General practice contractors - sufficient involvement: consultation analysis
Summarises feedback from 59 respondents in 2024 on whether current regulations governing sufficient involvement for GP contractors are appropriate. The purpose of the regulations is to ensure GP contractors are engaged in day-to-day provision of primary medical services.
Questions
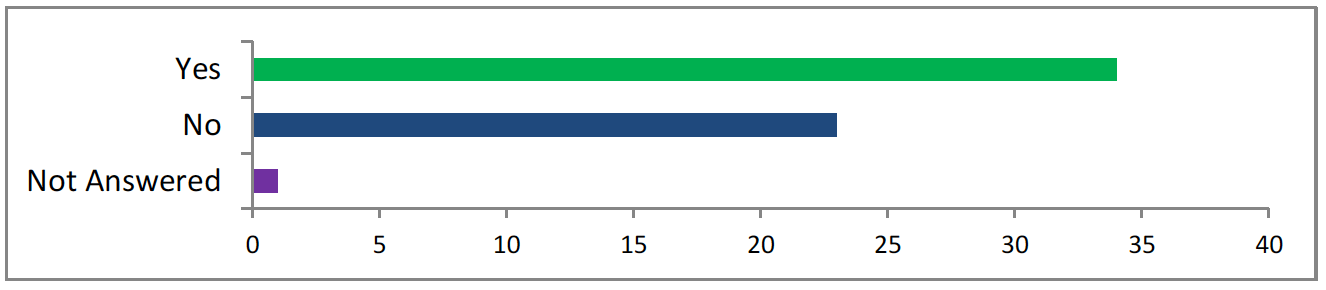
Question 1: Is 10 hours a week performing or engagement in the day-to-day provision of primary medical services a reasonable requirement for eligibility to be a GP contractor? If "no", what is the right amount of time?
Overview
The question asks whether requiring a GP contractor to engage for 10 hours a week in the day-to-day provision of primary medical services is a reasonable eligibility criterion. It also seeks suggestions for a more suitable time requirement if 10 hours is deemed insufficient.
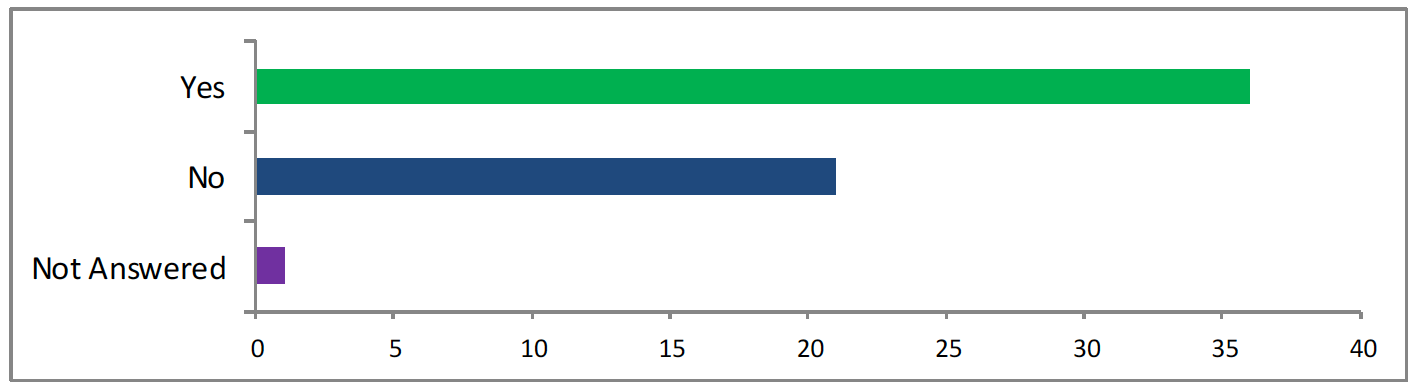
<36 answered yes, 21 answered no, 2 did not answer>
Key themes
- Appropriateness of 10 Hours
- Many respondents stated that 10 hours per week is too low, suggesting alternatives ranging from 15 to 24 hours, often tied to the need for more substantial involvement in patient care and practice operations.
- Concerns were raised about the adequacy of 10 hours per week for ensuring continuity of care, clinical competency, and patient safety. Some argued that more hours are necessary to maintain skills and provide consistent, high-quality care.
- There is a strong emphasis on the need to average hours over a longer timeframe to support flexible working arrangements, particularly in rural or remote settings. Many respondents noted that rigid weekly requirements could undermine successful job-sharing, locum arrangements, and succession planning.
- Definition of engagement
- The term "performing or engagement" was flagged as needing clearer definition. Respondents highlighted the distinction between direct clinical care (e.g., consultations) and broader roles such as managerial duties or supervision. Some suggested the requirement focus specifically on clinical care hours.
- Workforce and recruitment
- Several responses indicated that rigid requirements could discourage younger GPs from taking on contractor roles and lead to earlier retirements among older GPs. The need for flexibility was linked to workforce retention and attraction, particularly in rural and remote areas.
