Residential rehabilitation settings - detoxification and other support available: survey findings
This report presents findings from a survey of residential rehabilitation providers in Scotland. It seeks to establish the current provision of detoxification across residential rehabilitation facilities and explores how these services operate and are governed.
3. Findings
3.1 Detoxification
Most of the residential rehabilitation facilities surveyed either require their clients to complete detoxification prior to entering the residential rehabilitation programme (25%, n = 7) or approach this on a case-by-case basis (39%, n = 11). About a third (36%, n = 10) do not require this of their clients.
Half of the facilities (50%, n = 14) offer a detoxification service. One facility responded that they also offer this service to other residential rehabilitation providers. Across these 14 facilities, detoxification is principally offered within the residential rehabilitation facility (79%, n = 11), although one facility reported providing this at a separate location. Due to the question format, it is not possible to conclusively determine whether the two remaining facilities offer this on-site or at a separate location.
Around a third of facilities (36%, n = 10) do not offer detoxification services but maintain either formalised or ad-hoc arrangements with detoxification providers.
Four facilities (14%) did not select any of the pre-defined response options but provided additional detail in open-text responses to this question. These facilities distinguished between detoxing from illicit drugs and reducing prescribed medication (e.g. methadone). Some of these providers reported that clients can do this by working with their prescriber while others work alongside community-based addictions teams or general practitioners to support clients in doing so.
3.1.1 Treatment and support
