Suicide Bereavement Support Service: evaluation report - year 2
This report covers Year 2 of the multi-year evaluation of the Suicide Bereavement Support Service (SBSS). It draws on two years of the evaluation to date while also providing additional learning and evidence on experiences and outcomes.
4. Management and delivery of the SBSS service
This chapter explores experiences of managing and delivering the service and the learning generated. The findings are drawn from interviews with SBSS staff with oversight and management responsibility and practitioner staff who support people. Feedback from those who referred people to or received referrals from the service has informed the section on referral pathways and the wider support landscape.
The chapter is organised under the following headings:
- 4.1 Overarching service structure
- 4.2 Service delivery model
- 4.3 Delivering support
- 4.4 Learning about the needs of people the service supports
- 4.5 Staffing, training and support
- 4.6 Referral pathways and the wider support landscape
4.1 Overarching service structure
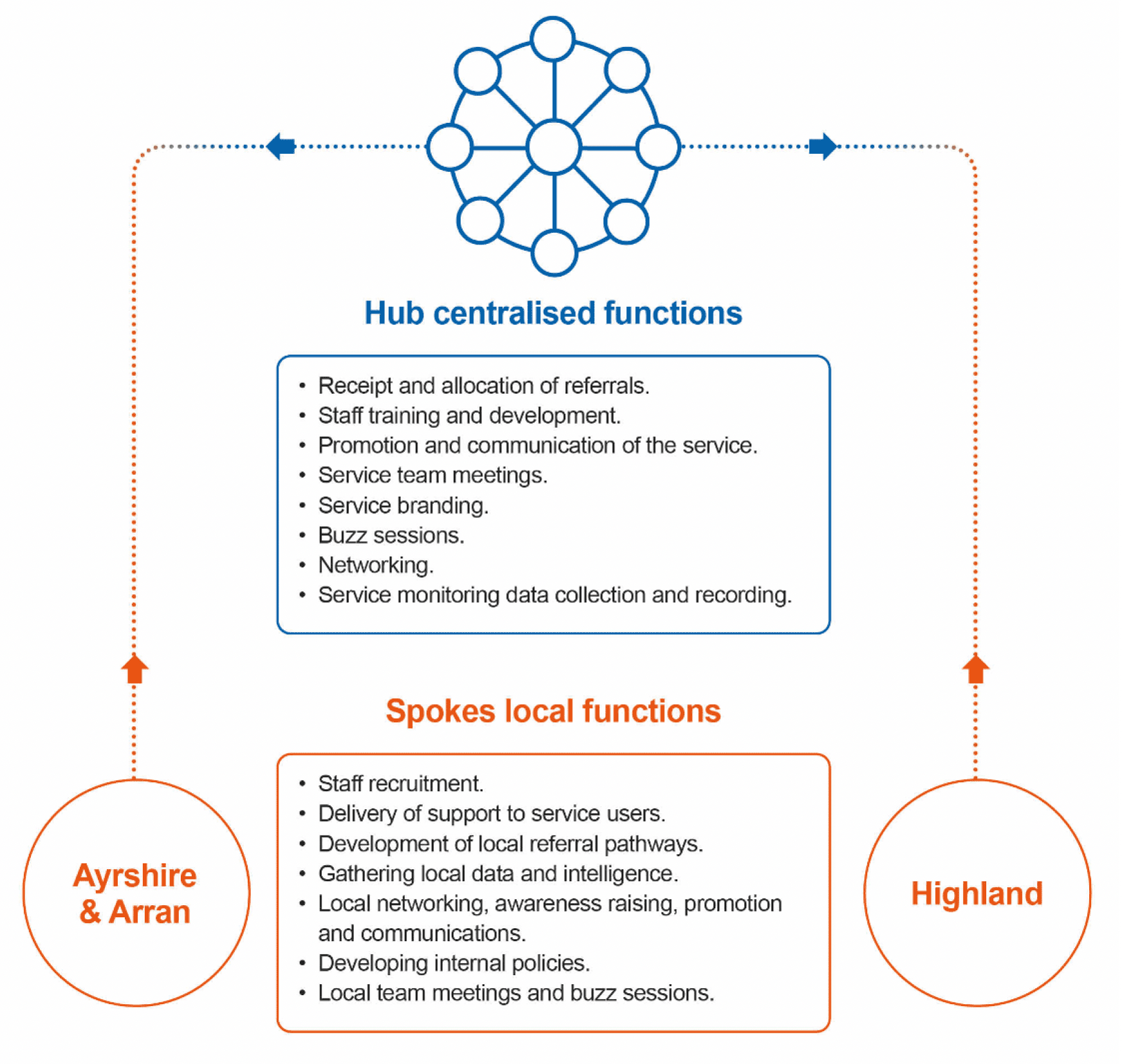
Link to detailed description of infographic content
The service is structured around a hub and spoke model, where the hub is responsible for centralised functions that support and influence local delivery, carried out collaboratively across the two partner organisations. The spokes represent the two delivery areas, with defined local functions and responsibilities.
