Chief Medical Officer - annual report: 2022
This annual report from the Chief Medical Officer (CMO) "Realistic medicine: a fair and sustainable future" is focused around five themes: collaborating for a healthier, fairer Scotland, personalising care through understanding, innovating for a more sustainable system, supporting our workforce and the health of our nation.
Collaborating for a Healthier, Fairer Scotland
Introduction
The social determinants which lead to inequalities in people’s experience of health are well understood and have been for some time. We know too that it will take leadership, joint ownership and collaboration with partners beyond our health and care system if we are to tackle the inequality that exists in our society. Without this co-ordinated and relentless approach I am concerned that the inequalities experienced by many may persist, deepen and affect many more.
The pandemic has shown us how precarious circumstances are for many of our communities facing the greatest hardships. But, it has also shown us how quickly and effectively we can mobilise to support those most in need.
Providing communities, leaders, funders and planners, across public services and beyond, with a deeper understanding of local needs, underpins the effectiveness of this response. It relies on mechanisms to capture data and evidence, routinely assess local needs and share learning to inform local and national decision making. This includes smarter use of public health data and intelligence, and linked data on outcomes. It must also include the knowledge and experience of people living and working within our communities.
Third sector, voluntary and wider community partners have an important role in shaping what we do. These voices, and the voices of those with lived experience of disadvantage, are crucial. We must ensure that local need can be identified and addressed through a shared vision and a strong ethos of collaboration and accountability. Ultimately, collaboration is key and cross-sector working will help to achieve an inclusive health and care system, and the fairer Scotland we all wish to see.
There are, however, some encouraging signs that we are heading in the right direction. We must continue to build on and learn from approaches that aim to address the social determinants of health and I want to highlight some examples that I would like to see become more widespread.
Scotland’s child poverty action plan
Almost one quarter of children in Scotland are living in poverty; an unacceptably high number, and one that requires a whole-nation effort to tackle. Experience of childhood poverty can negatively impact on the wellbeing of families and prevent children from realising their full potential.[2] The impacts of growing up in poverty can be wide reaching – including to education and health outcomes.
Child poverty affects educational attainment, future earning potential and is a key predictor of youth homelessness.[3] In our most deprived communities, people spend less time in good health than those living in our most affluent (more than 24 years lower for both males and females). People are 18 times more likely to have a drug-related death in our most deprived communities, and the suicide rate is three times higher than in our least deprived communities.[4] These facts are sombre, but not inevitable. Given what we know, we must make a relentless and collaborative effort to address the root causes of these inequalities.
Best Start, Bright Futures – tackling child poverty in Scotland
While a lot of the building blocks for tackling child poverty are already in place through initiatives like the Scottish Child Payment, Parental Employability Support Fund and embedded advice services, families living in poverty have reported that this is not enough. Initiatives are often said not to be working for them the way they need them to. A common theme is that services are not joined up when people need them most, creating financial and emotional barriers to accessing support.
These systemic problems should be addressed, and while there is no easy fix, continuing to operate in ways that don’t deliver change for people living in poverty is not an option.
90% of children in poverty come from one of six family types:[5]
- lone Parents;
- families with a disabled adult or child;
- minority ethnic families;
- larger families (three+ children);
- families with young mothers (under 25); and
- families with a baby under one.
Doing things differently, doing things better
In March 2022, The Scottish Government launched Best Start, Bright Futures, the second action plan intended to tackle child poverty. The fact that this is the second plan recognises that there is much more to be done to improve the lives of children living in poverty in Scotland. It outlines the key actions needed: increasing income from employment, reducing household costs and maximising families’ income.
The approach taken to develop the plan is particularly encouraging. Close collaboration between local and national government, healthcare and third sector organisations working alongside families with lived experience has led to a shared understanding of what is needed to tackle child poverty in Scotland.
It is not a plan for the Scottish Government but a plan for all of Scotland – recognising the contribution all parts of our society must make to deliver the change needed.
Best Start, Bright Futures sets a commitment to trial new multi-agency ways of working and engagement. Work is commencing in Glasgow and Dundee, two pathfinder areas to personalise support for everyone – delivered with kindness, dignity and respect.
Listening to and understanding what’s important to families, what they need, and when they need it, sits at the heart of this approach. By doing so the aim is to deliver support and services that families value, and deliver them in a way that reduces the difficulties people can face when they navigate a complex system.
