Creating Hope Together: Scotland's Suicide Prevention Action Plan 2026-2029
The second three year action plan of Creating Hope Together: Scotland’s Suicide Prevention Strategy (2022-2032)
Wider Context For Scotland’s Suicide Prevention Work In 2026-2029
Our understanding of suicide and how this informs our approach
This action plan takes an evidence-based approach to suicide prevention and covers a range of responses: prevention; early intervention; intervention; postvention; and recovery[3]. The pathways to poor mental health and suicide are complicated. To this end, our work is guided by the three phases of The Integrated Motivational Volitional (IMV) Model of Suicidal Behaviour,4 which provides a public health framework to understand and prevent suicide. According to the IMV model, suicide results from unbearable emotional pain which is influenced by social, psychological and biological factors.
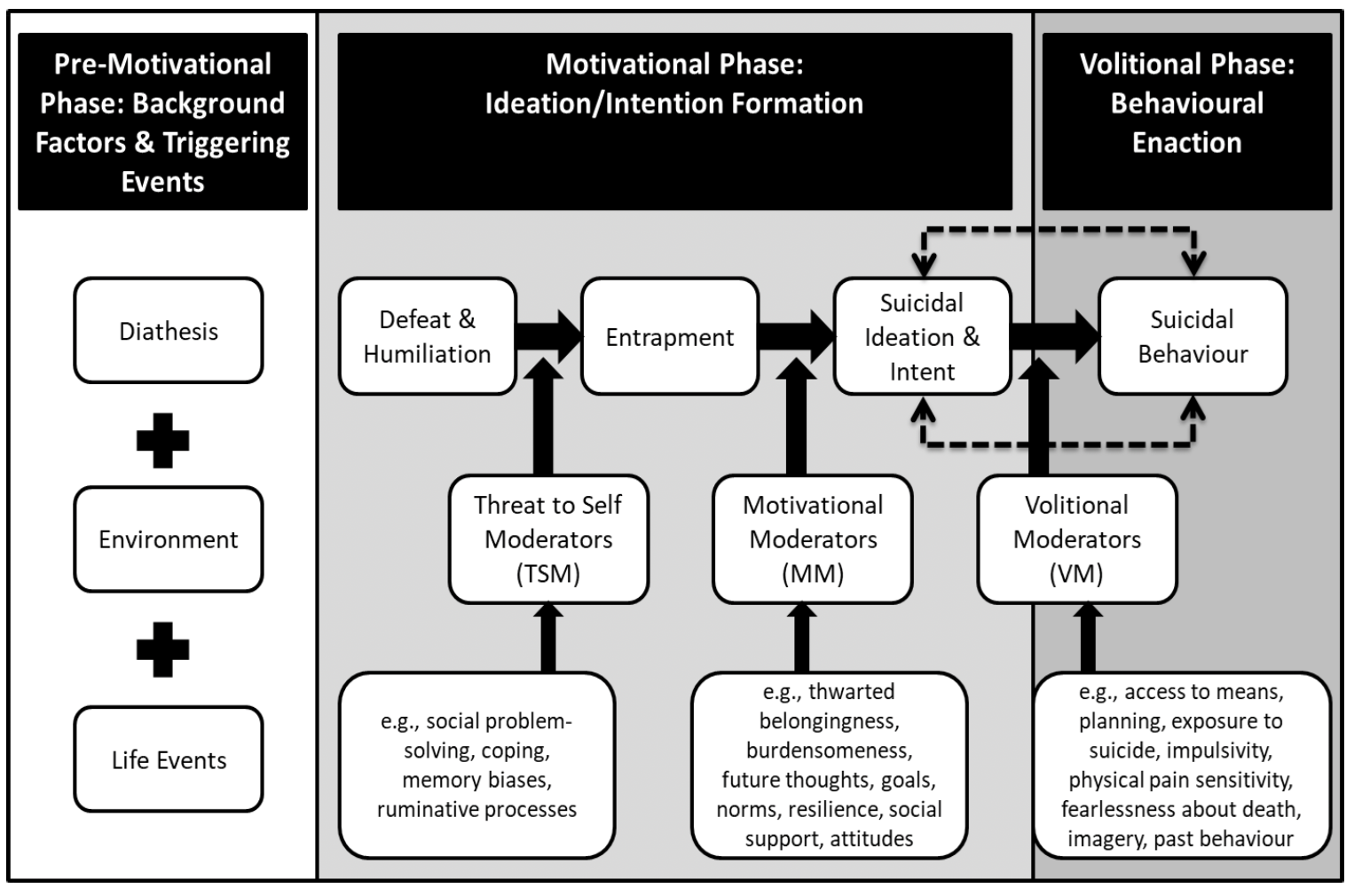
A conceptual diagram illustrates the Integrated Motivational-Volitional (IMV) Model of suicidal behaviour. The diagram is divided into three phases: Pre-Motivational Phase:
1. Background Factors & Triggering Events (left section)
Includes three stacked boxes connected by plus signs labelled:
Diathesis
Environment
Life Events
2. Motivational Phase: Ideation/Intention Formation (centre section)
Arrows connect three boxes showing progression from:
Defeat & Humiliation to
Entrapment to
Suicidal Ideation & Intent.