4.2 Service delivery model
Several core components of the delivery model were consistent throughout the pilot:
- Rapid response to referrals/self-referrals received (24hr target).
- Provision of person-centred emotional and practical support aligned with needs.
- For delivery features such as the format, frequency and duration of support sessions to be led by the person being supported.
An overview of the service delivery model if provided in the infographic on the following page.
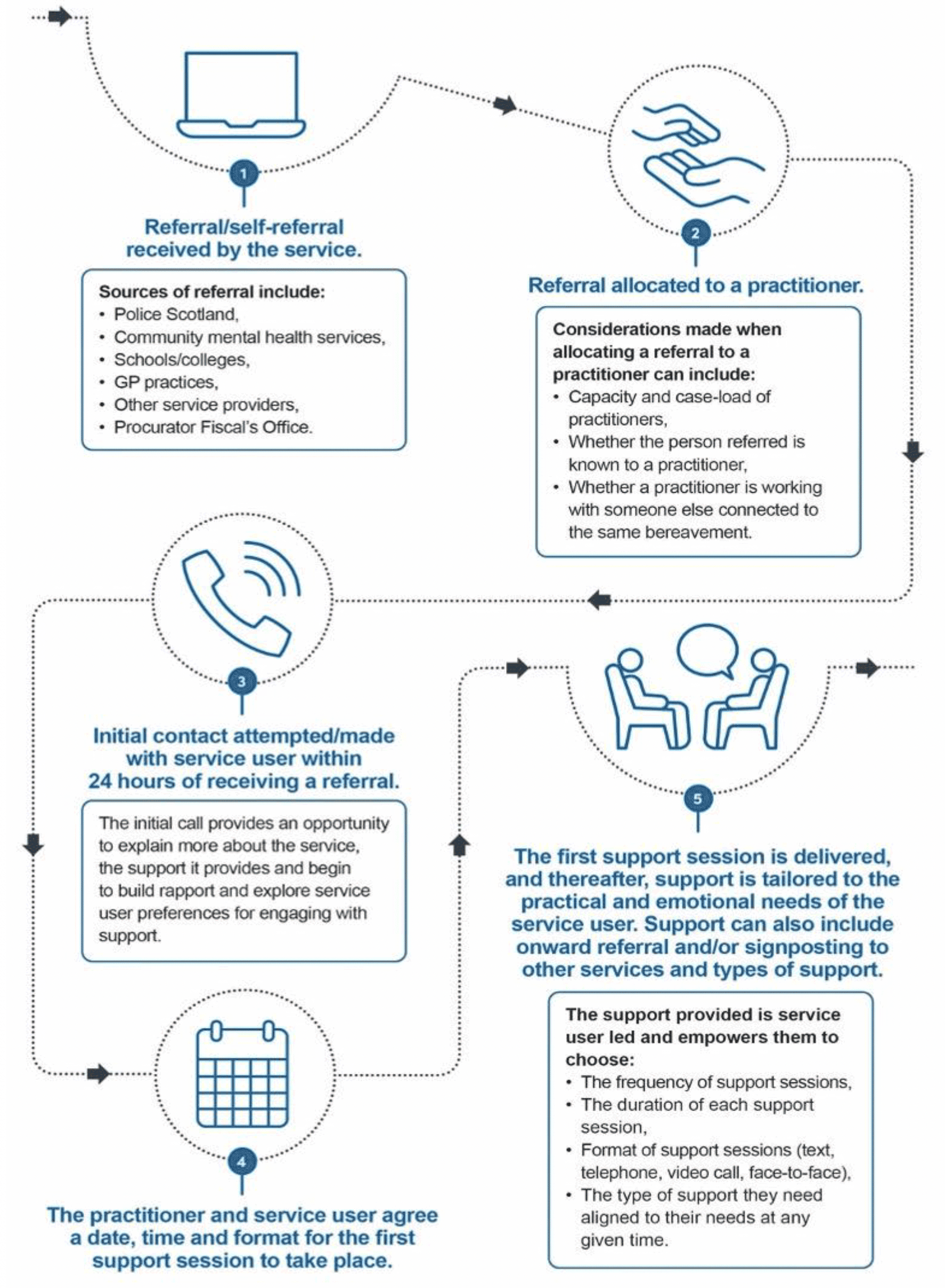
Link to detailed description of infographic content
4.3 Delivering support
This section explores the different components of service delivery.
Mode, frequency and duration of support
The service launched in August 2020 when COVID-19 restrictions were still in place. Support could only be provided via telephone or video calls. As restrictions were lifted, the service began offering face-to-face support sessions.
During the recent fieldwork phase, service staff reported that most people receiving support still opt for telephone or video calls, though several have taken up the offer of face-to-face or accessed a mixture of both. One practitioner reported that most of the people they support now receive face-to-face sessions but did not know why that was the case. Face-to-face sessions can include ‘walk and talk’, home visits or meetings in other public spaces. This presents some practical and logistical challenges, particularly in winter when the weather makes it difficult to meet outdoors. Suitable indoor public spaces that provide enough privacy and a suitable environment are also difficult to identify. The additional travel time for support workers was also highlighted, and service staff acknowledged that it could become difficult to manage if many people being supported start taking up the face-to-face offering.
“Covering such a wide area as well can be really difficult because, for example, if I was going on a home visit to the lady I was talking about, or even further afield, it takes me over two hours to get there and then the same back, so then it cuts down the amount of people that I could see in that day.”