- Some noted that enforcing a fixed time requirement could deter doctors from taking on principal roles, exacerbating workforce challenges.
- Rural and remote practices featured prominently with many respondents noting that inflexible requirements could disrupt successful models that rely on locums or rotational coverage.
Conclusion
The responses underscore a consensus that the 10-hour requirement needs to be re-evaluated, with flexibility, rural practice considerations, and a clear definition of "engagement" being central to any proposed changes. While some support 10 hours, many believe it should be increased or at least made flexible over time to better reflect modern workforce needs and ensure the sustainability of primary care services.
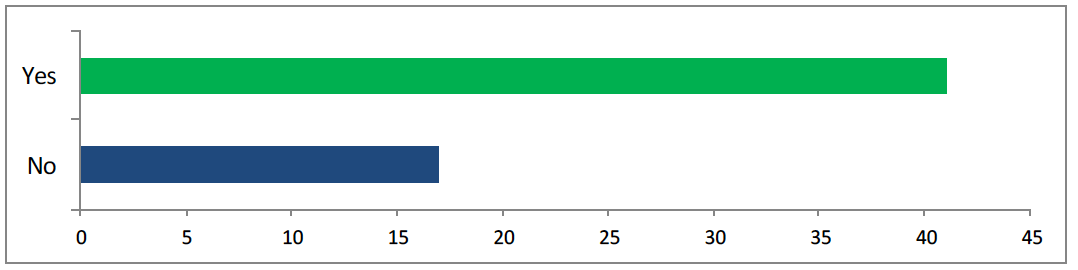
Question 2: Is the requirement to perform or engage in the day-to-day provision of “primary medical services” a sufficient requirement? Please give your views
Overview
The question on whether engaging in the provision of "primary medical services" is sufficient. Key themes included the need for clearer definitions, the balance between clinical and managerial roles, and concerns over absenteeism. Many emphasised direct patients care as essential, while others highlighted the evolving responsibilities of GPs and the need for flexibility in practice models.

<42 answered yes, 17 answered no>
Key themes
- Ambiguity of terminology
- Several responses stressed the vagueness of “perform or engage in the day-to-day provision of PMS”. Clarity is needed, especially to distinguish between direct patient care and administrative or managerial roles. Terms such as “primary medical services” and “engagement” require explicit definitions to avoid inconsistent interpretations.
- Rural and remote practices often rely on non-traditional models, such as rotational staffing or shared responsibilities. These practices might struggle to meet overly rigid definitions of “engagement” or “provision”.
- Respondents noted that general practice has evolved, with portfolio careers, remote working, and specialized roles becoming more common. Any requirements should be flexible enough to account for these modern arrangements without compromising care quality.
- Many respondents emphasised the importance of direct patient care as a fundamental requirement for GP contractors. Suggestions included stipulating a specific number of hours dedicated to patient-facing roles or patient-related activities such as consultations and referrals.
- Role of management and leadership
- There is recognition that modern GP roles, especially for partners, often involve significant managerial and leadership responsibilities, including overseeing multidisciplinary teams. Some stated that these responsibilities should be explicitly included under PMS.
- Multiple responses expressed concern about contractors being disengaged from practice operations, delegating clinical work entirely to salaried staff while focusing on profit. The term “absentee landlordism” was frequently used to criticise this model.
Conclusion
The responses reflect that the current wording of "performs or is engaged in the day-to-day provision of primary medical services" is too vague. A combination of direct patient care and practice-related responsibilities, with clearer definitions to prevent abuse and promote quality care. The need for flexibility in rural and modern practice contexts is also a recurring concern, balancing clinical, managerial, and leadership responsibilities in a way that maintains the integrity of primary care services.
Question 2.1: Should GP contractors be required to perform or engage PMS activities in the practice area they are or will be contractors in or should they be allowed to continue on a wider basis? Please give us your views
Overview
The question asked whether GP contractors should be required to engage in providing PMS within the specific practice area they are contracted for, or if they should be allowed to continue operating on a broader basis.

<37 answered “in a practice they are or will be”, 22 answered “on a wider basis”>
Key themes
- Impact on continuity of care
- A significant portion noted that contractors should prioritise serving their practice areas, with concerns that multi-contract arrangements can dilute focus, compromise continuity of care, and lead to absentee leadership. This can be addressed by setting minimum required hours for direct involvement.
- Respondents stressed the need for contractors to be actively engaged in the communities they serve. Ensuring personal investment and continuity of care were cited as essential for patient outcomes and community trust.
- Challenges in recruitment and retention
- The pressures of recruiting and retaining GPs were frequently cited, with suggestions that strict area-specific requirements could worsen staffing challenges. Flexibility in roles and work locations was seen as a potential mitigator for these issues.
- Many respondents emphasised the importance of flexibility, particularly for rural and remote practices. They noted that allowing GPs to operate across a wider area enables the sharing of specialised expertise, which smaller or remote practices might not otherwise access.
