Doctors' and Dentists' Remuneration - 2026-2027 pay round: written evidence
The Scottish Government's remit letter and written evidence document for the 2025 to 2026 pay round, submitted to the Doctors' and Dentists' Remuneration (DDRB) review body for their consideration.
The Scottish Government's written evidence to the review body on doctors' and dentists' remuneration (DDRB) for the 2026-27 pay round
Scottish Government Health Directorates' submission to the DDRB 2026
1.1 A. Introduction
1. This evidence has been prepared by the Scottish Government Health and Social Care Directorates (SGHSCD), and we are now pleased to be able to submit this to the Review Body on Doctors’ and Dentists’ Remuneration (DDRB) for consideration.
2. Our remit letter to the DDRB for this pay review round was submitted on 24 September 2025 by the Cabinet Secretary for Health and Social Care. This sets out that we are seeking recommendations for all medical and dental staff in NHS Scotland, for medical and dental contractors in primary care, but not for Resident Doctors or Resident Dentists.
3. In 2025/26, the Scottish Government accepted the DDRB recommendations for participating staffing cohorts. We believe that these were reflective of the economic conditions within Scotland and the United Kingdom at large. More broadly, the Scottish Government has pursued a path of fairness, equity, and affordability in respect of public sector pay deals with a number of multi-year pay agreements being reached which reflect the projected economic conditions.
4. The Scottish Government remains committed to ensuring that people of Scotland have access to high quality healthcare when they need it. This commitment to high quality public service must however be linked to both prudent financial stewardship, fiscal sustainability and to reform which secures the delivery of improved outcomes and services over the medium term. It is clear that the NHS workforce and how they are renumerated will form a critical part of this process.
5. Plans around pay for the relevant Medical and Dental groups in 2026/27 should align with our broader approach to fairness, equity and affordability across the public sector but also need to be balanced against our continued commitment to no compulsory redundancies and broader reform and renewal activity that is underway across NHS Scotland.
1.2 B. The Scottish Context
Health and Social Care Reform and Renewal
6. Through the Population Health and Health and Social Care Service Renewal Frameworks announced in June 2025, we have already set out our long-term plans for the reform and renewal of health and social care in Scotland. Our focus now is on delivery, translating those ambitions into tangible improvements for patients and communities.
7. The Scottish Government, in partnership with COSLA, is driving this reform through the Service Renewal Framework (SRF) and the Population Health Framework (PHF). Together, they take a whole-system, medium- to long-term approach to address the systemic challenges facing health and social care over the next decade.
8. The frameworks are underpinned by four shared values that mirror international health reform efforts and are supported by increased investment for health and social care in the 2025-26 Budget:
- Prevention – helping people live longer in good health.
- Access – ensuring care is available when and where it is needed.
- Quality – delivering safe and effective treatment.
- Person-led – focusing on outcomes that matter to people.
9. Alongside this, the NHS Operational Improvement Plan published in March 2025 focuses on short-term improvements, while the SRF and PHF drive the longer-term shift towards prevention, joined-up services and efficiency across the health and social care system.
10. Within this reform agenda, general practice remains central. The 2018 GP Contract, developed in partnership with the BMA, laid the groundwork for a more sustainable model of General Medical Services. Since 2018, we have significantly expanded the multi-disciplinary team (MDT) workforce in primary care, with over 5,000 WTE staff now supporting general practice across physiotherapy, pharmacy, and phlebotomy. We continue to invest over £190 million in 2025-26 through the Primary Care Improvement Fund to sustain and develop these teams, supporting earlier intervention and improved access to care.
11. We are now building on this foundation. Work underway through the Primary Care Phased Investment Programme will help identify the conditions that enable effective MDT working and inform the next stage of reform. Findings early next year will shape future investment in primary and community care and support delivery of SRF and PHF priorities.
12. We remain committed to a modern, sustainable model of general practice that supports prevention, continuity, and access. This includes progressing Phase Two of the 2018 GP Contract with the BMA by exploring direct reimbursement of practice expenses and aligning future investment with the SRF and PHF to secure a sustainable, prevention-focused general practice service at the heart of our rebalanced health and care system.
1.3 C. Economic and Labour Market Conditions in Scotland
Economic and Labour Market Overview - Data up to 15 January 2026
13. The Scottish economy grew 1.1% on an annual basis in the 3-months to October 2025 and inflation is currently on a downward trend, however there are indications that the labour market has softened over the past year and as highlighted by the Scottish Fiscal Commission in their January 2026 forecasts, the economic outlook remains uncertain.
14. Looking ahead, economic growth is forecast to increase moderately in 2026 to 1.3% and inflation is expected to fall closer to its 2% target rate in April. Unemployment is forecast to increase to 4.2% in 2026-27 while average nominal earnings growth is forecast to slow to 2.9% over the same period.