While staff see the option of face-to-face support sessions as a positive development, one practitioner highlighted a need to be careful when offering this to existing people receiving support. In one instance, they made a person aware of the option to meet up face-to-face and found that this offer unsettled them as they had valued and took comfort in the anonymity of receiving support by phone.
People receiving support from the SBSS control the frequency and duration of support sessions and the length of their engagement with the service. Staff explained that they highlight this during early sessions and remind people that they are in control at later stages. Staff further reported that the frequency and duration of support sessions tend to reduce over time. However, the timeframe can vary significantly depending on the needs of each person being supported.
“There's just no rhyme nor reason to it, it's just, obviously, everybody's individual, and you know, their journey is very personal.”
Linked to a person’s needs around the timing of pivotal events, anniversaries, or incidents, Session frequency may reduce and then increase. Service staff highlighted that when people receiving support reduce the frequency of their sessions, it was important to reiterate that support can be increased again should people feel they need it. This prevents anyone from potentially needing support and not accessing it.
Practical support needs
Service staff observed that providing practical support was less common than delivering emotional support to meet people’s needs. While staff make efforts to explain the different types of support they can provide, people receiving support are less likely to explicitly express their practical needs. Instead, practitioners use their skills to pick up on and identify opportunities where practical support can be offered to meet a particular challenge, issue or need.
