact details for over a week before being able to make contact.
“I had the details, and I still remember going to make the call, and I just couldn’t. Even when I finally managed to, I had spent the morning staring at the phone and thinking about what I was going to say. It would have been easier if I hadn’t been the one having to do that … And because I was sort of in crisis at that point, trying to leave an answer phone message when you're crying. It's actually really quite hard.”
Feedback was mixed about the timeliness of accessing the service. Some people reported feeling that it would have benefitted them to have been able to access the service earlier than they had. This was particularly apparent for those referred to the service after accessing health services at a point of crisis.
“I took a complete breakdown [following the suicide]. I spoke to the manager at the [GP] surgery. And they, in turn, spoke to the mental health nurse who phoned me and arranged for the referral to the service.”
However, feedback from those who reported accessing the service at the right time suggests that what constitutes the ‘right time’ is different for every person. Some accessed the service within days of their bereavement, which was right for them. They reported recognising at that very early stage that they needed some form of support to help them with what they were experiencing. Some accessed the service weeks and months after their bereavement, which felt like the right time for them. For some of these people, this was because they were also dealing with other issues they felt they needed to address first, sometimes involving accessing and receiving support from other services and organisations. Others spoke about the need for support only becoming a consideration for them after a passage of time since the bereavement. Two people recalled being offered a referral by Police Scotland but declining it at that early stage.
“A bit of time had passed. I think I just wanted the funeral and everything out of the way before I thought about any of that. Yeah, that was obviously down to me though, that was like my timeframe.
And then, after several weeks, I felt I wasn't moving forward, and I needed to talk to somebody.”
First contact from the service
Following a referral/self-referral, people supported by the service reported that they received a rapid response from the service. While not everyone could recall the exact timeline, most reported being contacted within 48 hours. Several people reported that this had exceeded their expectations, and none had any concerns about the timeliness of the response. Some people also spoke about the initial call from the service, providing reassurance and comfort from how the member of staff spoke with them and how the service was described.
“[Service staff] really put my mind to rest, right from the very beginning from the minute I spoke to them.”
5.2 Reasons for accessing the service
Many of the people supported by the service that we spoke with explained that at the point of accessing the service, they did not specifically know what support they were looking for or what support would help. They just recognised and realised that they needed something. As two people described:
“I didn't go in with any expectations. I was just in a really bad place. I was just like, I know I need help.”
“At that point, no, you're absolutely in a traumatic state. A state of shock, you're not thinking, you obviously, you're busy trying to just take in the information of what's happened, and you're really not going to say I need this or that. You just don’t know what you need.”
Several people articulated how they felt when they first accessed the service and what they felt they needed support with, or access to. This included:
- Feeling isolated.
- Needing someone to talk to.
- Being able to better understand their experience.
- Having someone that would listen to them.
- To explore what they were feeling and why.
- Reassurance about what and how they are feeling.
- Advice and guidance.
5.3 Experience of support from the service
This section explores people’s experiences of how support is provided and the types of support they have received.
Format and frequency of support
Most of the people we spoke with received support from the service over the telephone or via video call. A small number were also having some sessions face-to-face. Most of those that received support over the phone or via video call reported that they had discussed the option of face-to-face support sessions but, for the time being, were happy with the current format. All understood and appreciated that it was their choice and received support based on their preferences. As two people described.
“We did start the walking and talking quite quick. We met up I think it was Monday, and then we were supposed to meet up again on Friday. But I wasn't doing too good, so we just had a phone call instead. It's usually a phone call or just go for a wee walk for an hour once a week.”
“I was given the opportunity to do Zoom calls, but we've just continued with the phone, I prefer the telephone contact. It is just a bit simpler and easier to have a telephone conversation. It's just a little bit less formal. It's more private, I suppose, a phone call. It sounds strange, but you might not kind of feel up to seeing someone in person on a Zoom call.”
People supported by the service explained that they led decisions about the frequency, duration and scheduling of support sessions. The frequency of support sessions varied among those we spoke to, with some engaging weekly, some fortnightly and others monthly or every six weeks.