GDP growth
15. Scotland’s economy grew 1.0% in 2024 and latest data indicates the economy has grown 1.1% on annual basis in the 3-months to October 2025.[1]
16. Most recently, RBS Growth Tracker business survey data indicates that business activity in Scotland softened slightly in the final quarter of 2025 with the business activity indicator showing a slight fall in activity over the 3-months.[2]
17. Looking ahead, the Scottish Fiscal Commission (SFC) forecast economic growth in Scotland to strengthen from 1.1% in 2025 to 1.3% in 2025 and 1.3% in 2026. This is slightly slower than the Office for Budget Responsibility (OBR) forecasts for the UK economy of 1.5% in 2024, 1.4% in 2026 and 1.5% in 2027, with the difference largely due to weaker population growth in Scotland.[3],[4]
Inflation
18. Consumer price inflation has increased over the past year from 3% in January 2025 to peak at 3.8% in the third quarter before falling back to 3.2% in November.[5] Following the UK Budget announcements on administered prices and indirect taxes, the Bank of England expects inflation to fall back closer to the 2% target rate in April 2026.
19. Reflecting the outlook for inflation, the Bank of England have continued to reduce the Bank Rate gradually in 2025, with three 25-basis point rate cuts taking the rate to 4%, its lowest rate since the start of 2023.[6] Reflecting the outlook for inflation, the Bank of England continued to reduce the Bank Rate gradually in 2025, with four 25-basis point rate cuts taking the rate to 3.75%, its lowest rate since the end of 2022.[7]
Labour Market
20. Labour market conditions have remained resilient in 2025 though have softened over the year.
21. Scotland’s unemployment rate was 3.8% in August to October 2025, up 0.2 percentage points over the year, while the employment rate rose 1.6 p.p to 74.9% and the inactivity rate fell 1.9 p.p to 22.0%.[8]
22. Wider labour market indicators for November show the number of payrolled employees in Scotland fell 0.6% over the year to 2.45 million, while Scotland’s claimant count unemployment rate fell marginally to 3.5%.[9]
23. RBS Growth Tracker business survey data indicates that there was a general pattern of falling private sector staffing levels during 2025, although latest data indicates staffing levels were more stable in for December.
24. The SFC forecast the unemployment rate to rise to 4.0% in 2025-26 and 4.2% in 2026 27.
Earnings
25. Earnings growth remained robust during 2025, however slowed notably towards the end of the year.
26. Median nominal PAYE monthly pay increased 1.1% over the year to November to £2,562 and once adjusted for inflation, fell 2.1% annually.[10]
27. At a sector level, latest data for August to October show that average weekly earnings for regular pay in Great Britain grew 7.6% on an annual basis in the public sector and 3.9% in the private sector.[11]
28. The SFC forecast average nominal earnings growth in Scotland to slow from 5.2% in 2025-26, to 2.9% in 2026-27 and 2.7% in 2027-28.
1.4 D. Resources, Affordability and Pay
29. This chapter sets out the financial context including assumptions on funding available in 2026-27.
Overall Funding
30. The Scottish Government published its 2026-27 Budget on 13 January 2026 which sets out almost £22.5 billion investment in health and social care services.
31. If approved by Parliament, in 2026-27 more than £17.6 billion will be provided to Health Boards to deliver front line and other key services, and this includes funding to honour our commitments to fair pay settlements for our health workforce. This represents a real terms uplift of 1.8% on Health Board baseline funding.
32. The Scottish Government has been consistently clear on the extent of the challenges faced, with successive budgets and medium-term financial strategies highlighting the choices and trade-offs necessary to deliver a balanced and sustainable position.
33. Whilst the UK Budget did result in an additional £820 million for Scotland over the UK Spending Review period, this is only a marginal increase on assumptions set out in the June 2025 Medium-Term Financial Strategy.
34. Resource funding is expected to grow each year by an average of 1.1% in real terms across the forecast period. This small uplift is not enough to change the difficult fiscal position that we face, meaning tough choices, reform, and efficiencies, are required to balance the demands for public spending within our funding constraints.
Affordability - the funds available
35. As outlined above, Health Boards will receive a 1.8% uplift on baseline funding in 2026-27. This includes the impact of the agreed 2 year pay settlements and is to meet the expected costs of 2026-27 pay in line with public sector pay policy (as set out in the section below) and also provides an inflationary uplift to support non pay budget lines.
36. Despite this funding increase, significant financial and operational challenge remains. The NHS Scotland Finance Delivery Unit, commissioned by Scottish Government, continues to work with all NHS Boards to drive sustainable improvement.
37. This includes supporting delivery of a minimum of 3% recurrent savings for NHS Boards, reviewing all local, regional and national opportunities, and setting out the medium to long term financial forecast assumptions for NHS Scotland to support delivery of longer-term financial sustainability.