“Not once has somebody said to me, can you do this for me? But then, you know, you'll hear it, you kind of just have to work instinctively. You know, somebody just said to me earlier on, I really want to access the police records, but I just don't know how to do it. And I said, listen, you don't have to, but if it's something that you want me to look at and see what the protocol would be, I'm absolutely happy to do that. And they were absolutely happy for that to be offloaded.”
Feedback from service staff suggests that there is little commonality in practical support needs across the people they support, with these needs specific to each person’s circumstances. Throughout the pilot, examples of practical support have included:
- Liaison with a local authority housing department.
- Help to access police records.
- Help to access their loved one’s phone.
- Contacting a GP on the person’s behalf.
- Support with locating a solicitor that had developed a will.
- Finding information and resources.
- Accompanying people to appointments.
- Supporting arrangements for scattering ashes.
- Looking into benefits.
While providing practical support is less common, service staff see it as valuable and necessary. They reported that people greatly appreciate the practical support they receive, giving them one less thing to think about and lessening the load.
Emotional support needs
While the service is not intended to replace or provide formal counselling or other talking therapies, a common feature of the support provided by the SBSS relates to emotional support needs. Service staff described the main features of emotional support as follows:
- Providing a safe space for people to share their thoughts, feelings and emotions.
- Helping people to explore and understand their feelings and emotions using different models and approaches.
- Reassuring people that their emotions and feelings are normal.
- Offering reflections from previous conversations and sessions.
- Providing constructive challenge, positive encouragement, guidance and advice.
- Sharing strategies and techniques that support emotional wellbeing.
- Sharing information and resources.
- Setting goals/actions/plans that support people to re-engage with day-to-day activities or hobbies.
- Helping people to recognise their progress.
Staff may deliver a range of emotional support at different points in each person’s journey and within each support session, depending on their needs and what is being discussed or explored at any given time.
“It’s just about knowing what is needed at that time. It might just be about listening and giving them that space to get it out, other times, it might be taking them back to something that you discussed in another call. It’s responding to what they need.”
4.4 Learning about the needs of people the service supports
Service staff have gained significant learning about the support needs of people that access the service, the factors that influence this, and the approaches and tools effective in meeting those needs. The main points of learning are detailed below:
- For most people who have been recently bereaved, immediate emotional needs relate to the impact of the trauma they have experienced. For those who enter the service later, the extent of this can be less acute.
- Those referred to the service in the days immediately after their bereavement can sometimes be more difficult to engage in support. In contrast, there is more effective engagement from those referred after a few weeks or months have passed. Some staff questioned whether a referral in the immediate aftermath of a bereavement is the most effective approach.
- Everyone is at a different point in their bereavement journey and has specific needs, which are influenced by circumstances and wider life events. Examples of factors that affect the extent of emotional support people require include existing personal support structures, other challenges they are facing (e.g. financial), returning to work following the bereavement, tensions in family relationships, birthdays and other anniversaries.
- There may be fluctuations in the intensity, frequency and types of support people need at any given time.
- It is important to ensure that people being supported understand that they can increase the support frequency again if they have previously chosen to reduce it. Furthermore, the service must have the capacity and flexibility to respond to these changes.
- Service staff need to have a range of tools, approaches, and models at their disposal to meet the emotional needs of the people they support. Service staff reported that the models and tools they gained through trauma informed practice training have proven to be useful and effective. Models that help people to understand the grief process, and the emotions they are experiencing have also been utilised to good effect.
- Beyond the early stages of support, there is often a shift to focusing on supporting people to identify and take the steps towards their new routine, returning to work, starting to socialise more, and resuming other day-to-day activities. People receiving support also become more open and ready to consider other forms of support, such as group-based peer support, employment support or assistance with issues not directly related to their bereavement.
- While people supported by the service often have practical support needs, they rarely proactively seek help for those needs. To identify and meet someone’s practical needs, SBSS staff must be vigilant to pick up cues that signal someone has a practical support need, then discuss it further and explore how to address it.
- A key role for staff is to help people see how far they have come. Staff take time to reflect on the activities that people previously could not picture themselves coping with and were now managing. This highlights the importance of listening, as they could identify small changes and progress that the person receiving support might not have recognised.
