Doctors' and Dentists' Remuneration - 2026-2027 pay round: written evidence
The Scottish Government's remit letter and written evidence document for the 2025 to 2026 pay round, submitted to the Doctors' and Dentists' Remuneration (DDRB) review body for their consideration.
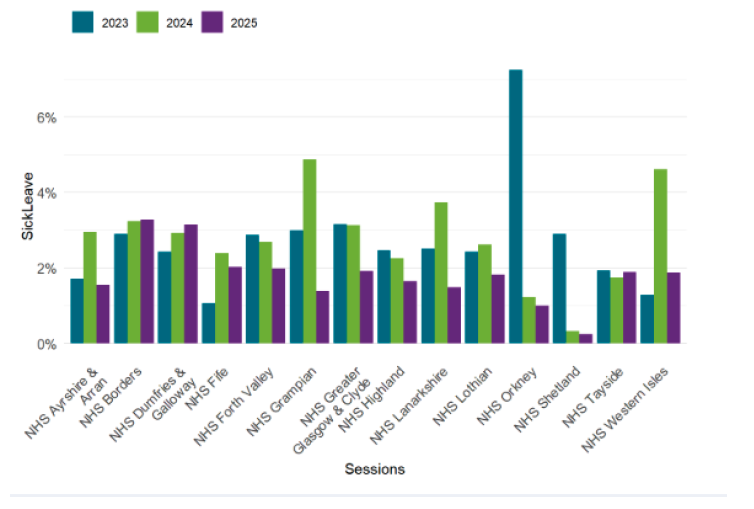
2. Estimated Absent GP Sessions by Reason (April 2023 - March 2025)
| Leave Type | 2023 | 2024 | 2025 |
|---|---|---|---|
| Sick leave | 2.6% | 3.0% | 1.8% |
| Maternity and Paternity leave | 2.6% | 3.4% | 1.9% |
| Parental leave | 0.0% | 0.1% | 0.0% |
| Special leave | 0.2% | 0.2% | 0.1% |
Recruitment and Retention
116. Between 2008 and 2017 the headcount of GPs remained roughly constant at around 4900. In 2017, Scottish Government committed to increasing numbers by at least 800 over the next ten years.
117. Since this time, we have delivered an additional 526 GPs and as of 30 September 2025, GP headcount in Scotland was 5,423. This is an increase of 171 GPs compared to the same period in 2024. GP Whole Time Equivalent has also also increased from 3,520 in 2017 to 3,591 in 2025.
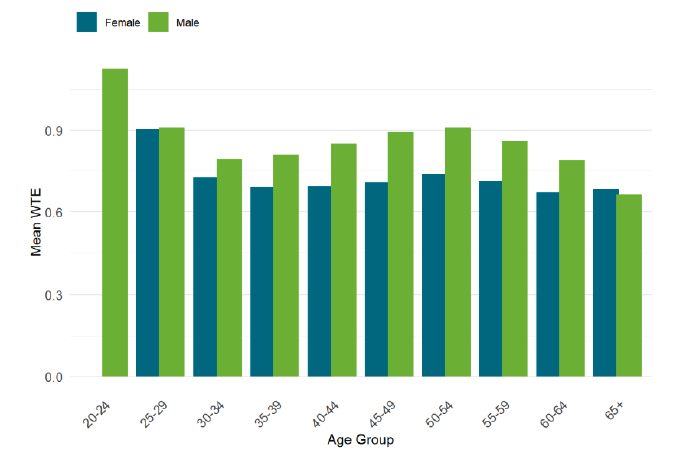
118. As of March 2025, there were more female GPs than male in every age group under 60 and the mean WTE was greater for males in every age group under 65.[17].
119. In November 2024 we published the GP Recruitment and Retention Plan. This sets out 20 measures to improve the GP training pipeline and career pathway to recruit and retain GPs in general practice.
120. This includes a focus on early career GPs where we have established a National Framework for Early Career GP Fellowships and used this to underpin an investment of £600k to 7 Health Boards this year, to establish approximately 25 new fellowship posts before the end of this financial year. NHS Education for Scotland also offer rural and health inequalities fellowships to support GPs to develop the right skills and experience to work in island and rural settings as well as areas of deprivation and bridge the gap between training and joining the workforce. We also offer enhance support for GPs in the first 5 years of practice through access to the Practice Based Small Group Learning scheme provided NHS National Education Scotland.
121. We have increased our investment in GP coaching to support GPs to navigate particular management and career related challenges. Funding for 73 additional coaching places, has been provided this year to meet rising demand and enhance support for GPs, offering a total of 175 places. We continue to work with NHS Education for Scotland (NES) to ensure that we meet the need for this support within the profession.
122. NES have reviewed and improve the GP Retainer scheme by combining the Staying Practice and Retainer Schemes into a single programme of support for GPs at risk of leaving the profession. The scheme was launched in August 2025 and offers flexible working, mentoring, and CPD support.
123. Seniority Payments for Scottish GPs are set out in chapter 10 of the annual Statement of Financial Entitlements (SFE)[18]. Seniority Payments reward experience, based on years of reckonable service adjusted for superannuable income factors. Seniority Payments are made to the practice for payment to individual GPs.
124. Presently a GP has to work for six years before any seniority payment is made; for 6 years to achieve a payment of £600 per annum, for 21 years to achieve a payment of £5,129 per annum, for 36 years to achieve £10,258 per annum, with the maximum of £13,900 per annum payable being made at the 47-year point[19]. The contractor has to have been in an eligible post for more than 2 years in order to be able to apply.
125. The annual cost for seniority payments to GPs was £15.9 million in 2024/25.
Rural
126. The Centre for Workforce Supply and the National Centre for Remote and Rural Health and Care, commissioned by the Scottish Government are developing a sustained model of direct support that will provide rural and island health and social care employers with the help they need to improve recruitment success.
127. This long-term, connective, and dynamic model of support will enable the whole-system approach which is needed to provide employers with the help they need to overcome recruitment challenges.
CWS
128. To support workforce capacity across NHS Scotland and ensure it has the right people, in the right place at the right time, we commissioned NHS Education for Scotland to establish the Centre for Workforce Supply (CWS) in November 2021.
129. The CWS undertakes a series of workforce recruitment, retention and diversification learning sessions for NHS Scotland Boards and Primary Care teams, including sessions on GP retention and rural and island medicine.
130. The CWS will continue to work collaboratively to support the implementation of workforce initiatives which help tackle priority supply challenges.
Salaried GPs
131. The General Practice Workforce Survey Scotland 2025 estimated that 67% of GPs were Independent Contractors[20]. It estimated that there were around 1466 salaried GPs (32%) and 56 GP retainees (1%).