Facilities that reported offering detoxification were asked follow-up questions designed to better understand how they deliver this service. It should be noted that the percentages presented in this section of the report have a base of 13 facilities unless otherwise stated. One facility was re-coded during analysis as offering detoxification based on open-text responses, and was therefore not presented with the follow-up questions through survey routing at the time of completion.
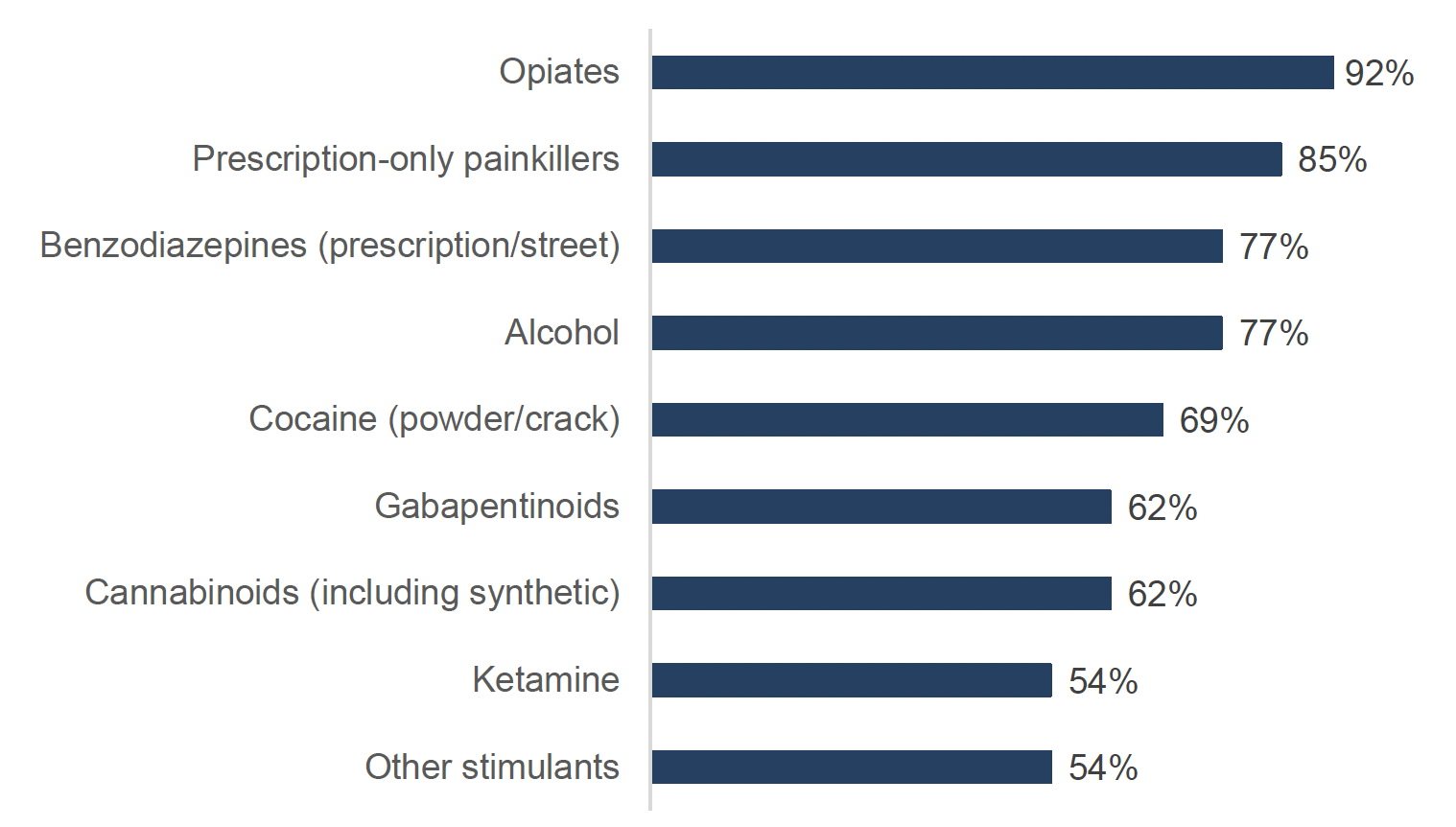
These facilities offer detoxification treatment for a range of substance use profiles (Figure 1). The most common substances for which detoxification is provided are for the use of opiates (92%, n = 12), prescription-only painkillers (85%, n = 11), alcohol (77%, n = 10), prescription or street benzodiazepines[6] (77%, n = 10) and crack or powder cocaine (69%, n = 9). One facility specified that clients can also be supported to reduce or stop prescribed medications or opioid substitution therapy.
Facilities are broadly evenly split between those that offer rehabilitation treatment to clients who will remain on medication assisted treatment (46%, n = 6) and those that do not (54%, n = 7). For those facilities that do, the most commonly used medications are injectable or long-acting buprenorphine and methadone.
3.1.2 Staffing
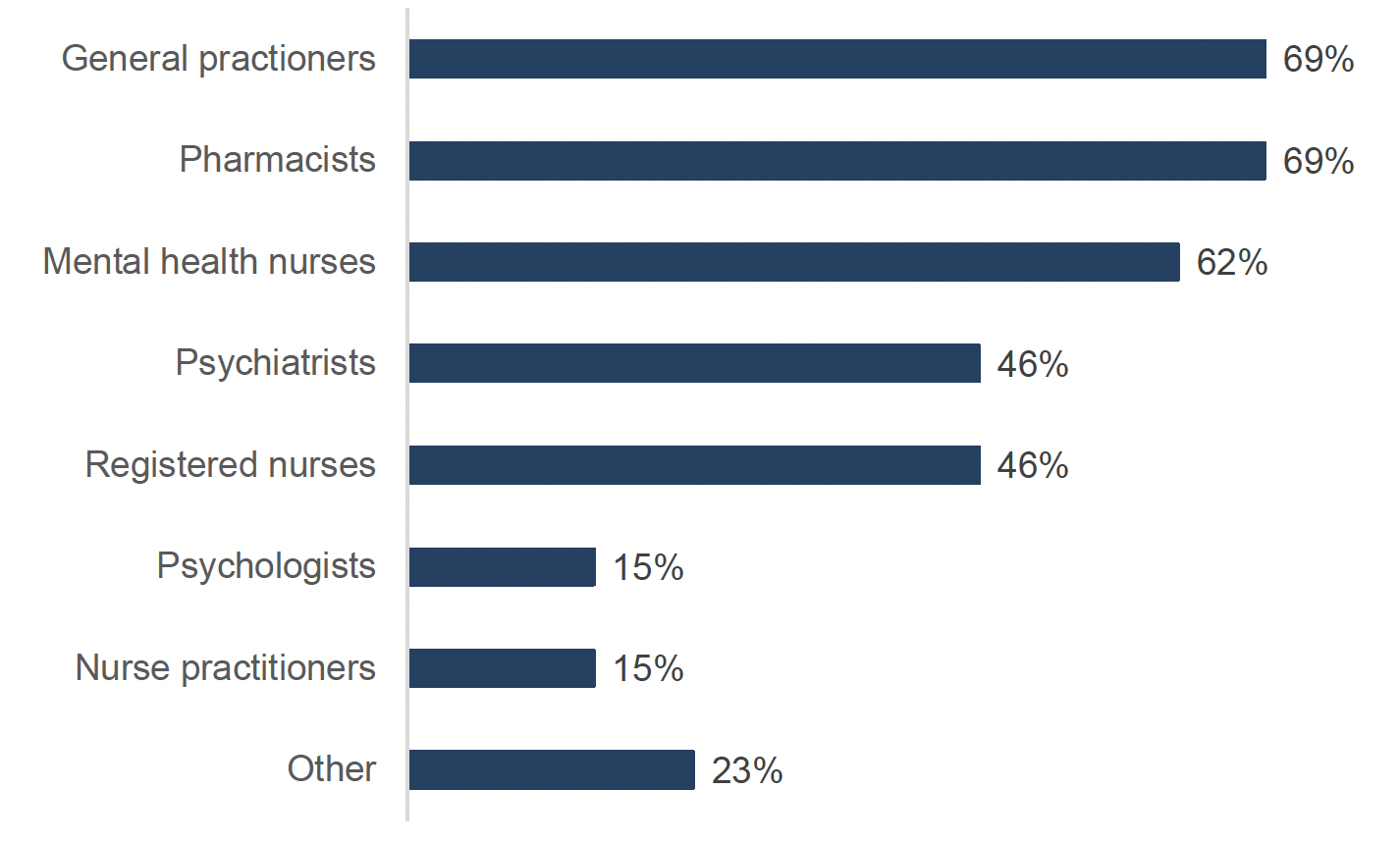
Clinical staff across a range of professions are involved in the detoxification service (see Figure 2). All but one facility reported involving more than one type of profession. The most commonly involved professions are general practitioners (69%, n = 9), pharmacists (69%, n = 9) and mental health nurses (62%, n = 8). Just under half of facilities reported that psychiatrists and registered nurses are involved (both 46%, n = 6). Psychologists and nurse practitioners are much less commonly involved in the detoxification service (both 15%, n = 2). Other professions involved include occupational therapists, therapists and physiotherapists. While not classed as clinical staff, a few facilities mentioned in open text responses that peer workers are also involved.