In the most recent fieldwork stage, service staff shared examples of cases where people had pressing support needs potentially related to or exacerbated by their bereavement, which fell outside the remit and expertise of the service. These examples related to mental health needs and problem alcohol and/or substance use. Staff explained that there are instances where these needs can be met by other services and provision alongside the suicide bereavement support provided by the SBSS.
However, there have also been instances where the severity of needs related to mental health and/or problem alcohol or substance use are identified by the person being supported as needing to be addressed before they can effectively engage with support for their bereavement. SBSS staff will assist them to access the required support if people are not currently engaged with services that can meet those wider needs.
Ending support
Feedback from staff suggests that people disengage from the service in one of two ways. Firstly, someone may simply stop attending sessions and stop responding to contact from the service. This has tended to follow a period of short, low-frequency sessions. While staff believed this reflected progress on the part of a person receiving support and the extent to which their needs had been met, it was still unsettling for staff. The lack of contact, and the support ending that way, is unexpected given the positive relationships that staff feel they have established with the people they support.
“I've had people that just stop engaging. You send them a text, or you phone and you just don't get anything back. Which can be worrying because you don't know what's happened. Like, have you got the support and you don't want to engage anymore? You've moved on and me texting or calling is triggering you and you don't want to think about that time? You just don’t know.”
In these instances, there is a protocol for staff to follow:
- Step 1 - attempt contact weekly for four weeks.
- Step 2 - attempt contact monthly for three months.
- Step 3 - send a final written letter explaining that they can re-access the service in the future if they need to.
Service staff feel that the protocol provides an approach that allows people to re-engage while not being overly intrusive. The second type of ending was described by service staff as a managed exit, agreed following discussion with the person and following a final session. Again, this typically follows a period where the frequency and intensity of support have reduced, and there are conversational cues, such as the topics that signal the support is becoming less necessary, for example, people talking less about their bereavement and the impact of it, and more about daily life and plans for the future. People who leave the service following a managed exit are informed that they can re-access support if needed.
“He didn't feel that the grief was the most important thing in his life anymore. He was kind of actively trying to move through that. And we had a discussion of, well, if you feel like that then that's great, you've got to a point where possibly our service is no longer needed. We agreed that I'd text him in the new year and if he wanted to engage, that's fine.”
Service staff explained that these types of concluding conversations need a lot of consideration and care. One described a situation where someone they were supporting had made significant progress and presented as coping well and returning to daily life. They prepared to have an exit conversation with them at their next support session. However, the staff member subsequently discovered that the person had been re-traumatised and needed the support to continue.
Supporting children and young people
During the pilot, the service worked with a small number of young people under 18. There were mixed experiences of successfully engaging young people in support. Sometimes, practitioners faced challenges scheduling appointments and having the young person attend those arranged. It was less of a problem for others as the young person readily engaged in support sessions.
Practitioners observed that it can take longer for a young person to begin talking about the impact of the bereavement than adults. As well as providing support through the service, practitioners will often signpost and refer young people to youth-specific grief and bereavement services, such as Winston’s Wish. The service also supports several parents/carers of young people who do not wish to engage with the service, or the parent/carer feel either the young person is not ready to engage with the service or they are receiving support from other organisations. In these instances, the parents/carers can also seek advice and guidance from the service on supporting their young person or may need reassurance that they are getting things right.
In the first annual report, we highlighted a practitioner’s suggestion that a live web chat function might be an effective way to engage with young people. More recently, this has also been requested by a young person receiving support from the service.
Supporting families
When the service supports more than one person from a family unit, this is rarely provided as whole-family support sessions. Most people opt for one-to-one support. Given what people receiving support from the SBSS have told us about the importance of being able to speak to someone outside of their network of family and friends, this is not surprising.