38. Prevention, early intervention and reform remain critical to delivering an effective, efficient and sustainable health and social care system.
Public Sector Pay
39. The Scottish Government have published an Integrated Pay and Workforce Policy for the first time, aligning pay decisions with workforce planning. This policy is the first step in operationalising the commitments in the FSDP to manage the public sector paybill and workforce size through a co-ordinated approach to pay and workforce planning.
40. Inflation-linked clauses were essential to secure agreements during a period of increased inflation. These measures ensured workforce stability and service continuity and future pay policies will review the role of inflation-linked clauses to maintain fiscal sustainability.
41. The integrated pay and workforce policy reflects that 2026-27 is the second year of the 3-year Public Sector Pay Policy announced with the 2025-26 Budget which set out multi-year pay metrics of a 9% pay envelope covering 2025-26, 2026-27 and 2027-28.
42. As the majority of the public sector have agreed 2-year deals covering 2025-26 and 2026-27, our Integrated Pay and Workforce Policy commits to reviewing the 2027-28 pay policy as part of the 2027-28 budget process.
43. Multi-year pay deals provide an opportunity to plan for and transform our public services to improve outcomes for the people of Scotland.
44. Inflation-linked clauses were essential to secure agreements during a period of increased inflation. These measures ensured workforce stability and service continuity and future pay policies will review the role of inflation-linked clauses to maintain fiscal sustainability.
45. Although inflation remains above target it has fallen from 3.8% in September and is forecast to fall further and average 2.5% across 2026, with falling interest rates also helping reduce household costs.
46. We recognise that pay and wider paybill costs are an important driver of our overall spend as a Government. Pay continues to place pressure on the sustainability of the public finances with the total paybill estimated to be around £30 billion in 2026-27. We must ensure that pay rises are affordable now and in the future.
47. To maintain financial and service sustainability, particularly in the face of rising workforce costs and easing inflationary pressures in 2026/27, it is vital that pay decisions continue to be made within this framework.
1.5 E. NHS Pensions and Total Reward
NHS Pension Scheme (Scotland)
48. The NHS Pension Scheme (Scotland) (NHSPS(S)) remains an integral part of the NHS remuneration package and is a key recruitment and retention tool for doctors and dentists. It provides a secure, defined benefit pension, which continues to be highly valued by staff and represents one of the most significant non-pay benefits available. Employers contribute 22.5% of members’ pay to the scheme which is significantly higher than employer contribution rates typically found in the private sector.
49. Occupational pension policy is generally reserved to the UK Government. Pension benefits and employee contributions in the NHSPS(S) are tightly constrained by a mixture of UK Government financial and legislative controls, and benefits mirror that of the scheme in England and Wales. HM Treasury (HMT) consent is required for the Scottish Government to make changes to the scheme regulations.
50. The NHSPS(S) is made up of two existing defined benefit schemes. The first is the final salary scheme, also known as the legacy scheme, which includes the 1995 and 2008 sections and is no longer open to new members. All new employees join the 2015 scheme, a career average revalued earnings (CARE) scheme that calculates benefits based on the member’s average earnings throughout their career. The key distinctions between the two schemes, apart from how benefits are calculated, lie in their normal pension ages and accrual rates, which are detailed in the table below.
| Scheme of Section | Normal Pension Age (NPA) | Accrual Rate |
|---|---|---|
| 1995 Section | 60 | 1/80th |
| 2008 Section | 65 | 1/60th |
| 2015 Scheme | State Pension Age | 1/54th |
51. The 2015 Scheme was established as part of reforms introduced by the Public Service Pensions Act 2013. As part of these reforms, members of public service pension schemes nearing retirement—specifically those within 10 years—were granted transitional protection, allowing them to stay in their legacy pension scheme. However, in December 2018, the Court of Appeal ruled that this protection was discriminatory towards younger members, a ruling that has since been referred to as the 'McCloud judgment.' The government acknowledged that this judgment also applied to other public service schemes, including the NHSPS(S).
52. The public service pension schemes remedy (‘the remedy’) for this discrimination has two parts. The first and prospective part, moved all members to the reformed 2015 NHSPS(S) from 1 April 2022. Secondly, to put right, or 'remedy,’ the discrimination, members’ pensionable service in the 2015 Scheme, for the remedy period (1 April 2015 to 31 March 2022), was moved back into the legacy (1995/2008 Sections) Scheme. Members will then be given a choice at retirement to receive the pension benefits from the legacy or the reformed scheme.
53. A key advantage of the 2015 scheme is that for active members, the pension they accrue is adjusted each April based on the Consumer Price Index (CPI) from the previous year, with an added increase of 1.5%. This process is known as ‘in-service revaluation.’ It ensures that pension benefits keep pace with the rising cost of living. As of April 2025, this adjustment reflected an increase of 1.7%.