For the majority of these facilities, detoxification or assisted withdrawal is prescribed by a clinician directly employed by the residential rehabilitation provider (69%, n = 9). It is next most commonly prescribed by a clinician acting in a private (i.e. non-NHS) capacity contracted to the prescriber (31%, n = 4) or by community-based prescribers such as a client’s GP or a specialist alcohol and drug service prescriber (23%, n = 3). Additionally, 3 facilities (23%) access a client’s GP or other medical history before prescribing (2 of which rely on clinicians directly employed by the residential rehabilitation provider while the other uses a combination of privately contracted clinicians and community-based prescribers).[7] One facility noted that their contract with Glasgow Alcohol and Drug Partnership[8] (ADP) includes access to a doctor who prescribes and oversees detoxification for anyone referred through this pathway.
All facilities monitor detoxification and assisted withdrawal. This is carried out by clinical staff (54%, n = 7) or by non-clinical staff trained in the application of withdrawal rating scales (62%, n = 8). Two facilities (15%) indicated that they employ both. Among the six facilities without clinical staff on-site, three (50%) reported that a partner GP monitors progress through regular medication reviews or that a registered mental health nurse and GP visit the facility regularly on specific days of the week.
The majority of facilities use a standardised withdrawal assessment tool as part of their detoxification service (85%, n = 11). The most commonly used assessment tools were the Clinical Opiate Withdrawal Scale (COWS) and the Clinical Institute Withdrawal Assessment for alcohol and benzodiazepines (CIWA, CIWA-Ar, CIWA-B). Some facilities also mentioned using the Alcohol Symptom Severity Checklist (ASSC) or using a proprietary tool developed by the provider.
