Healthy weight - local health systems support for pregnant women and young children: research
Research findings about how effectively local health systems seek to support pregnant women and children up to Primary 1 to have a healthy weight.
1. Introduction and methods
Policy background
In 2019, two-thirds (66%) of adults in Scotland were living with overweight, including 29% who were living with obesity[3]. These levels of obesity and overweight are problematic, both for the health of individuals affected and for the Scottish economy as a whole. Health risks from living with overweight or obesity include, among others, type 2 diabetes, certain cancers and cardiovascular disease. Treating such conditions places significant strain on the NHS (the annual cost has previously been estimated to range from £363 million to £600 million) and the annual cost to the Scottish economy (e.g. from lost productivity) has previously been estimated to be between £0.9 billion and £4.6 billion[4].
Living with overweight or obesity also carries risks during pregnancy. As well as immediate risks to the mother and unborn baby[5], there is an increased risk of the child going on to have an unhealthy weight[6].
Indeed, the proportion of children already at risk of overweight/obesity by Primary 1 (23% in 2019/20[7]) is a particular concern. As well as the known risks to their physical health, there is increasing evidence to suggest that children who are at risk of overweight/obesity are more likely to experience mental health concerns, bullying[8]and stigmatisation[9],[10]. Furthermore, they are more likely to experience obesity and related conditions as adults[11].
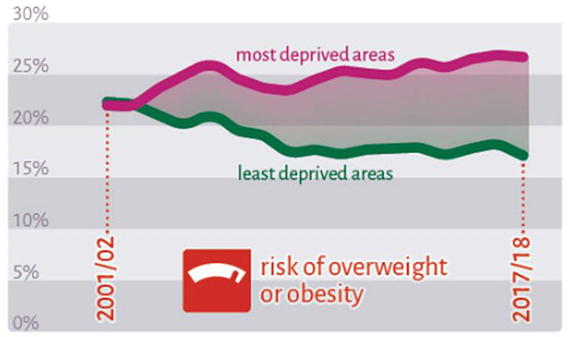
Despite significant efforts to reduce childhood obesity, these rates have remained stable in Scotland since 2001/2. What has changed is the distribution of overweight and obesity (Figure 1.1). In 2001/2, rates were virtually the same in the most and least deprived areas. However, the 2019/20[12] data shows that substantial inequalities now exist, with 27% of Primary 1 children in the most deprived areas at risk of overweight/obesity compared with 17% in the least deprived areas (and for obesity specifically, 13% in the most deprived areas compared with 6% in the least). Inequalities in the Scottish diet were also highlighted in the 2018 update of the Food Standards Scotland Situation Report[13]; those in the most deprived areas were consuming less healthy foods and cost was reported as a barrier.
Reducing overweight and obesity
Commitments relating to healthy weight in children are embedded in several key Scottish Government policies and frameworks including: The Public Health Priorities[15], Improving Maternal and Infant Nutrition Framework[16] and the Scottish National Performance Framework[17]. Getting it Right for Every Child (GIRFEC)[18], which recognises that every child has the right to expect appropriate support to allow them to reach their potential, also underpins the Scottish Government's overall approach.
Wider prevention work being undertaken in Scotland also includes the adoption of a whole systems approach to diet, healthy weight and physical activity[19] and the consideration of restrictions on promotion of foods high in fat, sugar or salt, which have been put on hold due to the COVID-19 pandemic[20],[21].
The detail of the Scottish Government strategy for reducing overweight and obesity is contained in A Healthier Future: Scotland's Diet and Healthy Weight Delivery Plan (2018)[22], which replaced Preventing Overweight and Obesity in Scotland: a route map towards healthy weight (2010)[23].
The Delivery Plan recognises the need to address issues related to weight at an early age and, as such, has a focus on prevention at its core. It sets out an ambitious aim of halving the number of children at risk of overweight/obesity by 2030 as well as significantly reducing health inequalities. It also recognises that interventions that require behavioural change at the individual level are less likely to be effective, particularly at reducing inequalities, than population-wide interventions to change the environment. The document contains more than 60 actions that are shaped around the following five key outcomes:
- children have the best start in life, they eat well and have a healthy weight
- the food environment supports healthier choices
- people have access to effective weight management services
- leaders across all sectors promote healthy weight and diet
- diet-related health inequalities are reduced
Acknowledging the influence of physical activity in healthy weight, A More Active Scotland: Scotland's Physical Activity Delivery Plan[24] provides further actions specifically related to this component of healthy weight.