Scheme Membership
54. The NHSPS(S) Advisory Board regularly monitors scheme participation rates across the workforce.
55. Participation in the NHSPS(S) remains high, with evidence showing that staff continue to view the scheme as both affordable and valuable. The table below shows the percentage of hospital doctors and dentists, by grade, who were members of the scheme in March 2025 and in comparison, to March 2024, March 2020, and March 2015.
| Profession | March 2025 | March 2024 | March 2020 | March 2015 |
|---|---|---|---|---|
| Foundation doctor Yr 1 | 96.4% | 96.1% | 95.9% | 99.2% |
| Foundation doctor Yr 2 | 95.2% | 95.9% | 94.3% | 97.4% |
| Speciality Registrar | 94.7% | 93.3% | 96.6% | 97.9% |
| Consultant | 94.1% | 92.7% | 87.7% | 94.3% |
| Speciality Doctor | 93.9% | 93.8% | 94.4% | 93.5% |
| Associate Specialist | 97.1% | 96.4% | 96.4% | 98.0% |
| Other | 89.6% | 87.9% | 87.3% | 89.6% |
| Total | 94.2% | 93.1% | 91.8% | 95.3% |
56. High participation rates amongst hospital doctors and dentists compare favourably with those across the wider NHS hospital workforce, where overall scheme membership stood at 93.4% in March 2025.
57. Amongst General practitioners (GPs) participation also remains relatively high with 87.1% of GPs participating in the scheme in March 2025. This is a marginal increase from 87.0% being members of the scheme in March 2024 and 79.0% in March 2023.
58. For General Dental Practitioners (GDPs) participation is slightly lower, with 84.0% participating in March 2025, up from 83.6% in March 2024 and 81.9% in 2023.
Retirement Options and Flexibilities
59. The Scottish Government has introduced significant changes to retirement flexibilities in recent years, with the aim of retaining senior doctors and dentists who might otherwise have left the workforce.
60. Retire and Return was introduced in April 2023 and allows members of the 1995 section of the NHSPS(S) to retire and return to pensionable NHS employment without the previous restrictions.
61. Partial Retirement was introduced from October 2023, allowing members to claim part of their pension while continuing to work in a reduced capacity, as an alternative to full retirement.
62. These flexibilities have proven popular. Around 30% of new retirement applications from hospital doctors and dentists are for partial retirement. Amongst GPs and GDPs uptake is lower with around 14% of retirements being on a partial basis.
63. There were 164 GPs and GDPs who took early retirement between 1 April 2024 and 31 March 2025. Claiming one, or both, of their final salary and CARE pensions before the respective scheme’s normal pension age. This is an increase on figures for the previous year, when 122 practitioner members retired early.
64. The retirement application form does not request reasons why a member is taking early retirement, so this type of detail is not held by SPPA. Also, SPPA would not be notified where a member takes early retirement and re-joins the workforce without re-joining the pension scheme.
65. Unfortunately, the pension data held by SPPA does not distinguish between job roles, so it is not possible to provide early retirement figures for hospital doctors and dentists.
Scheme Contributions
66. Members and employers are both required to contribute to the costs of the benefits accrued in the NHSPS(S). Currently, employers contribute 22.5% of each member’s pensionable earnings.
67. The NHSPS(S) moved from final salary benefits to career average revalued earnings (CARE) benefits in 2022 and, following the closure of the 1995/2008 Scheme, it was deemed an appropriate time to reform the member contribution structure. On behalf of Scottish Ministers, SPPA conducted a consultation on changes to member contributions and published a consultation response in September 2023.
68. The consultation response confirmed the introduction of changes to the structure by rebalancing contribution rates and narrowing the range of contribution tiers, assessing contribution rates based on actual pay rather than whole-time equivalent, and changing the approach to increasing tier boundaries in line with Agenda for Change (AfC) pay awards. It was proposed to implement the changes using a phased approach over two years, commencing in October 2023.
69. The second and final phase of these reforms, was introduced from 1 October 2024, and completed the planned adjustments to the member contribution structure.
70. As of 1 April 2025, the following member contribution structure will apply for the 2025 to 2026 Scheme year:
| Pensionable earnings bands | Contribution rate from 1 April 2025 |
|---|---|
| Up to £13,330 | 5.7% |
| £13,331 to £26,762 | 6.4% |
| £26,763 to £31,669 | 7.0% |
| £31,670 to £39,734 | 8.7% |
| £39,735 to £41,669 | 9.8% |
| £41,670 to £50,650 | 10.5% |
| £50,651 to £54,811 | 11.2% |
| £54,812 to £76,652 | 11.6% |
| £76,653 and above | 12.7% |
Pension Taxation
71. There have been significant changes to Annual Allowance (AA) and Lifetime Allowance (LTA) pension tax rules, introduced through UK Budgets in 2023. These changes saw the AA limit increase from £40,000 to £60,000 and the minimum tapered AA increase from £4,000 to £10,000. The adjusted threshold income for the tapered AA has also increased from £240,000 to £260,000. Finally, the abolition of the LTA from 2024 means that fewer doctors and dentists are likely to incur tax charges on their pension savings, than in previous years.