All of the facilities that responded to questions about their detoxification service (13) have a written policy in place for managing early discharge from the detoxification and residential rehabilitation service.
3.1.3 Governance and regulatory frameworks
All facilities operate within a regulatory framework[9]. Most are registered with the Care Inspectorate (71%, n = 10). A smaller number are registered with Healthcare Improvement Scotland (21% n = 3) or have internal NHS governance structures (14%, n = 2).
All facilities have governance arrangements in place for their detoxification service. Most facilities (62%, n = 8) are subject to external regulation or inspection by bodies such as the Care Inspectorate or Healthcare Improvement Scotland. The remainder are either managed directly by an NHS health board (23%, n = 3) or overseen by an internal clinical governance group (23%, n = 3). One facility reported that their detoxification service is governed by a private general practitioner. Only two facilities (15%) involve service users in the design or review of the service they provide.
3.2 Other forms of support or treatment offered
The survey asked questions aimed at better understanding the support or treatment delivered alongside residential rehabilitation and any detoxification services. Support is divided into that available for individuals prior to starting their residential rehabilitation treatment (pre-care), that available alongside their treatment (through care), and that available following discharge (after-care). All 28 facilities responded to these questions.
3.2.1 Pre-care support
Most facilities (79%, n = 22) offer some form of pre-care support or service, other than detoxification or assisted withdrawal, prior to a client starting the residential rehabilitation programme.
Facilities described a broad range of pre-admission support designed to psychologically or practically prepare clients for residential rehabilitation treatment and facilitate their transition into the programme. A person-centred approach is evident in both the type of support offered and how it is delivered. Several facilities noted that this preparatory work can extend for the duration of any time spent on a waiting list prior to entry, although some specified that it is only available once an individual is accepted onto the programme and on a waiting list. Different options were available, either through regular phone calls or in-person contact from dedicated pre-care or referral workers. Some facilities noted that the provision of a person-centred support plan can involve joint working with local alcohol and drug services or other services (e.g. mental health services).
This preparatory support can take a variety of forms, including early assessment, which is a key aspect of rehabilitation-readiness noted across the facilities. Many reported that they carry out initial screenings or assessments intended to help determine readiness, identify risks and inform the development of personalised preparatory plans.