Our role as healthcare professionals
Delivering personalised care is a key principle of Realistic Medicine and also sits at the core of Best Start, Bright Futures. Many families in, or at risk of, poverty, have regular contact with healthcare and with third sector organisations. Healthcare professionals are well placed to help tackle child poverty. By building on our contacts with families and using our trusted role within communities, we can ensure families are aware of the support they can access, which often sits beyond health. We must be able to signpost them easily to reliable, high-quality financial, emotional and practical support that meets their needs.
Best Start, Bright Futures aims to create a ‘no wrong door’ approach to support, with a particular focus on further embedding additional non-clinical and social support roles in General Practice, including benefit and welfare experts to support families who may not be in touch with other services.
Collaboration is key
This plan is an attempt to shift more focus to prevention and providing personalised support at the right time, for as long as people need it, to help break the cycle of crisis management and improve health inequalities in the long term in Scotland.
I am keen to promote the multi-agency, collaborative approach that has been taken here. It is evident that Best Start, Bright Futures has been developed around the needs of the people it aims to help and I commend everyone involved. It is precisely the kind of approach we need to help address health inequalities across all of the social determinants of health.
Anchor institutions
I welcome the work to position NHS and social care providers as ‘anchor institutions’ within our communities; working with others, such as housing associations, local government and universities, to nurture the conditions for health and wellbeing.
We can do this by amplifying opportunities in local communities through:
- increased access to employment in health and care; and,
- considering how communities can use NHS land and buildings to support their health and wellbeing.
We must work in partnership with the third and voluntary sectors to support people who need our help the most, helping build strong relationships that connect the building blocks of a healthy community.
Navigating towards a better life
Case Study 1: Overcoming adverse childhood experiences
Background The Navigators met “Craig” in the ED when he was brought in suffering from extreme anxiety. At the time he was in prison. Craig has been in the care system since the age of three because his mother was addicted to heroin and couldn’t look after him. His childhood was traumatic. On release from prison he reconnected with the Navigator Service.
Navigator Support The Navigators have been working with Craig since his release. Initially, he was living in homeless accommodation but now has his own home. The Navigators connected him with Fresh Start, a charity who provided all his white goods and essentials and they decorated his house. Craig has custody of his 5-year-old son; social work were involved on Craig’s prison release but they are no longer needed due to his progress. Although Craig still suffers from anxiety things are improving with the help of his GP. The Navigators also connected Craig to the “CALM” helpline for men, which he has used on a few occasions particularly during lockdown. The “Running on Empty” fund has helped Craig with food vouchers and phone credit and he now has a temporary job. The Navigators are in regular weekly contact and will support Craig for as long as he needs them.
We know that people who have adverse experiences in childhood have poorer health outcomes and this increased risk continues throughout life. There is also evidence that this experience may put people at greater risk of violence, both as victims and perpetrators. We must adopt a supportive approach, seeking to provide understanding, personalised care and agency for people experiencing the adverse effects of violence, to help break these destructive cycles.
The Navigator project provides support within nine Emergency Departments in Scotland. It’s run by the charity “Medics against Violence.”[6] The service works closely with local Alcohol and Drug Partnerships given these issues can often affect the same people. 23 highly skilled people make up the Navigators team, some with lived experience, some with a vast amount of professional experience and some with both.
Although primarily set up as a violence reduction programme, violence rarely comes alone as a concern, and the team are skilled in helping empower people to address a wide range of issues. Navigators provide psychosocial support to people who experience difficulties with drug and alcohol use, are affected by violence, or are in a heightened emotional state. Some clients are living in substandard housing, or are homeless. Others may be people who are victims or survivors of domestic abuse, sexual abuse or assault, and people who are affected by a loved one's drug and or alcohol use.
People they engage with may feel completely overwhelmed by their current situation or may feel let down by services in the past. There’s no “three strikes and you’re out” in the approach taken by this service, a critical aspect of their approach. Instead, the Navigators roll with any resistance and try to find any safe way possible to engage with people. Key to this is understanding that trusting another person or “worker” can be incredibly difficult for some.
People in crises may be managing their situation as best they can and the Emergency Department can seem the only safe place to go. Navigators work in a person-centred way. They provide a safe space and listen to help people explore the reason why they have been in hospital. Navigators actively seek out people who may need their support and use this window of opportunity – the “reachable moment” – to plant the seeds of change.