132. The survey also found that Performer GPs, had the highest average WTE.
| Year | Designation Group | Headcount | WTE | Mean WTE |
|---|---|---|---|---|
| 2025 | Performer | 3,079 | 2,532.5 | 0.82 |
| 2025 | Performer Salaried | 1,466 | 1,029.3 | 0.70 |
| 2025 | Performer Retainee | 56 | 29.6 | 0.53 |
| 2025 | All GPs | 4,582 | 3,591.5 | 0.78 |
1. Doctors may have more than one designation, so the national headcount may not equal the sum of the designation totals.
GP Expenses
133. Data on GP income and expenses data is provided annually by NHS Digital on behalf of the four countries, and which, for the tax year 2023/24, was published on 28 August 2025. We invite DDRB to consider this report in its entirety, but for the purposes of independent contractor GPs in Scotland the report showed that:
134. The average taxable income for contractor GPs in General Medical Services in the UK was £158,700 in 2023/24. In Scotland, the average taxable income for contractor GPs was £128,300.
135. Work to deliver direct reimbursement of some non-staff practice expenses is underway. In April 2025 the Scottish Government undertook an evidence gathering exercise with all practices on an agreed list of soft and hard facilities management expenses to better understand practice running costs. These data are informing plans to introduce direct reimbursement for an agreed set of non-staff expenses in phases over the years 26/27, 27/28 and 28/29. Funding of £40m (recurring) will be allocated to deliver this.
| Contract Type | Year | Report Population | Gross Earnings | Total Expenses | Income Before Tax | Expenses to Earnings Ratio |
|---|---|---|---|---|---|---|
| GPMS | 2022/23 | 3150 | £276,600 | £156,700 | £120,000 | 56.6% |
| GPMS | 2023/24 | 3900 | £258,400 | £141,300 | £111,900 | 54.7% |
| GPMS | Change | +750 | -6.6% | -9.8% | -6.7% | -1.9 Percentage Points |
| GMS | 2022/23 | 2800 | £272,200 | £152,900 | £119,200 | 56.2% |
| GMS | 2023/24 | 3450 | £257,600 | £140,300 | £111,900 | 54.5% |
| GMS | Change | +650 | -5.3% | -8.2% | -6.1% | -1.7 Percentage Points |
| PMS | 2022/23 | 350 | £312,200 | £186,400 | £125,800 | 59.7% |
| PMS | 2023/24 | 450 | £265,500 | £149,300 | £116,200 | 56.2% |
| PMS | Change | +100 | -14.9% | -19.9% | -7.6% | -3.5 Percentage Points |
Workforce Data for Scotland
136. The General Practice Workforce Survey Scotland 2025 captures aggregate workforce information from Scottish general practices and each of the NHS Board-run GP Out of Hours services. It provides the most comprehensive information available on the staffing cohort of general practice, both in hours and out of hours, but does not provide the cost. The costs of running a practice are a matter for the GP partners, including what pay they award employees. The 2025 survey was published on 26 August 2025.
137. The 2025 results for Scottish general practices are based on survey data received from 669 responding practices. The response to the survey was less than 100% and appropriate weighting has been applied to statistics calculated from the survey data to provide representative estimates at NHS Board and national levels. Statistics including headcounts, WTE, numbers of contracted hours and sessions, and numbers of vacancies are therefore survey-based, weighted estimates.
138. For this year’s survey NHS Education for Scotland have also addressed missing data using data imputation methods. Missing data on contracted and vacant hours, contracted GP sessions, and staff age have been imputed using a donor-based imputation that relies only on this year’s survey sample data for replacement values and preserves existing relationships and distributions present in the sample data. These methods help to provide a more complete data set for analysis.
The results include information on: -
- Estimated WTE numbers of GPs in post in Scottish general practices, along with information on patterns of sessional commitment by age and gender (a GP's week is typically defined in terms of sessions rather than hours, with a working day generally being comprised of two or sometimes three sessions).
- Estimated headcount and WTE numbers of nurse practitioners and other registered nurses employed by Scottish general practices, along with information on the age profile of these staff.
- Use of locum GP time and extra nurse time by Scottish general practices.
- Known vacancies for these professional groups in general practices from April 2022 to March 2023.
139. The 2018 GP Contract mandates the provision of workforce data to be made mandatory. This enables us to understand staffing levels across practices in Scotland and will inform projections around future staffing need to meet local population health need.
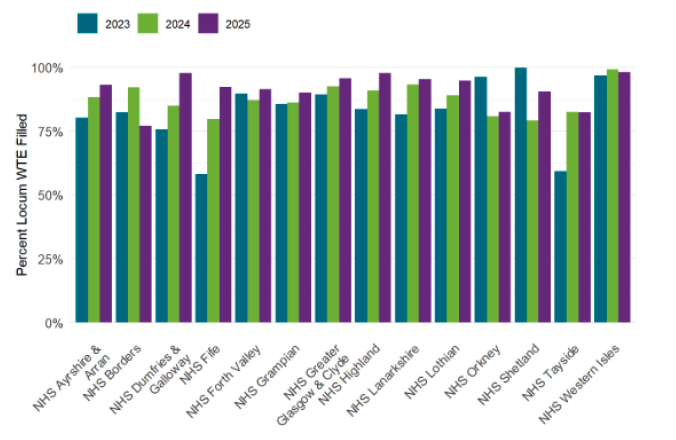
| Health Board | Practices using locums | WTE locums required | WTE locums filled | Percent Locum Filled |
|---|---|---|---|---|
| NHS Ayrshire & Arran | 73.0% | 11.8 | 11.0 | 93.0% |
| NHS Borders | 88.9% | 6.5 | 5.0 | 77.0% |
| NHS Dumfries & Galloway | 75.0% | 5.7 | 5.6 | 97.7% |
| NHS Fife | 82.5% | 22.9 | 21.2 | 92.3% |
| NHS Forth Valley | 69.7% | 11.2 | 10.3 | 91.5% |
| NHS Grampian | 89.1% | 20.2 | 18.2 | 90.2% |
| NHS Greater Glasgow & Clyde | 84.2% | 67.1 | 64.2 | 95.7% |
| NHS Highland | 75.6% | 22.2 | 21.6 | 97.7% |
| NHS Lanarkshire | 78.3% | 46.5 | 44.4 | 95.4% |
| NHS Lothian | 90.8% | 41.3 | 39.1 | 94.7% |
| NHS Orkney | 100.0% | 1.5 | 1.2 | 82.5% |
| NHS Shetland | 100.0% | 5.0 | 4.5 | 90.5% |
| NHS Tayside | 87.5% | 19.5 | 16.1 | 82.3% |
| NHS Western Isles | 100.0% | 2.7 | 2.7 | 98.0% |
| Scotland | 82.9% | 279.0 | 260.3 | 93.3% |
140. The 2018 GP Contract mandates the provision of workforce data to be made mandatory. This enables us to understand staffing levels across practices in Scotland and will inform projections around future staffing need to meet local population health need.