A majority of facilities (61%, n = 17) reported that they carry out mental health and cognitive assessments of their clients.[10] Facilities that provided additional detail in a follow-up open text question indicated that these assessments are carried out prior to admission to determine whether an individual is ready to engage in the residential rehabilitation programme. A couple indicated that longer term monitoring takes place once a client is admitted. None of the facilities specified what tools are used to conduct these assessments.
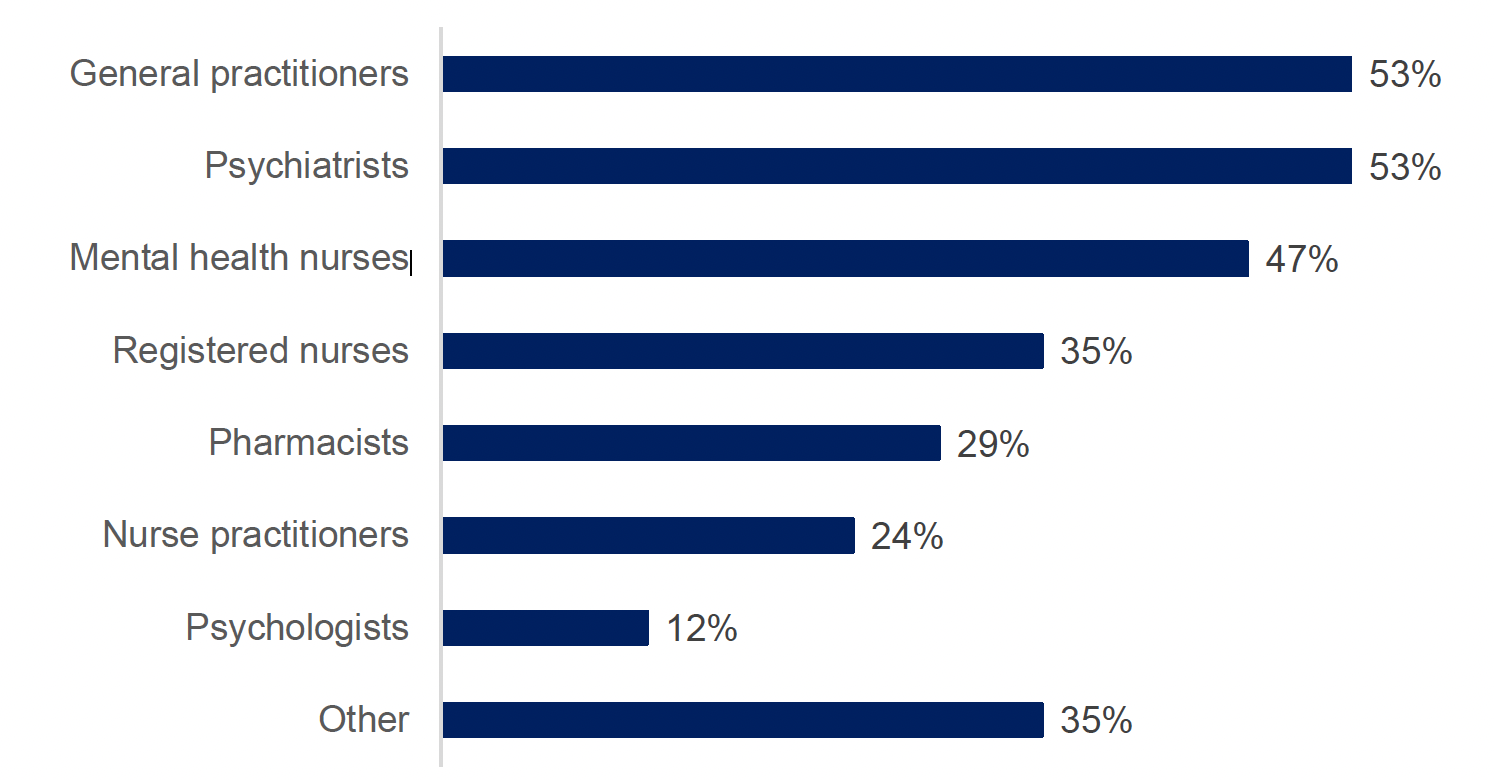
Clinical staff across a range of professions are involved in conducting these assessments (see Figure 3). Among the 17 facilities that carry out these assessments, the most commonly involved professions are general practitioners (53%, n = 9), psychiatrists (53%, n = 9) and mental health nurses (47%, n = 8). Psychologists are much less commonly involved in these assessments (12%, n = 2). Other professions involved include occupational therapists, counsellors and psychotherapists. While not clinical staff, a few facilities also mentioned recovery workers or peer bridge workers being involved in these assessments.
Almost half of the 17 facilities (47%, n = 8) reported involving two or more professions in assessments. Where only one profession was selected, this was most commonly a general practitioner (24%, n = 4). One facility reported that none of the listed professions are involved but did not provide additional information on who carries out the assessments.
Social support is another key component of pre-care support. This can take the form of one-to-one meetings, techniques such as motivational interviewing and information or orientation sessions to help people understand the expectations of the residential rehabilitation programme and the context in which it is to be delivered (e.g. living conditions). Some facilities arrange introductions to current residents (i.e. peers) to provide information about the programme, reassurance and reduce any anxieties about the move. Peer support groups were described by some facilities, noting that attending formal or informal meetings with peers can help people to build early connections and begin integrating into a recovery-orientated community prior to admission.
Finally, some facilities also noted that they engage with a client’s family members. This can take the form of family support workers or structured family groups and is aimed at strengthening support networks prior to admission.
3.2.2 Through-care support
Almost all facilities (86%, n = 24) reported providing a range of other support during a client’s stay, other than residential rehabilitation or any detoxification provided. The majority of the 28 facilities report offering family support (82%, n = 23) and mental health support (71%, n = 20). It was less common for facilities to offer medication assisted treatment prescribing (32%, n = 9). Other forms of treatment or support mentioned in open text responses were parenting or child-focused support, support with domestic violence, physical health assessment, management of chronic conditions and coordination with other services where needed, therapeutic and wellbeing activities (e.g. swimming, gym sessions) and life skills development (e.g. financial literacy, managing a home).