- Some respondents highlighted the operational and financial inefficiencies of multi-contract models, citing reduced patient satisfaction, weaker clinical governance, and over-reliance on locum staff.
- Recommendations included setting proportional requirements for contractors based on practice size, mandating direct patient care hours, and ensuring oversight mechanisms for service quality in multi-contract arrangements.
Conclusion
The responses reveal a balance between ensuring GP contractors are actively engaged in their practice areas and maintaining flexibility for broader health needs. Many support requiring contractors to prioritise local patient care while allowing flexibility for rural practices and system-wide contributions. A tailored approach with minimum local care commitments could address these concerns effectively.
Question 3: Should a proportion of the time a GP contractor must spend working in the practice area to be considered 'sufficiently involved' be spent working from the practice premises? If "yes", what proportion of time?
Overview
The question focuses on whether GP contractors should be required to spend a proportion of their time working in the practice premises to be considered ‘sufficiently involved’
<42 answered yes, 17 answered no>
Key themes
- On-site presence
- The suggested proportions vary widely, with the majority agreeing that at least 50% of the time should be spent in the practice premises. Some responses advocate for 100%, while others suggest a flexible approach around 50–80%.
- While remote working is acknowledged as useful, especially in rural or constrained settings, it is generally viewed as supplementary to on-site presence to maintain continuity of care, clinical governance, and teamwork within the practice.
- Rural practices
- There is concern that rigid on-site requirements could negatively impact remote and rural practices by limiting access to sub-specialised GPs or making it difficult to cover annual leave and other needs without compromising patient care.
- On-site presence is seen as essential for fostering clinical leadership, team support, and direct patient interaction. Special considerations are needed for rural practices, where flexible arrangements must be balanced with practical limitations.
Conclusion
Most responses support a requirement for at least 50% of the time to be spent working on-site in practice premises. While remote working is recognised as beneficial for certain tasks, it should serve as a supplementary option rather than a substitute for physical presence. Flexibility is essential, especially for rural practices where infrastructure and resources may be limited, but maintaining regular clinical involvement in-person is seen as critical for ensuring continuity of care, effective patient management, and strong team leadership.
Question 3.1: Should GP contractors be required to perform or engage in PMS activities in the area of the Health Board they have or will have a contract with? If "yes", how much time?
Overview
The question addresses whether GP contractors should be required to engage in PMS activities within the Health Board area they are contracted with, and if so, how much time they should spend doing so. Responses reflect a wide range of opinions, balancing the need for local engagement and flexibility with the challenges of remote and rural practice settings and the complexities of Health Board boundaries.
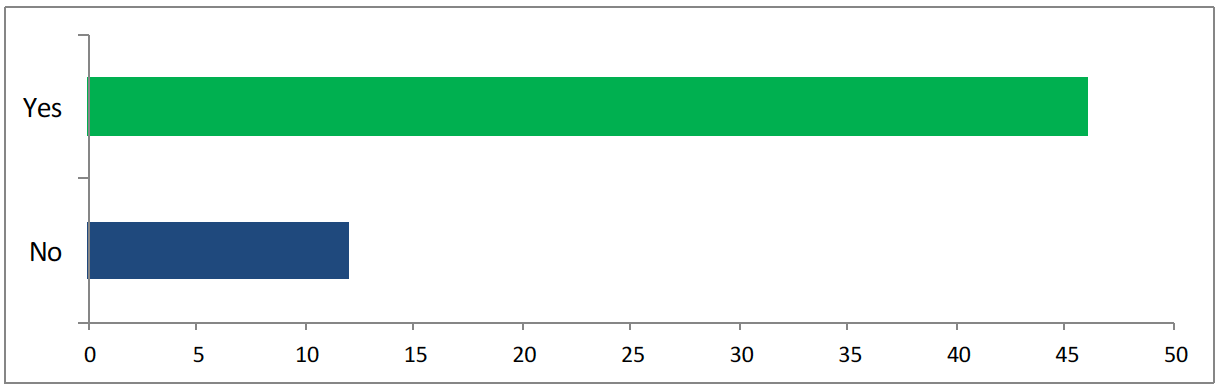
<47 answered yes, 12 answered no>
Key themes
- On-site engagement
- Majority of responses advocate for a minimum of 50% to 100% of time to be spent performing PMS activities within the Health Board area. Remote or part-time engagement is acknowledged but should supplement, not replace, on-site involvement.
- GPs should remain engaged in their contracted Health Board for primary care responsibilities, supporting community engagement and providing visibility for stakeholders.
- Flexibility and time
- While flexibility is necessary, particularly in rural or overlapping Health Board areas, consistent and local involvement is emphasized for maintaining continuity of care, relationships, and team cohesion.
- There is support for shared responsibilities and collaboration between practices, allowing for some flexibility within Health Board areas to meet broader healthcare needs.
- Managing responsibilities across multiple Health Boards is seen as a challenge, with calls for clear accountability and minimal disruptions in patient care and service continuity.
