Creating Hope Together: Year 2 Annual Report
This annual report from Suicide Prevention Scotland, covers progress on the second year of delivery of Scotland's Suicide Prevention Strategy, Creating Hope Together.
Appendices
Evaluation approach and methodology
The work set out in the appendices of this report has been carried out using a contribution analysis approach with all reporting being supported using an electronic recording system. This supports organisations to take a collaborative and outcome-focused approach to evaluation planning, implementation analysis and reporting. It is a theory-based approach to outcome monitoring, evaluation, learning and improvement that builds on contribution analysis.
Suicide Prevention Scotland has worked with evaluation experts to:
- Develop a theory of change (an outcome map) for the Creating Hope Together Suicide Prevention Strategy, informed by an understanding of the context in which it is operating.
- Agree pathways to impact that use this outcome map to show how Creating Hope Together activities contribute to its strategic outcomes, and what needs to be in place to make this happen, identifying clear change mechanisms by which the programme works.
- Collate and gather data to understand the action areas' early contributions towards the strategic outcomes and review this systematically against the stepping stones in the pathways.
- Summarise key findings against each of the six steps in the theory of change to tell the contribution story.
This report shows four pathways through the Creating Hope Together outcome map, one for each of the four Creating Hope Together strategic outcome. Each element, or 'stepping stone' of the pathways is colour coded. This provides a way to visualise Creating Hope Together's progress towards impact, and the confidence of the Delivery Collective in the strength of the data that supports this. The colour of each stepping stone shows the rating of progress towards impact, and the depth of the colour shows the confidence in the evidence.
| -- | Great Progress | Some Progress | No Progress |
|---|---|---|---|
| High Confidence | ■ High Confidence; Great Progress (dark green) | ■ High Confidence; Some Progress (dark amber) | ■ High Confidence; Low Progress (dark red) |
| Some Confidence | ■ Some Confidence; Great Progress (mid-green) | ■ Some Confidence; Some Progress (mid-amber) | ■ Some Confidence; Low Progress (mid-red) |
| Low Confidence | ■ Low Confidence - Great Progress (light green) | ■ Low Confidence - Some Progress (light amber) | ■ Low Confidence; Low Progress (light red) |
This makes it possible to see at a glance how the programme is progressing towards making an impact against its overarching outcomes and where the evidence behind this is stronger or weaker. It goes beyond a 'traffic light rating' of whether activities have been delivered (although an assessment of the delivery of activities against the delivery plan is also included in the body of the report) to provide an assessment of whether these actions are contributing towards the difference they were designed to make. Where a stepping stone has not been rated for progress and confidence, it shows as white. This is the case where all of the work behind it is still at the scoping stage, or very early in the delivery process, and we would not yet expect to see any impact. For example, if an activity to be included as part of 'What we do' has not yet been fully designed and delivery has not started, it would not be logical to expect that activity to yet have contributed towards 'What people do differently'.
This approach to assessing progress and confidence has been used across the actions in the Creating Hope Together action plan. The colour coding shown in this end of year report is therefore a collective rating that aggregates the action-level assessments of progress and confidence by outcome. This collective rating has been calculated for each stepping stone by assigning numerical values to each rating of progress and confidence (0= No rating, 1=Low, 2=Some, 3=High) and calculating the median across the individual reports from January 2025. Where the median falls between two ratings, the summary rating has been deciding using the following formula, which shares the scope of 2 equally across the three ratings:
<= 1.66 == Low > 1.66 & <= 2.33 == Some > 2.33 == High
At this early stage of a ten-year strategy, it would not be expected for Creating Hope Together to yet be making a strong, well-evidenced contribution to impact against all of its long-term overarching outcomes. Many of its actions are still in the scoping phase or early stages of delivery, and the impact of these will take time to be realised. This is reflected in the current colour-coding. The process will be repeated at regular intervals through the delivery of the strategy to track its growing impact and capture the development of a strengthening evidence base behind this.
Outcome 1
The environment we live in promotes conditions which protect against suicide risk – this includes our psychological, social, cultural, economic and physical environment.
What we do
| What we do: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Review data and information, and engage stakeholders to deepen understanding of the needs and challenges we are seeking to address | Great progress; high confidence |
| Bring people together to scope and define problems, agree priorities for action and co-design solutions | Some progress; some confidence |
| Provide guidance and support to policy makers so that they can support effective policy making in this area | Some progress; high confidence |
| Share evidence and learning on suicide prevention through events, reports and other channels and support people to put learning into practice | Great progress; high confidence |
| Develop and deliver a portfolio of accessible learning & development opportunities and resources | Great progress; high confidence |
| Work with local and national media to raise awareness about responsible reporting around suicide | Great progress; high confidence |
| Facilitate workshops and round table events with policy makers to share evidence, inform thinking and secure a commitment to action | Great progress; high confidence |
| Assess and identify how inequalities can and should be addressed through this work | Some progress; some confidence |
As outlined in detail in this report, we are confident that, overall, the Outcome is progressing well. There are some delays around Action Area 2 and work has slowed on Action Area 3 in the last quarter. However, planning is underway to progress this in line with the delivery plan in this year. The main barrier is where the scope of the ambition of the plan involves outside organisations, this has led to a slowing down of progress against the plan as we match up priorities.
| Action Areas towards Outcome 1 | Progress |
|---|---|
| Action Area 1: Whole of Government and society approach | On track in line with the delivery plan |
| Action Area 2: Access to means | On track in line with the delivery plan |
| Action Area 3: Media reporting | On track in line with the delivery plan |
Action Area 1: Whole of Government and society approach
We have gathered and reviewed evidence, data and information through the work of the Academic Advisory Group and the report commissioned from The Lines Between.
In order to identify priority areas for our Whole of Government and Whole of Society work we have carried out workshops with Scottish Government policy teams, the Public Health Scotland Suicide Prevention Network, and with The Lines Between themselves. In doing this we have focussed down onto the priority areas outlined in the ‘The Lines Between report’ and are beginning to scope solutions.
We have met regularly with the Suicide Prevention team at Scottish Government to monitor delivery against the commitments in Annex A of the Creating Hope Together Action Plan, supporting them to collaborate across government when appropriate.
We have shared learning from the ‘The Lines Between report’ and the work of the Academic Advisory Group with Strategic Outcome Leads and Delivery Leads to help shape the work more broadly.
Throughout the work we have been thinking about how we can identify and address inequalities that contribute to suicide risk. The evidence we have gathered will be our foundation for scoping and developing interventions that reduce suicide risk directly while addressing the inequalities that contribute to suicide risk.
Action Area 2: Action 2.1 - Locations of concern
Action 2 is progressing moderately, we have gathered evidence and carried out roundtables, drawing together learning and best practice from people across the country. This will contribute to our report from these workshops, which is still in draft, and PHS’ upcoming guidance on Locations of Concern.
We have concerns about our ability to use the learning from this work beyond helping to develop this guidance. The Action states that we will develop a national plan. We have outlined priority areas for action in our report developed from this work, however guidance is required about accountability and scope of a national plan to ensure that recommendations would be carried forward and delivered.
(Image caption: Engagement and gathering of best practice at the Locations of Concern workshops.)
Action Area 2: Action 2.2 - The Delphi Study
The Delphi study aimed to identify which evidence-based recommendations for the restriction of access to hanging and self-poisoning, could be realistically implemented to the real-world context. Within phase-two of this study, the Academic Advisory Group explored which of these recommendations were believed to be implementable in Scotland. Expert opinion was sought from residents of Scotland who were living with or have lived experience of suicide, Health Professions working in the field of suicide prevention and Academics of suicide prevention. Further support was provided by Samaritans.
Three leading recommendations for both restriction to means of hanging and self-poisoning were identified and are currently being explored for implementation in Scotland. The AAG learned that academics had differing opinions to the practitioners and the lived and living experience panel.
The findings are evidence-based, peer-approved and timely recommendations which reflect the views of key stakeholders of the target population. This greatly improves the likelihood of the success of these implementations, should they be implemented in Scotland.
Similarly to Action 2.1, appropriate channels now must be found to ensure this learning is shared more broadly and implemented.
Action Area 3 - Media reporting
This action has progressed well, with some areas needing further development. Samaritans Media Guidelines training sessions have been delivered to journalists and media professionals, including a session at BBC Scotland to Local Democracy Reporters. These journalists are part of a scheme where they receive training and support from the BBC, but are working for local newspapers. This meant we were able to train and speak to reporters from across Scotland, who are at the start of their careers, to embed suicide safe reporting in their practice early on. A session was also delivered to journalists from different outlets – print, online and TV – in Inverness. This session was set up in partnership with local Suicide Prevention Leads and hosted by Police Scotland.
Our Media Guidelines Training has also been delivered to people working locally on suicide prevention in three online sessions organised by the Suicide Prevention Implementation Leads and including Electrify.
As well as media professionals and those working on comms and with media locally, training has been delivered to groups of elected Councillors and MSPs and staff across The Scottish Parliament.
Learning from Year 2 delivery
Action Area 1: Whole of Government and Society approach
We have developed an evidence base on which to build our work on the Whole of Government and Whole of Society approach as laid out in our Prioritisation Framework. These are encapsulated in The Lines Between report and the two studies carried out by the Academic Advisory Group.
We believe the most effective areas for intervention will be:
- Poverty – The extent of intersecting risk factors across the different components of economic and social disadvantage suggests that successful work in this area could make a significant contribution to suicide prevention.
- Alcohol and substance misuse – The severity of increased suicide risk among those who misuse alcohol and/or other substances leads us to believe that this should also be an area of focus. Furthermore, the intersectionality with economic disadvantage and mental health enables a wider holistic approach that could align with wider work on poverty.
- Children and young people – Recent statistics suggest an increasing proportion of suicides are accounted for among children and young people. Taking steps to reduce and reverse this trend should be a priority area of work, with schools, colleges and universities providing potential settings to initiate activity.
In addition to the policy areas identified above, the Lines Between report recommends three thematic areas of focus. These are:
- Stigma and discrimination
- Transitions and life changes
- Isolation and loneliness
We will build on this by scoping interventions that can have an impact in these areas.
Action Area 2: Action 2.1 - Locations of concern
We have gathered the views of stakeholders in key locations across Scotland working directly on Locations of Concern. We will take the learning and feedback from these sessions to produce a final report, feed into Public Health Scotland guidance, and better understand our approach to a national plan.
Action Area 2: Action 2.2 - The Delphi Study
Three leading recommendations for both restriction to means of hanging and self-poisoning were identified and are currently being explored for implementation in Scotland.
The findings are evidence-based, peer-approved and timely recommendations which reflect the views of key stakeholders of the target population. This greatly improves the likelihood of the success if these recommendations were implemented in Scotland.
Action Area 3: Media reporting
We have learned more about the needs of local suicide prevention teams in terms of working with local media. We have adapted our work to support local teams and will continue to do this in year 3. Through our locations of concern workshops we also learnt about the challenges that media can bring in tackling suicide at locations of concern. There was a lot of discussion of social media as a newer source of spreading poor reporting and where unhelpful discussion of suicide can happen. We are now assessing how we might work to address this in year 3.
Who with
| Who with: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| People developing and implementing policy relating to inequalities and social determinants that impact on suicide at local and national levels | Some progress; high confidence |
| People and organisations whose work contributes to addressing inequalities and social determinants that impact on suicide | Great progress; some confidence |
| Suicide Prevention Scotland Delivery Collective | Great progress; high confidence |
| People working with people at risk of suicide or affected by suicide | Some progress; some confidence |
| People and communities with lived and living experience of suicide or the inequalities and or social determinants that impact on suicide | Some progress; some confidence |
| Local and national media across Scotland | Some progress; high confidence |
Through engagement activities around Action 1.1 - Whole of Government and Society approach, we have spoken to all groups we had planned to within the desired timeframe. For Action 2.1 - Locations of concern, we reached most of the stakeholders with whom we wanted to consult in the timeframes we wished to. We were especially pleased with cross sector engagement in different regions across Scotland, including from the third sector and Police Scotland. The group we wished to consult with further but who did not attend our engagement events were groups responsible for infrastructure e.g. BEAR Scotland, Transport Scotland, ScotRail.
Engagement for Action Area 3 - Media reporting reached more stakeholders than we had initially set out to, as there was great interest in the media training from non-media professionals who engage with media and perhaps release statements on suicide. However, we did not have as much engagement from national media as we had hoped. This is due to understaffed newsrooms and journalists having no time to take any training. We were still able to speak to larger newspapers and remind them of our guidelines for reporting suicide, and will adjust our plans for year 3 to look at how we can ensure larger outlets are receiving some kind of training from us.
In year 2, as part of outcome 1 engagement work, we engaged with:
- 3 research teams: The Lines Between; University of Manchester; University of Strathclyde.
- 2 bodies of elected representatives: Elected Councillors from Highland Council; Members of Scottish Parliament.
- 14 public bodies and health boards: Falkirk HSCP; Fife HSCP; Glasgow City HSCP; NHS Ayrshire & Arran; NHS Borders; NHS Dumfries & Galloway; NHS Forth Valley; NHS Greater Glasgow & Clyde; NHS Tayside; Police Scotland; Public Health Scotland; Scottish Prison Service; West Lothian HSCP; West Dunbartonshire HSCP.
- 17 commissioned service providers, voluntary sector and community groups: Citizens Advice Scotland; Change Mental Health; Crisis; Gamble Aware; Health in Mind Scotland; James Support Group; Joseph Rowntree Foundation; Mental Health Foundation; Mikeysline; Poverty Alliance; Queer Futures; RABI; Samaritans; Shelter Scotland; Survivors of Bereavement by Suicide (SOBS); The ALLIANCE; The Trussell Trust.
- 14 teams in national and local government: Scottish Government teams working on health inequalities; child poverty; employability; dementia; unpaid carers; Fair Work; veterans; building standards; and volunteering. COSLA; Scottish Borders Council; North Lanarkshire Council; Suicide Prevention Implementation Leads; Suicide Prevention local leads from across Scotland.