“It was very much self-directed, what my needs were, and that was the right thing. It wasn't being led for me; it was being led by me. They just went with what I said, and, you know, sometimes just through conversation, we would be able to plan out whether I needed it in a few days or at the end of the week, and it kind of led its own path naturally.”
Some people who have been engaged with the service over a longer period also described how the frequency of their support sessions had reduced over time. Within this were examples of support frequency reducing but increasing again due to an incident, event or anniversary that had impacted the person negatively and increased their support needs. Often after a period of increased frequency, this would then reduce again. Having the flexibility to adjust the regularity of when people received support was highly valued.
“At the beginning, it was weekly, and then it was fortnightly and then it went to monthly but then it had to go back to fortnightly again because of the time, of what was happening in my life. It was quite bad over the Christmas period. And so it was every fortnight, and then it went back to four weeks.”
Relationships and the approach of service staff
People supported by the service spoke about the importance of quickly establishing a relationship with the staff member supporting them, which made them feel comfortable opening up and sharing their thoughts, feelings and emotions. As two people described.
“That was something that I was worried about because you don't always, kind of click with somebody, and that's true for everybody. And you have to feel kind of reassured. But I must say, we established a very good relationship very soon.”
“I'm not one to open up easily, but very quickly I did. But it came down to the skills of [the practitioner] because normally I would not be able to do that.”
People reported that the ease and speed with which they were able to establish a positive and productive relationship with service staff was due to their approach and the following skills and qualities:
- Being a good listener.
- Having patience and letting the person move at their own pace.
- Being responsive and proactive.
- Showing compassion and having a caring nature.
- Calming.
- Non-judgemental.
Aligned with this, consistency in the staff member providing support is highly valued by those receiving support, providing them with much-needed continuity, comfort, and familiarity. The relationship between staff and the people they support is a core aspect of the service. When we spoke to people who had experienced a change in practitioner due to staffing changes in the service, their feedback their transition to working with a different staff member suggests that it was well-managed. However, several people did explain that they felt a sense of loss for a short period thereafter. People supported by the SBSS reported that they felt able to develop an equally positive and productive relationship with the new member of staff they are working with.
Practical support needs
As well as emotional support, the service also provides practical support to meet people’s needs. The supported people we interviewed provided various examples of the practical support that the service has provided, which aligned with the examples cited by service staff detailed in an earlier section.
“Sometimes she'll send me links by email or just follow up anything I request because early on, sometimes it's hard to take in information. I was so traumatised. And in the early days, you sometimes maybe don't want to follow up, or look for yourself and [practitioner] was able to pass me on information about anything that I wanted to find out about.”
People supported by the service explained that they valued this practical support as they often could not take those actions for themselves or invest the needed energy. Even though people described this as practical support, they often explained that it benefited their emotional wellbeing.
“I didn't really know where to go...the place my head was in, I couldn't even tie my own shoelaces. I needed someone that could just take that pressure off.”
A few also spoke about practical needs they planned on raising with the service, explaining that it had not previously been an immediate priority, but they were now in a place where they could turn their attention to it.
Emotional support
The emotional support provided by the service was described as invaluable and was the aspect of support that people spoke about and described most often during interviews.
“So you still remember things, and the silliest of things can bring back a memory, which can be painful. But [practitioner] has always been there whenever I've needed something. And that's been invaluable … it's a bit like a tsunami, when something like this happens, you feel that you're drowning, everything just swamps over you, and the waves coming are too high to swim. And time just means that the waves start getting a bit smaller and smaller, but they're still there. And occasionally, you'll get a wave that comes out of nowhere.”
Some people supported by the service spoke about previous experiences of grief and loss but described how the feelings and emotions are different when bereaved by suicide. People recounted experiencing various emotions, including sadness, anger, blame, guilt and shame.
“I can certainly, particularly the blame, the guilt, the anger. It has been helpful for me, particularly to stop and think, well, it's not my fault he's gone. And I can feel angry that he's not here. So it's been really helpful, I feel like I can understand why I feel or think like this, but I am not quite managing the processing my way through it on my own. And that's where [practitioner] kind of been able to say, let's talk about that.”