- Minimum time requirements vary widely from 10 hours to 20+ hours per week, with a strong emphasis on at least a portion of this time being allocated within a single practice.
Conclusion
Majority of responses highlight the importance of a minimum requirement for GP contractors to perform PMS activities within their Health Board area. While flexibility is acknowledged, particularly for rural and overlapping Health Board areas, on-site involvement is deemed crucial for continuity of care, team leadership, and effective engagement with local communities. The varying minimum time requirements reflect a desire for balance between consistency and adaptability in primary care provision.
Question 3.2: Should a GP contractor who is a partner in more than one practice in a Health Board’s area, be required to perform or engage PMS activities in each practice? If "yes", how much time?
Overview
The question explores whether GP contractors with multiple partnerships should engage in PMS activities across all their practices and how such time should be allocated. It addresses issues of fairness, feasibility, and the impact on healthcare delivery across different settings, particularly in remote and rural areas.
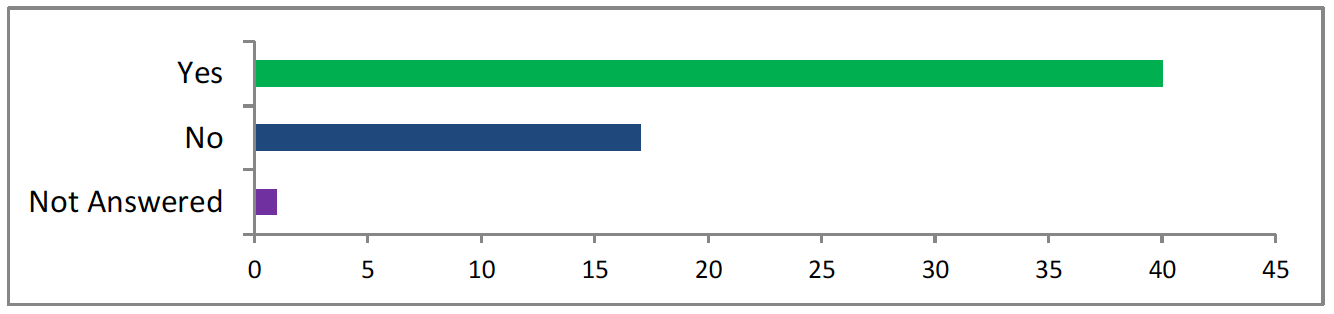
<41 answered yes, 17 answered no, 1 did not answer>
Key themes
- Time allocation
- Many responses support equitable division of time between practices (e.g., equal split, proportional to list size) to ensure that all practices benefit from the contractor's expertise and leadership.
- Suggestions for averaging hours over a period or setting minimum thresholds (e.g., 10 hours per week per practice) were common. A significant proportion of respondents advocate for a time commitment of at least 10–20 hours per practice per week.
- Some responses suggest alternative frameworks, such as allowing practices to collectively meet requirements based on patient numbers rather than individual GP time allocation.
- Flexibility and practicality
- Flexibility is considered critical, with some responses emphasising that strict time requirements may not be feasible, especially for rural or geographically distant practices.
- Concerns were raised about potential conflicts of interest and the practicality of managing responsibilities in multiple practices, particularly during emergencies or times of high demand.
- The role of GP contractors in maintaining continuity of care and building team relationships was emphasised, which may be challenging when dividing time across practices.
- Rural and remote practices
- Requiring engagement in multiple practices could disproportionately affect rural areas where long travel times and smaller practice sizes create logistical challenges.
- Responses highlight the need to balance accessibility to specialist skills with the realities of rural practice management. There is general agreement that active and visible involvement in each practice is important for maintaining high standards of care and operational efficiency.
- Many respondents stressed that GP contractors must have meaningful involvement in each practice, beyond token participation. This includes responsibilities for patient care, team oversight, and engagement with local populations.
Conclusion
While there is widespread agreement that GP contractors should engage in PMS activities in each practice they hold a partnership, there is less consensus on how time should be allocated. A flexible, proportional framework – allowing for minimum thresholds while accommodating local and operational variances – may provide a practical solution. Ensuring meaningful involvement in each practice is critical for continuity of care, effective leadership, and equitable healthcare delivery.