Priorities for engagement in Year 3
Action 1.1 - Whole of Government and Society approach
Our priorities for Year 3 are engaging with anyone involved in the development and implementation of interventions that impact on the priority areas identified through our work so far. By engaging with these groups, we will scope out proposals to be carried forward into the next action plan.
Action 2.1 - Locations of concern
We will engage with Public Health Scotland to ensure learning on locations of concern is taken into account in development of future resources.
Action 2.2 - The Delphi Study
We will engage with Scottish Government in planning next steps for implementation of recommendations from the Delphi Study.
Action 3 - Media reporting
More media engagement, engaging with journalism and media students to train the journalists of tomorrow, and continuing to engage with people who are likely to speak publicly about suicide.
How they feel
| How they feel: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| That suicide prevention is important, effective, will benefit everyone, and requires a holistic approach | Some progress; some confidence |
| People and / or organisations see how they can contribute to preventing suicide and are inspired to play their part | Some progress; some confidence |
| Safe, listened to, valued, included, encouraged, supported, and empowered | Great progress; some confidence |
| Policy makers feel heard, understood and understand how this can help their work | Some progress; some confidence |
Participant feedback shows positive engagement from those engaging in the work, with people valuing the opportunity to come together and share perspectives and best practice. For example, workshops participants told us:
'[I found [it] interesting and helpful using the lens of the cross-cutting areas... [a] focus on protective factors helps to see more practical interventions going forward.' (Participant in the workshops for policy teams)
‘Well-paced supportive environment & helped draw out a wide range of experience’ (Locations of Concern workshop participant)
‘...good to hear areas of good practice/what's happening in other Health Boards/ Local Authority Areas’ (Locations of Concern workshop participant)
‘It’s been great to meet all these wonderful people making a difference- this is a subject close to my heart & I am keen to help and make a difference.’ (Locations of Concern workshop participant)
What they learn and gain
| What they learn and gain: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| We understand the context for implementation and what this means for effective delivery | Some progress; some confidence |
| Understand existing good practice, gaps, what needs to change, the priorities for action and possible solutions | Great progress; some confidence |
| Media understands its role in suicide prevention | Some progress; some confidence |
| Awareness of suicide, risk factors, and understand what to do to prevent suicide and tackle associated inequalities and social determinants | Some progress; high confidence |
| Tested interventions, approaches, services and supports that are effective in preventing and responding to suicide | Some progress; some confidence |
Action Area 1: Whole of Government and Society approach
We have regular meetings with Scottish Government Suicide Prevention Policy Team to include them in the work and keep them updated on the progress. We have developed a plan for them to use the Comms Pack we have developed to work with teams across Scottish Government to improve awareness of how Creating Hope Together can support their work and how they can contribute to suicide prevention.
We have engaged academics and stakeholders on social determinants and are starting to plan our next steps around prevention and intervention measures. The progress is great for where we are in the work.
Although we are yet to test any interventions or approaches, we are on track in delivering the prioritisation framework. When we get to the Develop and Deliver stages of the framework, we will be exploring interventions that could be effective in preventing suicide.
Action Area 2: Access to means
Workshop participants from our pilot workshop in West Lothian provided feedback that suggests they gained knowledge on the appropriate approaches to address Locations of Concern (LOC). Follow up emails showed knowledge of good practice around the sensitivity of sharing information in relation to LOC being gained and shared.
Additionally, case studies of local LOC work have been widely shared through the Suicide Prevention Implementation Leads who attend local area steering groups including LOC specific groups and share knowledge of practice in other areas and the evidence base.
Action Area 3: Media reporting
Samaritans Media Guidelines training not only gives practical tools for reporting on suicide, it also provides evidence and knowledge on the impact of irresponsible reporting and even the impact the way we talk about suicide can have. At the end of each session there has been positive feedback and questions from participants. Feedback from the Inverness session with Council members was very positive and showed that the perception of suicide had been challenged and that the members left the session seeing things in a different way and would ensure that they talk about suicide in a better way in the future.
Case study: Whole of Government suicide prevention policy work, with a focus on inequalities and marginalised groups (Outcome 1, Action 1.1)
What we have done:
In year 2, we have been focusing on policy areas where actions focus on integrating or mainstreaming suicide prevention activity.
We have had a key focus on ensuring suicide prevention work is addressing the Gypsy/Traveller community, as one of the most marginalised groups in Scotland.
Who with:
Working with Samaritans, we brought these policy areas together to discuss how they could shape their policy actions, integrating suicide prevention.
38 officials joined our workshops from Scottish Government, COSLA and Public Health Scotland, across policy areas including: Mental health The Promise Migration and population diversity Child poverty Fair Work Adult Support and Protection
Members of our team were involved in cross- government conversations and forums that have shaped the Mental Health comments in the 2024-2026 Gypsy/Traveller Action Plan.
How they feel:
A policy workshop participant told us:
‘[It’s] good to have an opportunity to break out of siloes. [It] helps broaden the way we think.’
What has been learned:
There is increased awareness of the deep policy collaboration required to achieve the shift to integrate and mainstream suicide prevention considerations in policy work across government, and in areas covering some of the sharpest inequalities, such as homelessness, substance use, violence, experience of care, and prison.
For example, the 2024-2026 Gypsy/Traveller Action Plan includes actions to improve access to suicide prevention and self-harm training for staff working with Gypsy/Travellers and to build our understanding of the risk of suicide in Gypsy/Traveller communities.
What is being done differently?
The Suicide Prevention Policy Team is at the centre of active cross-government work exploring how closer connectivity between policies and services can improve response for people experiencing Severe and Multiple Disadvantage.
For example, work on the Gypsy/Traveller Action Plan kickstarted conversations about reciprocal training between two partner organisations, MECOPP and Penumbra. They facilitated a session for Suicide Prevention Independent Leads and are looking to speak with stakeholders in health boards to do the same.
What difference will this make?
In addition to other poor outcomes, experiencing severe and multiple disadvantage can create extreme vulnerability and heightened risk of suicide and other preventable deaths. We are working towards a policy environment that accounts for and responds to these inequalities and the crucial connections between them.
What they do differently
| What they do differently: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Work with wider stakeholders and partners to prioritise, plan, commission and deliver the work | Some progress; some confidence |
| Take action to prevent suicide and tackle the impact of inequalities and social determinants that impact on suicide | Some progress; some confidence |
| Organisations take action in partnership to restrict access to methods of suicide | Some progress; high confidence |
| Traditional media recognise and implement best practice in sensitively reporting, discussing and portraying suicide | Some progress; low confidence |
| Use quality data and appropriate evidence to inform priorities, develop interventions and make effective decisions | Great progress; some confidence |
| People and organisations play their part in scaling up and embedding effective interventions | Some progress; some confidence |
Action 1.1 - Whole of Government and Society approach
We are positive and hopeful, based on our engagement and experience so far, that the work on this action will contribute to meaningful change. We have found policy makers to be receptive and eager to learn from our scoping work into the social and environmental factors that contribute to suicide risk.
Our work so far has focussed on scoping policy areas, prioritising based on the evidence, and engaging to inform our decision making around the priority areas.
The next phase will look at interventions in these specific areas. This will provide recommendations and best practice examples to those designing and making policy. We know that there is a willingness to change and improve practice, behaviours, systems and policies in order to reduce suicide in Scotland, and our aim through this work is to provide evidence and guidance to assist that change.
Action 2.1 - Locations of concern
Our work on Locations of Concern has brought together voices of those working in suicide prevention in areas across Scotland where there are known locations of concern. By collecting their experience and evidence, we can see that there needs to be change in many areas. Some of this is more straightforward, such as learning which physical interventions can be placed on structures when they are built to ensure the location is not accessible as a means. Then using this information to inform planning and building, where we hope policy makers at a national and local level will utilise our evidence. But areas where we have less influence and access, such as data sharing between agencies is a slower and more complicated process.
Action 3 - Media reporting
For this action, a wider change to how the media operate is not achievable by us alone. However, through our work on Creating Hope Together, we hope to influence individual reporters and the journalists of the future. This could have an impact on local reporting and could contribute to more responsible reporting of suicide on a larger scale in the future.
Another target for this work is people who speak to the media about suicide, such as politicians and spokespeople for emergency services. By equipping them with the most responsible language and helpful ways to talk about suicide, we can change reporting to ensure it is safer.
What difference does this make?
| What difference does this make: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Outcome 1: The environment we live in promotes conditions which protect against suicide risk. | Some progress; some confidence |
Our early contribution towards achieving Outcome 1:
The aims of Outcome 1 are broad and ambitious. We are pleased with the progression and reception of our work across the actions so far and anticipate that the range of work being delivered will contribute a great deal to making the environment and society we live in safer and help to reduce suicide in Scotland.
We believe there has been some progress towards the overall outcome across the actions. For many of the actions we have completed initial scoping and planning and will be moving into delivery in the coming year. This will mean we are likely to have further examples in the year to come.
Action 1.1 - Whole of Government and Society approach
Overall, it is hard to code many stepping stones in this column as green due to the timescale, which is to be expected at this stage. Our work is to engage with stakeholders to change their behaviour and practice over time. However, based on the engagement and response so far, we are making good progress in this area.
Action 2.1 - Locations of concern
Similarly, we are at an early stage of work that could take many years before we see impact. Additionally, the scale of the work and the number of bodies who need to be influenced is vast. In some areas this progress will be quicker and easier where we have existing positive relationships with the relevant stakeholders, in other areas, we will need to develop new relationships in order to progress work.
Action 3 - Media reporting
The ability for journalists and others working across media to attend training is limited due to the demands on their time. This has caused a delay in the original plan to focus training on these groups; however, good progress has been made with local media, local spokespeople and future journalists.
Across all actions under Outcome 1, the main challenge is where progress or delivery depends upon external organisations prioritising suicide prevention. We have made great progress in engagement and collaboration externally and have successfully been able to highlight suicide prevention as being relevant to others’ work, even when not immediately obvious. However, ongoing influencing is needed to ensure recommendations stemming from our work is considered by external organisations.
Outcome 2
Our communities have a clear understanding of suicide, risk factors and its prevention – so that people and organisations are more able to respond in helpful and informed ways when they, or others, need support.
(Image caption: This colour-coded outcome map shows our theory of change for outcome 2 and our assessment of early progress towards it, including our confidence in the evidence we have to support this. This information is broken down in each section of the report that follows. The whole map can also be viewed more clearly online here.)
What we do
| What we do: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Review data and information, and engage stakeholders to deepen understanding of the needs and challenges we are seeking to address | Some progress; high confidence |
| Share evidence and learning on suicide prevention through events, reports and other channels and support people to put learning into practice | Some progress; high confidence |
| Support and foster the continued development of the suicide prevention social movement | Great progress; high confidence |
| Run co-ordinated suicide prevention campaigns for the public and targeting high risk groups | Some progress; some confidence |
| Develop and deliver a portfolio of accessible learning & development opportunities and resources | Great progress; high confidence |
| Provide training, guidance, tools and resources and support workforce development to support staff to respond compassionately and effectively | Some progress; some confidence |
| Embed a process of continual learning and improvement | Some progress; some confidence |
| Assess and identify how inequalities can and should be addressed through this work | Some progress; some confidence |
Overall, we are happy with progress under Outcome 2. Six of the eight actions are on track. The two which are behind schedule, are underway with plans in place and minimal risks against completion. Collaboration and information flow between the Outcome Lead and action leads is continually improving. Engagement with stakeholders during the scoping and development phases has gone to plan and been beneficial and effective. This has established a good base for future wider engagement with communities and community organisations.
| Actions towards Outcome 2 | Progress |
|---|---|
| Action 4.1: Social movement, campaigns and anti-stigma | On track in line with the delivery plan |
| Action 4.2: Learning resources | Behind schedule against the delivery plan |
| Action 4.3: Whole school approach to mental health | Scoping work in progress |
| Action 4.4: Develop age-appropriate school resources | Scoping work in progress |
| Action 4.5: Pre-registration training | Scoping work in progress |
| Action 4.6: Suicide prevention online portal | On track in line with the delivery plan |
| Action 4.7: Provide information in different formats | Scoping work in progress |
| Action 4.8: Help seeking and help giving | Behind schedule against the delivery plan |
Action 4.1 – Social movement, campaigns and anti-stigma
Three Stories of Hope films that tell the story of members of the United to Prevent Suicide movement have been produced and have reached over 10,000 people through our social media channels. The films show how people in the movement are helping to create hope for themselves and others. Our World Suicide Prevention Day content also reached around 35,000. A programme to re-engage with members included three in-person and three remote events and an online survey, in which over 100 people shared their views and ideas to inform our work in 2025-26.
The campaign development is progressing as planned with Electrify leading a co-production process which will result in a long-term series of continuous suicide prevention public awareness campaigns. People with lived and living experience are driving the production process. Creative development and campaign testing are running to schedule with launch planned for mid-April 2025. This action is aligned to the complementary Action 4.6 (Portal development) and opportunities for synergy between both are being identified and managed.
See-me led a Stigma and Discrimination session with representatives from the Suicide Prevention Scotland delivery collective in November 2024 to inform development of a framework for action. Mapping of stigma initiatives contributing to the Creating Hope Together strategy is underway. This and other information sources, like the soon to be published scoping review on suicide-related stigma, will help identify next steps for 2025/26.
Action 4.2 - Suicide prevention learning approach
The review of the mental health and suicide prevention learning provision in Scotland was published in October 2024. The review recommendations are being considered by Scottish Government prior to developing an implementation plan, which will enable findings relevant to suicide prevention to be taken forward.
NHS Education Scotland (NES) and PHS have revised the informed level Ask/Tell/Respond modules to enhance learner experience and to meet accessibility criteria. Between relaunch in September 2024 and March 2025, 2,306 learners engaged with the refreshed Ask, Tell, Respond eLearning modules with a completion rate of 82%.