People reported that emotional support provides them with a safe space to explore, understand, process or cope with their emotions and speak openly and honestly about their feelings. When exploring how that support is provided and the nature of the support they had received, the following were commonly cited:
- Being able to talk openly and be listened to without judgement.
- Offering advice and guidance when needed.
- Helping to understand and reassuring them that their feelings are normal and allowed.
- Strategies to help manage feelings.
- Reflecting thoughts and feelings back to explore and process them.
- Highlighting and celebrating the little successes and providing encouragement.
People who had been engaged with the service for longer reflected on how their emotional needs changed over time. This was commonly articulated as feeling better able to cope with their emotions, having more good days than bad and feeling less need for support. However, it was also highlighted that this could fluctuate, and periods of improved emotional well-being could be followed by periods of increased emotional need.
“And it kind of caught me off guard because I wasn't expecting to be upset about that. And then it wasn't till I sort of got my birthday card from Mum, just saying from mum, it was like, oh my god, and that was my first ever birthday without him. And it was like, this whole can of worms just exploded. And if I didn't have the service to have fallen back on at that point, being perfectly honest, I would be quite scared about where I would be now.”
Accessing other services
While people recalled discussions about additional support and available services, most who engaged in the evaluation felt that the service was meeting all their current needs. Even so, they acknowledged that they may need additional or different support in the future and appreciate being more aware of what is available. Examples of additional support taken up by people who accessed other services related to their bereavement include formal counselling services and group peer support.
“Yeah, I've started, so I have gone to a group in Perth. And then I've also gone too, I think it's facing the future by the Samaritans. So [practitioner] recommended both of those. And those are things I would never have known about or attempted because it would have been too daunting.”
While most people who accessed other support reported that it had benefited them or a loved one, a few found the peer support groups difficult. They explained this was because of people's different stages in their grief and some of the subject matter discussed.
“I've actually went, three or four times to the group session. I've now just withdrawn from that again because it's not suitable for me.”
People also appreciated that the service helped them identify organisations to support them with issues unrelated to their bereavement. Examples include help to access employment support, arts and crafts activities and Advocacy support. They also reported that the service had shared links and signposted them to a variety of different websites and resources that they could access.
5.4 Impact
When talking with people about the difference that support had made to them, the vast majority described improvements in their mental and emotional wellbeing and being better able to cope with and return to day-to-day life and activities. We discuss each of these in the following sections.
Improved emotional and mental wellbeing
People reported that being able to talk openly, share, explore and understand their feelings and emotions with someone who listens and responds in a compassionate and non-judgemental way was critical to the improvements they experienced in their mental and emotional wellbeing.
Many people described the difference in terms of how they were feeling. Commonly this related to a more positive outlook, increased confidence about the future, feeling mentally strong enough to get on with daily life, and doing things they hadn’t thought they would do again. It was, however, highlighted by people that while they had experienced improvements, and these could be maintained most of the time, there are things that can re-trigger/traumatise them and possibly lead to a period of feeling less emotionally and mentally well.
As with coping and re-engaging with their day-to-day lives, the extent of improvements in mental and emotional wellbeing varied among people. People supported by the service commonly described these improvements in one of three ways firstly, that they were experiencing the emotions associated with their bereavement less frequently.
“The feelings are still there; I think they always will be. But I suppose it’s not experiencing them as often as I was. And when I do, I can be present with them, I accept I’m feeling them, but they don’t affect me as much.”
A second improvement related to people being able to better manage their emotions and reduce the negative impact that they were having. Lastly, a small number spoke about the support having helped them to overcome feelings of self-blame and guilt.
“So I suppose I don't feel guilty now, obviously, I miss him dreadfully, but I don't feel guilty about it. Whereas at the very beginning, I felt so guilty about it. I didn't think I could laugh. I didn't think I could have a life.”
Other examples of improved emotional and mental wellbeing and the mechanisms that lead to these improvements included:
- Having the reassurance that someone is there for you.
- Reducing feelings of isolation and being alone.