People are encouraged to identify anything that may be a barrier to them accessing support or making changes. Navigators walk alongside people who need their help, empowering and enabling them to overcome those barriers. They also draw on their own lived experience, to provide empathy and offer hope.
Dr Sara Robinson, consultant in Emergency Medicine at the Royal Infirmary of Edinburgh was pivotal in bringing Navigators to Scotland.
“The Emergency Department is a hectic and unpredictable workplace, which is why I love working here. Our clinical skills and problem-solving abilities are being used constantly as we move from patient to patient. But sometimes the problem isn’t medical and we can’t help. Sometimes the result is medical but the source of the problem is not. Our health is a complex interaction between our physical, mental and social wellbeing. To improve health we need to tackle more than just the clinical aspects of it.
That’s where having a team like Navigator really adds value to the work we do and the patients we treat. The team that make up Navigator are among the most empathic, proactive people I have ever met. They help and support people to make meaningful changes in their lives. To move away from violence, addiction or negative social circumstances. They don’t judge, they listen. They don’t pretend to be able to fix problems, instead they help our patients find solutions. The Navigator team allow staff and the people we care for to hope.
Patients and clinical staff can’t fail to be inspired by the Navigators ‘can do’ attitude. Our Navigators challenge us all to be the best version of ourselves, and they support us to get there.”
Here are some views from people who have accessed the Navigator service:
A different service
“The thing is about Navigator is they come to you. ‘Cause a lot of people that need support don’t actually seek it out. They just kinda let it lie and then things get worse. Whereas Navigator, they kinda – not in a pressuring way – but they don’t really let you off.”
Connection with Navigator
“I felt like I was talking to a person, you know, not a professional, which was nice."
Empowerment
“The Navigators have definitely gave me that boost sorta reassurin’ us that I can totally change. They showed me that, it’s like I can dae it, eh? And that it’s possible to dae.”
Case Study 2: Being believed was the key to escaping abuse
Background In 2018 the Navigators met Gina when she attended the Emergency Department with her children, one of whom had been injured. She disclosed to the Navigators that the child’s father had caused the injury intentionally and that this was part of a pattern of ongoing abuse against Gina and her children by her husband who was a healthcare professional. Gina had never spoken to anyone about it before as she didn’t think anyone would believe her as to everyone around her, she seemed to have a lovely life.
Navigator Support Gina chose to report to the police and was supported to do this by the Navigators, who she asked to remain with her when she gave her statement. The Navigators left their contact details but didn’t hear from Gina again until recently.
Gina’s lawyer who is dealing with the legal side of this case put her back in touch with Navigator as she was keen to reconnect with them to investigate possible support for her children who had witnessed and experienced a lot of abuse. Gina is back at work and is receiving regular counselling. She remembered the impact of being believed on that night in the ED and said it gave her the strength to make a statement to the police thus ending her abuse. It is also without question that speaking to someone who had been in the same position as her also made a huge impact, demonstrating the value of the Navigators’ lived experience.
Importantly, the Navigator service also looks after their Navigators. It actively supports their workforce’s wellbeing and encourages them to develop and acquire new skills. Key to this is regular supervision and counselling, because this work is hard and can be challenging.
This is a fantastic example of collaboration that is actively seeking to improve the wellbeing of some of the most vulnerable people in our society. The way in which the Navigators take the time to listen – to find out what is going on in people’s lives – and ensure they can access the care and support they need and value, is an approach we can learn from across our health and care system.
I’m personally grateful to the people who have been willing to share their experiences of the Navigator approach in this report.