An evaluation of the Ask, Tell Respond informed and skilled level facilitation resources was undertaken which demonstrated positive support for the facilitator model. The recommendations will be used to develop an action plan in collaboration with the Facilitator Network.
NES have continued to engage with the unscheduled care working group to understand how work being delivered by different groups and organisations links together. NES are working towards finalising the Health Inequalities eLearning module. The module will be informed by the experience and learning of the See Me team, specifically in relation to intersectionality, stigma and discrimination linked to mental health and inequalities.
NES delivered one webinar on self-harm and non-suicidal self-injury in young people, attended by approximately 300 people, and another webinar in collaboration with Scottish Women's Autism Network titled Understanding and working with autistic individuals in mental health and suicidal crisis, which was attended by approximately 600 people.
Delivery of the Livingworks programmes has also continued with a focus on key target groups.
Action 4.3 – Whole school approach to mental health
Action 4.4 – Develop age-appropriate school resources
Action 4.5 – Pre-registration training
All three inter-dependent actions are in the scoping and planning stage, with ongoing engagement with stakeholders to identify opportunities and approaches to engage and influence effectively. Suicide Prevention Scotland has clear objectives for each action, however, has limited control over the plans and timelines of other stakeholders at this stage.
Action 4.3 has been informed by the Insight Report (Understanding suicide risk and behaviour amongst children and young people and the effectiveness of interventions) and focuses on education, youth work, and higher and further education settings.
In the education setting there has been progress towards influencing the inclusion of suicide prevention in the work plan of the Joint Scottish Government / COSLA Mental Health in Schools Working Group. The group’s terms of reference commits to considering suicide prevention, and a scoping activity was undertaken in December 2024 to explore opportunities to integrate suicide prevention into the continuum of mental health. Next steps are to work with Scottish Government and COSLA officers to identify ways to embed suicide prevention in the group’s workplans.
Engagement to understand the needs of the Association of Directors of Education in Scotland (ADES) and the Association of Scottish Principal Educational Psychologists (ASPEP) in relation to suicide prevention is ongoing. Engagement with Education Scotland, through their Safeguarding Leads Network, highlighted the need for support and pathways for staff and pupils on the topic of mental health, inclusive of suicide prevention.
Through work with local Suicide Prevention Leads, third sector colleagues, Education Safeguarding Leads and Community Mental Health and Wellbeing Framework Leads, five practice stories of suicide prevention being embedded in the whole school approach have been captured. These are being developed into a learning resource which will be accompanied by a podcast.
Addressing inequalities is being considered across all of this work, with engagement taking place with e-Sgoil (national e-learning service), people working in LGBTQ+ education, and with Celcis (the Centre for Excellence for Children's Care and Protection) who hold a virtual head teacher programme to understand practices for those who do not attend school in person.
In the youth work setting, meetings have taken place with Youthlink Scotland and Youth Scotland to discuss suicide. Youth Scotland highlighted the opportunity to embed suicide prevention in their training program for new youth workers, and PHS have been engaged to establish if the Ask and Tell resources can be tested.
As part of Youthlink Scotland’s annual conference on 5th November 2024, a workshop titled Raising Awareness of Suicide Prevention was facilitated by Children in Scotland and Suicide Prevention Scotland. This introduced Suicide Prevention Scotland’s Youth Advisory Group (YAG) and focused on the needs of young people in suicide prevention. Three workshops were held reaching 35 people. The workshop used case studies (developed by YAG) to help participants understand the stages of suicide prevention and how, in their role as youth workers, they can play an active role. Feedback was positive, including from COSLA spokesperson Councillor Buchanan.
Youth Links No Knives Better Lives program is developing training for youth workers about suicide prevention alongside Medics Against Violence and a training framework and other resources have been shared.
In the higher and further education setting, work was undertaken with the National Union of Students (NUS) Scotland to update their Think Positive Hub with the training and support available for staff and students about suicide prevention. The student mental health agreement now also addresses suicide prevention.
A national network for colleges and universities focused on suicide prevention was established with support from Universities Scotland, Colleges of Scotland, and the Association of Managers of Student Services in Higher Education (AMOSHE). The network agreed their terms of reference in December 2024, and the meeting benefited from inputs from EmilyTest’s work in universities and colleges. PHS discussed the role of local Suicide Prevention Leads and how universities and colleges can connect with them. Feedback received from network members noted the value they saw in having a space to get support from their peers and to share practice.
Strathclyde University’s suicide prevention action plan advisory group met four times in 2024, and part of their focus going forward will be on sharing learning with other colleges and universities. The Student Mental Health Action Plan was published and a structure will be created to oversee implantation which will ensure suicide prevention is considered.
For action 4.4, positive engagement has taken place with Education Scotland colleagues working on the Personal & Social Education (PSE) review as a key opportunity to embed suicide prevention within the curriculum. The review will be teacher-led and at this stage and we are building clarity on how the Creating Hope Together Strategy commitments will be taken into account by the review.
Suicide prevention data was shared with Education Scotland and the CYP Delivery Lead attended the PSE leads network in February to discuss their review and understand their views on what suicide prevention support could look like. Education Scotland (who lead the network) made a request for suicide prevention curriculum resources to be provided, in preference to individual teachers creating their own resources.
For Action 4.5 a process has been developed to map where suicide prevention is included in existing pre-registration courses in Scotland, and to what extent. The mapping will help prioritise professions to focus on in 2025/26 where suicide prevention can be strengthened within their curricula. This approach should also help identify areas of good practice which can be documented and used to advocate for wider inclusion of suicide prevention in pre-registration courses for health and social care professions, youth work and teaching staff.
Action 4.6 Suicide Prevention online portal
Development of the Suicide Prevention Scotland Online Portal is on track, with launch of a minimum viable product scheduled for mid-April 2025, and launch of the 'final' product schedule for end May 2025. This aligns to the campaign development timeline under Action 4.1.
Ember Technology Limited, a Fife based company, have been contracted to develop the portal. A working group, with representation from across the Suicide Prevention Scotland Delivery Collective, has been established to inform and guide the development process. A process is underway to develop a directory of suicide prevention services available to people in Scotland. It has been agreed with Scottish Government that SAMH will be responsible for portal management and administration post-development, with the intention to transition the site to a public sector hosting environment in the longer term.
Action 4.7 Provide information in different formats
This action is in the early scoping stage and will be taken forward in 2025/26 in partnership and dialogue with community-based organisations.
Action 4.8 – Help seeking and help giving
Under this action we have reviewed research and data and engaged in consultations to inform a report that will improve understanding of help-seeking/help giving behaviours in Scottish residents when experiencing suicidal ideation. The Academic Advisory Group undertook a rapid review of help seeking and help giving and their paper "Understanding help giving and help seeking behaviours in Scottish residents when experiencing suicidal ideation: A rapid review" was published in February 2024.
Consultations took place as conversation café topics at CHT Conference March 2024, with a focus on the following topics: Men; Women; LGBTQ+; Race & Ethnicity; Neurodiversity; Children & young people; Faith & belief; Substance misuse; Gambling, Care Experience. Consultation sessions were also held in May and June 2024 with the Lived and Living Experience Panel, the Participation Network, the Suicide Prevention Scotland Network, and the Youth Advisory Group.
Following a pause due to staff departure/recruitment this work was picked up again as of November/December 2024, with further inputs and guidance sought to develop useful guidance, which will be available in 2025-26.
Who with
| Who with: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| People developing and implementing policy relating to inequalities and social determinants that impact on suicide at local and national levels | Some progress; some confidence |
| People and organisations whose work contributes to addressing inequalities and social determinants that impact on suicide | Some progress; some confidence |
| Suicide Prevention Scotland Delivery Collective | Some progress; some confidence |
| People working with people at risk of suicide or affected by suicide | Some progress; high confidence |
| People and communities with lived and living experience of suicide or the inequalities and or social determinants that impact on suicide | Great progress; high confidence |
| Interested members of the public in Scotland | Great progress; high confidence |
Engagement under Outcome 2 has been going well, leading to meaningful and inclusive collaboration across a number of actions.
People with lived and living experience have been engaged throughout campaigns develop and in social movement initiatives, and campaigns testing will involve a wider group of stakeholders. Scoping and planning for actions focusing on school systems and professions have engaged a significant number of stakeholders to date.
To date all parts of the Delivery Collective and representation from the key stakeholder groups have been involved in the portal development process. Consultation meetings were held with the Lived and Living Experience Panel (LLEP) and the Youth Advisory Group (YAG), and survey feedback was provided by: PHS; University of Edinburgh and University of Glasgow staff; 13 respondents from HSCP/Local Authorities; 8 NHS Board members; 6 respondents from Police Scotland; and representatives of the following organisations: Highland Third Sector Interface, James Support Group, Scottish Recovery Network, SAMH, Action for Children, VOX, Papyrus, With YOU, Samaritans and Change Mental Health. A portal working group has been established to guide and advise on the development process and will be directly involved in establishing a resource identification and approval process, coordinating user testing and advising on launch and promotion.
Across the actions working towards outcome 2 this year, we engaged with:
- 2 research teams: University of Edinburgh; University of Glasgow.
- 4 panels of people with lived and living experience: The Lived and Living Experience Panel; the Participation Network; VOX Scotland; the Youth Advisory Group.
- 3 professional networks and membership organisations: NUS Scotland; Universities Scotland; Youthlink Scotland.
- 16 public bodies, health boards, and health and social care partnerships (HSCPs): Clackmannanshire/Stirling HSCP; Dundee HSCP; East Dunbartonshire HSCP; East Renfrewshire HSCP; Education Scotland; Falkirk HSCP; Fife HSCP; NHS 24; NHS Ayrshire & Arran; NHS Education Scotland (NES); NHS Forth Valley; NHS Lanarkshire; NHS Greater Glasgow and Clyde; Police Scotland; Public Health Scotland; West Lothian HSCP.
- 16 commissioned service providers, voluntary sector and community groups: Action for Children; Association of Directors of Education in Scotland; Association of Scottish Principal Educational Psychologists; Change Mental Health; Children in Scotland; Cruse Scotland; Highland Third Sector Interface; James Support Group; Papyrus; Penumbra Mental Health; Samaritans; Scottish Association for Mental Health (SAMH); Scottish Recovery Network; VOX; withYOU; Youth Scotland.
- 6 teams in national and local government: COSLA; Edinburgh City Council; East Ayrshire Council; Highland Council; Highland Council (Whole Family Wellbeing Programme); Highland Council (Community Planning Partnership).
For Outcome 2 to be successful wide engagement with communities is essential. The engagement undertaken to date will be built on in year 3 particularly post-development and testing of the campaigns work and the portal, and through scoping and implementation of Action 4.7, where community organisations will be more directly involved.
How they feel
| How they feel: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| That suicide prevention is important, effective, will benefit everyone, and requires an holistic approach | Some progress; some confidence |
| People and / or organisations see how they can contribute to preventing suicide and are inspired to play their part | Some progress; some confidence |
| Safe, listened to, valued, included, encouraged, supported, and empowered | Some progress; some confidence |
The Lived and Living Experience Panel (LLEP) has been significantly involved in co-production of campaigns work and have felt involved and listened to, with their input directly shaping the approach and final outcomes. LLEP members have also welcomed being involved in portal development from an early stage, and representation of Delivery Leads and other stakeholders on the portal working group has been welcomed.
Education Scotland safeguarding leads see value in the work Suicide Prevention Scotland are liaising with them on. Local Suicide Prevention Leads have reported that they feel valued and that it feels we are collectively working. Both Youthlink and Youthwork Scotland were grateful that suicide prevention is being focused on, as they felt there are gaps with this and in the focus on wider mental health.
Strathclyde University welcomed the support to have the suicide prevention network for universities and colleges work come to fruition, and valued the policy links and advice on developing the student mental health action plan. NUS reported that the Student Mental Health Agreement leads enjoyed and gained a lot of knowledge from the session provided.
People who part in training as part of the actions towards outcome 2 told us,
‘The group and trainers were really supportive and it was an enjoyable 2 days despite the topic. Good to build on some skills and knowledge that I already have and network with people in similar roles in the area. Thank you!’ (School Counsellor on ASIST)
‘I feel much more confident now in my role particularly in exploring suicide and creating safety plans.’ (School Counsellor on ASIST)
‘The training was very good and we were able to use it in one of our conversations in class. Thank you.’ (Educator participant on safeTALK)
What they learn and gain
| What they learn and gain: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| We understand the context for implementation and what this means for effective delivery | Some progress; some confidence |
| Understand existing good practice, gaps, what needs to change, the priorities for action and possible solutions | Some progress; high confidence |
| People affected by/ at risk of suicide are confident that they will be able to access the help they need without experiencing stigma | Low progress; some confidence |
| Awareness of suicide, risk factors, and understand what to do to prevent suicide and tackle associated inequalities and social determinants | Some progress; some confidence |
| Knowledge, confidence, skills, resources and support to provide effective and compassionate support to people at risk of / affected by suicide | Some progress; some confidence |
| Co-ownership of a social movement and the opportunity to work with others to reduce risk, stigma and prevent suicide | Some progress; some confidence |
| Knowledge, skills and confidence to deliver tests of change and / or use evidence to support learning and improvement | Some progress; some confidence |
| A collective of people and organisations committed to delivering on the Suicide Prevention Strategy | Some progress; some confidence |
Action 4.1: Social movement, campaigns, and anti-stigma
The See-me workshop on Stigma and Discrimination introduced the SCIP model which will support those leading on delivery of actions in CHT to identify and mitigate against structural, cultural, institutional and personal levels of stigma and discrimination. This model has been included in the resources delivery and outcome leads utilise throughout the development and delivery of their work.
Action 4.2: Suicide prevention learning approach
Over the last year, we have used a targeted approach to delivering the range of suicide prevention learning resources ensuring the learning opportunities are reaching people who work in:
- Health and social care including emergency responders and community pharmacy.