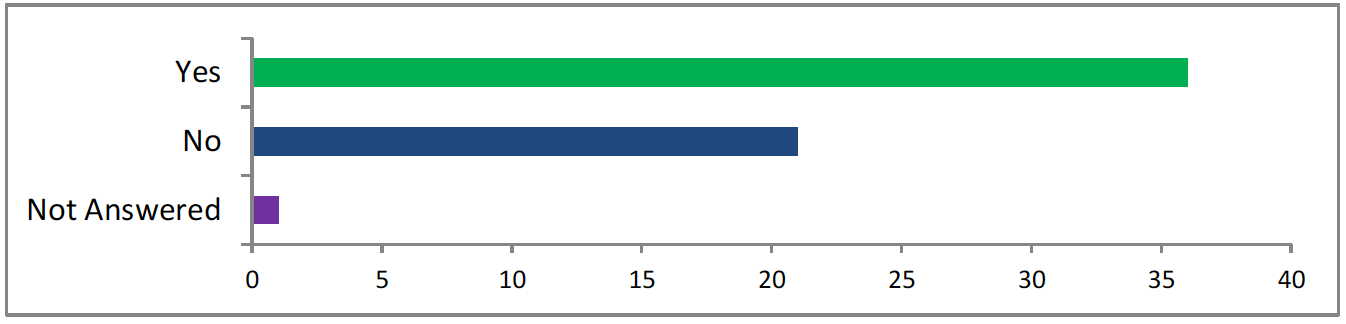
Question 3.3: Should administrative or organisational work connected to the operation of a practice be considered PMS activities for the purposes of ‘sufficient engagement’?
Overview
This question examines whether administrative and organisational tasks performed by GP contractors should be classified as part of Primary Medical Services (PMS) activities, which contribute to their “sufficient engagement” in a practice. It seeks to clarify the boundaries of administrative and organisational tasks considered eligible for PMS activities.
<34 answered yes, 23 answered no, 2 did not answer>
Q: If "yes", What types of administrative work should count?
Key Themes
- Administrative work scope
- Suggestions for inclusion range from patient-related administrative tasks (e.g., reviewing results, hospital letters, and referrals) to broader responsibilities such as clinical governance, quality improvement, staff management, and financial oversight.
- Some responses emphasise limiting administrative tasks to ensure GP contractors focus primarily on clinical work.
- The role of GP principals has expanded to include significant management responsibilities, particularly in practices without robust managerial support. This shift has led to increased administrative workloads, particularly in remote and rural areas where resource constraints are pronounced.
- Clinical and administrative engagement
- Many respondents argue for a balance, suggesting that administrative work should count as PMS activity but only to a certain extent (e.g., 20–50% of engagement time).
- Administrative burdens are often more pronounced in rural settings due to additional roles (e.g., emergency care, community involvement). These complexities necessitate recognising a broader scope of activities as PMS engagement.
- Some respondents warn against over-inclusion of administrative tasks, fearing it could dilute the clinical focus and potentially lead to misuse of “sufficient engagement” definitions.
Q: If "yes" What types of administrative work should not count?
Key Themes
- Clinical and non-clinical administrative work
- There is consensus that not all administrative tasks should qualify as PMS activities. The focus should remain on tasks that are patient-centric or essential to the operation of the practice.
- Tasks such as preparing private reports, managing private finances, or handling property issues unrelated to NHS care are frequently cited as activities that should not count.
- Delegable Tasks
- Work that can reasonably be handled by non-clinical staff, such as practice managers, is often considered ineligible. Examples include general financial management, HR duties, and logistical or business planning.
- Many respondents draw a distinction between administrative work with a direct clinical or operational impact (e.g., reviewing patient results) and work that is more peripheral, such as external meeting attendance or morale-boosting activities.
Conclusion
There is broad recognition of the importance of administrative and organisational work in supporting the effective operation of practices. However, most respondents advocate for a balanced approach: administrative tasks should count as PMS activities but within defined limits to ensure GPs maintain a strong clinical focus. Flexibility, particularly in rural and remote settings, is essential to address unique operational challenges. The evolving role of GP principals necessitates a nuanced framework that acknowledges both clinical and administrative contributions to sufficient engagement.
The consensus is that administrative work connected to direct patient care and essential practice operations should count as PMS activities. However, tasks that are private, non-NHS related, or delegable to non-clinical staff should be excluded. This approach balances the recognition of the administrative burden on GPs with the need to maintain focus on clinical responsibilities and operational efficiency.
Question 4: Are the exceptions to the requirement reasonable? Please give your views
Overview
The question explores whether the existing exceptions to the requirement for engagement in certain GP roles and responsibilities are justified, practical, and equitable. The responses reveal a range of perspectives on the flexibility of these exceptions, their potential for abuse, and their role in addressing current workforce challenges.

<50 said yes, 8 said no, 1 did not answer>
Key Themes
- Flexibility
- Some respondents believe the existing exceptions are reasonable and align with the needs of a flexible workforce. Although the need for flexibility in exceptional cases, such as maternity leave, illness, or unforeseen staffing shortages, to retain staff and address individual needs were highlighted.
- Several responses warn about the potential for abuse of exceptions, particularly by GPs avoiding patient-facing roles while maintaining multiple practice partnerships. There is a recurring suggestion for routine reporting and monitoring to ensure that exceptions are not misused and remain transparent.
- Workforce challenges
- Some respondents view the exceptions to address GP burnout and retention challenges but stress that these should not undermine the core clinical focus of the profession.
- Study leaves and posts that shift newly qualified GPs into non-clinical roles are criticised for detracting from patient care. Respondents argue that newly qualified GPs should prioritise clinical work to develop practical experience.