However, a few instances of group support were described by staff. One couple received a blend of one-to-one and joint sessions. The practitioner observed different dynamics across the two formats, where the people receiving support seemed less open in discussions during joint sessions. Another couple initially received support sessions together but moved to one-to-one sessions due to each person engaging at a different pace and needing different types and intensities of support. Each wanted space to focus on their own needs and journey. The final example involved parents and a child who initially accessed group-based support though only had a single session in this format before opting to move to one-to-one sessions.
When the service has received referrals for more than one person in a family unit or connected through the same bereavement, efforts are made to ensure that each person works with a different practitioner. This stems from early learning in the pilot, where a practitioner supporting more than one person from a family identified risks in maintaining confidentiality and the need to navigate the dynamics and relationships of the family members. There is one example however, where a parent/carer and their child are receiving support from the service, and a single practitioner supports each of them with one-to-one sessions.
Service capacity
As has been consistent throughout the pilot, service staff reported that their caseloads were manageable and that they could take on additional people requiring support to varying extents. For some, this fluctuated as they responded to the changing needs of the people they were supporting during periods when an increase in frequency was required.
As caseloads have grown, service staff commented that it can be more challenging to always accommodate people’s preferences around the day and time of support sessions. This has not created any issues; however, staff are conscious that it will become more challenging with a larger caseload. Should referrals come at a faster rate than people are disengaging, then this is a challenge that the service will need to address in the future. To mitigate capacity challenges and support planning, local service teams have caseload review sessions, supplemented with regular discussions about team capacity.
Service staff were clear that an assessment of caseload capacity could not be based solely on the number of people they were supporting due to the often-changing needs and frequency of support. Instead, they felt capacity was better determined by the number of support sessions a practitioner could manage on any given day. This was suggested to be three to four support sessions. However, this was seen by staff as a guide rather than an absolute, given that this could differ from day to day, and people may need longer support sessions (e.g. those lasting over an hour). For support sessions that were particularly emotionally challenging, practitioners need more time to write notes or might need a debrief after a difficult session. Furthermore, other components to practitioners’ roles influence capacity, such as training, research, attending events and other activities to raise awareness of the service and develop referral pathways.
4.5 Staffing, training, and support
The staffing structure in each delivery area is slightly different. In Ayrshire and Arran, the service comprises a service lead, a service manager, an assistant manager and three full-time practitioners who support those accessing the service. The assistant manager also has a caseload of people that they support. In Highland, the service is staffed by a service lead, a manager and five part-time practitioners.
Throughout the pilot, the service has experienced staff turnover at practitioner level in both areas and at manager level in Ayrshire and Arran. Service staff in Ayrshire and Arran acknowledged that their original service manager's departure came at a time when data collection processes were not yet fully embedded, which, in turn, led to a lack of consistency in approach. Changes in practitioner staff led to some pinch points in capacity, but staff reported these were manageable in the short term.
Changes in practitioner staff also meant that people being supported had to be reallocated to another practitioner. Service staff reported this was managed well, with most affected responding positively and remaining engaged with the service. This was echoed in feedback from people supported by the service who reported that they had quickly developed a positive relationship with their new practitioner. Service staff reported that a small number of those re-allocated to a new practitioner did disengage from the service but felt they were ready to do that anyway.
Initial training and ongoing development
Practitioner staff undertake initial training of four to eight weeks when they enter the post. Staff have consistently described it as comprehensive and that it equips them for their role. Some staff members that have previously worked in other related or similar roles reported that the training content was similar to previous roles, but they still appreciated the refresher it provided.
Staff commonly reported that while the initial training equipped them with the needed skills, they were still nervous and apprehensive before delivering their first support session. Staff that joined the service following staff changes reported that they benefitted from drawing on their colleagues’ experiences, which made it less daunting as they had a good idea of what they could expect. Service leads and managers explained, however, that it can be challenging to access and organise the full suite of initial training for individual staff members timeously. Some aspects of training require a minimum number of attendees before it can be delivered, and there can be delays in accessing it for new staff. Service managers and leads also acknowledged the need to define the minimum training required before a practitioner could start the role, informed through the learning they have gained.