- Frontline supporters including the following sectors: debt/money advice, housing and homelessness, care-experienced, violence against women and girls, community justice; addictions services, transport (e.g. bus/taxi drivers); hospitality and retail (including hairdressers/barbers), leisure, fitness and sport.
- Education including higher and further education, counsellors, youth work.
- Third sector agencies including voluntary organisations and charities.
Between 1st April 2024 and the 17th February 2025, 3050 people undertook ASIST training and 1377 attended safeTALK. The feedback from participants is captured on the PHS training dashboard and shows the majority of participants feel better prepared and more confident to help someone at risk of suicide as a result of attending the training. A selection of comments is included in the 'How they feel' section of this report.
Action 4.3: Whole school approach to mental health
Action 4.4: Develop age-appropriate school resources
Action 4.5: Pre-registration training
As part of the case study gathering on the whole school approach and curriculum, we have been shown some great emerging practices across Scotland that will be useful to evaluate and use for advocacy and planning purposes. We will also consider how we can share these across Scotland through the learning events.
The National Union of Students (NUS) Think Positive Hub has been updated with the training and support available for staff and students about suicide prevention, improving the awareness and understanding of suicide across colleges and universities. The national network for colleges and universities has begun to bring together these sectors to work collaboratively and learn from each other to help address suicide risk.
Case study: A campaigns framework to shape suicide prevention public awareness campaigning (Outcome 2, Action 4.1)
What we have done:
Our campaign concept has three core objectives:
1. Normalising the idea of conversations about suicide
2. Building confidence to have these conversations
3. Signposting to the new suicide prevention website.
Who with:
It was developed through workshops and co-production sessions with participation from:
- The Suicide Prevention Lived and Living Experience Panel (LLEP)
- Local communities
- The Academic Advisory Group
- The SeeMe campaign
- The United to Prevent Suicide Social Movement
How they feel:
The Action 4.2 detailed report notes:
‘There's a clear recognition from all involved in Suicide Prevention that campaigns will provide a vital piece in our efforts to prevent suicide with very high levels of commitment.’
What has been learned:
Our co-design process challenged us to think at a high level about inequalities.
We recognised that traditional demographic profiles like “men aged 35-55” are transcended by how people feel — and the associated risks.
Instead, we are looking at how the campaigns can be targeted based on the likelihood of needing to seek help, or the confidence to support someone else.
What is being done differently?
We are trying to include as great a breadth of experiences as possible in the campaign concept as we refine and test. Our user testing will be weighted to reflect the higher risk of people living in higher-ranked SIMD areas. From here, we will be able to better diversify campaigns - e.g. considering cultural differences, language, gender identity etc.
What difference will this make?
We've built a framework for an ongoing heartbeat of campaigning through the coming years. It will focus on ‘two sides of the coin’: giving confidence to people in distress to ask for help, and confidence to the people around them to respond and talk about suicide.
Effective campaigning will raise public awareness, and we will seek to measure change in public attitudes.
Cross action learning
The key learning, particularly relating to actions focusing on school systems and professions, has been that partnership work is key to enabling the desired changes to be made, and a deeper understand is required, particularly at leadership level, about how the sectors we are trying to influence and change see their role in suicide prevention.
There is also scope to consolidate actions and set clear milestones to achieve across the actions for 2025/26. This will increase focus, allow for better planning and resource management, and streamline reporting.
For Outcome 2 to be successful, wider engagement with communities is essential. In year 3 we will build on the engagement to date particularly in post-development and testing of the campaigns work, and through scoping and implementation of Action 4.7.
What they do differently
| What they do differently: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Work with wider stakeholders and partners to prioritise, plan, commission and deliver the work | Some progress; some confidence |
| Take action to prevent suicide and tackle the impact of inequalities and social determinants that impact on suicide | Some progress; some confidence |
| Respond effectively and with time, space and compassion to people at risk of / affected by suicide | Low progress; low confidence |
| People affected by/at risk of suicide access quality, timely, equitable support, including recovery, wellbeing and support to address inequalities | Low progress; some confidence |
| Take co-ordinated and collective approaches to raising awareness and continuing to build the suicide prevention community | Low progress; low confidence |
Outcome 2 is designed to ensure our communities have a clear understanding of suicide, risk factors and its prevention, so that people and organisations are more able to respond in helpful and informed ways when they, or others, need support. Many of the actions under this outcome are in design and development stage and are not yet making the difference anticipated.
What difference does this make?
| What difference does this make: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Outcome 2: Communities understand suicide, risk factors and its prevention - so that people and orgs are able to respond in helpful, informed ways | Some progress; some confidence |
Our early contribution towards Outcome 2:
As many of the actions in Outcome 2 are still in the development stage, it is not yet fully possible to track their impact to the overall outcome. There are some key examples where we can see the difference individual actions are having and can identify the learning about what is driving this.
Action 4.1: Social movement, campaigns and stigma
Evidence suggests that as part of a wide programme of work effective campaigns raise awareness of suicide and give people seeking help and potentially asked to give help the confidence needed. Over a sustained period, we should be able to measure public attitudes towards confidence in talking about / responding to suicide through the market research built into this action.
The social movement work being undertaken now will also contribute to this in the longer term.
Action 4.3: Whole school approach
The approach to building suicide prevention into the whole school approach to mental health has shown that people value connecting and shaping this work. The insight report noted that education colleagues wish to be part of suicide prevention work whilst ensuring they do not hold all the responsibility for suicide risk.
Stakeholders across settings have reported that they now understand their role more and, in some areas, we have seen local partnerships forming such as East Lothian through their education structures.
We have also learned from areas that it is beneficial to have someone driving forward the work that has network and influence and that resource and engagement with young people is necessary.
In working with the YAG and PN knowledge is being gained, that at times aligns with the approach being taken and at times signals there is a need to pause, reflect, and adjust the work.
Action 4.4: Develop age-appropriate school resources
The approach taken in gathering practice studies is working well and is demonstrating the importance of working alongside the sector, so they have ownership of the outputs.
Outcome 3
Everyone affected by suicide is able to access high quality, compassionate, appropriate and timely support, which promotes wellbeing and recovery. This apples to all children, young people and adults who experience suicidal thoughts and behaviour, anyone who cares for them, and anyone affected by suicide in other ways.
(Image caption: This colour-coded outcome map shows our theory of change for outcome 3 and our assessment of early progress towards it, including our confidence in the evidence we have to support this. This information is broken down in each section of the report that follows. The whole map can also be viewed more clearly online here.)
What we do
| What we do: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Review data and information, and engage stakeholders to deepen understanding of the needs and challenges we are seeking to address | Some progress; some confidence |
| Bring people together to scope and define problems, agree priorities for action and co-design solutions | Some progress; some confidence |
| Share evidence and learning on suicide prevention through events, reports and other channels and support people to put learning into practice | Some progress; some confidence |
| Develop and deliver a portfolio of accessible learning & development opportunities and resources | Some progress; some confidence |
| Provide training, guidance, tools and resources and support workforce development to support staff to respond compassionately and effectively | Some progress; some confidence |
| Develop, test and deliver human rights based, preventative, recovery-oriented services and supports for people at risk of / affected by suicide | Great progress; high confidence |
| Assess and identify how inequalities can and should be addressed through this work | Some progress; some confidence |
Table: Action Area 5 (towards Outcome 3) - progress update against the delivery plan
| Actions towards Outcome 3 | Progress |
|---|---|
| Action 5.1: Distress Brief Intervention (DBI) adaptation | On track in line with the delivery plan |
| Action 5.2: Respond to diverse needs of communities | On track in line with the delivery plan |
| Action 5.3: Peer support capacity | On track in line with the delivery plan |
| Action 5.4: Family, friend and career response | On track in line with the delivery plan |
| Action 5.5: Education staff response | Behind schedule against the delivery plan |
| Action 5.6: Prevent suicidal behaviour in children and young people | Scoping work in progress |
| Action 5.7: Prevent suicidal behaviour in older adults | On track in line with the delivery plan |
| Action 5.8: Primary care response | Behind schedule against the delivery plan |
| Action 5.9: Clinicians in unscheduled care settings | On track in line with the delivery plan |
| Action 5.10: Improve clinical care and support | Progressing in advance of the delivery plan |
| Action 5.11: Provide suicide bereavement support | On track in line with the delivery plan |
| Action 5.12: Single Scottish Telephone Number | No activity scheduled for Year 2 |
The following provides an overview of activity that has been carried out across each of the different actions in Outcome 3.
Action 5.1: Distress Brief Intervention (DBI) adaptation
Work to progress this action has included:
- A wide range of dissemination activity to share learning from the DBI evaluation alongside opportunities for stakeholders to discuss and debate the findings.
- Activity to explore whether DBI has a potential role in offering follow-up support or contact with people following a planned exit from support.
- An independent evaluation which is considering how DBI might help prevent suicide is underway, and workshops and sessions have been held with the DBI community, including a focus on DBI and Time Space and Compassion and Suicide Prevention.
- Activity to incorporate level 2 referrals into existing frontline services, to help facilitate uptake and adoption of DBI.
- Activity that will help to ensure effective links across alcohol brief interventions and distress brief interventions has commenced.
Enablers, barriers and changes to delivery plans
Aspects of activity that have worked well and contributed to progress include:
- Co-ordinated multi-pronged approach to disseminating evaluation findings and bringing stakeholders together to share and discuss learning and findings.
- Successful embedding of referral process and form into the internal systems of referral partners.
- Continued activity to ensure strong strategic links to Alcohol and Substance misuse leads via local DBI implementation groups.
- The survey of Senior Clinical Decision Makers (SCDM)/Flow and Navigation Centres/mental health assessment units that are already involved in or planned to be involved in DBI received, there was an excellent response rate which provided encouraging results.
- DIME evaluation progressing well, with strong support from the DBI programme, DBI Central Team and Public Health Scotland.
Learning
- The flexibility of being able to embed referrals within internal systems is working well. Provided the essential information on the DBI referral form can be shared via standard systems, this is an option that can be further developed.
- While strategic links to Alcohol and Substance misuse leads have been developed through local DBI implementation groups, and clear operational pathways to Alcohol and Substance misuse support, the extent to which this is in place varies across the DBI Level 2 services and HSCPs. Therefore, DBI Central will commit to an audit of current practice, and seek national parity from this point.
- Opportunities for further work to be undertaken on the longer-term impact of DBI on individuals and the wider service system.
- Opportunities for analysis into some of the factors associated with increased distress among some individuals at the end of Level 2 based on the PHS DBI Level 2 dataset, to see if there are any differences in key measures that can be identified.
Action 5.2: Respond to diverse needs of communities
Work towards designing a test of change approach, including identifying target groups and settings where there is a higher risk of suicide, and testing new approaches to provide support and encourage help seeking has included:
- Completing recruitment of four community-based groups to carry out the required research. These include organisations working with people who experience stigma, discrimination and/ or the socio-economic inequalities associated with increased risk of suicide such as deprivation, people experiencing poor mental health, young people and people who are refugees or seeking asylum.
- Establishing a steering group to oversee the research.
Enablers, barriers and changes to delivery plans
- The Community Led Action Research has progressed as set out in the delivery plan
- Strong stakeholder support and engagement from community groups has been an enabler of progress.
- The recruitment and initial training process proved successful and ensured initial aims were met.
Learning
- Importance of effective support for those involved in completing the research. The steering group alongside SCDC will continue to provide the required support during year 3.
- learning from the research and the benefits of community partnerships that have been developed will be disseminated after completion of the research.
Action 5.3: Peer Support Capability
Overall progress has been good and in line with initial delivery plan, while also being alert to opportunities that can inform the direction of travel. Delivery to date has included:
- Creating Hope with Peer Support resource co-designed and shared over 300 times.
- Creating Hope with Peer Support workshop delivered 10 times, with a further 7 scheduled through 2025.
- Held a variety of participative network events including information sessions, learning and networking events, focus groups, and training pilot sessions. 2025 will see the delivery of 4 more learning and networking events along with 2 online information and support sessions, and one national in person event.
- Progressing the planned evaluation programme which will support community-based groups to develop their ability to assess the impact of their peer support services (delivery through Feb-June 2025).
(Image caption: Perth learning & networking event - Mindspace sharing their experience of delivering peer support for people in mental health crisis.)
(Image caption: Participants in the Creating Hope with Peer Support 2-day training pilot.)
Enablers, barriers and changes to delivery plans
- The main challenge has been related to internal staff changes but has not prevented delivery of planned activities.
- The original intention of producing a 2-day training programme has been revised following feedback from the pilot. This has now been developed as a resource that organisations can use in a way that best fits their circumstances.
- An addition to the delivery plan for 2025 will include a review of local suicide delivery plans to explore how peer support is integrated and the potential supportive role of the Creating Hope with Peer Support resources.
Learning
- Effective scheduling of activities to ensure momentum can be maintained, whilst ensuring space to respond to emerging opportunities.
Action 5.4: Family, friend, and carer response
Activity to date has involved undertaking an extensive mapping exercise of available resources and support for carers, beginning at a national level and working down to a local level. A priority has also been engaging those with lived experience, specifically Young Carers and Unpaid Carers. Engagement activity has included:
- Young Carers Conference in March 2024.
- Engagement with stakeholders to consider the most strategic approach to supporting carers across Scotland, and how best to engage with support/service providers.
Enablers, barriers, and changes to delivery plans
- Staffing changes led to some aspects progressing more slowly than planned.
- Strong collaboration across Outcome 3 leads, and strong leadership have been enablers of progress.
Learning
Engagement with those who have lived experience has been incredibly valuable so far and has provided some interesting insights around:
- Engagement activity with those who have lived experience has generated valuable learning and insights including the experiences of those who have been bereaved by suicide and at-risk groups to help shape the support that would be most suitable and beneficial.
- Engagement activity has also generated insights and ideas for potential improvement to carer support.
- Further work is required around understanding the gaps and what this means for what we do next.
Action 5.5: Education staff response
The work on this action has been combined with the delivery of action 4.3 (Whole school approach to mental health) as there is a need to look at staff wellbeing at the core of this work.