- Being able to get things off their chest and having an outlet when they needed to vent.
- Being in a place where they could accept and understand what had happened.
- Feeling stronger and more mentally resilient.
For some people, the difference was more profound. It was not uncommon for people to explain that they feared suffering drastic consequences because of their bereavement had it not been for the support of the service. As two people described.
“I'm not saying this lightly, but I would either be in hospital, jail, or in the ground basically.”
“Absolutely massive. I just wanted to die. I didn't want to be alive anymore. I don't feel like I actually want to die now. Without that service, I maybe wouldn't be here, to be honest.”
Measuring improvements in mental wellbeing
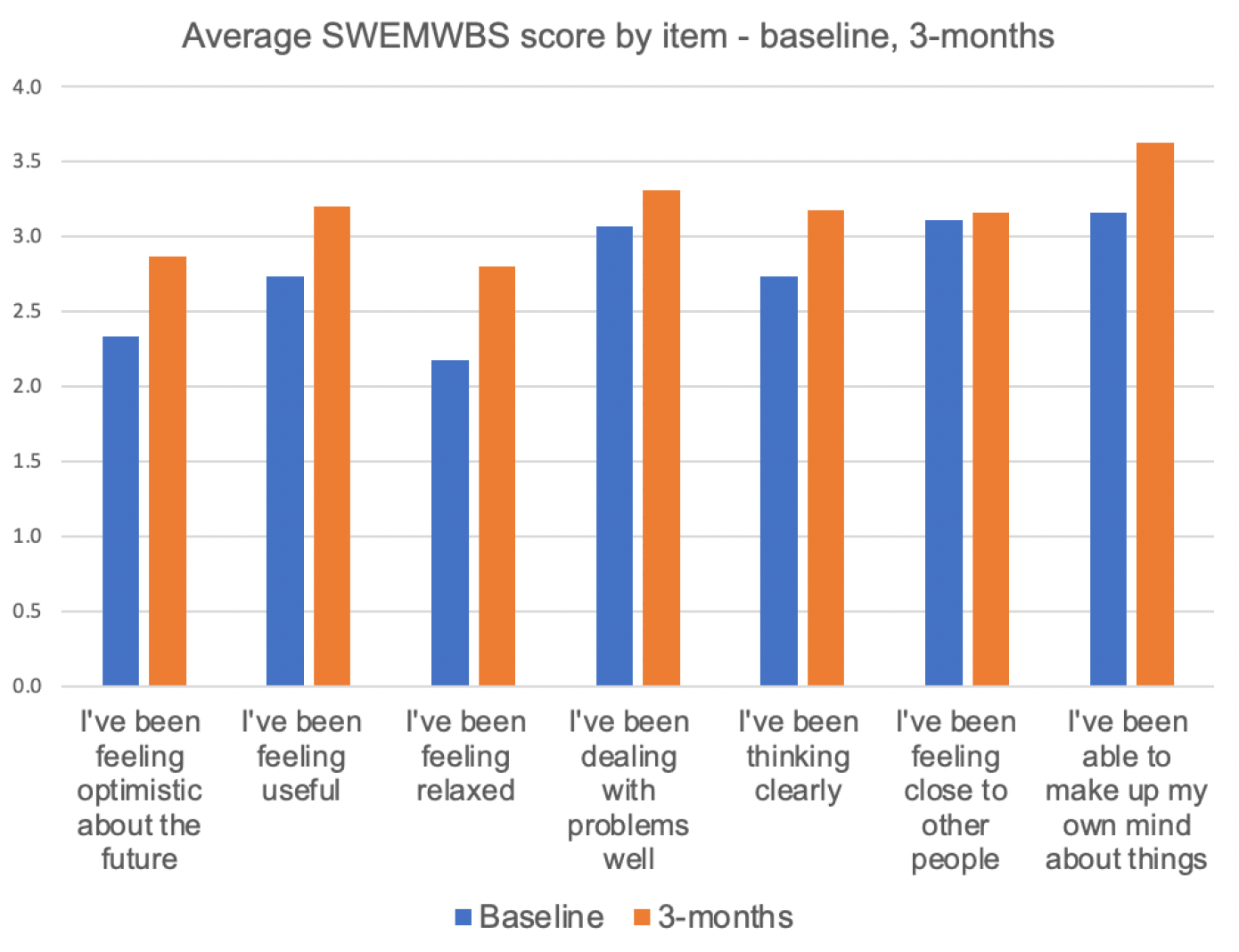
To further understand the service’s impact on the mental and emotional wellbeing of the people they support, service staff administer the Shortened Warwick-Edinburgh Mental Wellbeing Scale (SWEMWBS). This is done at three different time points in a person’s support journey to measure the change in levels of mental wellbeing over time.