NHS Scotland Public Dental Service
141. The Public Dental Service (PDS) has been in operation in Scotland since 2013 and was formed in response to the 2006 Review of Primary Care Salaried Dental Services which recommended a single managed service in primary care. The PDS was therefore created by the merger of the previous Community and Salaried Dental Services.
Statutory basis
142. The legal underpinning of the PDS is Section 36 of the National Health Service (Scotland) Act 1978 (“the Act”), ensuring delivery of NHS dental services where General Dental Services (as enacted in Section 25) have either:
- Not secured adequate provision of services, such as in rural and/or island areas; or
- Not ensured that sections of the population – such as those with special and/or complex care needs – are receiving satisfactory treatment.
Underpinning principles and function
143. PDS is managed and delivered directly by NHS Territorial Boards and must have due regard to its local population and the following factors which must be balanced in service delivery:
- Complementarity with General Dental Services (GDS). Independent contracting services providing GDS continue to be Scottish Government’s preferred vehicle for the delivery of primary dental care. While there is recognition that independent contractor services are not always viable in all parts of Scotland, Scottish Government has invested in service reform (implemented November 2023) which is intended to the reinvigorate the GDS offer. In addition, the March 2025 NHS Operational Improvement Plan commits to revision of available allowances to better support rural and island areas of Scotland where access to GDS may be more variable. Where gaps do exist in provision, routine dental care should be provided to the population by PDS until such a time as rebalancing of care between the services can be achieved.
- Sustainability. It is incumbent on Boards to ensure both service and financial sustainability of the PDS, and this may involve cross-boundary working with neighbouring Boards to support economies of scale.
- Equity. NHS Boards are required to ensure that NHS dental service are available to all who wish to access them in their local area. As set out in the legal underpinning, this includes vulnerable groups who – due to complexity of care required – may not be able to access GDS.
- Compliance. PDS is required to comply with all relevant legislation and regulations.
144. The role of PDS was set out in the 2006 Review and sets out the following tenets which the PDS continues to uphold:
- Provision of a full range of NHS dental treatment to adult and child patients with special care needs;
- Referral and signposting to other heath and social care practitioners, as required;
- Ensuring equity of access for socially excluded and vulnerable groups who may be unable to access GDS;
- Provision of specialised and specialist services including special care dentistry, paediatric dentistry, sedation and general anaesthesia;
- Universal access services where there are known gaps in GDS provision, and facilitation of out-of-hours services; and
- Teaching and research, including supporting undergraduate outreach services and dental core training.
145. The PDS also fulfils a dental public health function as it delivers dental inspection services to education establishments under the auspices of the National Dental Inspection Programme (NDIP), which reports on the oral health of Primary 1 and 7 children at both the local and national level, and is also responsible for health promotion and an element of Childsmile delivery. Childsmile is a national oral health improvement programme which delivers universal and targeted interventions to children to support population oral health and reduce health inequalities driven by socioeconomic deprivation.
146. Core funding for the PDS has been baselined to NHS Boards from the Directorate of Primary Care since 2024/25, while annual pay uplifts are provided through in-year allocation in the usual way. In addition, the Outcomes Framework bundle previously provided annually to Boards via the Directorate of Health Finance was also baselined in 2024/25. This funding covers Childsmile activities and a range of other service outcomes. Finally, the PDS receives funding from NHS Education for Scotland (NES) who support outreach services in partnership with the three Universities supporting Bachelor of Dental Surgery education.
Workforce
147. Each frontline NHS Board has a Director of Dentistry who is responsible for oversight of both GDS and PDS functionality in their area. Scottish Government meets regularly with the Directors as a network to understand challenges and issues across NHS dental services.
148. Workforce statistics for NHS Scotland are regularly published by NES and headcount over the past five years for the PDS is set out below (showing data at 31 March and 30 September).
| Year | 31 March | 30 September |
|---|---|---|
| 2025 | 340 | n/a |
| 2024 | 336 | 334 |
| 2023 | 363 | 334 |
| 2022 | 375 | 365 |
| 2021 | 359 | 375 |
| 2020 | 369 | 367 |
149. NES also publishes a biennial report on the NHS dental workforce specifically, with the last publication on 28 October 2024. This provides detail on inflow, outflow, and stock of dentists however data is broken down by GDS/PDS and Hospital dental services such that PDS cannot be separately identified. The information can be accessed at Dental Workforce Report 2024.
General Dental Practitioners (GDPs) and Dental Bodies Corporate providing NHS General Dental Services in Scotland
NHS Dental Services – Independent Contractor Sector
150. The reforms made by Scottish Government to payments for NHS General Dental Services have been in operation since 1 November 2023. The broad position is that these changes have supported the sector significantly to deliver high volumes of care and treatment to NHS patients across Scotland. There are local challenges across certain remote and rural locations, where challenging workforce and wider economic factors have disproportionate impact on service delivery.
151. The intention of the payment reform was to improve the underlying Item of Service fee structure, as being crucial to the delivery of NHS dental care and treatment – simply fees drive activity within the sector. The reform uplifted the value of fees available on average by around 20 to 25 per-cent bringing these in line with market rates and supporting practice profitability. On introduction the revised fees were further enhanced by Ministers acceptance of the 6% pay award for 2023/24.
152. In the context of pay the Scottish Government has accepted DDRB pay recommendations for dentistry since introduction of reform, maintaining the value of fees relative to the inflation position across the wider economy. Uplifts are generally applied to fee per item and capitation elements of the pay package, which feeds into the expenses side through the earnings link between fees and the General Dental Practice Allowance (GDPA), which is capped.
153. Scottish Government is presently focused on building on the payment reform to maintain and grow the NHS dental sector through a range of measures. This work is supported by Ministers maintaining the position to apply the DDRB 4% recommendation for 2025/26, building on a sector that has delivered 4.2 million courses of treatment in the previous financial year, and over 7 million claims from 1 November 2023 to end July 2025.
154. Scottish Government remains committed to undertake bilateral dialogue with BDA (Scotland) in respect of the expense’s element of the overall pay package. However, Scottish Government has moved in the current pay uplift to introduce an uplift of 4% to the GDPA cap which will allow practices at the cap additional funding. It will be of value to Ministers if the DDRB were to offer a view on the metrics and elements across the wider payment system it would consider within the scope of bi-lateral discussions on these matters between BDA (Scotland) and Scottish Government.