To date the following activity has been delivered, or is planned for delivery:
- Developed a document setting out what education's role is in suicide prevention.
- Setting up a roundtable discussion to bring those working in education, social work, health, to explore their roles and how they work together.
- Working with ADES, COSLA, and Education Scotland on their work to embed support and supervision for staff to see where a suicide prevention lens can be added to this work.
Enablers, barriers, and changes to delivery plans
No milestones were set for this action in the year 2 delivery plan which has meant there were also no milestones or resources set aside to deliver it. Although work has been progressed due to its alignment with action 4.3, milestones etc for year 3 will be included in the delivery plan for 2025/26.
Action 5.6: Prevent Suicidal Behaviour in Children and Young People
Overall, this action is progressing in line with the delivery plan. To date the following has been delivered:
- Dissemination of an Insight Report to increase knowledge about young people’s needs.
- Submitted a paper to the Child and Family Mental Health: Joint Strategic Board (JSB) asking that they consider and enact our recommendations to include suicide prevention throughout their working groups.
- Connected with organisations that deliver intervention work for children and young people.
- Working with stakeholders to connect The Promise Leads and Local Suicide Prevention Leads.
- Attended the LGBTQI+ mental health network meeting to explore how at a policy level we may be able to support the network.
- Established a bi-monthly Children and Young People's forum to bring together local leads and relevant colleagues.
- A crisis support framework is being developed therefore, discussions with colleagues progressing this are being undertaken to ensure the unique needs for suicidal crisis addressed through this.
- Working with Children in Scotland and Penumbra to develop a tool kit that enables conversations between adults/ parents/ carers and young people and peer conversations.
- Developing effective communications which enable sharing of learning and experiences with local areas.
Enablers, barriers, and changes to delivery plans
- While work is on track, system readiness and ability to consider and deliver the work continues to be a point of consideration.
- Work to connect with organisations that deliver intervention work for children and young people has not happened at the desired pace. This is due to there being no easy way to identify and reach out to services.
- Ensuring there is sufficient resource to deliver the crisis support required to address the gaps identified for CYP requires ongoing discussion. This is something that has been advocated for in the Insight Report and through the JSB structures.
Learning
- The work undertaken has enabled enhanced understanding of good practice which can be shared to encourage and inform the development of practice across Scotland.
Action 5.8: Primary Care Response
Positive progress has been made, at a slower pace than set out in the delivery plan. Some activity scheduled for year 2 will extend into year 3. Delivery this year has included:
- Developing understanding of how best to support improvement in the primary care system.
- Continuing to build work and relationships with key Scottish Government policy teams.
- Contributing to the development of the Mental Health in Primary and Community Care Report.
- Working with partners on a TSC primary care practice story and a TSC primary care podcast.
- Delivery of a practice/learning session for SG professional advisors, mental health, and primary care policy leads on emerging practice in primary care.
Enablers, barriers, and changes to delivery plans
- Pressures in primary care limit the time and capacity key stakeholders can bring to national projects and improvement activity. In response to this, work is being undertaken to align this work with existing change programmes and identify opportunities for smaller scale improvement projects.
- Work has been carried out with Scottish Government colleagues to start scoping these opportunities. Scottish Government colleagues have supported activity to test ideas for focused work with key stakeholders and equality groups as part of their wider engagement work on primary care mental health. This work is now part of the Scottish Government Mental Health in Primary Care and Communities Governance Group work programme.
Learning
- Pre-registration training, regional GP training leads, and practice managers are key people/places to start.
- GP practice teams and managers cover all aspects of health and wellbeing, meaning they can be overwhelmed with requests relating to all aspect of health and wellbeing. Thoughtful and practical communication and engagement plans will be key.
- Work on action 5.10 has generated key learning that will be transferable to the work being carried out in primary care.
- There is a key link between this work and the development of Psychiatric Emergency Plan guidance.
Action 5.9: Clinicians in unscheduled care settings
The main work on this action during year 2 has included:
- Completed a MHUC in acute setting Time Space Compassion podcast.
- Delivered a joint webinar on Suicide Prevention and Trauma Informed Practice.
- Providing keynotes at HSCP conferences on suicide prevention.
- Representing Suicide Prevention Scotland work on the MHUC Governance Group and partnership network, and in regular meetings between Scottish Government and Scottish Ambulance Service.
- Undertaken an initial phase of engagement with both the governance group and learning network on learning from work under 5.10.
- Working with Scottish Government Policy colleagues to integrate Time Space Compassion principles in the Safe Spaces Scoping Report.
- Joint facilitation of a session for the Scottish Government led Psychiatric Emergency Plan Review Working Group.
- Effectively embed Time Space Compassion and suicide prevention resources in the latest version of the Mental health unscheduled care services: resources.
Enablers, barriers, and changes to delivery plans
- Whilst we supported four boards with focused engagement/promotion work on TSC, available resources limited the depth and extent of that work. We will look at ways to scale this work in the 25/26 workplan.
- This decision has led to delays in the publication of the podcast and reduced engagement with the wider MHUC network/partners.
Learning
- Illustrative practice has helped to bring policy off the page in realistic and relatable ways and offer ideas for practical action.
- MHUC improvement work and policy is complex – it takes time and expert support to engage with it in a meaningful way.
- Learning generated in relation to risk management and supporting communities impacted by discrimination, stigma, inequality, and wider social determinants can also help shape this area of work.
Action 5.10: Improve clinical care and support
Activity for this action is progressing well and on track, and has included:
- Establishing a core delivery team, plan, and collaborative working arrangements.
- Co-producing the delivery plan and learning sessions with the three participating Health Boards, running three improvement planning workshops with the three board, and three deep dive learning sessions for practitioners from the boards.
- Facilitating two on-line practice sharing sessions with leading English NHS Trusts.
- Developing and testing new ways to support Boards to engage with lived experience insights from the LLEP and key marginalised groups.
- Developing and initiating work to engage and collaborate with key organisations who work with marginalised communities.
- Working with the LLEP and YAG to shape our early thinking and understanding of this work.
- Engaging with the Royal College of Psychiatry suicide prevention lead for Scotland.
Enablers, barriers, and changes to delivery plans
- Resourcing challenges in partner organisations has resulted in delays and gaps in critical areas of the project team.
- Buy in from Boards has exceeded expectations and helped to progress activity.
- Buy in and support from wider stakeholders, and the sharing of learning and resources from English Trusts helped to accelerate progress.
Learning
- Workforce resourcing pressures and restructures disrupt the work, though also opens opportunities to combine forces and budgets in creative and productive ways.
- Collaboration is powerful but is also resource intensive and takes a lot of time and effort to embed.
- People respond well to carefully designed and facilitated sessions. Making people feel welcome and cared for is important when doing hard and emotionally challenging work together.
- Moving from aspiration to practical improvement activity will be key to securing buy in and maintaining momentum.
Action 5.11: Provide Suicide Bereavement Support
The Suicide Bereavement support service continues to provide high quality support to people bereaved by suicide. Ongoing activity to maintain referral pathways and engage with stakeholders continues. Overall, service delivery is in line with the delivery plan.
Work to support local areas to develop support services for people affected by suicide has recently started with the recruitment of the staff member leading this work. Since the lead came into post, the following activity has been commenced:
- Making connections across the Creating Hope Together community.
- Drafting an action plan to support the planning process.
- Arranging meetings with interested health board areas.
- Establishment of a steering group (incl. terms of reference) to oversee the work.
- Production of a briefing document that provides an overview of the work, and the learning generated from the evaluation of the Suicide Bereavement Support Service pilot.
- Initial contact made with all local Suicide Prevention Leads.
Enablers, barriers, and changes to delivery plans
Delivery of the Suicide Bereavement Support Service continues to be in line with the delivery plan, with no challenges or barriers impacting on this.
Ensuring service practitioners are kept up to date with development opportunities and that support is constant and ongoing is a key enabler in providing a high-quality service.
The work to support other areas to develop a suicide bereavement support service is still in its early stages with the lead having only been in post for a few months. However, Health Board areas have already been identified that are keen to develop a suicide bereavement support service and have begun to make progress.
Learning
The Suicide Bereavement Support Service reflected on the importance of building and maintaining relationships to ensure effective referral pathways, but also in ensuring that the service profile is continually developed, and their learning and impact shared. This has been a focus of their work over the previous 6-months.
Their learning also highlights the importance of investing in support and continuing professional development for practitioners, and the usefulness of shared development experiences.
As the work to support the development of suicide bereavement support services in other areas is in its early stages, learning to date is limited. However, it has been acknowledged that collaborative working will be essential, and this will influence the pace and extent of progress that is made.
Who with
| Who with: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| People developing and implementing policy relating to inequalities and social determinants that impact on suicide at local and national levels | Great progress; some confidence |
| People and organisations whose work contributes to addressing inequalities and social determinants that impact on suicide | Some progress; some confidence |
| Suicide Prevention Scotland Delivery Collective | Great progress; some confidence |
| People working with people at risk of suicide or affected by suicide | Great progress; high confidence |
| People and communities with lived and living experience of suicide or the inequalities and or social determinants that impact on suicide | Some progress; some confidence |
| Interested members of the public in Scotland | Some progress; some confidence |
Across the actions working towards outcome 3 this year, we engaged with:
- 3 research teams: University of Glasgow; University of Manchester (NCISH team); University of Stirling; University of Strathclyde
- 3 panels of people with lived and living experience: the Lived and Living Experience Panel; the Participation Network; the Youth Advisory Group.
- 1 media organisation: Seeing the Magic (producers of ‘The Low Road’).
- 15 professional networks and membership organisations: Association of Directors of Education in Scotland; Association of Managers of Student Services in Higher Education; Association of Scottish Principal Educational Psychologists; Colleges Scotland; General Practice in Inverclyde and West Dumbartonshire; Mental Health Unscheduled Care Learning Network; Mental Health Unscheduled Care Governance Group; NUS Scotland; Parenting Scotland, Royal College of Psychiatry, The Promise Leads Network; The Psychiatric Emergency Plan Working Group; Universities Scotland; Unscheduled Care CAMHS Staff; Youth Link Scotland.
- 23 public bodies, health boards, and HSCP: Distress Brief Intervention Programme Team (NHS); Dumfries & Galloway HSCP; Dundee HSCP; Education Scotland - PSE and Safeguarding Leads Networks; Fife HSCP; Health Improvement Scotland; Mental health leads and MHUC leads across NHS Boards; Mental Welfare Commission; NHS 24; NHS Ayrshire & Arran; NHS Borders; NHS Dumfries & Galloway; NHS Education for Scotland (NES); NHS Fife; NHS Highland; NHS Suicide Prevention teams; NHS Tayside; Perth & Kinross HSCP; Police Argyll and Bute; Police North; Police Scotland; Public Health Scotland; Scottish Ambulance Service; Scottish Borders HSCP.
- 54 commissioned service providers, voluntary sector and community groups: Dumfries and Galloway Alcohol and Drug Partnerships Peer Support; Andy’s Man Club; Bipolar Edinburgh; Child Bereavement UK; Centred (Discovery College); Change Mental Health; Children in Scotland and the National Parent Forum of Scotland; Connect; Cruse; DBI Level 2 providers; Dundee Volunteer and Voluntary Action; Equality Network Scotland; Families in Trauma; Fostering Network Scotland; Hope Point Dundee; Independent Living Support; James Support Group; Kick Mental Health; LGBT Health & Wellbeing Scotland; The Living Warriors Project; Man on Inverclyde; Men Matter Scotland; Men United; Mental Health Foundation; Mikeysline; Mindspace, Perth & Kinross; Movember; Neil’s Hugs Foundation; Papyrus; Penumbra and the Self-Harm Network; Reach Across; Rosemount Lifelong Learning; Samaritans; SAMH and Sam’s Café Fife; Scottish Community Development Centre; Scottish Recovery Network; Scottish Refugee Council; See Me; Shakti Women’s Aid; Shetland Link Up; Survivors of Bereavement by Suicide (SOBS); Stepping Stones for Families; SWAN Scotland; The Carers Trust; The Hive, Fife; The Neuk; Tony’s Safe Place; United to Prevent Suicide Campaign; V&A Dundee; Veterans 1st Point; Wellbeing Works; Winston’s Wish; Women's Wellbeing Club; Young Women’s Movement; Youth Scotland.
- 11 teams in national and local government: COSLA; Highland Council; Child and Family Mental Health Joint Strategic Board; Local leads, subgroups and taskforces for suicide prevention and substance use; National Improvement Leads for trauma informed practice; NSPAG Primary Care Expert; Personal and Social Education Review Local Implementation Group Chair; Scottish Government Equality & Human Rights Forum; Scottish Government policy leads for mental health (including mental health unscheduled care), substance use and primary care; Time Space Compassion Delivery Lead.
For a small number of action areas, various pressures and challenges have impacted on the involvement of some stakeholders and partners. Overall, however, engagement across the diverse range of stakeholder groups and organisations has largely been in line with expectations, and in some cases exceeded hopes and plans. Action leads recognise the collaborative approach that is required for success and acknowledge the key role that stakeholders and partners have had in the progress that has been made to date.
The suicide bereavement support service continues to undertake activities to extend the reach of the service and ensure it is accessible to harder to reach and marginalised groups.
How they feel
| How they feel: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| That suicide prevention is important, effective, will benefit everyone, and requires an holistic approach | Some progress; some confidence |
| People and / or organisations see how they can contribute to preventing suicide and are inspired to play their part | Some progress; some confidence |
| Safe, listened to, valued, included, encouraged, supported, and empowered | Some progress; some confidence |
The range of activity that has been delivered through Outcome 3 is wide and varied. Feedback from the delivery leads about how those who have been involved in their work have felt, has been positive. People engaged during the delivery of actions towards Outcome 3 told us:
‘Energised, enthusiastic, confident. The content of the facilitation of the course was amazing, facilitators managed the balance between being laid back and authoritative, knowledgeable and valuing the knowledge in the room.’