SWEMWBS data gathered by the service demonstrates an overall increase in wellbeing at the three-month follow-up compared to the baseline. The chart below provides the average score across each item of SWEMWBS based on 45 people (30 Highland, 15 Ayrshire and Arran) who completed SWEMWBS at baseline and three months later.
Twenty-four people (18 Highland, six Ayrshire and Arran) have completed SWEMWBS at baseline, then three and six months later. The results are shown in the chart on the following page.
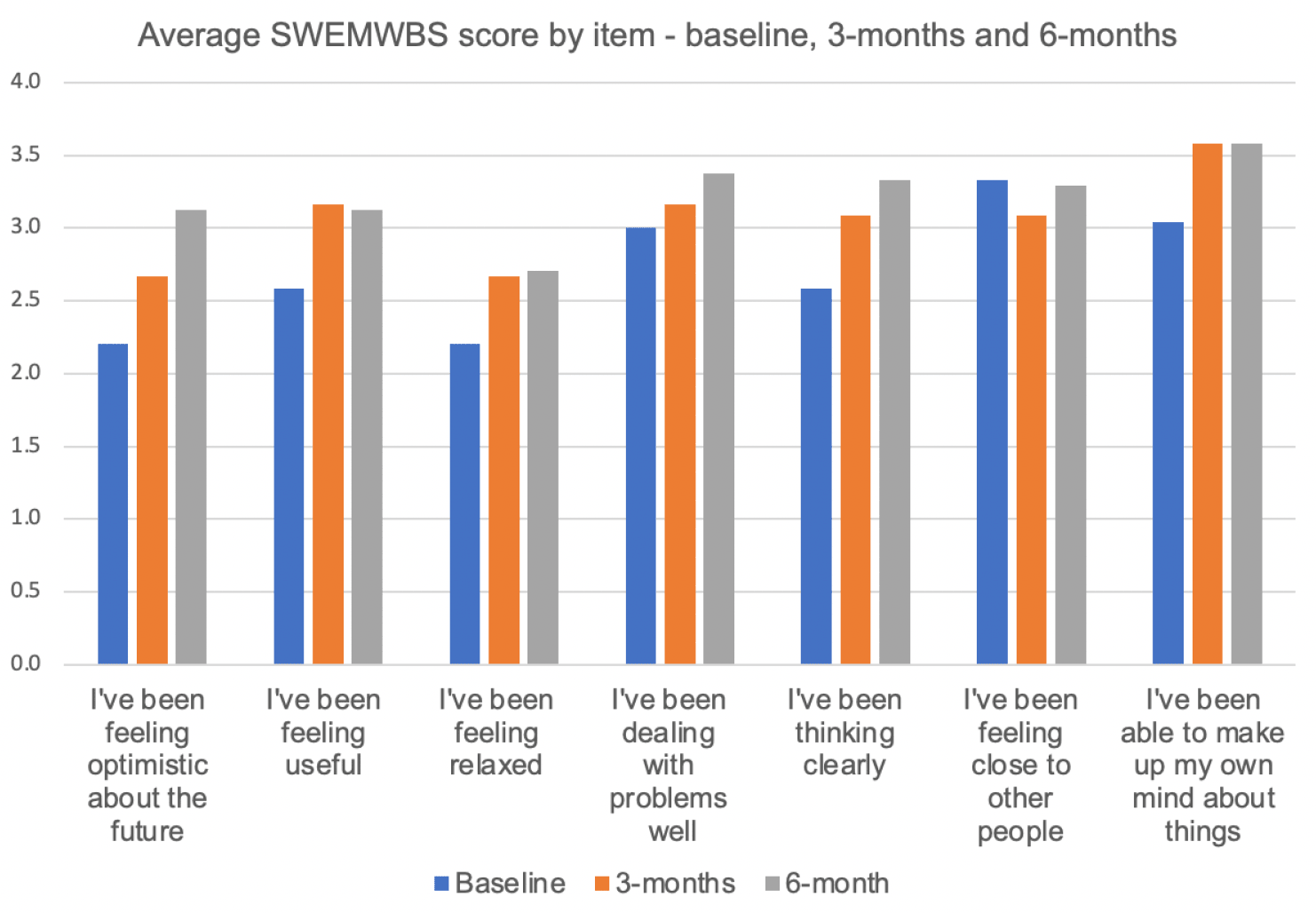
After three months and at six months, scores were significantly higher than baseline. The average SWMWEBS score at baseline for the three-month group was 19.3, which rose by 2.8 to 22.1 after three months. For the subset whose SWMWEBS scores were measured at six months, scores rose by 3.5 from 19.0 to 22.5.
The average score across all but one item (“I’ve been feeling close to other people”, which returned to baseline levels following a dip at the three-month point) increased from baseline compared with the six-month follow-up. There is a very slight drop in score in one item (“I’ve been feeling useful”,) and another item has remained the same (“I’ve been able to make up my own mind about things) when comparing the 6-month follow-up with the three-month follow-up.
Better able to cope and return to day-to-day life
A recurring theme throughout the evaluation has been the positive impact the service has had on supporting people to cope better with their day-to-day lives. People supported by the service highlighted the interlinked nature of improved emotional and mental wellbeing as an enabler to coping and returning to everyday activities, further helping their mental and emotional well-being.
The extent to which people feel better able to cope with daily life and have returned to activities they had participated in before their bereavement varied. Generally, those at an earlier stage in their support journey described small steps and improvements, whereas more significant changes tended to be reported by those who have engaged with support for longer.
Those that described small changes and steps provided examples which included:
- A shift from not wanting to get out of bed to managing to get up and do some household chores.
- Being reliant on home deliveries for groceries, but now going to the supermarket for essentials.
- A reluctance to be outside of their home to now going out for a coffee.
