FIT testing for patients with colorectal symptoms: secondary care guidance
Secondary care clinical guidance on the use of faecal immunochemical testing (FIT) for faecal haemoglobin (µgHb/g) in addition to clinical acumen so that investigation of patients with colorectal symptoms can be targeted to those with the highest risk of colorectal.
Quantitative Faecal Immunochemical Test (qFIT) for Patients with Colorectal Symptoms
Guidance for Secondary Care
January 2022
This document is designed to provide guidance on the use of a quantitative faecal immunochemical test (FIT) for faecal haemoglobin (f-Hb) as an adjunct to clinical acumen so that referral and investigation of patients with colorectal symptoms can be targeted to those with the highest risk of significant colorectal pathology.
Individual symptoms are poor predictors of colorectal cancer1,2. The predictive value of colorectal symptoms can be improved using FIT3,4,5. Twenty-two percent(19-28%) of Scottish patients with colorectal symptoms, will have a f-Hb 10gHb/g faeces3,4,5,6. Up to 95% (84-95%) of patients referred who are then diagnosed with colorectal cancer will have a f-Hb 10g Hb/g faeces4,5,7,8. Referral and management triage applying qFIT in symptomatic patients, shortens time to diagnosis, is cost effective and there is emerging data that its application may result in a migration to an earlier cancer stage at diagnosis3,9. qFIT will also prevent harm through the avoidance of investigations in patients who are not likely to have significant pathology.
With the return to pre-Pandemic endoscopy activity, most Boards will have endoscopy capacity to ensure that patients with colorectal symptoms AND a f-Hb 10gHb/g faeces are investigated in a timely manner, along with competing demands such as bowel screening. If a FIT is requested for asymptomatic, vague, acute or non-colorectal symptoms, 12% will still have a f-Hb 10gHb/g faeces, but the costs and endoscopy demand will not be sustainable, patients will continue to wait for their investigations and the diagnostic yield will be low10. There are alternative referral pathways and bowel cancer screening (if eligible) for these patients.
As an adjunct to clinical acumen, primary care clinicians are strongly encouraged
- To provide a qFIT result (where it is available in primary care) at the time of referral, except for patients with a rectal or abdominal mass, or where there is a reason that prevents completion of the FIT. Primary care clinicians have been asked to make the reason for the incomplete FIT clear in the referral.
- To provide a blood Hb and where it is indicated a serum ferritin and iron studiesa to complete the investigations for iron deficiency anaemia.
- To request a second qFIT where the patient has severe persistent symptoms AND a f-Hb < 10gHb/g faeces if referral is considered.
- To only refer patients who have
- a f-Hb 10gHb/g faeces,
- a rectal mass,
- an abdominal mass,
- iron deficiency anaemia,
- a family history of colorectal cancer that requires screening outwith the bowel screening programme11,
- colorectal symptoms and a patient who is unable to complete a qFIT,
- severe persistent symptoms where there is a significant clinical concern of significant pathology despite two f-Hb < 10gHb/g faeces,
- severe persistent symptoms requiring symptom management.
These recommendations are to align with the current colorectal referral guidelines for Urgent Suspicion of Cancer (USoC) as provided below12.
- - A persistent (>4week) change in bowel habit, especially to looser stool, not simple constipation
- - Repeated rectal bleeding without an obvious anal cause
- - Any blood mixed with the stool
- - Abdominal pain associated with weight loss
- - Iron deficiency anaemia (symptomatic or asymptomatic)
As an adjunct to clinical acumen, Secondary Care clinicians are strongly encouraged to review the referral symptoms with the qFIT result. Table 2 proposes a referral triage for review and investigation. The following is recommended
- Priority access to investigation should be provided for patients who have a f-Hb 400gHb/g faeces, an abdominal or a rectal mass.
- Where resources allow, priority access may be appropriate for those patients with both iron deficiency anaemia and a f-Hb 10-399 gHb/g faeces. The data is currently under review. Iron deficiency anaemia is a low Hb, defined by the local laboratory criteria AND either a ferritin < 30g/LOR a ferritin 30-100g/LAND a low serum iron with a transferrin > 3g/L..
- In the absence of an abdominal or rectal mass, Secondary Care clinicians are strongly encouraged not to triage patients direct to investigation where the f-Hb < 10gHb/g faeces.
- Patients referred with a f-Hb < 10gHb/g faeces, excluding those with a rectal or abdominal mass, may be triaged to Urgent or Routine clinic appointments while clinical resources remain challenged. Please be mindful that in the presence of a f-Hb < 10gHb/g faeces, the USoC upper gastrointestinal investigation requirements for iron deficiency anaemia may persist. (see National Iron Deficiency Anaemia Pathway).
- To help support patients from backgrounds, who are less likely to complete a qFIT, Secondary Care consider carefully the triage of those patients who do not return a qFIT to Primary or Secondary Care. Primary Care clinicians have been encouraged to advise, in the referral, if there is an expectation that the qFIT will not be completed for socioeconomic, ethnic or other reasons.
- Discharge of patients who have not completed a qFIT, without a clinical review, is NOT acceptable where
- the Primary Care clinician has advised that the patient has an incapacity preventing qFIT completion, declined FIT for legitimate reasons or unlikely to complete the qFIT for socioeconomic reasons as provided in the referral OR
- the Primary Care clinician has referred the patient requesting symptom management
- the Primary Care clinician has referred the patient with persistent severe symptoms and has raised a clinical concern of significant colorectal pathology in the referral.