‘I feel uplifted and validated. I feel proud to be a peer support worker and appreciated the opportunity to meet other peer support workers especially because I am new at the NHS.’
I have so enjoyed the calls with my practitioner, she listened and very skilfully made me realise that there was light and a life at the end of the “tunnel” If she had said that at the beginning of our journey, I simply would not have believed it! However, 3 years on I feel empowered to live my life, and that suicide will not define me as a person.’
A higher-level summary of the feedback we have received on our engagement with a range of stakeholders is as follows:
- Involved, listened to, and heard – through the collaborative approaches being utilised, and the consultation activity being undertaken.
- Curious and interested – about plans, what is trying to be achieved, benefits and how they can be involved.
- Supported – through the work that is being undertaken, or through the service they are accessing.
- Cautious – about the practicality of making system change work in a context of varied pressures and limitations.
- Willing and confident – to be involved and take activity forward.
- Inspired – to take action.
- Keen – to see the work progress.
- Cautious trust – people gauging the extent to which ideas will be followed through.
- Passionate – about being involved, contribute to addressing the challenges and making positive change.
- Valued – for their role and the contribution they are making.
- Grateful – that this work is being focussed on, and action taken.
What they learn and gain
| What they learn and gain: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| We understand the context for implementation and what this means for effective delivery | Some progress; high confidence |
| Understand existing good practice, gaps, what needs to change, the priorities for action and possible solutions | Some progress; some confidence |
| People affected by/ at risk of suicide are confident that they will be able to access the help they need without experiencing stigma | Some progress; some confidence |
| Awareness of suicide, risk factors, and understand what to do to prevent suicide and tackle associated inequalities and social determinants | Some progress; some confidence |
| Knowledge, confidence, skills, resources and support to provide effective and compassionate support to people at risk of / affected by suicide | Some progress; some confidence |
| Tested interventions, approaches, services and supports that are effective in preventing and responding to suicide | Some progress; some confidence |
| A collective of people and organisations committed to delivering on the Suicide Prevention Strategy | Some progress; some confidence |
The varied nature of activity delivered through the actions in Outcome 3 means that different people will learn and gain different things. For a few actions, delivery is at such an early stage that there is a little to report on in relation to this area. However, the following sets out what people are learning and gaining as a result of this work:
- Increased insight, knowledge, understanding, skills, tools, and/or resources and materials related to suicide prevention, social and intersectional factors (gaps, challenges, learning, good practice etc.).
- Opportunities to share lived experiences, and alongside this, opportunities to reflect on lived and living experience, including how this differs and intersects for marginalised groups.
- Local approaches to issues and solutions within suicide prevention
- High quality compassionate, emotional and practical support (SBSS supported people).
- Increased awareness of available provision.
- Learning and insight into the needs and preferences of different communities and the barriers and challenges they face.
- Opportunities to test and share practice, and to promote and share learning with others.
- Streamlined processes and systems.
- An opportunity to be involved and shape the work.
- Access to subject matter experts, ideas, evidence, guidance, practice, peers and support.
- Recognition that this work is not starting from scratch and there is much existing practice, experience and learning that can be drawn on and shared.
Case study: Community-Led Action Research (CLAR) (Outcome 3, Action 5.2)
What we have done:
We commissioned Scottish Community Development Centre (SCDC) to support, train and mentor 4 organisations in community-led action research.
The organisations were recruited through a competitive tendering process involving stakeholders, including members of the Lived and Living Experience Panel.
The 4 organisations have participated in training and been allocated mentors to support them.
Who with:
The organisations conducting research are:
- PAPYRUS Prevention of Young Suicide – delivering in Maryhill Glasgow, an area of economic deprivation, the research will explore how to best support children, young people and care givers who are at risk of suicide.
- Rosemount Lifelong Learning – working in North East Glasgow, this project will work with those most disadvantaged in the area including asylum seekers and refugees.
- Shetland Link Up – working with the most vulnerable adults in the wider Shetland community, and who have lived experience of suicidal thoughts or actions, or experienced bereavement by suicide.
- Tony’s Safe Place – A community-led mental health and suicide prevention charity, carrying out their action research in Cumbernauld with people experiencing high levels of economic disadvantage, poor mental health and/or who have been affected by suicide.
How they feel:
The Papyrus application to the programme read:
A research project in Maryhill [will] provide valuable insights about how suicide prevention can cater to the diversity of need within an economically deprived location.’
‘
(Image caption: Representatives from the mentored organisations at CLAR training provided by the Scottish Community Development Centre.)
What has been learned:
The Action Research projects aim to:
- Amplify the voice of community members, develop confidence and skills, and provide opportunities for involvement in decision-making processes.
- Gather learning and deepen understanding of where and how suicide impacts on local communities, and what needs to change to prevent/reduce this.
The projects are currently conducting their research, with analysis planned March–June 2025.
What difference will this make?
These projects will bring together community resources to codesign and co-deliver responses to prevent/reduce the impact of suicide on families and communities. They will enable people to respond more confidently and appropriately to people affected by suicide.
The CLAR will deepen knowledge and understanding about suicide and influencing factors. This will inform the development of wider appropriate, high quality, effective support to prevent suicide and reduce the inequalities that affect suicidal behaviour.
What they do differently
| What they do differently: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Work with wider stakeholders and partners to prioritise, plan, commission and deliver the work | Some progress; some confidence |
| Take action to prevent suicide and tackle the impact of inequalities and social determinants that impact on suicide | Some progress; some confidence |
| Respond effectively and with time, space and compassion to people at risk of / affected by suicide | Some progress; some confidence |
| People affected by/at risk of suicide access quality, timely, equitable support, including recovery, wellbeing and support to address inequalities | Some progress; some confidence |
| Take co-ordinated and collective approaches to raising awareness and continuing to build the suicide prevention community | Some progress; high confidence |
| Use quality data and appropriate evidence to inform priorities, develop interventions and make effective decisions | Some progress; some confidence |
| People and organisations play their part in scaling up and embedding effective interventions | Some progress; some confidence |
The following provides a summary of how delivery of the different actions in Outcome 3 are seeing or anticipating people and organisations are doing things differently:
- Research findings and evidence, and insights and learning, is used to inform policy and decision making.
- Organisations and service providers will include and value the input of people with lived experience and recognise peer support as an indispensable part of mental health care and service delivery.
- Time Space and Compassion is mainstreamed into policy and improvement work, and in practice across relevant organisations and services.
- Increased connections across the system that enable and support the sharing of learning and practice, and more active and connected improvement/development activity being carried out.
- Organisations and service providers utilise resources, toolkits, evidence, learning and good practice to inform priorities, and the development of interventions and/or improvement activity.
- People and organisations understand and recognise their role and act relevant to their role and setting.
- Relevant stakeholders engage to create the conditions that enables development and improvement activity.
- Those affected by bereavement by suicide accessing support start to build a life around their grief and find ways to have hope for the future.
What difference does this make?
| What difference does this make: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Outcome 3: Everyone affected by suicide is able to access high quality, compassionate, appropriate and timely support - which promotes wellbeing and recovery | Some progress; some confidence |
The overarching outcome for Outcome 3 is that everyone affected by suicide is able to access high quality, compassionate, appropriate and timely support - which promotes wellbeing and recovery.
The following sets out how the main themes in how it is anticipated that the different actions will contribute to this overarching outcome:
- Contribute towards the availability of services and support provision, as well as enhancing joined up working and coherence across different services and support.
- Ensuring improvement activity and/or interventions are developed using available evidence, insights, learning and is embedded in practice.
- Enhancing the capacity of community-based suicide prevention provision.
- Building the evidence base and providing guidance/resources that communicate how best to support the needs of different communities.
- Understanding and responding to the unique needs of different communities
- Creating the conditions and providing the support that enables well planned and informed development and/or improvement activity.
- Evidence, learning and experience being gained can inform course correction which ensures work being delivered through the actions reflects what is required to meet the overarching aims.
- Creates an environment for collaboration and joined up working, to ensure suicide and suicide prevention is considered across the system.
- Enhance the accessibility, availability and quality of support for people affected by suicide.
Outcome 4
Our approach to suicide prevention is well planned and delivered, through close collaboration between national, local and sectoral partners. Our work is designed with lived experience insight, practice, data, research and intelligence. We improve our approach through regular monitoring, evaluation and review.
(Image caption: This colour-coded outcome map shows our theory of change for outcome 4 and our assessment of early progress towards it, including our confidence in the evidence we have to support this. This information is broken down in each section of the report that follows. The whole map can also be viewed more clearly online here.)
What we do
| What we do: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Review data and information, and engage stakeholders to deepen understanding of the needs and challenges we are seeking to address | Great progress; high confidence |
| Bring people together to scope and define problems, agree priorities for action and co-design solutions | Great progress; high confidence |
| Share evidence and learning on suicide prevention through events, reports and other channels and support people to put learning into practice | Great progress; high confidence |
| Embed a process of continual learning and improvement | Some progress; some confidence |
| Build the data and evidence ecosystem to underpin current and future suicide prevention work | Some progress; some confidence |
| Provide support and guidance to people delivering on actions including delivering tests of change and making good use of data to improve systems | Some progress; high confidence |
| Assess and identify how inequalities can and should be addressed through this work | Some progress; some confidence |
The following provides an overview of activity that has been carried out across each of the different actions in Outcome 4.
Table: Action Area 6 (towards Outcome 4) - progress update against the delivery plan
| Actions towards Outcome 4 | Progress |
|---|---|
| Action 6.1: Suicide prevention action plan | On track in line with the delivery plan |
| Action 6.2: Suicide cluster guidelines | On track in line with the delivery plan |
| Action 6.3: Lived experience model | On track in line with the delivery plan |
| Action 6.4: Improve recording and reporting suicide deaths | On track in line with the delivery plan |
| Action 6.5: New evidence digest | Scoping work in progress |
| Action 6.6: Multi-agency suicide reviews and a learning system | On track in line with the delivery plan |
| Action 6.7: Host learning events | On track in line with the delivery plan |
Action 6.1: Suicide prevention action plans in high-risk setting
The initial work on this action set out the definition and scope of suicide prevention action plans. There was a recognition that this may differ across different sectors/ agencies and that it would be key to draw out learning as different approaches were tested.
Engagement with relevant stakeholders in housing, prisons, Police Scotland and care experienced sector has taken place to identify the actions required in these settings to address the inequalities experienced by both staff and service users that might impact on their suicidal risk. Members of the LLEP who have expressed an interest in this work have also been included in discussions.
PHS also internally reviewed how a suicide prevention lens can be applied to wider mentally flourishing workplace activities being co-ordinated by PHS and tested by national and local employers across a range of settings to extend the scope of this action across other sectors.
An internal group within PHS has developed a FAQ sheet setting out key areas that organisations might ask when contemplating the development of suicide prevention action plan. A draft framework for consolidating, strengthening or developing SP Action Plans has also been developed and will be tested in the high-risk settings identified above. This is being reviewed by those members of the Lived Experience Panel who are working to support this action and by Suicide Prevention Leads whilst the focused sector stakeholders will use and review the framework as part of their implementation processes.
The AAG are also undertaking a review of effective interventions in workplace settings which might form the basis of an organisation's action plan.
Action 6.2: Suicide Cluster Guideline
This action has focused on the support provided to local areas to implement the suicide cluster guidance published by PHS in November 2022 and the review and redevelopment of the cluster guidance.
A suicide response workshop was developed to support local areas in their preparedness around suicide clusters.
Work to support the roll out of a standard Police notification form has also supported discussions around cluster response.
Work is ongoing to review the PHS cluster guidance with a view to updating based on knowledge and insight from supporting local areas and strengthening the guidance around CYP.
PHS is also exploring the potential of an early warning system for new and emerging methods either by dovetailing with existing processes or developing a specific process for methods specific to suicidal behaviour.
Action 6.3: Lived Experience Model – Lived and Living Experience Panel (LLEP)
The LLEP has been fully operational since January 2024 and has held monthly meetings with the full panel – a mix of online and in person, with engagement from colleagues across Suicide Prevention Scotland. The monthly meetings are well attended with participation from across the panel.
Sub-groups have also formed to focus on specific pieces of work including co-production of campaign strategy, development of online portal and personalised risk management (NCISH).
All panel members have received Introduction to Suicide Prevention training, plus sessions on sharing safely and maintaining boundaries. Work is also underway to facilitate SMHFA, ASIST and Wave After Wave training for panel members.
All panel members have had at least one 121 meeting with the lead for wellbeing and training focussing on their wellbeing.
Initial feedback from Panel members on their experience is overwhelmingly positive, with panel members reporting they enjoy the work, they feel safe and supported and are feeling benefits to their own mental health through their participation. Some suggestions for improvement which will also be taken into consideration (e.g. evening meetings aren't working out well for everyone; general preference for in-person over online).
Suicide Prevention Scotland continues to look at ways we can improve engagement with the LLEP.
Action 6.3: Lived Experience Model – Youth Advisory Group (YAG) and Participation Network
The group has shared their views on a number of key topics that are important to them to inform the work of Suicide Prevention Scotland and the delivery of Creating Hope Together. This has included:
- The suicide prevention needs of children and young people.
- The role of peer support for young people.
- Help seeking behaviour.
- Recommendations for clinical care.
Alongside delivering the Youth Advisory Group, Children in Scotland also deliver a Participation Network. The network meets 4-5 times a year and provides a space for practitioners working with children and young people to share their views and experiences on areas of Creating Hope Together. Most of the work with the group is aligned to the topics covered with the YAG to provide a space to share the YAG's views and to add weight to what we have heard.
Additional participation work to ensure we hear from groups not reflected within the Youth Advisory Group or where we feel there is value in hearing more about particular experiences has also taken place over the last year. This was delivered by OPEN in Shetland who shared about the experiences of young people on the island.