Addressing inequalities
There are already several measures in place across a range of settings explicitly aimed at tackling inequality in the early years and improving health outcomes (including healthy weight) for young children and their parents. These include:
- Scotland's Baby Box
- Free vitamins for all pregnant and breastfeeding women and children up to 12 months in Scotland
- Best Start Foods smart card
- Best Start Maternity Grant
- The expansion of the Family Nurse Partnership (FNP)
- The transformation of both maternity care (through the Best Start five year plan[25]) and Health Visiting (through the Universal Health Visiting Pathway (UHVP)[26])
- The expansion of free Early Learning and Childcare, from 600 hours (in place since August 2014) to 1,140 hours a year for all 3 and 4 year-olds and eligible 2 year-olds.
Local health systems
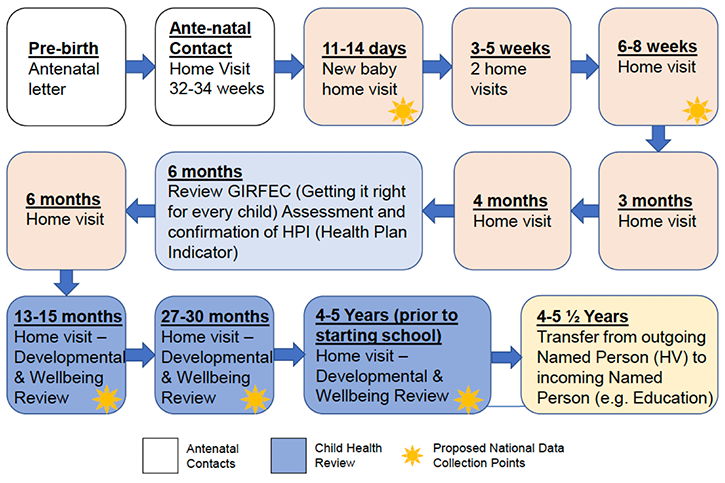
The current study is focused on the local health systems in place from pre-birth to Primary 1. Maternity services and the UHVP form the backbone of the contact between families and health systems in the preschool period and there are numerous contact points between the identification of pregnancy and the Primary 1 Health Review. In the case of identifying children with a high BMI, these contact points offer opportunities for health professionals to play a role in the prevention of child overweight and obesity – by offering support and information on healthy eating and physical activity from an early stage – and in identifying and referring children who are at risk. Figure 1.2 shows the UHVP contact points.
All health boards also have child healthy weight[27] programmes which comprise both preventative and treatment services. Although the Scottish Government had previously issued guidance on these programmes, it was recognised that variation in their design and content existed. As one way of addressing some of these inconsistencies, the Diet and Healthy Weight Delivery Plan[28] included an action around the development of standards for weight management services for children and young people.
NHS Health Scotland (now Public Health Scotland (PHS)) undertook a mapping of weight management services across Scotland. The findings supported the need for greater consistency in service provision. Using the best available evidence and through convening relevant professionals, NHS Health Scotland developed a set of standards for tier 2 and tier 3 (treatment) aspects of child healthy weight services and interventions[29].
This tiered approach (summarised in Figure 1.3), which is broadly consistent with The UK Obesity Care Pathway[30], is intended to "ensure a consistent, equitable and evidence-based approach to the treatment of overweight and obesity for children and young people up to the age of 18 years across weight management services in Scotland".
Figure 1.3: summary of standards tiered approach
Tier 1: Universal prevention
Prevention and reinforcement of healthy eating and physical activity behaviour messages. This includes school/nursery and (non-clinical) community-based interventions.