Funding and Expenses
155. The overall level of funding provided for NHS dental services in the 2025/26 Budget reinforces Scottish Government’s commitment with an increase of almost 15%. This funding is for primary care dental services and takes total funding to over half a billion pounds for the first time.
156. Scottish Government must act within a budgetary envelope, and this can be impacted by external economic factors about which it cannot control. Recent DDRB reports have identified inflationary pressures and general labour market conditions, including impacts of EU withdrawal and cost of living as having a bearing on dental provision and ability to attract dentists in certain often rural and island areas. The application of pay award is applied to all independent contractor dentists across Scotland.
157. The matter of recognition of NHS dental expenses remains an area of contention between BDA (Scotland) and Scottish Ministers and it is recognised that this requires attention. In recent years Scottish Government committed in 2023/24 pay negotiations to a working group on expenses with BDA Scotland and an initial discussion has taken place. At present further bi-lateral engagement is not planned, however, the commitment was re-affirmed in last year’s evidence that expenses is a focus moving forward.
158. It should be noted that the overall financial position remains challenging with the additional context of a Scottish Parliamentary election due in May 2026. Scottish Government considers it essential that a common understanding with BDA (Scotland) is a necessary pre-requisite for discussions around expenses. This could be helpfully supported by an indication from DDRB around what it considers would be in the scope of expenses across the range of payments being made. Scottish Government is mindful of the wider economic and fiscal landscape that remains challenging.
Programme
159. At present Scottish Government is engaged on the delivery of a wide programme of work that builds on the core proposition put forward to the sector under the payment reform, which remains the basis for dental policy in Scotland. The Scotland-wide position to provide the basis for the maintenance of sustainable NHS dental services set in the reform allows government to necessarily focus attention on improving governance arrangements, supporting access in challenging areas and delivering Oral Health Improvement programmes in the community.
160. The ambition of Scottish Government in maintaining service provision is to expand that where services are limited. The Assurance and Workforce space highlights the work being done to ensure that NHS dental services in Scotland are able to deliver modern dentistry for all NHS dental patients.
Assurance
Secondary Legislation
161. It is the intention of Scottish Ministers to lay secondary legislation to make amendments to the National Health Service (General Dental Services) (Scotland) Regulations 2010 ‘the regulations’ relating to mandatory training and prior approval. Amendments are likely to come into force in early 2026.
Mandatory Training
162. Workforce and patient access remain key priorities for Scottish Government. Representation from Health Boards, particularly from those with rural communities, suggests that in some circumstances the present mandatory training (MT) arrangements can discourage dentists from applying to join a dental list where there is a need to wait for several months to undertake MT. Ministers would like to enable a dentist to be added to a dental list on a provisional basis for a 6 month period in order for them to complete both the MT course and pass the test of knowledge.
Prior Approval
163. Ministers also intend to make certain changes to elements of prior approval (PA) in general dentistry (excluding orthodontics) to allow for a new requirement for approval based on clinical criteria. The intention is that this new basis for approval will replace the current arrangements where prior approval is required for those courses of treatment that exceed, or are likely to exceed, an amount set out in the Statement of Dental Remuneration (SDR) (currently £600). The intention is to introduce provisions to enable PA to operate in a way that supports clinical assurance.
164. The changes will require amendment to the regulations, but we anticipate that the detailing of the clinical criteria will be included in the SDR. This will support the development of an appropriate clinical framework that can be more easily updated as clinical considerations evolve without further changes to the regulations. We have been working with Practitioner Services on a clinical model of PA and would like to share the substance of these proposals with a view to seeking BDA’s comments in the first instance.
Terms of Service
165. It is our intention to take steps to ensure that the terms of service of dentists and dental bodies corporate have improved visibility with the profession. This is partly in response to a number of reports that suggest certain contractors and dental bodies corporate are not meeting their terms of service. It seems reasonable given the long history of this situation, during and in the aftermath of the pandemic, that a general communication from Scottish Government is appropriate. The intention is to issue a PCA to the sector around October-time this year. The PCA will reference key considerations for contractors and enclose terms of service guidance.
Declaration of Compliance
166. We are also beginning to explore the idea of introducing some form of declaration of compliance (DoC), which we first mooted in the recent LDC Conference, under which dentists and dental bodies corporate could be required to self-declare that they are meeting their terms of service obligations. Ostensibly this would aim to provide assurance to the NHS Board that dentists in their areas are meeting their terms of service. Again, as we move through the various development stages, we would like to have several bilaterals at key stages.
Workforce
167. Following the significant disruption to the dental workforce caused by the Covid-19 pandemic, the NHS Scotland Operational Improvement Plan, published in March 2025, sets out a package of actions to seek to improve the sustainability of the NHS dental workforce, supported by new funding in 2025/26. This includes a 7% increase in domestic student dentist numbers from September 2025 – the first regular increase in student numbers in ten years – to ensure an expanded pipeline of new dentists entering the workforce from 2029. We are also working with NHS Education for Scotland to develop an innovative training package for General Dental Council (GDC) registered dental therapists – who have qualified overseas – to articulate to full dentist registration status. This will allow them to establish their own practices, if they wish, as well as to deliver care directly to patients in existing practices.
168. Following payment reform in 2023, we have seen that the number of high street dentists working in Scotland has increased by almost 5% from March 2024 to March 2025, according to recent NHS Education for Scotland statistics. However, we are aware that localised challenges remain in the workforce, particularly in rural areas such as Dumfries and Galloway, the Highlands, as well as in island areas. We are therefore also working with NHS Boards to refine the financial incentives in place to support dentists moving to work in rural areas, supporting sustainable access across Scotland.
169. NES also publishes a biennial report on the NHS dental workforce specifically, with the last publication on 28 October 2024. This provides detail on inflow, outflow, and stock of dentists however data is broken down by GDS/PDS and Hospital dental services such that PDS cannot be separately identified.
Oral Health Improvement
170. Oral health improvement recognises that improvements in patient oral health is the ultimate goal. Scottish Government’s flagship Childsmile programme offers every child attending nursery in Scotland free daily supervised tooth brushing, and fluoride varnish application to those in our most deprived communities. Official statistics from October 2024 show that the difference in the percentage of P1 children with no obvious decay in the most and least deprived areas has decreased from 32.2 percentage points in 2010 to 23.5 percentage points in 2024. This is the lowest recorded gap and shows the success of the programme.
171. As part of payment reform, we have also introduced oral health metrics for the adult population. This will be done in the background as part of the claims process, enabling over time the assemblance of oral health data that in turn will inform the policy interventions of the future.