Naloxone: improving services for people who use drugs
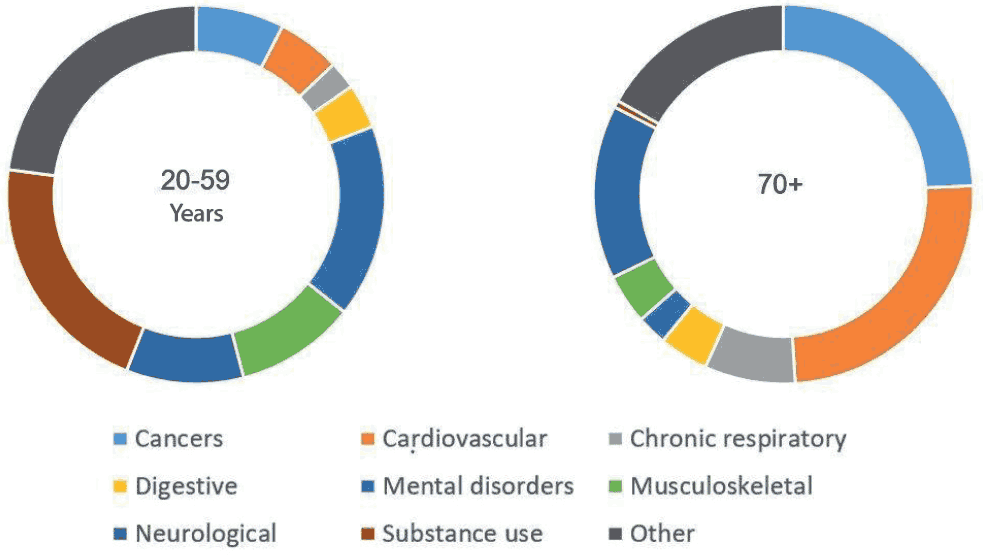
People who access care in crisis are often struggling with multiple issues beside health. Addiction is often involved. Substance use costs more healthy years in 20-59 year olds than any other single pathology.
Drug deaths leave a devastating impact on individuals, families and the wider community. They remain unacceptably high in Scotland. I want to draw attention to the work being done on take-home naloxone. Since 2015, Scotland has been working to distribute naloxone kits; this demonstrates the progressive collaboration we need to see to provide access to those most at risk.
The benefits of Naloxone
In 2020, 1,339 people died as a result of a drug-related death.[8] A further 1,190 died due to causes related to alcohol.[9] Alcohol and drug-related deaths occur more frequently in communities affected by socio-economic hardship. These deaths are preventable causes of premature mortality. The numbers of people dying prematurely has been increasing in recent years, further contributing to a widening of the gap in life expectancy between our most well-off and least well-off communities.
Preventing drug and alcohol-related harms and reducing inequalities that occur as a result of substance use require all those involved to embrace the principles of Realistic Medicine.
It requires an approach to people that empowers them to be equal partners in their care and encourages them to articulate what is important to them. Many people who experience drug and alcohol dependency have also experienced trauma and adverse experiences in childhood.
Building trust and working through trusted relationships is a key means by which people are supported from the moment of crisis to achieve their own recovery goals. At a time of crisis and high risk drug use, people may have multiple and complex needs and a limited support mechanism to draw on.
Naloxone is a lifesaving emergency treatment that can reverse the effects of an opiate overdose. Scotland was the first country in the world[10] to introduce a national naloxone programme, empowering individuals, families, friends and communities to reverse an opiate overdose.
When someone receives a naloxone kit, they also take part in a wider conversation about the risks they experience, ways to keep safe and other supports they may need. Naloxone kits can be given out by trained peer workers, homeless outreach teams and the Ambulance Service. This diversity of skills and experiences is crucial in establishing meaningful connections with people and increasing the effectiveness of the programme approach.
The principles of Realistic Medicine also inform and highlight the importance of a Recovery-Orientated System of Care (ROSC) for people at risk of drug and alcohol harm. A ROSC is a co-ordinated network of community based person-centred services and supports working to build on the strengths of individuals, families and communities. A ROSC acknowledges the role that family members, care givers, significant others, friends and the community can play in a person’s recovery.
Understanding, supporting and promoting this approach is particularly apposite in the light of the impact of COVID-19. At a time when many statutory and third sector frontline services were extremely limited in terms of their ability to deliver harm reduction and recovery support, Recovery Communities across Scotland quickly responded and moved online, providing a diverse and innovative range of activities and assistance to people in active addiction and those on their recovery journeys. Individuals were provided with the required equipment, data services and training to access online tools. For a traditionally digitally excluded community, this represented a major step change and a foundation to build on as we move out of the pandemic.