Action 6.4: Improving recording and reporting of suicide
PHS produces regular analyses of data on deaths by probable suicides. This includes:
- Management focused monthly reports to local areas on deaths from Police Scotland database covering name, gender, residence, location of incident and method used.
- ScotSID (Scottish suicide information database) reports on characteristics of those who have died by suicide - pulling together data from routine datasets covering maternal, prescribing, unscheduled care, mental health inpatient attendance - feedback has been sought from local and national stakeholders on the utility and scope of ScotSID publications to support improvements.
Over 2024/25 work has been undertaken to improve and expand datasets. This has included:
- Explore the extension of existing PHS datasets to include suicidal behaviour.
- Testing out a new format for monthly reports with local areas to address disparities between these and the published NRS data.
- Engagement with Police Scotland on their wider mental health and wellbeing datasets to include suicidal behaviour data.
- Identifying areas of collaboration and data linkages across PHS.
- Presenting the initial findings around existing self harm data collection (both intentional and non-intentional) to SG policy teams and other stakeholders to support the implementation of the self-harm strategy.
- Supporting local areas to consider how suicide data is currently collected and explore how appropriate datasets from a range of stakeholders might be identified and integrated at local level to support both forward planning and potential clusters/crises responses. Learning will support the review of implementation guidance to support local area action plans.
Action 6.5: Horizon scanning
An approach to this has been tested through the development of a briefing on safety planning which has been shared with local Suicide Prevention Leads for comment. Further work will be undertaken to review whether this is an approach that could be applied to other emerging developments around suicide prevention
Action 6.6: Multi-agency suicide reviews and learning system
A series of online sessions were held with local Suicide Prevention Leads and national partners to raise awareness of the QES system components and encourage update. This system will enable:
- Local areas to record and report on reviews of deaths by probable suicide.
- National reports to be developed by PHS using local data extractions.
The system's baseline dataset was adapted to produce a Scottish relevant dataset with the agreement of national data managers and local areas this included fields to identify the impact of inequalities.
Four areas have undertaken system training and are now using the system with three further local authorities in the process of adopting and five further local authorities expressing an interest.
Regular meetings of those using the system are hosted by PHS to support shared learning on a continuous basis.
PHS has worked with Police Scotland to finalise their suicide death notification form for use across Scotland and in particular with those using the electronic reporting system. Ongoing feedback on the form's use is being sought so that learning can be shared and improvements made as appropriate.
Engagement with other review systems such as the Child Death Review process and the SAER process has taken place to share learning and facilitate common approaches.
Action 6.7: Host learning events
Over 2024/25 a number of different events have taken place to bring together people working across different sectors with an interest in suicide prevention and to allow opportunities for people affected by suicide to come together. These events include:
Side By Side After Suicide (Sept 2024) which brought together around 80 people from across Scotland and provided an opportunity for peer support, to connect with others and to learn about the support available across Scotland and the different ways people have coped with their grief.
Building Connections events – focused sessions to help progress work under outcome 3 have taken place with invited trusted organisations with a focus on gendered perspective on suicide and self-harm.
Suicide Prevention Network meetings – these sessions provide opportunities for a wide range of stakeholders to come together, to hear about activity happening at a national level and to contribute to its development and delivery. There are over 300 people now registered on the Network and the sessions are always well attended.
Webinars – a number of webinars have been delivered throughout 2023/24, these include neurodiversity and suicide, self harm, online harms, social media after a suicide, implementing recommendations from the Delphi study and trauma informed practice and suicide prevention. The webinars are well attended by a broad range of sectors.
Gathering Hope event (January 2025) – this provides an opportunity for third sector organisations from across Scotland to come together, network and learn about the work happening across Scotland. Over 70 organisations attended this event, and the feedback was overwhelmingly positive recognising the benefit of connecting with others working in suicide prevention.
SPIL Led events and meetings – These include the monthly drop-in sessions for local Suicide Prevention Leads which provides a space for them to hear about progress on national delivery of CHT, connect with the NDL and outcome leads and provide insight from their local experiences. In addition to these regular meetings, workshops on communications and Gypsy Traveller Awareness have also been held.
Who with
| Who with: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| People developing and implementing policy relating to inequalities and social determinants that impact on suicide at local and national levels | Some progress; high confidence |
| People and organisations whose work contributes to addressing inequalities and social determinants that impact on suicide | Some progress; some confidence |
| Suicide Prevention Scotland Delivery Collective | Some progress; some confidence |
| People working with people at risk of suicide or affected by suicide | Some progress; high confidence |
| People and communities with lived and living experience of suicide or the inequalities and or social determinants that impact on suicide | Some progress; high confidence |
Across the actions working towards outcome 4 this year, we engaged with:
- 4 panels of people with lived and living experience: Scottish Government Care Experienced Group; Youth Advisory Group; Lived and Living Experience Panel; Participation Network.
- 2 teams in local and national government: Local Suicide Prevention Leads; National Suicide Prevention Advisory Group (NSPAG).
- 1 membership organization: Scottish Federation of Housing Associations (SFHA) and members.
- 1 media organization: Electrify
- 5 commissioned service providers, voluntary sector and community groups: SAMH; Samaritans; Penumbra Mental Health; V&A Dundee; MECOPP.
- 1 research team: the Academic Advisory Group
- 7 public bodies, health boards and HSCPs: Four nations suicide prevention colleagues, including Public Health Wales; NHS24; Police Scotland; Public Health Scotland and local public health teams; Scottish Ambulance Service; Scottish Fire and Rescue Service; Scottish Prison Service.
Action 6.1: Suicide prevention action plans in high-risk settings
Initial work has been with leads within identified stakeholder sectors:
- justice setting - particularly through Police Scotland and Scottish Prison Service
- housing setting - particularly through the Scottish Federation of Housing Associations and then further engagement with selected local housing associations
- care experienced - initially through the SG managed Care Experienced Group with further engagement with individual providers
Engagement with the Lived and Living Experience Panel resulted in members offering to support this work with individual members linked to different sectors – their role is to provide that lived experience perspective both in relation to developed resources but also work alongside sectors as they develop their action plans.
Action 6.2: Suicide cluster guidelines
Local area Suicide Prevention Leads, public health teams and Police colleagues, wider PHS colleagues including those linked to drugs/alcohol and mental health work, suicide prevention colleagues across the four nations (including links to Public Health Wales who are developing cluster guidance).
Action 6.3: Lived and Living Experience Model
Panel members have engaged directly with the following:
- SAMH (online portal, help seeking)
- Samaritans (Whole of Government - annex A)
- Electrify (campaign co-production; social media)
- AAG (access to means study)
- Delivery Lead (various)
- SG/Linda Hunter (TSC/personalised risk management in clinical settings)
- Penumbra (community led action research) joining July meeting
- NSPAG (quarterly meeting Jan 2024)
- NHS24 (Surviving Suicidal Thoughts video)
- PHS (outcome 4)
It is worth highlighting that YAG includes young people who experience inequalities including:
- Young people living rurally
- Care experienced young people
- Young carers
- Members of the LGBTQ+ community
Action 6.4: Improving recording and reporting
The primary stakeholders include Public Health Scotland and national stakeholders such as NHS 24, SAS, Police Scotland, SFRS and third sector agencies. Both quantitative and qualitative datasets are being gathered to build up a better picture of suicide related data.
Action 6.7: Host learning events
Learning events have been attended by a wide range of people and organisations from across Scotland representing all sectors.
How they feel
| How they feel: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| That suicide prevention is important, effective, will benefit everyone, and requires an holistic approach | Some progress; some confidence |
| People and / or organisations see how they can contribute to preventing suicide and are inspired to play their part | Some progress; some confidence |
| Safe, listened to, valued, included, encouraged, supported, and empowered | Great progress; some confidence |
Outcome 4 includes the co-ordination of the Lived and Living Experience Panel, Youth Advisory Group and Participation Network. These have been carefully designed and established to ensure meaningful participation with support and recognition for those involved. Members of these groups describe the experience of being involved:
‘I think it works really well. I appreciate having the agenda in advance to 'prepare' both mentally and in terms of content. Meeting frequency is appropriate and I always feel heard in discussions.’ (Lived and Living Experience Panel member)
‘Co-ordinators do a very good job of keeping an eye on who wishes to speak and definitely make a concerted effort to ensure everyone who wants to contribute is heard.’ (Lived and Living Experience Panel member)
‘Without sounding too over the top the biggest highlight for me has been being heard. Sometimes living with mental health issues and having survived suicide attempts feels like living with a dirty secret. For the first time it feels like something positive can come out of such a dark period of my life...I'm so incredibly grateful to have been given the opportunity to be part of this and I'm enthusiastic about everything we can achieve together.’ (Lived and Living Experience Panel member)
‘Thank you to both Tracy and Keir for making this panel an enjoyable and safe space. They make talking about the S word (haha) less traumatic and instead actually healing, all while helping others.’ Lived and Living Experience Panel member
'I’ve enjoyed it all, I feel like there has been a lot of opportunity to get involved with things this past six months. And I’ve had the opportunity to really have input to work being done.' (Youth Advisory Group member)
‘I'll go and read the Insight Report properly, and the development plan for year 2. I want to get in touch with professionals who can come and deliver some in-person whole staff training (we are a very small staff of 13!) on supporting yp with self-harm, suicide ideation, and they'd be interested to understand all the work that's going on in the background’ (Participation Network member)
What they learn and gain
| What they learn and gain: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| We understand the context for implementation and what this means for effective delivery | Some progress; some confidence |
| Understand existing good practice, gaps, what needs to change, the priorities for action and possible solutions | Some progress; low confidence |
| Awareness of suicide, risk factors, and understand what to do to prevent suicide and tackle associated inequalities and social determinants | Some progress; some confidence |
| Improved information systems and timely and actionable data and information about suicide risks, deaths, clusters and trends | Some progress; some confidence |
| Knowledge, confidence, skills, resources and support to provide effective and compassionate support to people at risk of / affected by suicide | Some progress; high confidence |
Action 6.1: Suicide prevention action plans in high-risk settings
Those engaged in this work have developed an appreciation of the complexity of suicide prevention and an understanding that having the courage to take small steps and monitor progress without overextending themselves is key to improvements.
Action 6.2: Suicide Cluster Guidance
Informal feedback around the clusters guidance and support has been positive with local areas identifying opportunities to improve the response to suspected clusters through multi-agency engagement.
Action 6.3: Lived Experience Model
Opportunities for personal development are a key part of contributing as a LLEP member. The continued development and training for the panel is improving their knowledge, confidence and skills in suicide prevention work. They have shared that they are now feeling more comfortable in having conversations about suicide as a result of their training, and their membership of the LLEP.
One LLEP member was a central part of the Side by Side After Suicide event, recording her story for use on our social media channels, and also speaking on the day. She reflected afterwards that she wouldn't have had to confidence to do this a few years ago and partly credits her involvement with the LLEP and the wider Suicide Prevention Scotland collective in building her up to do this.
Engagement with LLEP, YAG and PN has also been invaluable in work across the action plan with involvement in the design, development and delivery of all actions ensuring the guiding principle of co-developing work with people with lived and living experience is enacted.
Action 6.4: Improving recording and reporting of suicide
By improving the data and evidence available, we will be able to develop evidence informed action to reduce suicide across all sectors at local and national level.
Action 6.6: Multi-agency suicide reviews and learning system
Through this approach we expect to see improved collaboration across different stakeholders around the review process as well as improved shared learning on what service responses might be required to reduce further deaths at both local and national levels.
Action 6.7: Host learning events
By delivering learning events, we expect to see improved understanding and awareness of suicide and realise our ambition to build Suicide Prevention Scotland as a network of people with an interest in or working in suicide prevention.
Case study: Gathering Hope 2025 (Outcome 4, Action 6.7)
What we have done:
We host learning events that bring people together to share learning and good practice between and across sectors on suicide prevention.
Gathering Hope 2025 focused on the role of stigma and discrimination as a common experience across different groups and communities, exploring how this increases suicide risk, and sharing promising approaches to address this.
Who with:
Gathering Hope 2025 brought together 70 third sector organisations working to prevent suicide in Scotland.
(Image caption: Organisations working together at Gathering Hope 2025)
How they feel:
A participant in the event provided the feedback:
“Networking, communication, community, warmth and kindness... I attended last year and this year and was left, both times, with a warm and fuzzy feeling of connection and strength.”
What has been learned and gained:
People who attended Gathering Hope 2025 told us they were taking away new knowledge about supporting members of the LGBTQ+ community and planning to reflect further on the input around data, recording, and funding/sustainability.
They valued the opportunity to meet and network with like-minded people, especially through group conversations during the conversation cafés. This gave them new insight into what other organisations are doing and the goals and challenges they have in common.
What is being done differently?
People shared their enthusiasm and increased confidence to follow up new connections, seek out other organisations in their local area, visit other organisations and explore more partnerships and collaborations.
Others planned to access the signposted resources and training and reflect their learning in their practice and services. For example, several organisations said they would be implementing learning in the way they engage with and support members of the LGBTQ+ community.
What difference will this make?
The Gathering Hope events are building the network between organisations working to prevent suicide in Scotland, disseminating knowledge about new research and promising approaches and building consensus around good practice. Effective campaigning will raise public awareness, and we will seek to measure change in public attitudes.
This will contribute towards suicide prevention work across Scotland, whoever is delivering it, being informed by lived experience insight, practice, data, research and intelligence, so that people affected by suicide are consistently able to access high quality, compassionate, appropriate support.
What they do differently
| What they do differently: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Work with wider stakeholders and partners to prioritise, plan, commission and deliver the work | Some progress; some confidence |
| Take action to prevent suicide and tackle the impact of inequalities and social determinants that impact on suicide | Low progress; low confidence |
| Take co-ordinated and collective approaches to raising awareness and continuing to build the suicide prevention community | Some progress; some confidence |
| Use quality data and appropriate evidence to inform priorities, develop interventions and make effective decisions | Some progress; some confidence |
| People and organisations play their part in scaling up and embedding effective interventions | Not currently rated as work has not begun. |
Overall Outcome 4 aims to ensure our work on suicide prevention is well planned and delivered through close collaboration between national, local and sectoral partners. Taking an approach to our work which builds in lived and living experience, practice-based evidence, academic evidence and improved data and intelligence ensures we are embedding a co-ordinated, collaborative and integrated approach. Work to ensure we have robust monitoring and evaluation processes in place to measure the impact of our work also sits under Outcome 4 and will help ensure we remain on track to deliver the ambitions of the CHT strategy and its associated action plans.