3.2.3 After-care support
All but one facility (96%, n = 27) report offering some form of after-care support in preparation for or following a client’s discharge from their residential rehabilitation placement. The only facility that does not offer this support directly is able to make referrals to community-based services. The most commonly offered types of support are peer support (82%, n = 23), housing support (68%, n= 19) and employability support (57%, n = 16).
Open text responses provided further detail on these categories of support, all of which aim to facilitate an individual’s reintroduction into the community and help them to sustain long-term recovery. Once again, a person-centred approach is evident in both the type of support offered and how it is delivered, which extends to flexible timeframes. There was a variation in the length of support offered across facilities, ranging from 3 months to 2 years, with some types of support appearing to be more open ended than others based on individual need. Many facilities indicated that a dedicated member of staff would help to develop an exit or support plan, which might include making connections or referrals with community-based services.
Many facilities combine one-to-one support with a more structured programme of group activities that can include a focus on relapse-prevention or life-skills development and can be delivered either in person or virtually. Peer involvement was a common feature of the support described, with peer mentors, volunteers or former residents helping to maintain a connection once an individual has returned to living in the community. More informal arrangements were also mentioned, such as drop-in sessions that former residents could use to seek support.
Several facilities reported offering supported or transitional housing, ranging from small move-on flats to larger recovery housing services or support with identifying suitable housing in the community. Practical assistance, such as helping with navigating benefits, appointments, employment, financial literacy or setting up a new home, were all described.
4. Considerations for future research
The results of this survey provide a high level understanding of the detoxification and other pre-, through- and after-care support available to people within residential rehabilitation settings. For future research, consideration could be given to exploring these services in greater depth with providers, including to better understand delivery models; the levels of need and demand; service user profiles; service user outcomes and associated facilitators and barriers. This would support better understanding of how the services are delivered and any potential gaps in provision.
In seeking to better understand these aspects of detoxification and pre-, through- and after-care, it would also be beneficial to complement service-level data by conducting research into the lived and living experiences of current service users, people seeking referral or access to these services and the people who support them (e.g. referrers and family members). This would allow for a more nuanced understanding of the needs and barriers experienced by people engaging with these services.
Annex A: Survey questions
A survey was developed by Health and Social Care analysts to gather information about the current provision of detoxification within residential rehabilitation settings. The survey also included questions about separate research into residential rehabilitation bed capacity in Scotland, expansion plans and placement funding status. These are not reported in this publication.
Survey questions related to the analysis presented in this report were:
1) Which, if any, of the following bodies is your residential rehabilitation facility registered with? Please select all that apply.
[multiple choice]
- HealthCare Improvement Scotland
- Care Inspectorate
- Internal NHS governance structures
- Other (please specify)
2) Does your service align with this definition of residential rehabilitation: “offering programmes which aim to support individuals to attain an alcohol or drug-free lifestyle and be re-integrated into society, and which provide intensive psychosocial support and a structured programme of daily activities which residents are required to attend over a fixed period of time”?
[single option, mandatory]
- Yes, completely
- Yes, in part
- No
- I don’t know
[If “yes, in part”, “no” or “I don’t know”]
3) How does the service you provide differ from the description above?
[open text, mandatory]
4) Do you carry out mental health or cognitive assessments with clients?
[single option]
- Yes
- No
[if yes]
5) Please specify which.
[open text]
6) Which of the following types of clinical staff are involved in these assessments? Please select all that apply.
[multiple choice]
- GPs
- Pharmacists
- Nurse practitioners
- Registered nurses
- Psychologists
- Psychiatrists
- Mental health nurses
- Other (please specify)
7) Are your clients required to complete detoxification prior to entering your residential rehabilitation programme?
[single option]
- Yes
- No
- On a case-by-case basis
- Other (please specify)
8) Do you offer detoxification services?
[single option, mandatory for survey routing purposes]
- Yes - we offer a detoxification service on-site (co-located with the residential rehabilitation facility)
- Yes - we offer a detoxification service and this takes place in another location to the residential rehabilitation facility
- Yes – and we also offer a detoxification service for other residential rehabilitation providers
- No we do not offer a detoxification service – but we have established links with detoxification providers
- Other (please specify)
[If any of the “yes” options]
9) For which substances do you offer detoxification or assisted withdrawal services? Please select all that apply.