72. Where senior clinicians continue to incur AA tax charges, the scheme pays facility allows them to meet their tax lability from their pension benefits, without needing to find the funds upfront. Analysis from the Government Actuary’s Department shows that for most members, Scheme Pays is a proportionate way of dealing with an AA tax charge. The analysis shows that it may be a sound financial decision for clinicians to incur an AA tax charge and to use Scheme Pays to deal with it, as it will have a relatively small impact on accrued pension benefits. While the Scheme Pays deduction will reduce the value of pension accrued, the growth in benefits represents a good return on contributions made.
73. The highest-earning doctors and dentists might face a reduction in their AA due to a process known as ‘tapering.’ This means that as their income rises, their AA decreases. According to the changes implemented during the 2023 Budget, the minimum tapered AA is set at £10,000.
74. The tapered AA applies when an individual's ‘threshold income’ exceeds £200,000, and their ‘adjusted income’ goes beyond £260,000. Given the benefits of the NHS Pension Scheme, it is anticipated that most doctors and dentists making more than £200,000 will likely have an ‘adjusted income’ surpassing £260,000, thus falling under the tapered AA.
75. It is recognised that this situation can lead to a cliff edge, where even a slight rise in earnings can activate the taper and result in a significant increase in tax liability. Consequently, the possibility of tapering might deter doctors from accepting additional work, as their extra earnings could be offset by pension tax charges.
76. Doctors and dentists who exceed the tapered AA can utilise Scheme Pays to cover their tax liabilities. Scheme Pays deductions are typically larger for individuals with a tapered AA compared to those with a standard AA. However, these deductions are expected to be considerably smaller than their overall pension, which will continue to grow as they near retirement.
1.6 F. Workforce Planning
77. The Health and Social Care: National Workforce Strategy sets out our vision for the health and social care workforce. The strategy supports the ambition of recovery, growth and transformation of our workforce and the actions we will take to achieve our vision and ambition. This includes our commitment to increase the number of GPs by 800 by 2027.
78. In November 2024 we shared with the profession our GP Recruitment and Retention Action Plan which sets out in more detail our package of measures to deliver on the commitment to increase the number of GPs by 800. This includes 20 key actions across the GP training pipeline and career pathway, including increasing the number of GPST placements through to improving the fellowship programme for early career GPs and reviewing and developing the retention initiatives to support GPs to remain in practice.
79. There has been good progress in a number of areas including improvements to workforce data, guidance for practices and IMGs on visa requirements to work in General Practice. We have also established new leadership training for mid-career GPs in terms of their role within the practice and early career GPs, who may be considering entering Partnership, offered through the Royal College of GPs.
80. National Education for Scotland have expanded their GP coaching programme and have also launched the new GP Retain and Sustain scheme. This will replace the Staying Practice and GP Retainer Scheme will offer support to GPs who are at risk of leaving the profession for a range of reasons not just due to childcare challenges. We are working closely with Health Boards to expand the GP Fellowship schemes to support Early Career GPs to transition into the workforce. We continue to work with stakeholders to deliver on the longer-term actions within the plan.
Projecting future GP requirement
81. We are committed to taking an evidence informed approach to building and developing a sustainable workforce that best meets the needs of the Scottish population. Our new investment to expand workforce capacity will grow year on year and give practices flexibility to shape their teams according to patient need and to ensure sufficient levels of GP input per practice population. Assessment of population health need and the required workforce will be informed by the Future Medical Workforce Project and the strategic direction set by the Primary Care Route Map.
Incentive Schemes
82. We incentivise GPs into taking up harder to fill posts, mainly those in rural and deprived areas, through our £10,000 'Golden Hello' scheme. This scheme offers a bursary of up to £10,000 to every GP taking up an eligible post. ‘Golden Hellos’ for Scottish GPs are set out in chapter 11 of the annual Statement of Financial Entitlements (SFE)[12]. Golden Hellos can also be paid to new GP performers if the local Health Board believes the practice is experiencing significant difficulties around recruitment and retention. These are just for GPs in GMS practices with the exception of Golden Hellos for remoteness and rurality which are for all practices regardless of contractual status.
| Reason | Payment |
|---|---|
| Recruitment Difficulty | £5,000 (minimum) |
| Remoteness or Rurality | £10,000 |
| Deprivation | £7,500 - £12,500 |
83. The rate of payment for part time GPs, with a time commitment fraction of less than 4 sessions per week is 60% of the full payment.