- For all other patients, except those with an abdominal or rectal mass, it would be appropriate for secondary care to send a further qFIT or reminder to complete where a qFIT has not been completed. A pause of the waiting times measure is legitimate while the result is pending.
- Where resources allow and a patient is referred with persistent symptoms and only one qFIT completed with a f-Hb < 10gHb/g faeces, that a second qFIT be considered. There is growing evidence that requesting a second qFIT, in patients where the first f-Hb was < 10gHb/g faeces, increases the qFIT sensitivity from 84 to 97%13. It will however, also increase colonoscopy demand by up to 9.7% unless applied only in patients with persistent symptoms13.
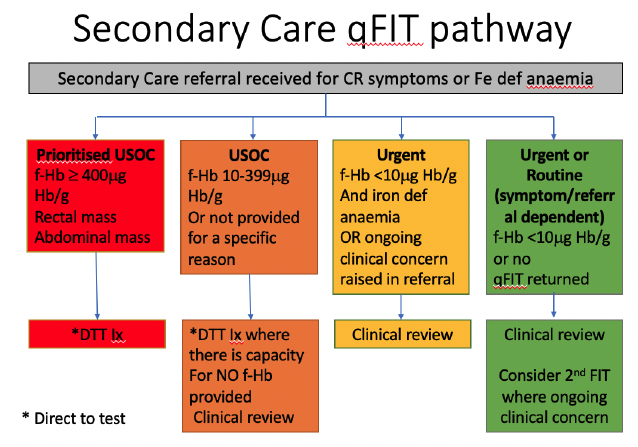
Secondary Care Referral Triage Categories will vary dependent on local resources however the following recommendations are designed to support the application of the qFIT guidance provided to primary care (see Primary Care Guidance).
Prioritised Urgent Suspicion of Cancer access should be given to patients with an abdominal or rectal mass or a qFIT ≥ 400 gHb/g faeces. Where there is capacity, direct to test triage should be considered.
Urgent Suspicion of Cancer access should be given to patients with a qFIT ≥ 10 and < 400 gHb/g faeces or for those patients who are not able to provide a qFIT sample for specific reasons as provided in the referral. Where there is capacity, direct to test triage should be considered for those with a qFIT result and clinical review for those without a qFIT result.
Urgent access should be given to patients with a qFIT < 10gHb/g faeces and iron deficiency anaemia or a primary care referral advising ongoing concerns of colorectal cancer. Clinical assessment of both groups of patients in the first instance is advised.
Routine access is recommended for all remaining patients. Direct to test triage of these patients is strongly discouraged. A second qFIT is advised if there are ongoing clinical concerns.
References:
1.Ford AC, Veldhuyzen van Zanten SJ, Rodgers CC, et al. Diagnostic utility of alarm features for colorectal cancer: systematic review and metanalysis. Gut 2008;57:1545-53.
2.Vulliamy P, McCluney S, Raouf S, et al. Trends in urgent referrals for suspected cancer: an increase in quantity, but not in quality. Ann R Coll Surg Engl 2016;98:564-567.
3.Pin-Vieto N, Tejido-Sandova C, de Vicente-Bielza. Faecal immunochemical tests safely enhance rational use of resource during the assessment of suspected symptomatic colorectal cancer in primary care: systemic review and metanalysis. GUT 2021;2022;71:950-960.
4.Mowat C, Strachan JA, McCann RK et al. Faecal haemoglobin concentration thresholds for reassurance and urgent investigation for colorectal cancer based on a faecal immunochemical test in symptomatic patients in primary care. Ann Clin Biochem 2021;5(3):211-219.
5.McSorley ST, Digby J, Clyde D et al. Yield of colorectal cancer at colonoscopy according to faecal haemoglobin concentration in symptomatic patients referred from primary care. Colorectal Disease 2021;23(7):1615-1621.
6.The total number of FIT tests and the percentage of tests with a f-Hb 10g Hb/g faeces in 2021have been provided from all FIT laboratories across Scotland.
7.Maeda Y, Gray E, Figueroa JD. Risk of missing colorectal cancer with a COVID-adapted diagnostic pathway using quantitative faecal immunochemical testing BJS Open 2021;5(4): https://doi.org/10.1093/bjsopen/zrab056
8.Macdonald S, Macdonald L, Godwin J et al. The diagnostic accuracy of the faecal immunochemical test in identifying significant bowel disease in a symptomatic population. Colorectal Disease 2021;24(3):257-263.
9. Delson D, Ward M, Haddock R et al. Impact of faecal haemoglobin-based triage of bowel symptoms presenting to primary care on colorectal cancer mode of presentation and stage at diagnosis. Colorectal Disease (submitted for publication).
10. Data kindly provided by Bowel Screening Scotland.
11. Monahan KJ, Bradshaw N, Dolwani S et al. Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG). Gut 2020;69:411-444.
12. Scottish Referral Guidelines for Suspected Cancer. 2019.
13. Gerrard A, Maeda Y, Miller J, Gunn F, Theodoratou E, Noble C, Porteous L, Glancy S, Maclean P, Pattenden R, Dunlop M, Din F. A cohort study comparing test performance characteristics of a single faecal immunochemical test (FIT) with double FIT testing for patients referred with symptoms suspicious of colorectal cancer (submitted for publication).
**The above guidance has been developed through a collaboration of over 120 primary and secondary care clinicians and service teams from across all Health Boards, patients and Scottish Government.
Contact
Email: ceu@gov.scot