[multiple choice]
- Alcohol
- Benzodiazepines (prescription/street)
- Cannabinoids (including synthetic)
- Cocaine (powder/crack)
- Other stimulants
- Gabapentinoids
- Ketamine
- Opiates
- Prescription-only painkillers
- None of the above
- Other (please specify)
10) How is detoxification or assisted withdrawal prescribed? Please select all that apply.
[multiple choice]
- Prescribed by clinicians directly employed by the residential rehabilitation provider
- Prescribed by clinicians acting in a private (non-NHS) capacity contracted to the prescriber
- Prescribed by community-based prescribers (e.g. patient’s GP or specialist drug/alcohol service prescriber)
- We access the individual’s GP or other medical history before prescribing
- Other (please specify)
11) How do you monitor detoxification or assisted withdrawal? Please select all that apply.
[multiple choice]
- Clinical staff on site do this
- Non-clinical staff on site are trained in application of withdrawal rating scales
- No clinical monitoring takes place
- Other (please specify)
12) Do you offer rehabilitation treatment to clients who will remain on medication assisted treatment?
[single option]
- Yes
- No
- I don’t know
[If yes]
13) Which medications are commonly used? Please select all that apply.
[multiple choice]
- Methadone
- Buprenorphine
- Injectable/long-acting buprenorphine
- Naltrexone
- Benzodiazepines
- Other (please specify)
14) Do you use a standardised withdrawal assessment tool as part of the detoxification service?
- Yes (please specify)
- No
- Other (please specify)
[if yes]
15) Please specify what withdrawal assessment tool you use.
[open text]
16) Which of the following types of clinical staff are involved in the detoxification service you offer? Please select all that apply.
[multiple choice]
- GPs
- Pharmacists
- Nurse practitioners
- Registered nurses
- Psychologists
- Psychiatrists
- Mental health nurses
- Other (please specify)
17) Do you have a written policy for managing early discharge from the detoxification/residential rehabilitation service?
[single option]
- Yes
- No
- I don’t know
18) What are the governance arrangements for your detoxification service? Please select all that apply.
[multiple choice]
- Managed directly by an NHS Health Board
- Overseen by an internal clinical governance group (e.g. a multi-disciplinary team or medical director)
- Subject to external regulation or inspection (e.g. Care Inspectorate, Health Improvement Scotland)
- Community prescribing is regulated by HSCP or community NHS services
- Involves service users in the design or review of the service
- Other (please specify)
[If “no” or “other” to Q8]
19) Do you have links with detoxification providers for your clients to undertake this process prior to starting their residential rehabilitation treatment with you?
[single option]
- Yes – formalised arrangements with external detoxification providers
- Yes – ad hoc arrangements with external detoxification providers
- No
- I don’t know
[If either of the yes options]
20) Please list the detoxification providers that you have links with.
[open text]
[Ask all]
21) Other than detoxification or assisted withdrawal, do you provide any other pre-care to residential rehabilitation treatment?
[single option]
- Yes
- No
- I don’t know
[If yes]
22) Please describe what pre-care is offered.
[open text]
23) During a client’s stay in residential rehabilitation: Other than any residential rehabilitation and detoxification you have already told us about, which other forms of treatment and support do you offer? Please select all that apply.
[multiple choice]
- Medication Assisted Treatment prescribing
- Mental health support
- Family support
- We do not offer any other forms of treatment or support
- Other (please specify)
[if any option other than “we do not offer any other forms of treatment or support]
24) Please provide more detail on what these other forms of treatment and support are.
[open text]
25) After a client has been discharged from their residential rehabilitation placement: Do you offer any of the following aftercare services? Please select all that apply.
[multiple choice]
- Housing support
- Employability support
- Peer support
- We do not offer aftercare support
- We do not offer aftercare support but we make referrals to community-based support services (please specify)
- Other (please specify)
[if any other option than “we do not offer aftercare support”]
26) Please provide more detail on the aftercare services you offer.
[open text]