84. The Scottish School of Primary Care are currently evaluating the Golden Hello scheme to assess the role that financial incentives play in supporting GP recruitment and retention. The final report will be available in October 2025.
GP Partners
85. The number of GP Partners has reduced since 2017 from 3482 in 2017 to 3071 in 2025. This reflects a broader trend towards fewer and larger practices incorporating multi-disciplinary teams to provide a wider range of services. On average Partners work 0.82 WTE.
86. We recognise from our work with GPs that becoming a Partner can present particular challenges and require the development of new skills. We have funded a new RCGP project ‘First5 to Partnership’ this year with an aim to support the future leaders of General Practice. We are also working with NES to expand their ‘Preparing for GP Partnership’ course to include all GPs and not just First 5’s with a view to running this as a free course for all in 2026.
Vacancy data
87. The percentage of practices reporting vacant GP sessions has fallen from 39% in 2023 to 14% in 2025. The vacancy rate has fallen from 10.9% in 2023 to 3.8% in 2025.
88. The latest GP Workforce Survey published on 26 August 2025. In this year’s survey GP Practices were asked whether, for the vacancies they reported, they were actively seeking to recruit for the post.
89. Of the vacant sessions where practices were not seeking to recruit, practices were asked to provide a reason, from No funding available, No suitable candidate, or Other. The most common reason given was Other with 70.0%, followed by No funding available with 19.5%. We continue to work with the profession to understand the reasons for this and address any issues relating to GP unemployment.
90. We continue to work with NES and engage with GP representatives and other stakeholders to understand the trends in GP vacancies and to take appropriate action to address identified challenges.
91. The General Practice Workforce survey is now being run on an annual basis. The most recent publication was on 26 August.
Workforce Statistics
NHS Scotland Medical & Dental Workforce from 2006
- Numbers of medical and dental staff in post have risen from 10,160.9 WTE in Sept 2006 to 15,780.7 WTE in June 2025. This represents an increase of 55.3%.
- There are 6,224.3 WTE medical and dental consultants (incl director-level consultant) employed by NHS Scotland at June 2025 – an increase of 71.2% (2,587.5 WTE) since Sept 2006.
- M&D Doctors in Training up 24.7%, or 1,315.6 WTE (from 5,336.2 WTE as at Sept 2006 to 6,651.8 WTE as at June 2025).
- Doctors (excluding dentists) up 57.2%, or by 5,493.4 WTE (from 9,600.4 WTE as at Sept 2006 to 15,093.8 WTE as at June 2025).*
[*Note: These figures slightly overstate the true increase as locum appointment training (LAT) grade staff started to be included in Doctors in Training from September 2018.]
Dentists
- The number of dentists working in the General Dental Service or as Hospital Dentists has increased by 4.2% over the past year to 3,260. The majority of dentists are independent contractors and are in addition to medical and dental employment figures quoted above.
DDRB remit groups
- Numbers of medical and dental staff in post have risen from 12,501.2 WTE in June 2015 to 15,780.7 WTE as at June 2025. This represents an increase of 26.2%.
- For medical and dental specialties, the median age is 39 and 12.1% of staff within this specialty are aged 55 and over.
Vacancies
- Medical consultant vacancy rate (as a percentage of establishment) is 7.2% (464.4 WTE) as at June 2025 a slight increase from 7.1% (450.6 WTE) as at June 2024.
- Medical Consultant Vacancy rate of six months or more (as percentage of establishment) is 2.8% as at June 2025, a decrease from 3.9% as at June 2024.
- As at June 2025, the number of vacant consultant posts in dental specialties was 4.3 WTE with a vacancy rate of 4.6%, a decrease from 7.2% (6.9 WTE) as at June 2024. Of these, 3.3 WTE have been vacant for 6 months or more, representing a 6 months or more vacancy rate of 3.5%.
Staff Turnover
- Official data on turnover (staff leaving and joining NHS roles) is published on an annual basis at June with data as at 31st March.
- Turnover excludes medical and dental staff on training grades. This is to avoid the distortion caused by the frequent rotation of staff in training placements.
- For medical and dental staff across Scotland, the turnover rate in 2024/25 was 11.8%, this is higher than the turnover rate of 6.3% for all NHS Scotland staff.
- The turnover rate for medical and dental consultants was 4.5% in 2024/25.
- The number of medical and dental staff who left NHS Scotland in the last financial year increased by 2% on the previous year.
- The number of medical and dental staff who joined NHS Scotland in the last financial year decreased by 13% on the previous year.
Medical Agency Locum Spend
- In the last financial year Medical Agency Locum Spend decreased by 16.7% on the previous year from £129.6m to £108m in 2024/25.