Service staff described an environment that encouraged and supported ongoing learning and development and said they value this, as they often face new situations requiring further knowledge, awareness or skills.
Ayrshire and Arran is a pilot site for the Significant Adverse Event Review (SAER). SAERs take place following events that have resulted in unexpected death or harm and it focuses on analysing factors that have contributed to the circumstances of the event. The service has identified this as an area where they would like to develop practitioner knowledge. Staff have been supporting people involved in these reviews following their bereavement and having a better understanding of the process and what is involved will enhance the support they can provide during that time.
Supporting practitioner staff
Throughout this evaluation, practitioners have consistently reported that there are mechanisms in place to ensure they have the support they need when it is required.
“What I've found with this organisation, if I'm comparing it to any previous organisations, roles, is this organisation has given me time to process my thoughts and process my work and reflect on that in between clients. With this project it's exceeded my expectations, and the level of support that I've had has been phenomenal.”
There are several formal support structures in place for practitioners, including:
- Supervision sessions (every four to six weeks with a manager).
- Morning meetings.
- De-briefs (with managers, service leads, or another practitioner).
- Daily check-ins (peer-to-peer and across areas if necessary).
- Reflective practice sessions.
Over and above the more formalised support mechanisms, peer support within and across the service areas is highly valued by staff and seen as essential. Service staff recognise and acknowledge the emotionally demanding nature of their job and the importance of having these different support structures in place.
“I don't think we could do the role that we are doing if there wasn't a kind of open-door policy. You know, if you've had a really bad call, phone me, talk to me, you know, and it's just being able to offload that information. And I think we're quite a small team, but with the Highland team as well, you know, we could phone them, and that wouldn't be a problem, you know. We try once or twice a week to meet in the morning or an afternoon and kind of talk over our cases and things, but I really think being able to talk about what our day has looked like is so important. And because there are really horrific things that we have to hear about, and quite graphic detail, and not, being able to talk that through and leave it at work, it’s so important.”
Although staff reported feeling well supported in their roles, during the most recent fieldwork, two practitioners reported being reluctant to take annual leave, particularly when working with someone requiring more intensive support. Mechanisms are in place to ensure that other practitioners can provide support when someone’s usual practitioner is off during periods of leave or absence. However, if it is felt inadequate in specific circumstances, ways of supplementing this should be explored.
4.6 Referral pathways and awareness of the service
When the service launched in August 2021, self-referral and referrals through Police Scotland were the only official pathways into the service. Towards the end of that year, work to increase awareness of the service and expand referral routes commenced. This involved identifying the likely touch points that someone bereaved by suicide is likely to have with different organisations and services (e.g. GPs, mental health teams, funeral directors, and third-sector organisations). Work to expand referral pathways has remained a consistent and growing activity of all staff in the service since then, involving:
- Distributing information.
- Email contact.
- Discussions with other organisations.
- Attending other organisations' team meetings.
- Attending stakeholder meetings (e.g. local Suicide Prevention Steering Groups, Choose Life groups).
- Working with other stakeholders involved in suicide prevention activity (e.g. Choose Life co-ordinators).
- Attending networking events and open days.
- Visiting organisations to leave leaflets and talk about the service.
The work by services to raise awareness and expand the referral pathways resulted in an increased variety of referral sources but did not change the average number of people entering the service from month to month. At the same time as the service expanded the diversity of referral sources, there was also a noticeable reduction in referrals from Police Scotland. Of the total referrals made into the service by Police Scotland to date, 71% were received in the first eight months in Ayrshire and Arran (10 out of 14) and 79% over the same period in Highland (26 out of 33). Against the backdrop of staff changes in Police Scotland, service managers and leads have been working with their contacts to understand why and what is required to rectify the situation.
“One thing we're exploring at the moment is our relationship with police because that was one of our main referral routes in prior to August last year. And we haven't had any referrals in from them since then. They're currently doing a review, a suicide review, in terms of the number of suicides that they've had in the area and they're feeding back to me on that… we'll try and get some clarity as to why that's tailed off, and what we can do, and then we can work on how to build it up again.”