Tier 2: Targeted lifestyle weight management interventions
Overweight and obesity weight management interventions for children/young people greater or equal to the 91st centile. Family-based, multicomponent approach, delivered as one-to-one or group sessions, by appropriately trained child healthy weight specialists from a range of professional backgrounds.
Tier 3: Specialist services
Management of more complex cases (e.g. higher degrees of obesity and obesity with associated comorbidities, psychosocial difficulties, special needs). These may require a variety of interventions to be delivered in specialist multidisciplinary teams composed of highly trained dietitians with direct clinical psychology support and agreed pathways to paediatric endocrinology and physiotherapy.
Research aims and objectives
The overarching aim of the research was to enhance the Scottish Government's understanding of how effectively local health systems seek to support pregnant women[31] and children up to Primary 1 to eat well and have a healthy weight.
The overall objectives of the project were to:
- Describe the local points of contact within health systems that seek to identify weight issues and support healthy weight.
- Understand how the risk of overweight and obesity is identified and acted on throughout the different opportunities for contact in the formal health pathways.
- Understand current culture and practice in engaging with, supporting and empowering pregnant women, parents and carers to eat well and have a healthy weight and encourage their children to do the same.
- Understand how consistent and coherent local health systems are and if there is continuity of care/messaging across the different contact points.
In addressing these, the research sought to answer the following research questions:
- How local health systems seek to support healthy weight in the early years.
- The extent to which these local systems align with national standards/guidance.
- What actually happens in practice – and the extent to which there is consistency and coherence within local systems.
- What the barriers and challenges are to effective implementation of local systems.
- What supports effective implementation of local systems.
- How pregnant women and parents engage with/react to the local systems.
- What are the opportunities for improvement?
Scope of the research
There are numerous factors, across the whole system, that contribute to child healthy weight. This piece of research did not attempt to explore practice across the whole system but is focused specifically on the local health systems in place and, rather than attempting to cover the full childhood period, it is focused on pre-birth to Primary 1 (the period considered by the World Health Organisation (WHO) to be most critical for obesity prevention[32]).
Methodology
The research was qualitative in nature (in-depth interviews) and was undertaken by Ipsos MORI between March 2020 and September 2021, while the COVID-19 pandemic was ongoing. It comprised two main stages:
- Stage 1: overview of the local health systems in place within health boards across Scotland
- Stage 2: case study research with five selected health boards to gather more in depth information, from a wider range of professionals involved in maternal and child healthy weight systems.
Stage 1 sample
Letters were sent jointly by the Scottish Government and Ipsos MORI to Directors of Nursing and Directors of Public Health in all health boards asking them to identify an appropriate individual (or individuals) who would be best placed to describe their local systems in place to support healthy weight from pregnancy to the early years.
Thirteen of the fourteen health boards participated in this stage, with a total of 17 interviews undertaken. In nine health boards, one individual was interviewed, while in four health boards, two were interviewed (typically one covered the early years and one covered maternity services). Participants' roles included child weight management lead, nutrition/infant feeding lead/coordinator and dietician.
Stage 2 sample
Following initial analysis of Stage 1 findings, five case study health boards were selected[33]. Selection was designed to ensure a spread of health boards in terms of a number of factors including: geographical location; urbanity/rurality; size of board; and current child healthy weight provision.
In selected case study boards, the individual who had participated in Stage 1 was re-contacted by Ipsos MORI and asked to assist in the recruitment of Stage 2 participants within their board by forwarding an invitation from Ipsos MORI.
A total of 41 participants took part in Stage 2 and the sample profile is shown in Table 1.1.
Table 1.1: Stage 2 sample profile
Job title: Number interviewed
- Midwife manager: 2
- Midwife: 7
- Health visitor manager: 6
- Health visitor: 10
- Family Nurse Practitioner supervisor: 1
- Family Nurse Practitioner: 1
- School nurse: 6
- Public health/dietetics professional: 8
- Total: 41
Interviews
Interviews were undertaken by telephone or Microsoft Teams and each lasted around an hour[34]. Stage 1 interviews were conducted between September 2020 and February 2021. Due to recruitment difficulties, a small number were undertaken after work on Stage 2 had begun. Stage 2 fieldwork ran from December 2020 to August 2021. The fieldwork period was longer than intended due to the additional burden placed on health boards by the COVID-19 pandemic.