Those who were further along their support journey described how, over time, they had been able to get back to doing much of the things they did before their bereavement. Examples of this included:
- Going on holiday again
- Being able to remain at work, return to work or apply for new roles.
- Re-engaging with hobbies, interests and social activities.
- Some of these experiences are recounted in more detail by supported people below:
“I think going [on holiday] gave me a bit more confidence that I can do things myself. And a lot of that has to do with the work that [practitioner] has done with me, I think, just sort of saying [to myself], I can do it, that I am strong, that I am going to get through this. And that it's absolutely fine to have wee blips. It did give me that sort of confidence, that I could go off and do things.”
“One of the things that I really kind of struggled with was sort of that going out, and maybe not even having a meal, but like going for a coffee. And I've actually managed to be able to do that by myself.”
In terms of coping better, some people tended to articulate this as being able to get on with their day-to-day lives, having more good days than bad, and the bad days not being as difficult as they had been. Others spoke about being able to get on with life more easily, and as mentioned previously, people tended to link this to experiencing improved mental and emotional wellbeing. Aligned with this, some people highlighted that although they generally felt better able to cope, there could still be days that set them back, where they felt less able to manage again.
A small number of supported people spoke about how engaging with the service had helped them rebuild their confidence, which again was an enabler to better coping with life and returning to daily activities. A few people explained how they now felt more comfortable and better able to talk about their experience of bereavement and use their loved one’s name in conversation again. This was attributed to having been able to explore their experiences in a safe space with the service, which gave them the language, confidence and comfort to do so with others. As two people described.
“Before I started doing this, you know, I found it impossible to say my son's name. But for example, last weekend, there was a community event, and I went to this event, and I could actually reference him. Now for me, that was a huge step.”