Summary
172. In conclusion, NHS dental payment reform has embedded well across the sector, with local challenges to be overcome. The core policy to maintain services and grow access to provision is being delivered through a range of policy interventions. As described above the strategic focus of the Scottish Government going forward is to maintain the positive engagement from the sector by ensuring that the comparative attractiveness of the new fees keeps pace with the cost to deliver care and treatment.
173. Scottish Government maintains a regular dialogue with BDA Scotland, however, in the absence of an agreed frame of reference on expenses this matter is likely to remain unresolved. The significant challenge facing the public finances must be seen as a major factor in connection with expenses, and with pay more generally.
174. The Scottish Government would like DDRB to provide its recommendation on pay to include an assessment of the dental expenses position in Scotland.
Consultants, Specialty Doctors and Associate Specialists (SAS) and Resident Doctors
Pay
175. Scottish Government accepted the recommendations from the DDRB report for 2025/26 for a 4% pay uplift for Consultants and SAS Doctors, this was implemented in pay circulars in July 2025. This means a Consultant at the top of the pay scale will now earn £148,064 and Specialty Doctors £99,974.
176. These pay uplifts go beyond the Scottish Public Sector Pay Metrics for this year and recognises the vital contribution our NHS Staff provide to the people of Scotland whilst ensuring equity and sustainability.
Consultants
177. The agreement reached with BMA Consultants from 2024/25 also included a commitment to undertake further work via task and finish groups under the Joint Negotiation Committee between Scottish Government, BMA Scotland, and NHS Employers. These groups will seek to conclude in 2025/26 which were tasked with:
- Taking forward discussions on the balance of different elements of the job plan for consultants to facilitate attractive employment opportunities within NHS Scotland and to enable retention of the existing workforce. This work has now concluded and a DL promoting the changes has issued to the service, this can be accessed here (insert link)
- Discussions to agree a national rate for internal short-term cover to improve continuity of care and help alleviate agency and locum spend within NHS Scotland.
Specialty Doctors and Associate Specialists (SAS)
178. The offer made to SAS doctors in 2024/25 also included the opportunity for SAS doctors to work with NHS Employers and Scottish Government on the following areas:
- The development of an agreed policy which would provide a mechanism to facilitate the potential regrading of Specialty Doctors to Specialist Doctors. A new policy has been agreed by all parties, and we are now working to finalise this.
- Discussions to agree a national rate for internal short-term cover.
179. We hope to conclude these areas of work by the end of 2025.
DDRB Reform
180. In the 2025/26 remit letter the Scottish Government gave full support to the agreed reforms to the DDRB process which formed part of the Department of Health and Social Care’s offer to Consultants in England for 2024–25. These reforms were successfully implemented by the DDRB.
181. The Scottish Government will continue to work with the DDRB on all aspects of reform and consider any further action that is presented in future reports.
Engagement
182. We continue to engage the medical profession on Terms and Conditions of Service issues via the Joint Negotiation Committee comprising of with MSG (NHS Scotland employers/Scottish Government) and BMA Scotland Consultants, Resident Doctors, and SAS committees.
183. This forum replaced the previous tripartite arrangements in late 2023, it considers the more strategic issues that impact on the terms and conditions of the medical professions and has been responsible for delivering the reform components of the agreed consultant pay deal from 2024/25 and those aspects which relate to the SAS doctor pay offer also from 2024/25.
Distinction Awards and Discretionary Points for Consultants
184. It remains the position in Scotland that no new Distinction Awards have been made as these do not align with progressive pay principles of the Scottish Government. There are Consultants who received awards priory to the freeze who are still in receipt. It remains the case that extant arrangements for DAs will remain in place.
185. Although DAs are frozen to new Consultants, the availability of new DPs increases in line with the number of consultants in post and we have recently uplift DP payments from £3204 to £3600 as part of the recent consultant pay agreement.
Summary and Recommendations
186. The Scottish Government remains committed in our support of the DDRB process and the independent recommendations that the pay review body sets. We are committed to delivering fair, equitable and affordable pay awards for NHS Scotland’s staff.
187. Accordingly, we are seeking recommendations from the DDRB for all medical and dental staff in NHS Scotland, with the exception of Resident Doctors and Resident Dentists. We remain committed to our agreement with Resident Doctors, and Resident Dentists in training and will therefore not be seeking a recommendation for these groups.
188. Additionally, as a result of the increase in DP rate, which ensures that Scotland continues to offer a competitive pay package for consultants, we are not seeking any recommendations from DDRB on distinction awards and discretionary points.
189. In considering recommendations the Scottish Government would ask that the DDRB pays cognisance to the path we have pursued in term of fairness, equity and affordability in respect of public sector pay deals, the expected trajectory of economy based on the relevant date available to the DDRB and our continued commitment to no compulsory redundancies and the broader reform and renewal activity that is underway across NHS Scotland.
2.1 I. Employee Experience, Morale, and Motivation Wellbeing
190. Health services continue to face immense pressures. Ensuring sustainable support that aligns with both current and emerging needs at national and local levels is essential. The Scottish Government remains actively engaged with stakeholders, sector leaders, and frontline staff to identify sources of stress and implement further initiatives to enhance staff wellbeing.
191. Alongside local support, we provide access to a range of national resources for staff wellbeing. These wellbeing services include self-service resources through the National Wellbeing Hub, access to psychological interventions and therapies. Registered staff can also receive confidential mental health support through the Workforce Specialist Service (WSS). These resources all have long-term funding which enables us to respond more effectively to the evolving needs of staff.
192. Additionally, all health staff have access to a 24/7 compassionate listening service via the National Wellbeing Helpline (delivered by NHS 24).
193. These interventions highlight the need for resources that extend beyond the capacity of a single employer and are delivered on a spend-to-save basis. The resources help staff to manage mental health challenges, facilitate a smooth return to work, and improve staff retention, ultimately enhancing patient safety and raising standards of care.
194. Scottish Government continue to invest £2.5 million annually to the national programmes, designed to support the wellbeing of the workforce, reinforcing our commitment to their welfare. However, with this funding already allocated to the existing wellbeing programmes, it leaves no capacity to undertake additional initiatives that would require centralised funding support.
195. We continue to support employers in promoting workforce wellbeing and fulfilling their duty of care. Recognising the vital role of staff in delivering healthcare, we remain committed to investing in sustainable national initiatives that strengthen wellbeing, workplace culture, and retention, supporting long-term recovery and service reform.
196. A set of facilitated reflective practice groups for GPs, funded by the Scottish Government, was launched in March 2025 running for 12 months.