Due to the activity to deliver the actions in 2024/25, we are aware that:
- Many local areas are taking action and making improvements to their procedures and protocols following the launch of the clusters guidance and follow up discussions around cluster responses.
- LLEP members have reported improved confidence and awareness of suicide as a result of their participation in the work.
- there have been opportunities for the YAG to engage on a range of topics and their views have been used to inform priorities.
- analyses from the multi-agency reviews have enabled local areas to identify where service responses could be improved including reduction in access to means, supporting time space compassion approaches and postvention supports.
- Data and intelligence are being used across the delivery of the action plan to inform the approaches taken.
What difference does this make?
| What difference does this make: outcome map stepping stones | Rating of progress and confidence in the evidence to support this |
|---|---|
| Outcome 4: Our approach to suicide prevention is well planned and delivered - with close collaboration, co-design, evidence informed, ongoing improvement | Some progress; some confidence |
Work under outcome 4 has an impact across all outcomes. This work has helped ensure we are
- taking action based on learning
- initiating different and new options to monitor and evaluate progress with a mix of feedback from data, lived experience, staff voices and practice implementation
- celebrating success and encouraging open and transparent sharing of learning
- working towards having more integrated and detailed data at both local and national level with the aim of providing more data and intelligence around the impact of those inequalities that lead to suicidal behaviour
Local delivery of suicide prevention
Suicide prevention activity in local areas across Scotland was established with the implementation of the Choose Life suicide prevention strategy and action plan in 2002. Every Life Matters set out an ambition to support local areas to develop local action plans which was supported by the development of guidance for local leads, and the establishment of three Suicide Prevention Implementation Leads in PHS to support their needs and build strong connections between local and national work.
Over the last few years, an annual survey of the local leads has been undertaken which has attempted to capture both the practical aspects of the role as well as information about the focus of local delivery. In January 2025, the questionnaire was completed by 24 of the 32 local authority areas. A summary of the responses is set out below.
Leads were asked about their current capacity, experience and resource to deliver suicide prevention. It is clear from the responses that there is variation across the country with some areas having no dedicated role or resource and others having experienced, full-time roles with considerable funding to support local action.
Local leads identified that the lack of dedicated roles and budgets for suicide prevention presented some challenges to the ability to take action and build capacity, including the ability to provide training and learning resources. Where resource and capacity were available, they felt this significantly improved the ability to drive suicide prevention work forward.
They noted that their Suicide Prevention roles often overlap with other responsibilities, making it challenging to focus solely on suicide prevention. Local leads also cover topics such as drug-related deaths, mental health and health improvement. They highlighted the positive impact of collaboration across teams and sectors in supporting innovation and driving forward work.
There is a wide range of experience across the local leads. The Suicide Prevention Implementation Leads have played a part in providing ongoing support and induction work to those who have taken up posts over the last three years. There are many benefits to this range of experience which include opportunities for learning and support across areas.
Leads were asked about the status of their local suicide prevention action plan (see figure 1). Seventeen leads indicated they had a current plan which was specifically focused on suicide prevention, these included plans which covered more than one local authority area. The remaining responses all identified that a plan was in development, embedded in other wider topic action plans or that activity was underway without a firm plan in place. This compared to the previous year when 8 areas had a current plan or one awaiting publication, and 7 had plans in development.
Local leads were also asked if their action plans reflected the Creating Hope Together guiding principles (see figure 2) and whether they were supported by local senior leadership as set out in the Creating Hope Together strategy.
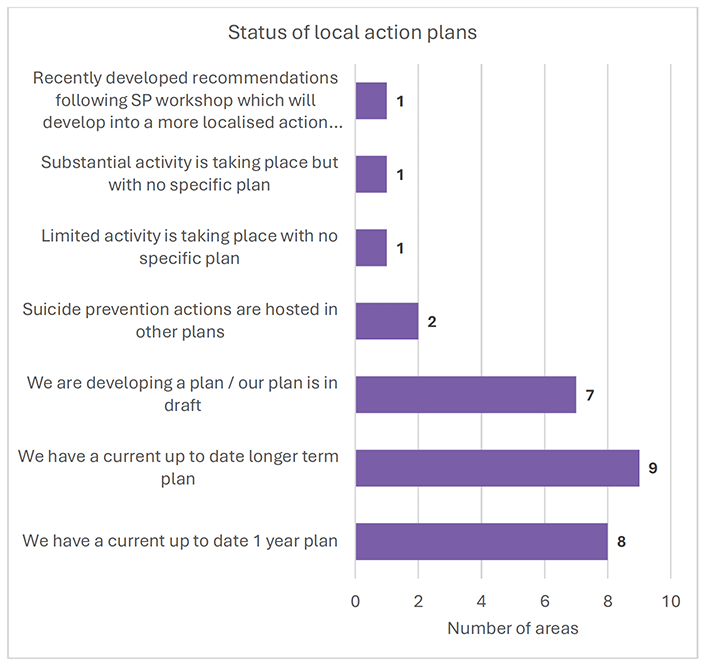
The graph below (figure 3) demonstrates that the vast majority of principles are embedded in local plans with only the participation of livesd and living experience being more challenging. We are aware of these challenges and are working to support local areas to enhance participation.
There was also evidence of strong local multi-agency partnerships and the majority of plans had senior leadership support.
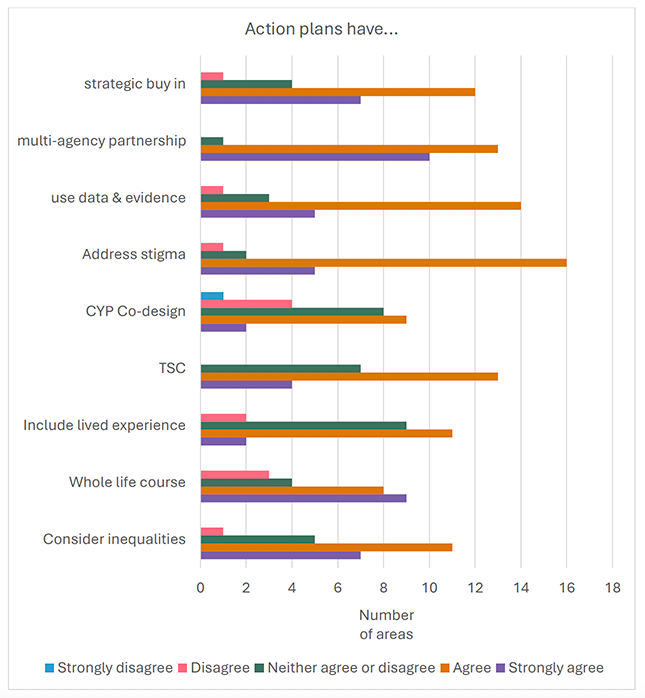
The ambition for Suicide Prevention Scotland is to create a network for people and organisations across sectors. The local Suicide Prevention Leads are a core group, and we have invested in various approaches to support their needs. These include the Suicide Prevention Implementation Leads (SPILs) and capacity building roles within PHS. Opportunities for local leads to come together to provide peer support, support learning, provide practice-based evidence which supports local and national work have also been established.
As part of our ongoing commitment to evaluation and review, we asked local leads for their views on what specific support they had received from the SPILs (figure 3), how connected they felt to the work of Suicide Prevention Scotland (figure 4) and how useful the communication approaches were to support their work (figure 5).
The majority of leads either agreed or strongly agreed that the SPILs had been supportive across all the domains. This includes specific developments or actions in local areas and also ensuring connection for local leads into national areas of work.
Local leads mentioned that SPILs have been instrumental in supporting local work and connecting stakeholders. They appreciated the individual approach taken by the SPILs, which considers the unique challenges and solutions of each location but also identified that at times there was a need for better understanding of local pressures.
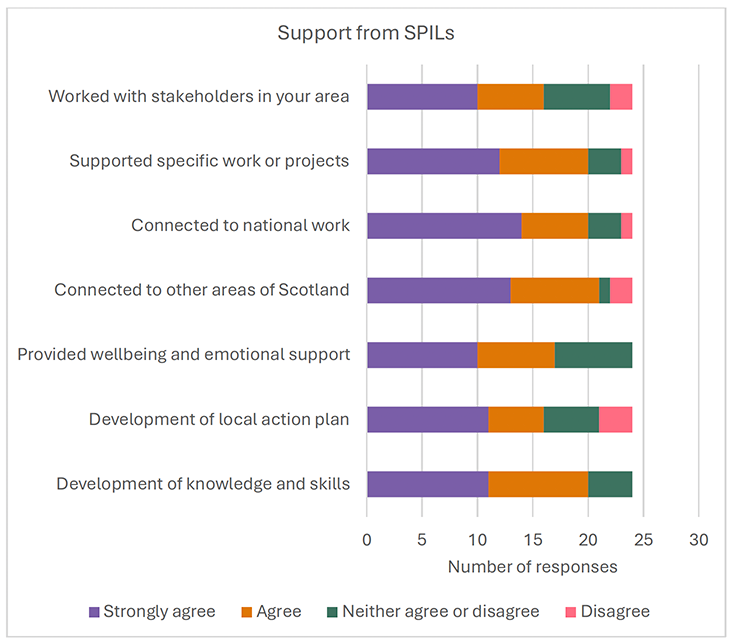
The majority of respondents also either agreed or strongly agreed that they felt connected and part of Suicide Prevention Scotland. Regular contact through national networks and local leads meetings are valued and updates from Suicide Prevention Scotland are appreciated, but the challenge of keeping up to date due to capacity was highlighted.
There were a small number of comments which mentioned that at times the number of requests from Suicide Prevention Scotland, the rationale for them and where they fit in the overall plan was unclear, however there is a strong appreciation for the work being done.
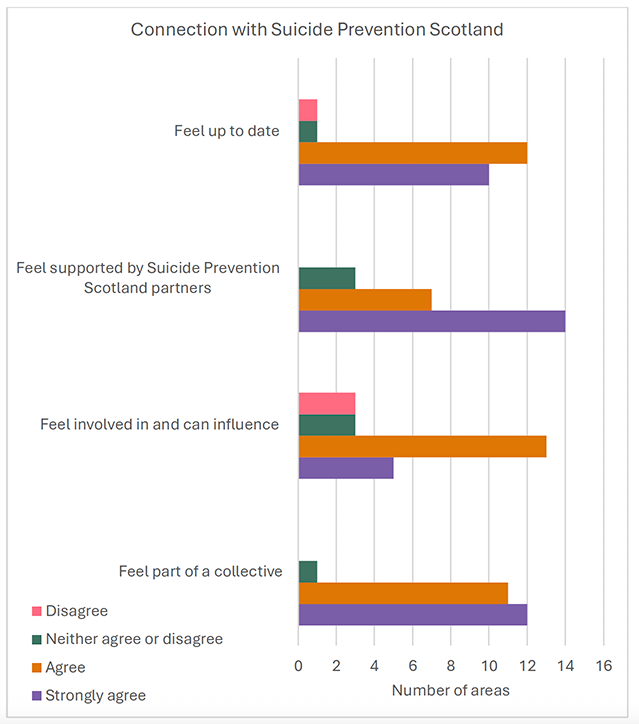
The local leads felt that some communication methods were more useful than others. Those that were felt to be most useful include emails, newsletters, network sessions and SPILs at 1:1 or steering group meetings. Social media channels were felt to be less useful for the local leads. Although feedback on support group for local leads and buddying, were also identified as being less useful, this is due to the small numbers who have taken part in these to date, for those who have been involved, these have been positive experiences and there is now a plan to extend the reach of these to make them available to all.
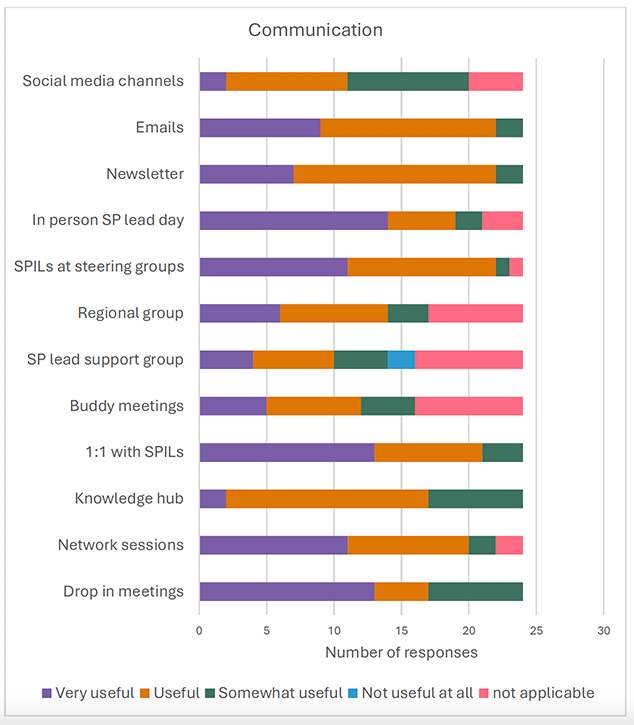
There was recognition of the importance of the various communication methods and the need to cater to different styles. However, they also mentioned that due to their capacity and local priorities the volume of information can be overwhelming.
Conclusions from the survey
The results of the survey will be used by Suicide Prevention Scotland to help shape our approach to communications and engagement with local Suicide Prevention Leads. It will also help shape the work plan to support local delivery for the coming year.
Contact
Email: Leeanne.McSharry@gov.scot