Conclusion
The exceptions to the requirement are generally seen as reasonable in principle, particularly for circumstances like maternity leave, illness, or temporary staffing crises. However, there is strong concern about their potential for misuse, particularly in allowing avoidance of clinical duties. Striking a balance between flexibility and accountability, with clear monitoring mechanisms, is essential to ensure that exceptions address genuine needs without undermining the core responsibilities of GPs.
Question 4.1: Are there any other circumstances where the 10-hour rule should not be applied?
Overview
This question examines whether additional exceptions should be considered for the 10-hour minimum engagement rule for GPs, exploring unique circumstances, workforce challenges, and the implications of strict adherence to this requirement.
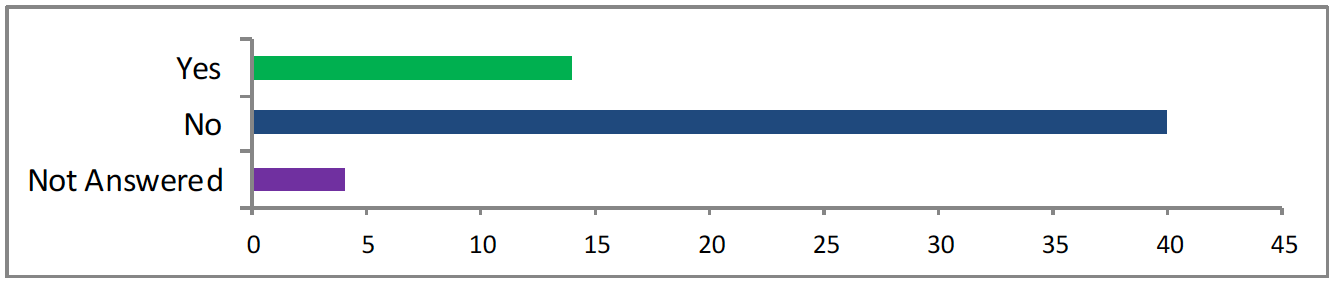
<14 said yes, 41 said no, 4 did not answer>
Key themes
- Flexibility for remote and rural practices
- Respondents frequently mention the unique challenges of remote and island practices, where GPs often work in rotational models or spend extended periods away from the practice for personal or professional reasons.
- Some responses emphasise innovative approaches to service delivery, such as rotational coverage by small groups of GPs in isolated practices, as requiring flexibility in the 10-hour rule.
- Historical practices, such as time spent away to reduce isolation or engage in non-NHS activities, are viewed as critical for sustainability in these areas.
- Life circumstances and workforce retention
- Personal circumstances, including phased retirement, caring responsibilities, illness, and maternity leave, are highlighted as situations where exceptions could help retain experienced GPs in the workforce.
- Support for part-time roles (e.g., 1 session clinical, 1 session administrative per week) is proposed as a solution for those facing temporary challenges.
- A significant number of respondents argue against reducing the 10-hour minimum, stressing that this already represents a low threshold and should not be further diluted except in extreme circumstances.
- The importance of establishing a formal appeals process to evaluate individual cases is noted to ensure fairness and prevent misuse of exceptions.
- Emergencies, practice collapse, or extreme recruitment difficulties are seen as valid but time-bound reasons for relaxing the rule.
Conclusion
While there is consensus on the need for flexibility in certain situations – especially for remote practices and personal life circumstances – many respondents caution against broadly relaxing the 10-hour rule. They stress the importance of maintaining clinical engagement as a core requirement while addressing exceptional needs through formalised processes. Clear guidelines and oversight mechanisms are essential to balance flexibility with accountability, ensuring the rule remains fit for purpose while supporting workforce sustainability.
Question 4.2: Of the current exceptions to the 10-hour rule, are there any which you think should be removed? Please give your views
Overview
This question seeks feedback on whether any existing exceptions to the 10-hour rule should be reconsidered or eliminated. The responses provide insights into the consensus and specific areas of concern about current exceptions.
Key themes
- Support for current exceptions
- Most respondents explicitly state "no" or similar affirmations, signalling widespread agreement that the current exceptions should remain unchanged.
- Some respondents advocate for expanding exceptions to enhance retention and career development across all stages of a GP’s career, highlighting the need for flexibility and support in the workforce. Although there were concerns about study leave exception, suggesting it could be misused or detract from clinical responsibilities.
- Suggestions are made for evaluating specific cases, such as short-term suspensions for single-handed GPs, to ensure fair application of exceptions.
Conclusion
The responses indicate broad support for the current exceptions to the 10-hour rule, with many respondents seeing no need for removal. However, a small subset raises concerns about the study leave exception, suggesting increased scrutiny or oversight to prevent misuse. There is also a minor push for expanding exceptions to better support retention and career development. Overall, the current policy appears well-aligned with the needs of the majority, but targeted adjustments and reviews may address the specific concerns raised.
Question 5: What would the impact of either tightening or loosening the requirement have on the sustainability of general medical services provision?