“I've always thought of myself as being quite a strong, maybe not independent, but a strong person. And I think all that happened with [loved one]. It just pulled the rug out from under me, and I think I am getting back to that person that I was.”
People valued that they could move forward at their own pace and did not feel any pressure from the service. They reflected that while there could be periods where they didn’t feel like they were moving forwards and sometimes moving back, the service was always there alongside them.
“They [the service] help me reflect and helped me move forward at a pace that I can cope with, and `they've been really excellent at helping me take the next step forward and whether I want to take the step forward. Some days I've not felt like taking that step forward. And I just have to stand in the same place many, many times. And I think the biggest thing I want to say is that they stand there with me… you're not alone.”
5.5 Strengths and areas for improvement
The following provides a summary of the identified strengths of the delivery model and areas that people supported by the service suggested could be further developed or improved.
Strengths of the service delivery model
Several features of service delivery were commonly identified as strengths by people supported by the service. Each of these is described below:
- The service staff and their approach – staff skills, qualities, and ways of delivering support was the most cited strength of the service. Their approach was described as non-judgemental, compassionate and sensitive, responsive to needs and demonstrating empathy.
- Person-led and person-centred – a highly valued feature of the service is that the person receiving support dictates the format, frequency and duration of their support sessions. Furthermore, knowing that they can bring whatever they want to discuss, and that each session is focussed on their needs was also important to people.
- Flexibility and availability – people are reassured that if they choose to reduce the frequency of support, it can be increased again should they need it. Furthermore, people appreciated the understanding shown by service staff if they were unable to make an agreed appointment and their flexibility in arranging another date at the earliest opportunity. Knowing that they can contact the service if they need support between their scheduled appointments also provides people with a great deal of reassurance and confidence that someone is there to help them when needed.
- Someone outside their family and social network – people consistently spoke about the value of being able to talk to someone who is not a friend or family member. This was for a range of different reasons, most commonly not wanting to burden friends and family, to be able to say things they would not be comfortable saying to friends and family and to avoid upsetting them.
- Consistency in support – people supported by the service value a consistent connection with a practitioner, believing this enables service staff to develop an in-depth understanding of them, their circumstances, and their needs. It means they do not have to cover the same ground with different members of staff. However, it is also important to highlight that those that have experienced a change in the member of staff supporting them reported the transition as smooth, despite finding it daunting. People reported that their new practitioner had a thorough understanding of their situation and circumstances, quickly put them at ease, made them feel comfortable, and were quickly able to develop a positive relationship with them.
- Speed of access – being able to start receiving support so soon after the initial contact and having no waiting lists was considered essential. People explained that they needed the support at the point they had been referred, and any delay would likely have had a negative impact.
- No time limit – having no limit on the length of time that a person can access the service was seen to remove any potential pressure to be progressing with how they were coping with their bereavement and allowed people being supported to go at a pace they were comfortable with.
The strengths of the model, as identified by people receiving support, were also viewed as essential components for any roll-out of the service beyond the pilot areas.
Suggested improvements
The area most suggested for improvement by people supported by the service related to awareness and accessibility, particularly amongst those that feel they would have benefitted from engaging with the service earlier. Several people described struggling to find support when they were looking for it. Furthermore, many of those that were referred to the service commented that they had not come across or seen anything about the service since that point.
There is a strong feeling among the people supported by the service that it needs to be more visible. Other than awareness of the service, there were no other commonly suggested areas for improvement. However, there were some further suggestions from individuals. These were:
- Being sensitive to the value someone receiving support places on anonymity and considering this when offering face-to-face sessions.
- Offering people therapeutic interventions, such as CBT, in the context of not being able to easily access it elsewhere.
- Having an information pack available that includes links and resources that they commonly share with people, as well as containing information about the emotions people will likely experience, and details of other organisations.
- Creating short bios for service staff that can be shared with people accessing the service so that they know a little about the person supporting them.
- Forming peer support groups.
- An email address or online form as an alternative to phoning the service when making a self-referral.
Contact
Email: socialresearch@gov.scot