Medical Locum
92. More broadly, the Scottish Government recognises that supply challenges for the medical workforce have a consequential impact on financial and service sustainability within NHS Scotland and engagement on this issue with Staff and Employers is critical.
93. NHS Scotland has made clear progress in reducing reliance on medical agency workers, with expenditure down 16.7% in the past year. Across combined medical, nursing and midwifery agency use, we have seen a reduction of more than £110 million.
94. This is in keeping with our commitment to direct as much of our resources as possible towards frontline services and has allowed Health Boards to re-invest upwards of £110 million in the delivery of those services most valued by the Scottish public.
95. Medical agency expenditure has decreased by 16.7% in the past year to £108 million.
96. Medical agency expenditure decreased in 10 territorial NHS Boards in the year ending 31 March 2025.
97. Whilst the use of temporary staff will always be needed in NHS Scotland, our aim is to limit all agency use as much as possible, with more shifts being filled either by substantive staff or through NHS Board staff banks.
98. This is supported by the year-on-year growth we have seen in our workforce for over a decade and the 67% increase in Scotland’s medical undergraduate intake since 2015.
1.7 G. Education and Training
99. We are not asking DDRB to make recommendations for Resident Doctors or Resident Dentists. We have however included as Annex A, Information on medical trainees.
1.8 H. Specific Staff Groups – Pay, Terms and Conditions
General Medical Practitioners
Introduction
100. This section provides information relating to general practice (independent contractor GMPs) and the delivery of contracted services through the NHS Boards. This section also provides additional background to developments with the GMS arrangements in Scotland, and the implementation of the new contract in 2018.
Background
101. The majority of GMPs working to provide primary medical services in Scotland are independent contractors, self-employed or partnerships running their own GP practices.
102. The General Practice – GP practice list sizes was published on 15 July 2025. As of 1 July 2025, there were 885 GP practices[13] in Scotland and 84.7% were on the national General Medical Services contract. The number of practices in Scotland has decreased by 10.9% from 994 practices in 2013, reflecting a trend towards larger practices with more GPs serving a larger number of patients. GMPs operating under Section 17C or 2C arrangements provide services based on locally agreed contracts, and any uplift in investment for these arrangements is a local matter for the Health Board.
As of 1 July 2025:
- 750 practices operated under the General Medical Services Contract;
- 78 practices operated under the 17C contract; and
- 57 practices operated under the 2C contract[14].
103. The average (or mean) size of a Scottish GP practice in terms of numbers of registered patients was 6822 in 2025[15], however there was considerable variation, ranging from under 200 patients for practices in remote locations or practices which addressed specific health needs of patients (e.g. those with challenging behaviours or homelessness), to practices of over 20,000 patients in densely populated urban areas.
Pay and Contractual Uplift 2022/23
104. For 2025/26 the Scottish Government implemented the DDRB recommendation to uplift GP pay net of expenses by 4%. In total the Scottish Government uplifted the GP contract by £46 million. This also included a 4.25% uplift to practice staff expenses, and a 4.5% uplift to wider practice expenses. This also included £6.4 million funding to cover population growth in 2024/25.
105. The contractual uplift was applied consistently across all general practices.
Investment in General Practice
106. In 2024/25 the sum of NHS Scotland payments made to 892 General Practices was £1.156.9 billion. Investment had increased by £88.6 million (8.3%) when compared to 2023/24.
- £981.4million was paid to 746 General Medical Services (GMS) contracted practices run by GPs;
- £127.9 million was paid to 84 locally negotiated contracted practices (17C) run by GPs; and
- £47.6 million was paid to 62 NHS Board run practices (2C).
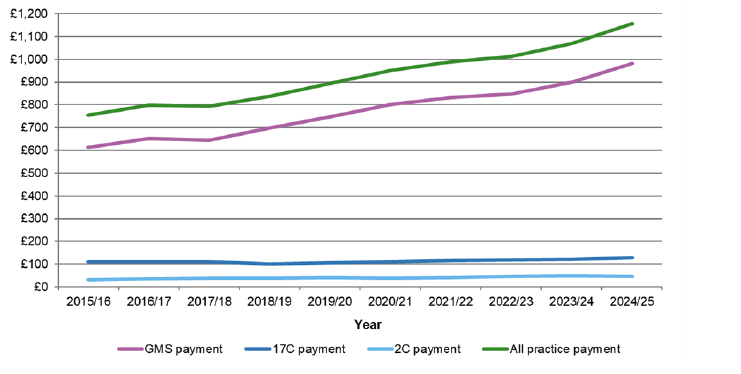
107. Of the £1.156.9 billion paid in 2024/25, the Global Sum was the largest payment amounting to £836.5 million paid to 892 General Practices.
108. In addition to the £1.156.9 billion, an amount of £23.5 million was paid to 82 General Practices for dispensing services in 2024/25.