197. The monthly online groups offer participating GPs a facilitated and confidential space to connect with peers, share experiences, and seek support for the challenges they encounter in their professional roles. Through reflective group work, GPs are supported not only in finding solutions but also in managing the wide-ranging demands of their work while creating opportunities for personal and professional growth.
198. A national resource for peer support and reflective practice has been developed with the aim of creating a self-sustaining model of support for staff and is now available on the National Wellbeing Hub.
199. Improving Wellbeing and Working Cultures (IWWC) was published in 2024. IWWC is about supporting good working cultures through national and local programmes of work that focus on the pillars of wellbeing, leadership and equality. It describes our vision and explains why activity in wellbeing, leadership and equalities is important for improving working culture. Work is ongoing to develop IWWC Case Studies which will provide illustrative examples of initiatives which are already making a difference and improving working cultures across the sectors. The purpose of these case studies is to connect, support and inspire individuals, teams and organisations by sharing examples which they may choose to adopt or adapt in their own workplace. An initial tranche of case studies have been posted to the Leading to Change Website, with more to follow in 2026.
200. We continue to work closely with those who can enable and support culture change, with a focus on prioritising compassionate and collaborative leadership, wellbeing, and equality, diversity, and inclusion across the health workforce.
201. Long-standing challenges remain around improving staff facilities, such as access to hot food and adequate rest spaces. These issues are particularly difficult to address due to budget constraints and because they fall within the responsibility of individual employers.
202. We remain committed to strengthening the provision of essential support for health and social care staff. Our scoping work has now concluded, and we have presented the findings to the Scottish Workforce and Staff Governance Group (SWAG) with the aim of establishing a dedicated subgroup on Health, Safety and Wellbeing. This subgroup is expected to be formed by Spring 2026.
Nursing and Midwifery Taskforce and other considerations
203. The Ministerial led Nursing Midwifery Taskforce (NMT) recommendations were published on 13th February 2025, these recommendations are designed to support Nurses and Midwives across Scotland considering 4 key areas – Attraction, Wellbeing, Education & Development, Culture & Leadership. Work is currently ongoing to implement the recommendations, and it has been agreed that these will be implemented for all staff where this is appropriate.
Health Workforce Equality
204. Fostering an inclusive culture and supporting individuals – both patients and staff – from all backgrounds is paramount in ensuring we deliver the best care for the people of Scotland.
205. We are working to improve equality, diversity, and inclusion across all professions in health. We have required all NHS Boards to develop anti-racism plans which are now in the process of development. To support this, work the Cabinet Secretary for Health and Social Care published a statement about anti-racism in August 2024 alongside guidance on how NHS Boards can develop meaningful and effective anti-racism plans. We have recently launched new anti-racism training materials for all staff and managers, produced by the Coalition for Racial Equality and Rights (CRER).
206. We have received drafts of the anti-racism plans from all Boards and are now in the process of providing feedback that will help Boards further implement and deliver support.
207. Also, following on from the Supreme Court decision on the definition of “woman” we are working through with legal colleagues to understand the implications of the decision on the practical application of this decision.
2.2 J. Conclusions and Recommendations
208. The remit letter to the DDRB from the Cabinet Secretary for Health and Social Care sets out that we are seeking recommendations for all medical and dental staff in NHS Scotland, for medical and dental contractors in primary care, but not for Resident Doctors or Resident Dentists.
209. You are aware the Scottish Government works within a fixed budget with many competing socio-economic demands on this. Despite this, we endeavour to invest, but we acknowledge however that the Health and Care system in Scotland needs reform to meet the challenges of the 21st Century and to cope with the demands of an increasingly ageing population in Scotland.
210. The Scottish Budget endeavours to balance the competing socio-economic demands we face and be clear that going forward, pay and workforce must, more than ever, be explicitly linked to both fiscal sustainability and to reform, in order to secure the delivery of effective public services over the medium term and ensure Scottish Government are committed to delivering fair, equitable and affordable pay awards for NHS Scotland’s staff.
211. We invite you to consider this evidence and make recommendations for the year from 1 April 2026 to 31 March 2027.
2.3 ANNEX A
2.4 Postgraduate – Foundation Training
A two-year Foundation Programme is the first stage of postgraduate medical training in the UK following graduation from medical school. Recruitment to the two-year programmes in the Scottish Foundation School is undertaken as part of the UK-wide recruitment process to a national UK agreed timetable.
The Scottish Foundation School is one of the largest in the UK, providing a wide range of programmes and offering a unique experience, covering different types of populations, teaching hospitals, remote and rural practice, and specialties as well as geographical diversity.
The Scottish Government has funded increases to Foundation Training places to match the output of our increased investment in Scottish Medical School places.
Number of Foundation Year 1 posts in Scotland by region, as at August 2025.
| East | North | South-East | West | TOTAL |
|---|---|---|---|---|
| 114 | 189 | 258 | 540 | 1101 |
Source: Foundation Training in Scotland | Scottish Medical Training
Foundation Programme preferencing data for Scotland for the past three recruitment years is shown below:
|
UKFP Year |
Number of programmes | First choice preference | First choice ratio | First preference ratio after pre-allocation / manual matching |
|---|---|---|---|---|
| 2025 | 1109 | 1117 | 1.01 | 1.01 |
| 2024 | 934 | 933 | 1.00 | 1.00 |
| 2023 | 879 | 831 | 0.95 | 0.94 |
Source: First preference ratios - UK Foundation Programme
Note: This data is based on the number of Foundation Programme (FP) places at the time of the national allocation to foundation schools and the number of applicants remaining in the process at that point in time. FPP programmes, and the applicants who accepted FPP offers, are not included. Applicants who withdrew prior to allocation are also not included.
Postgraduate – Specialty Training
Annual review of specialty training establishments
The medical education and training pipeline aims to ensure that there are a sufficient number of trainees coming through the system/pipeline to deliver and sustain a medical workforce with the right skills for the future while meeting patient and service need in the present. Planning for the future medical workforce is complex as we need to make assumptions about population needs, future service delivery models, training capacity, workforce demographics, global mobility of the medical workforce, individual working and training patterns and geographic preferences.
The Scottish Government undertakes annual reviews of the number of specialty training places needed in order to meet anticipated future service demand and consultant need and has funded the creation of hundreds of additional specialty training places in Scotland across multiple different specialties since 2014, including 47 new specialty training places added in 2025. These specialty training places have been created in response to recommendations made by the Scottish Shape of Training Transitions Group (SSoTTG) which includes NHS Education for Scotland (NES), the British Medical Association, the Academy of Medical Royal Colleges, and various Health Board representatives including regional workforce planners.