Overview
This question seeks insights into the consequences of stricter or relaxed regulations around the 10-hour rule and related requirements. Responses reflect a spectrum of potential impacts, ranging from benefits like improved accountability to risks such as workforce attrition and destabilization of general medical services (GMS), particularly in rural and remote areas.
Q: Impact of tightening
Key Themes
- Workforce and Retention
- Tightening requirements may discourage GPs with portfolio careers or other commitments, leading to workforce attrition.
- Experienced GPs nearing retirement might leave earlier, and part-time GPs could find compliance challenging.
- Large practices or multi-site setups may face operational challenges, such as employing more partners or restructuring their business models.
- Some practices might struggle to maintain contracts under stricter conditions, leading to more practices being managed by health boards.
- Rural and Remote Practices
- Respondents highlight the potential collapse of rural and island healthcare due to unique staffing challenges and reliance on flexible arrangements.
- Stricter rules could destabilise remote practices and reduce continuity of care in underserved areas.
- Patient Care and Accountability
- A more engaged and visible GP workforce could improve leadership, continuity of care, and decision-making aligned with local patient needs.
- While stricter requirements could enhance oversight and promote patient-centric practices, they risk creating an unattractive work environment for new and existing GPs.
- Some respondents view tightening as a way to address perceived abuses of the system, such as "absent landlord" practices. Strengthened partnerships might foster better governance and responsiveness.
Q: Impact of loosening
Key Themes
- Quality of Care
- Concerns about declining continuity of care, increased reliance on locums, and risks to patient safety due to less experienced staff handling complex cases.
- Risks of practices being taken over by absentee contractors or large commercial entities prioritizing profit over patient care, leading to reduced local accountability and standards.
- Workforce and Retention
- Potential impacts on GP retention, sessional commitments, and opportunities for more flexible or innovative working arrangements.
- Emergence of "mega practices" or corporate-led models, with possible benefits in efficiency but concerns over a loss of community focus and increased referrals to secondary care.
Conclusion
Tightening the 10-hour rule could have mixed impacts on GMS sustainability. While it may improve patient care, governance, and local accountability, it risks exacerbating workforce shortages, destabilizing rural and remote practices, and increasing health board-managed practices. Respondents underscore the need for a balanced approach that considers the unique challenges of rural settings, and the diverse roles GPs play within the healthcare system. Sensible, consultative adjustments could mitigate risks while fostering stability and improving patient outcomes.
Loosening the requirements for GMS provision has both potential benefits and significant risks. While it may promote flexibility, innovation, and retention, these advantages could come at the cost of reduced care quality, patient continuity, and community accountability. Careful consideration and safeguards are required to balance sustainability with maintaining high standards of patient care.
Question 5.1: If the requirement was changed, should GP contractors in existing contracts be required to meet the new requirement? Please give us your views
Overview
The question seeks opinions on whether GP contractors with existing contracts should be required to meet new, potentially tighter, contractual requirements if those requirements are changed.
<37 said yes, 21 said no, 1 did not answer>
Key themes
- Transition Period and Flexibility
- The need for a lead-in time to allow practices to adjust to new requirements is emphasised. Many responses call for a gradual transition period (e.g., 3-5 years) to accommodate existing contractors without destabilising practices.
- Opinions are divided on whether new requirements should apply uniformly to all contractors, with some advocating for equal treatment, while others suggest new contractors should adopt these requirements while existing ones are allowed flexibility.
- Legal and Practical Concerns
- There are concerns about retrospectively applying new requirements, which could lead to legal challenges and destabilization of existing practices. An appeal process involving LMC, Health Boards, and independent representatives is suggested to ensure fairness.
- Increasing requirements might lead to the hand back of contracts or reduced sustainability, particularly if GPs are forced to meet new, more stringent demands. Conversely, some believe that reducing the requirements could allow for a less demanding workload, though this could undermine the partnership model.
Conclusion
A gradual transition period is widely supported to prevent destabilisation, while ensuring accountability and alignment with the GP partnership model. However, the challenge lies in applying new requirements to existing contracts without causing unintended consequences such as contract hand backs or legal disputes.
Other questions
– What is your name? – There were 57 responses to this part of the question.
– If responding as a GP contractor, what is your practice ID? – There were 40 responses to this part of the question.
– Do you consent to Scottish Government contacting you again in relation to this survey? F uture contact/internal sharing – There were 58 responses to this part of the question.