Between defeat and humiliation, and entrapment there is a box titled Threat to Self-Moderators (TSM).
Examples of Threat to Self-Moderators are provided:
Social problem-solving
Coping
Memory biases
Ruminative processes.
Between entrapment, and suicidal ideation and intent there is a box titled Motivational Moderators (MM).
Examples of Motivational Moderators are provided:
Thwarted belongingness
Burdensomeness
Future thoughts
Goals
Norms
Resilience
Social support
Attitudes
3. Volitional Phase: Behavioural Enactment (right section)
Shows Suicidal Behaviour connected to Suicidal Ideation & Intent with solid and dashed arrows representing cyclical nature.
Between suicidal ideation and intent, and suicidal behaviour there is a box titled Volitional Moderators (VM).
Examples of Volitional Moderators are provided:
Access to means
Planning
Exposure to suicide
Impulsivity
Physical pain sensitivity
Fearlessness about death
Imagery Past behaviour.
The diagram uses black and grey boxes with arrows to indicate progression and moderators influencing transitions.
The first phase of the model recognises that suicide risk is influenced by a range of vulnerability factors and social determinants. These can include early life adversity, marginalisation, stigma, socioeconomic inequalities and disadvantage.
The second phase of the model describes the pathway to the emergence of suicidal thoughts, specifically, that people become suicidal when they feel trapped by feelings of defeat and humiliation. Shame, rejection and loss can also contribute to the emotional pain that drives suicide risk.
Finally, the third phase of the model posits that people are more likely to act on their thoughts of suicide when certain factors are present, such as when they have ready access to the means of suicide. In this action plan, to maximise our reach, we address each phase of the model by focusing on targeted clinical interventions as well as taking a wider public health approach. Each of these phases is further shaped by social, cultural, political and economic factors.
Across national and local government, statutory and third sector services, further and higher education and in our communities, we are focused on addressing the key drivers and underlying causes of poor mental health and increased suicide risk. We have a particular focus on: poverty/child poverty; education; being care experienced; employment and employability; housing and homelessness; substance use; domestic abuse; and criminal justice. We recognise that, locally, these issues may impact individual people differently and that people could be experiencing more than one of these factors, compounding potential risks. We also hold in mind that factors such as gender, age, ethnicity, religion and sexual orientation can further shape the likelihood and nature of suicide risk, and how it is recognised and responded to.
Recognising the important role that different people, communities and sectors across Scotland have in supporting mental health and wellbeing, our efforts are focused on working collaboratively with partners and communities across the system to ensure a whole system approach is being taken to address the underlying causes of poor mental health and drivers of suicide.
Actions to tackle these are being delivered through a wide range of cross-cutting strategies and policies, such as:
- Scotland’s Population Health Framework
- The Mental Health and Wellbeing Strategy
- The Self-Harm Strategy and Action Plan
- The Tackling Child Poverty Delivery Plan
- The Promise
- Ending Destitution Together Strategy
- The Student Mental Health Action Plan
- No One Left Behind - Employability Strategic Plan
- The Fair Work Action Plan
This includes a range of preventative approaches in non-clinical settings/frontline services. One example of this is our joint work with Scottish Prison Service (SPS) to support the development of their approach to suicide prevention in prisons, ensuring that this is consistent with the broader vision and approach set out in our national suicide prevention strategy. Another example is our work with employability partnerships and employers to create and promote mentally healthy workplaces, ensuring more people are able to access and remain in work.
It also includes work to develop an understanding of mental health and suicide prevention in local communities, ensuring there is a range of provision and capacity at that level. For example, the grass-roots community projects supported through the Communities Mental Health and Wellbeing Fund for Adults are supporting individuals and groups disproportionately at risk of poor mental health, ensuring that support is available in local communities across Scotland.
Wider action to support people in distress and crisis, who may also be suicidal, is also underway and contributes to our collective efforts to prevent suicide. As well as our Distress Brief Intervention (DBI) programme, we are also undertaking collaborative work with a range of national partners, including our emergency services, to improve unscheduled care. Together this has made a significant contribution to improving mental wellbeing and reducing suicide risk. This action plan will build on and strengthen that work to maximise opportunities to connect this work across our policies, services and communities and prevent suicide.
“Suicidal thoughts should be taken seriously, people are reaching out for help at this point to try to prevent suicidal acts, there should be help available at that point to prevent people dying.”
Workshop participant
Building On Our First Action Plan
The Action Plan for 2022-2025, published in September 2022, set out the actions to implement the first stage of the Scottish Government and COSLA’s long-term suicide prevention strategy.
More information[5] about work under the first action plan includes:
- Suicide Prevention Scotland’s annual delivery plans which provide further detail of the work taken forward in each of the three years
- annual reports set out progress against these delivery plans
- annual reports from our independent National Suicide Prevention Advisory Group