109. General practice will receive additional funding of £531 million over the next three years to support core general practice. This is the largest investment in core GP services to date in Scotland.
110. The funding will help boost recruitment, staff numbers, and capacity, support day-to-day operations, and make it easier for people to access GP services. This is not a pay deal – it is about stabilising practices, getting more staff into general practice, and strengthening the foundation of community care.
Subject to future budget processes, the investment breaks down as follows:
- An initial investment of £98 million in 2026-27
- £183 million in 2027-28
- £249 million in 2028-29
111. This investment is designed to expand the workforce with new posts and flexible options, GP partners, salaried roles, locums, fellowships and administrative support. It will allow practices to shape their teams around local need, not one-size-fits-all targets. As part of Phase Two it will support reform of expenses to reduce financial volatility for practices and to support fairer funding. It includes improvements to sick, maternity and study leave arrangements to support wellbeing and retention, and it creates conditions for GPs to focus on clinical leadership and quality.
112. In the short-term the investment aims to deliver more reliable and appropriate access, improved continuity of care, and stronger management of long-term conditions. Practices will experience greater stability through direct reimbursement of expenses and more resilient workforce planning.
113. In turn, this will drive medium-term outcomes including fewer avoidable hospital admissions; earlier intervention and prevention of disease progression; reduced unwarranted variation in access and outcomes between deprived and affluent communities; and higher levels of patient and workforce satisfaction.
114. The long-term impacts are aligned with the aims of the Service Renewal Framework and the Population Health Framework. The investment will lay the foundations for more care to be delivered closer to home, and for reform to ensure that prevention is embedded as an organising principle of the system.
| Priority | 25/26 (£m) | 26/27 (£m) | 27/28 (£m) | 28/29 (£m) | Total recurring (£m) |
|---|---|---|---|---|---|
| Workforce | n/a | 35 | 31.6 | 51.7 | 118.3 |
| Workforce Tranche 1 | 15 | n/a |
n/a |
n/a |
15 |
| Workforce Tranche 2* | n/a | 15 |
n/a |
n/a |
15 |
| Sickness, Maternity etc. Cover | n/a | 7.5 | n/a | n/a | 7.5 |
| Expenses | n/a | 10 | 21.7 | 8.3 | 40 |
| Premises | n/a | - | 15 | 15 | |
| Inequalities | n/a | - | 5 | 5 | 10 |
| Digital and access | n/a | 5.5 | 8.7 | n/a | 14.2 |
| Quality | n/a | 2 | 3 | n/a | 5 |
| Digital prescribing | n/a | 8.14 | 0.4 | 0.82 | 9.36 |
| Total additional funding | 15 | 83.14 | 85.4 | 65.82 | 249.36 |
| Total (cumulative) | 15 | 98.14 | 183.54 | 249.36 | 249.36 |
Vacancy, Turnover and Attrition Rates
115. According to the General Practice Workforce Survey Scotland 2025, 14% of practices reported they had vacant GP sessions at March 2025, in comparison with 39% at March 2023. The overall vacancy rate was 3.8%. The vacancy rate varies by NHS Boards, ranging from 0.8% in Forth Valley to 15.5% in Highland.
| Health Board | % of practices with vacancies | Vacant GP sessions | Contracted GP sessions | Vacancy rate (%) |
|---|---|---|---|---|
| NHS Ayrshire & Arran | 17.0% | 63.8 | 1,964.5 | 3.1% |
| NHS Borders | 13.6% | 15.2 | 649.0 | 2.3% |
| NHS Dumfries & Galloway | 6.2% | 11.7 | 723.6 | 1.6% |
| NHS Fife | 11.5% | 35.4 | 1,763.5 | 2.0% |
| NHS Forth Valley | 4.2% | 12.2 | 1,485.5 | 0.8% |
| NHS Grampian | 21.4% | 93.0 | 2,887.7 | 3.1% |
| NHS Greater Glasgow & Clyde | 8.0% | 102.4 | 5,975.8 | 1.7% |
| NHS Highland | 22.0% | 440.3 | 2,400.0 | 15.5% |
| NHS Lanarkshire | 11.7% | 112.9 | 2,523.6 | 4.3% |
| NHS Lothian | 7.8% | 59.2 | 5,461.0 | 1.1% |
| NHS Orkney | 71.4% | 26.0 | 268.9 | 8.8% |
| NHS Shetland | 60.0% | 24.0 | 162.2 | 12.9% |
| NHS Tayside | 28.8% | 129.5 | 2,271.9 | 5.4% |
| NHS Western Isles | 33.3% | 25.7 | 194.7 | 11.7% |
| Scotland | 14.4% | 1141.3 | 28,731.9 | 3.8% |
Sessions lost to sick leave have decreased by 1.2 percentage points.