All interviews were conducted by members of the Ipsos MORI Scotland project team, using flexible discussion guides (Appendix 1) to ensure that key issues were covered with each participant.
Analysis
Qualitative interviews were summarised into thematic matrices[35] developed by the research team and drawing on the research questions. These thematic matrices were then reviewed to identify the full range of views and experiences on each issue.
Challenges and limitations
All research is subject to challenges and limitations. The following were encountered as part of the current study, and should be borne in mind when interpreting the findings.
First, it should be noted that the current study was not designed to be a service audit or service mapping exercise. The information gathered about the services delivered or planned within a given health board was very much dependent on the role and knowledge of the individual/s interviewed for that board. Indeed, it was often the case that the individual we interviewed during Stage 1 was very knowledgeable about their board's systems for either pregnancy or the early years/Primary 1 rather than both. Therefore, while the data gathered provides a sound overview of current provision and practice, it cannot be guaranteed that full details of all programmes in all boards will have been gathered. For example, at various points in the report, examples are given of programmes or practices that happened in one health board. It may have been that similar programmes operated in other boards but, particularly when boards were not case studies, this did not emerge – either because the individuals being interviewed were unaware or because they simply omitted to mention it.
The additional burden placed on health boards as a result of the COVID-19 pandemic resulted in delays to the project – during points at which the pandemic restrictions were at their highest, and boards were under greatest pressure, it was not considered appropriate to ask healthcare professionals to give up their time to participate in this research. This meant that a substantial amount of time had passed between the Stage 1 interviews being conducted (Sept-Dec 2020) and the publication of this report. It may then be that some of the information presented in this report is already out of date, although, in saying that, professionals recognised that reducing overweight and obesity in the early years was a long-term task. The COVID-19 pandemic had also led to a number of delays in planned roll outs of new programmes and, in some boards, planning work was also put on hold due to staff being redeployed in other roles. This meant that there was greater uncertainty, particularly around timescales for improvement work.
The case study fieldwork, like all qualitative research, was not intended to provide an indication of the prevalence of issues but rather to capture as much breadth and depth of opinion and experience as possible. As such, qualitative samples are not designed to be statistically representative, but rather to ensure a range of different people and perspectives are included. The way in which recruitment was necessarily undertaken, however, may also have resulted in some bias, which should be acknowledged.
As described above, Stage 2 participants were recruited via those who had participated in Stage 1 (the researchers had no means of contacting them directly). As the research team had no control over the selection of participants, it is not unfeasible that those who agreed to participate had a greater interest in child healthy weight issues than their colleagues.
There were particular difficulties recruiting midwives for the research. We had intended to conduct roughly equal numbers of interviews with midwives and health visitors. However, as Table 1.1 shows, nine midwives/midwife managers were recruited compared to 16 health visitors/health visitor managers. While it is not clear why midwives were less likely to volunteer for the research, there was some suggestion that they did not see the direct relevance to them, given the project was labelled primarily as being about healthy weight in the early years. The small numbers of midwives participating in the research has led to some gaps in the data relating to support provided by midwives.
Finally, where the report discusses how pregnant women and parents experience the system, this is health professionals' perspectives, rather than their own views and experiences.
Report structure and conventions
The remainder of this report is structured as follows:
- Chapter 2 focuses on the prevention work undertaken by boards.
- Chapter 3 explores the identification and referral processes.
- Chapter 4 describes the interventions available to those identified as having a high BMI.
- Chapter 5 examines levels of consistency and coherence across child healthy weight systems.
- Chapter 6 draws together findings from other chapters to identify the key factors influencing child healthy weight provision.
- Chapter 7 provides the main findings and implications of the study.
As already discussed, the majority of findings are based on qualitative interviews, which aim to establish the range of views and experiences rather than their prevalence. As such, as far as possible the report avoids the use of quantifying language (including terms like 'most' or 'a few').
When referring to those working in non-clinical roles, the term 'public health professional' is used.
Contact
Email: socialresearch@gov.scot