Specialty training recruitment
The latest fill rates will be published w/c 1 September. This section will be updated then.
Noting a number of stakeholder concerns around UK doctors struggling to obtain specialty training places in recent recruitment rounds due to increasing competition ratios, the Scottish Government will work with NES to provide greater transparency on recruitment data including competition ratios, existing training vacancies and the location of training posts to resident doctors in Scotland. This will enable them to take better informed choices and gain greater personal agency over their careers.
We note that entry to specialty training is through a competitive application process, and it is not always possible to secure a specialty training place of an individual’s choice in the location of their choice as planning takes account of workforce needs at a national level. While recruitment has been very successful over the past few years, there are usually still a number of specialties that do not fill all vacancies (as reflected by recent overall fill rates which are less than 100%). A linear career from medical school through to becoming a consultant or a GP is not the only career pathway available to resident doctors, and doctors at all levels of experience provide a valuable contribution to the NHS.
The Scottish Government recognises the calls for greater workforce planning which accounts for the changing landscape of delivering medical care in NHS Scotland, the expectations of patients, and ensures that medical careers remain attractive. The Future Medical Workforce project will seek to explore these issues and hear directly from doctors in order to make the improvements to the medical education pipeline and ensure we can deliver the medical workforce Scotland needs.
Supporting priority specialties: General Practice
Recruitment to General Practice Specialty Training has been successful in recent years, with 99% of advertised posts filled in 2024 (data accurate as of November 2024), comparable with 100% of posts filled in 2023. Since 2022 100 additional GP Speciality Training posts have also been created.
Shifting the balance of care to early intervention and community care is a key part of the Ministerial NHS reform programme and General Practice is an important part of this. A GP Recruitment and Retention Action Plan was developed and published in November 2024, to support progress in this area. This plan sets out 20 measures to improve GP recruitment and retention in Scotland.
As part of the GP Recruitment and Retention Action Plan, we are taking forward the following initiatives to support GP training.
- We are working with partners to better understand challenges and opportunities in relation to training capacity in primary care across Scotland. We are taking this forward through a stakeholder working group which will assess and suggest how to improve training capacity. The group, which is co-chaired by NES and Scottish Government includes representatives from academic General Practice, inclusion health/Deep End General Practice, the BMA, NHS Boards, the Royal College of General Practitioners and University Medical Schools. This group is aiming to produce an interim report in October 2025 and a comprehensive report by early 2026 which will include an assessment of the current capacity and a forecast of the future capacity requirements.
- We will explore with stakeholders how the GP training experience in secondary care settings can be improved.
- We are working to support International Medical Graduates in GP training in Scotland and understand the career intentions and journeys of our GP specialty trainees to enable better planning. This work is being progressed in partnership with NES, the Centre for Workforce Supply, and a number of other stakeholders.
Supporting priority specialties: Psychiatry
Recruitment and retention in psychiatry remains a challenge. This problem is not unique to Scotland and other UK nations are facing similar issues.
The Psychiatry Recruitment and Retention Working Group was established in 2023 to explore how to support the recruitment and retention of trainee doctors and the workforce including consultant and specialty grade doctors. The Group has included representatives from NES, service providers, the Royal College of Psychiatrists in Scotland and various trainee representatives.
In collaboration with the Working Group and working with NES, the Scottish Government has already delivered a number of initiatives and improvements to psychiatry training. The Working Group’s report which was published on Monday 23 June 2025, sets out recommendations for both the training and education of psychiatrists and how to recruit, support and retain the psychiatric workforce in NHS Scotland.
The Scottish Government is working with the Royal College and wider stakeholders to consider the report’s recommendations to determine and assess their feasibility and impact on implementation.
Trainee Experience
Rotational Training
While rotational training can have a range of benefits, it is recognised that it can in some circumstances have negative impacts on resident doctors. Therefore, measures are in place, through NES, to support the health and wellbeing of resident doctors in training including the improvement of placement distribution to ensure more stable and less disruptive rotations, focus on resilience and support including access to flexible working arrangements, and the provision of a Trainee Development and Wellbeing Service.
2025 GMC National Training Survey
The GMC National Training Survey (NTS) is the largest annual survey of doctors across the UK. It gathers the views of doctors in training on the quality of their postgraduate medical education, and work environments. It also seeks feedback from trainers about their experiences as clinical or educational supervisors.
This year, over 71,000 doctors in training and trainers across the UK, completed the survey (5,997 in Scotland). Although the response rate for trainees (70% ↓6 percentage points) and trainers (33% ↓5pp) (71% ↓7pp and 25% ↓6pp in Scotland) was lower than 2024, there is still a robust dataset which allows the GMC to effectively monitor the quality of training environments across all four UK countries. The full survey is available on the GMC website, here.
Across the four nations, Scotland are number one with an overall satisfaction ranking of 80.35% for 2025.
| Nation | 2021 | 2022 | 2023 | 2024 | 2025 |
|---|---|---|---|---|---|
| Scotland | 78.39 | 77.44 | 78.61 | 79.28 | 80.35 |
| England (Average of English Deaneries) | 79.03 | 77.57 | 78.21 | 77.76 |
78.19 |
| Northern Ireland | 79.92 | 78.50 | 76.06 | 76.27 | 78.55 |
| Wales | 79.01 | 77.33 | 77.06 | 78.20 | 78.12 |
This year NHS Education for Scotland (NES) have 21 training programmes within Scotland ranked 1st in their programme groupings for overall satisfaction. Some of the rankings are for its regional programmes, whilst others are for Scotland as a whole.
| Programme | Region | Ranking |
|---|---|---|
| ACCS - Emergency Medicine | NHS Education for Scotland (East Region) | 1st of 18 |
| Acute Internal Medicine | NHS Education for Scotland (North Region) | 1st of 17 |
| Anaesthetics | NHS Education for Scotland (East Region) | 1st of 18 |
| Broad Based Training | NHS Education for Scotland (East Region) | 1st of 1 |
| Cardiology | NHS Education for Scotland (South-East Region) | 1st of 18 |
| Clinical genetics | NHS Education for Scotland (West Region) | 1st of 8 |
| Clinical neurophysiology | NHS Education for Scotland (West Region) | 1st of 3 |
| Core Anaesthetics Training | NHS Education for Scotland (East Region) | 1st of 18 |
| Endocrinology and diabetes mellitus | NHS Education for Scotland (North Region) | 1st of 16 |
| Forensic histopathology | NHS Education for Scotland (West Region) | 1st of 1 |
| General psychiatry | NHS Education for Scotland (West Region) | 1st of 18 |
| General surgery | NHS Education for Scotland (East Region) | 1st of 23 |
| Haematology | NHS Education for Scotland (South-East Region) | 1st of 16 |
| Internal Medicine Training | NHS Education for Scotland (North Region) | 1st of 23 |
| Medical psychotherapy | NHS Education for Scotland (West Region) | 1st of 2 |
| Occupational medicine | NHS Education for Scotland (West Region) | 1st of 7 |
| Old age psychiatry | NHS Education for Scotland (North Region) | 1st of 13 |
| Paediatrics | NHS Education for Scotland (North Region) | 1st of 18 |
| Respiratory medicine | NHS Education for Scotland (South-East Region) | 1st of 17 |
| Urology | NHS Education for Scotland (West Region) | 1st of 16 |
| GP programme - in a GP practice | NHS Education for Scotland (National) | 1st of 17 |
| Vascular surgery | NHS Education for Scotland (National) | 1st of 14 |
Note: The total number of programmes used for the UK ranking relates to programmes that received more than 3 responses. There may be more programmes across the UK than reflected in that total.