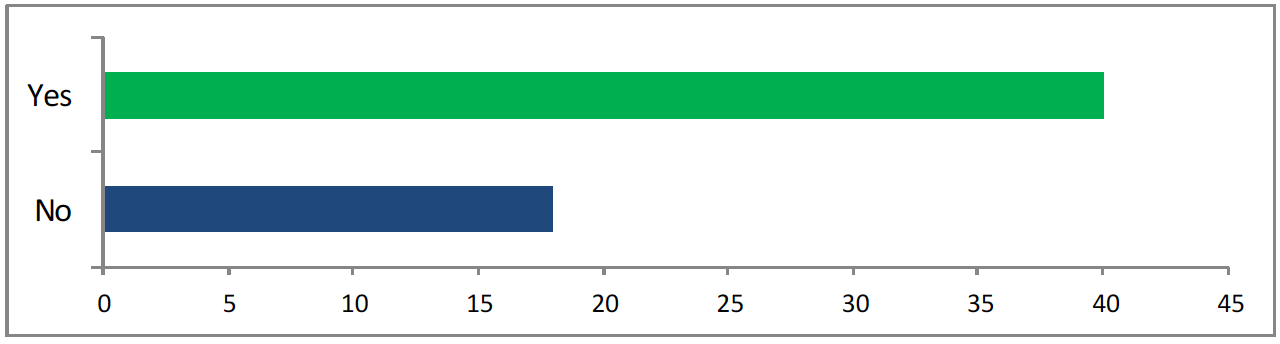
<41 said yes, 18 said no>
– What is your email address? – There were 58 responses to this part of the question.
– I confirm that I have read the privacy policy and consent to the data I provide being used as set out in the policy. – There were 58 responses to this part of the question.

<59 gave consent>
– Please help us improve our surveys by answering the questions below.
How satisfied were you with this survey? – There were 50 responses to this part of the question.
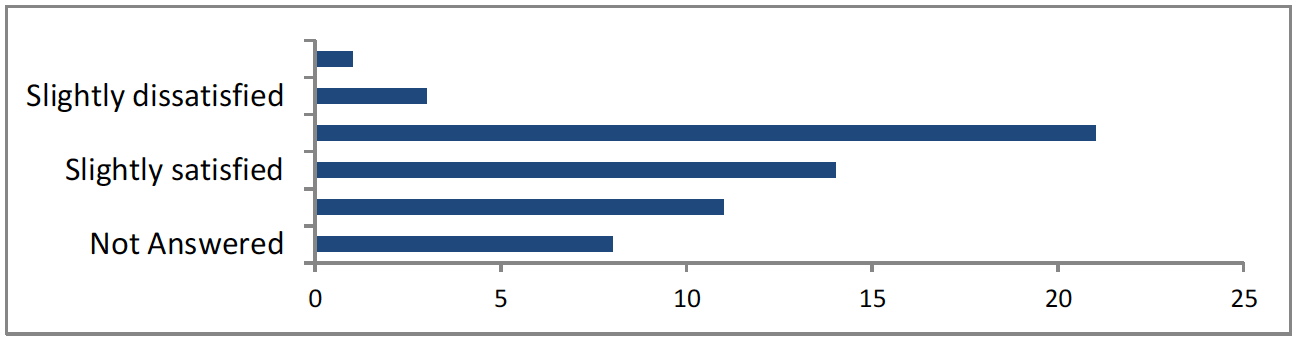
<1 very dissatisfied, 3 slightly dissatisfied, 21 neither satisfied nor dissatisfied, 14 slightly satisfied, 11 very satisfied, 9 not answered>
Please enter comments here.
There were 11 responses to this part of the question.
– How would you rate your satisfaction with using this platform (Citizen Space) to respond to this survey?
There were 49 responses to this part of the question.
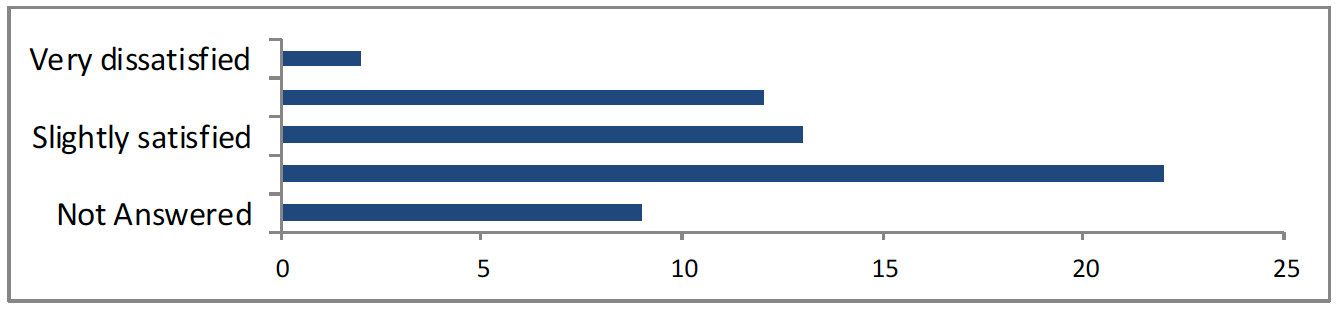
<2 very dissatisfied, 12 neither satisfied nor dissatisfied, 13 slightly satisfied, 22 very satisfied, 10 not answered>
Please enter comments here.
There were 4 responses to this part of the question.
Contact
Email: Esther.black@gov.scot