Some service staff reported a spike in referrals following awareness-raising activity but saw it reduce again. They highlighted the importance of continually building awareness of the service, so it becomes embedded in referrer’s minds.
Experience and perspectives of referral organisations
Feedback from organisations that have referred people to the service has been wholly positive. The service is perceived to fill an important gap. While most of the organisations were aware of other services that could provide people with emotional support, they reported that the SBSS was the only one specifically designed to meet the needs of people affected by suicide. Organisations appreciated being able to offer a referral to the service as an option to the people they are supporting.
“It's been very worthwhile for us … in our job being able to signpost people and refer people on to something like this, it’s just massive, so important.”
From the perspective of referring organisations, the following strengths of the model were highlighted:
- No waiting list and fast access (e.g. simple and quick referral process).
- Excellent communication from service staff with referrers, letting them know that a referral has been received and when contact has been made with the person they referred.
- The service can provide longer-term support and provides emotional and practical support.
A few organisations described a need to raise awareness of the service. They commented that after finding out about the service, they had seen no other materials, literature or presence. One GP explained that before their discussion with the evaluation team, they had asked their colleagues about their own experiences of referring to the service so that they could share some wider views. However, most of their colleagues were unaware of the service even though they would have received the same materials. This further highlights the need to continually revisit and maintain momentum around awareness-raising activity and connections with other services.
Only one organisation reported experiencing challenges in offering a referral to someone bereaved by suicide. Police Scotland staff in the evaluation highlighted that due to their very early engagement with the bereaved, it was often not appropriate or possible to discuss a referral. In these instances, the officers attending leave an information pack that contains details about the service and how to contact them. We know from some people that they revisit this information, but it can be many weeks later.
A small number of referral organisations also explained that they had experiences of people declining the offer of a referral, even where they had expressed needs related to bereavement by suicide. In those instances, the individuals did not think the service was what they needed or wanted.
“One of them was a person that had quite a chaotic lifestyle and she was involved with the community mental health team and the addictions team. I'd mentioned that and she just said that it wasn't the right time she was wasn't in the headspace to engage in anything like that.”
A few organisations reported ongoing contact with the person they had referred to the service. In all instances, they had received positive feedback and reported that they would not hesitate to make future referrals.
“I have spoken with a few of the people [we referred], that kind of came back at a later point. And they have mentioned what a good service it is and how well supported they felt. So it's not just one or two, it seems to be kind of across the board. Anybody that's kind of accessed it, it's favourable, and said good things about the service. So that's important.”
Onward referral pathways
SBSS staff report that, as appropriate and necessary, they speak to the people they support about different, additional support and external services available to meet their needs. They reported that there was a strong collective awareness and understanding of the different support and services available to meet a range of different needs across the team. There were no specific gaps in external service provision highlighted by SBSS staff. However, waiting times to access some services – such as counselling, CBT and similar therapies – did create barriers to access.
Feedback from SBSS staff suggests that people often prefer to receive details about different external support options and then decide if and when they might seek to access it. When people supported by the SBSS would like a referral or help to contact and engage with another service, practitioners will do this. Examples of referrals made to other organisations include the bereavement charity CRUSE, the Distress Brief Intervention Service and The Lennox Partnerships, a social enterprise which supports people to access employment.
The evaluation has engaged with three organisations that received referrals from the SBSS. Two offer group-based peer support to people bereaved by suicide, one of which also provides other social activities such as arts and crafts. The third organisation provides employment support. All three organisations reported that the referrals they had received from the service were appropriate in terms of the support they provide, and the needs of the person being referred. The two organisations that provided peer support to people bereaved by suicide welcomed the addition of the SBSS in their areas, feeling that there was no duplication of service and that each service offered something different. They acknowledged that different forms of support were required by people bereaved by suicide. Neither had any concerns that referrals from the service would impact their service delivery or capacity.
Contact
Email: socialresearch@gov.scot