The Ambulance Service experience
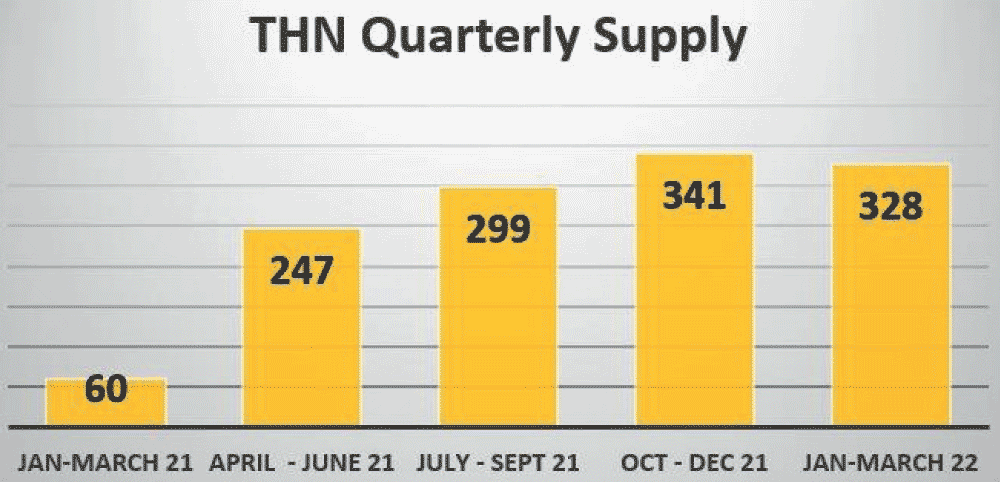
The Scottish Ambulance Service (SAS) has created a network of specialised clinical leads to engage with staff on Take-Home Naloxone (THN), aiming to provide the training required to allow clinicians to supply THN. As well as training paramedics and technicians, community first responders have also been included, taking care to the patient as quickly as possible. The supply of THN is expected to be standard practice in the ambulance service by January 2023.
SAS staff have received education and development related to drug harm reduction and the supply of THN across Scotland. As of 31 March 2022, 1,275 THN kits have been supplied.[11]
THN has not only been given to people at risk (34% of kits), but to their friends and family (40% of kits), with the remaining kits distributed to services supporting those at risk.
78% of people requesting another kit said the previous one had been used to reverse an overdose.
Alongside staff training, a public information campaign has been running since December 2021. This has encouraged the public to engage with THN supply.
Health board/Alcohol and Drug Partnerships and data sharing
The Scottish Ambulance Clinical Effectiveness Leads (CEL) have forged strong links with all territorial NHS boards and Alcohol and Drug Partnerships (ADPs) across the country.
From July to December last year, 4,330 incidents were reported to NHS boards via the Scottish Ambulance Service Non Fatal Overdose Pathway.
Early feedback indicates that around 40% of people reported were not known to services, or receiving any support for addiction.
The CELs have collaborated with drug treatment and support services to look at the potential for connecting people with support services when the 999 call is made, ensuring more timely and equitable access to support regardless of where people live. SAS are also working together with Police Scotland and Scottish Fire & Rescue service to replicate the Non Fatal Overdose Pathway across all of Scotland’s emergency services. I would like to hear from other professions about their experiences and the lessons learned.
In the future, in order that we address these complex challenges, it is important that we ensure that we involve and activate all of our assets, practising Realistic Medicine and continuing to personalise care and share decision making. We must harness the strengths and resilience in our communities who are well placed and well informed to help tackle preventable deaths and to radically reduce drug and alcohol harm.
Conclusion
We must remove barriers to good health where these exist but I remain optimistic that we can overcome the challenges, if everyone has a fair chance to thrive. The time for co-ordinated and relentless action is, however, never more urgent.
Multi-agency collaboration is required to tackle health inequalities, enable system change and deliver a healthier Scotland.
In this chapter I have shared some excellent examples of collaboration at a strategic, population and service level. We need to promote and learn from each of them, and work in partnership across our system and beyond our traditional way of doing things.
We should be prepared that any progress to tackle our entrenched health inequalities will be incremental. There’s no easy blueprint for success, and it will take genuine determination to collaborate, moving away from an organisation-focused approach, to thinking about what we can achieve together across systems.
Considerations
- How can you ensure that the people you care for never experience opening a “wrong door” while centring services around their needs?
- How can we personalise the care we provide and ensure we deliver better value care for the people who need our help the most?
- How can you collaborate with partners beyond health to help tackle the inequalities affecting the people you care for?
Contact
Email: RealisticMedicine@gov.scot