Key findings
While there are positives to take from this year’s results, the data reveals the impact that working in a system under sustained pressure is having on doctors in training and trainers. As well as highlighting ongoing concerns about rota gaps and heavy workloads, there are also worrying results relating to workplace cultures:
- A fifth (21%) of all trainees, (21% in Scotland), reported they felt apprehensive or hesitant about escalating a patient to the supervising clinician. This figure rose to more than a quarter for those in emergency medicine, medicine, and obstetrics and gynaecology.
- It is also clear from the results of questions relating to discriminatory behaviours that some doctors with certain protected characteristics are having a different training experience to their colleagues.
- 89% of doctors in training in Scotland rate their clinical supervision highly (87% UK wide). 86% also said they had a good or very good experience in their post (84% UK wide).
- 89% of trainers In Scotland said they enjoy their role (90% UK wide). However, only 48% can always use their allocated time for training specifically for that purpose (52% UK wide). 28% of trainees and 35% of trainers in Scotland also said training was adversely affected because rota gaps were not dealt with appropriately (26% and 29% respectively UK wide).
- 56% of trainees and 46% of trainers in Scotland are considered to be at moderate or high risk of burnout (61% and 47% UK wide). 64% of trainees UK wide said they always or often feel worn out at the end of the working day, compared with 47% of secondary care and 60% of GP trainers.
- 21% of doctors in training in Scotland reported feeling apprehensive or hesitant about escalating a patient to a supervising clinician (21% UK wide). UK wide this rose to 26% for trainees in emergency medicine and medicine, 27% in obstetrics and gynaecology, and 29% in surgery.
- Of those that completed optional questions on discriminatory behaviours, 36% of gay and 46% of bisexual trainees in Scotland (39% and 45% UK wide), reported hearing discriminatory comments, compared to 24% of heterosexual trainees. 18% of female trainees reported being ignored or excluded, compared to 12% of male trainees (17% vs 13% UK wide). And 33% of Scottish graduates from an ethnic minority background report experiencing behaviours like micro-aggressions from colleagues, (34% vs 25% UK wide, compared to 25% of their white colleagues).
The Scottish Government welcomes the valuable insights in the GMC’s annual National Training Survey about the experiences of doctors in training and their trainers over the past year. Whilst we welcome the positive feedback on aspects such as the majority of trainees remain positive about their training - with 76% saying their teaching was good or very good, and 87% rating their clinical supervision highly, we recognise that there is still work to do in a number of areas.
The Future Medical Workforce project which will seek to understand the needs of the future medical workforce and ensure we can deliver the medical workforce Scotland needs in the future. Through this project, we will hear directly from doctors and explore a range of issues including those raised in this report (such as pressure on trainers) and we will work closely with NES and others in order to make improvements to the medical education pipeline.
Less Than Full Time (LTFT) Working
The Scottish Government recognises the impact of Less Than Full Time (LTFT) training and has, through the past annual review of medical training establishments processes, funded a number of additional training posts in impacted specialties to work towards addressing this.
Recognising the need for a more strategic and holistic approach to respond to this changing pattern of working across multiple specialty groupings to take into account the changing choices of resident doctors while ensuring workforce sustainability, the Scottish Government is continuing to work with stakeholders to explore sustainable solutions through future workforce planning taking account of current service and training need, supervision and future trained workforce requirements. Specifically, our intention is to simplify funding arrangements for Whole Time Equivalency adjustment and review post allocation to ensure an equitable distribution across specialties and regions.
We also continue to work with NES to streamline selection and recruitment processes, improve flexibilities within medical training to assist movement into and through specialties, and offer Out of Programme opportunities so that trainees can undertake clinical training/experience, research or take a career break.
Future Medical Workforce project
The Scottish Government recognises the need for a workforce plan to account for what patients and the public want and need from their health service, and to ensure the attractiveness of medical careers.
We are undertaking a project to consider Scotland’s future health care needs and the medical workforce required to deliver care in 15 – 20 years’ time.
The project will involve extensive engagement with the workforce and other stakeholders, as well as analytical scenario modelling to gain an understanding of future demand and supply, with the ultimate aim being to arrive at a workforce plan for Scotland’s medical workforce.
The Future Medical Workforce project will not cover current pay or terms and conditions.
Undergraduate - Scotland’s medical undergraduate intake
Medical Student Intake Numbers
The Scottish Government’s Health Workforce Directorate convenes the Medical Undergraduate Group (the MUG) to consider Scotland’s annual medical undergraduate intake. The Group’s primary purpose is to ensure an appropriate supply of high-quality trained doctors to meet the needs of NHS Scotland’s medical workforce whilst avoiding, or minimising, the possibility of medical unemployment.
For 2025-26, Scottish Ministers approved a medical undergraduate intake of 1,417, a 67% increase compared to the 2015-16 intake of 848. The MUG will meet in early 2026 and the Scottish Government will send the guidance letter on the 2026-27 undergraduate intake to the Scottish Funding Council thereafter.
Widening Access (WA) to a career in medicine is key to creating a diverse environment that benefits students and medical practice in Scotland. WA is a key to medicine is one of the Scottish Government’s key policy priorities. We therefore fund a number of places every year which are reserved for students who meeting the criteria for WA, targeting those from the lowest quintile of multiple deprivation (SIMD 20).
2.5 ANNEX B
Relevant GDS data is available:
Dental Activity
This report includes information on dental activity, participation, and registration.
Dental Workforce
The information can be accessed at Dental Workforce Report 2024.
This provides detail on inflow, outflow, and stock of dentists however data is broken down by GDS/PDS and Hospital dental services such that PDS cannot be separately identified.