Review Body on Doctors' and Dentists' Remuneration (DDRB): written evidence - 2024-2025 pay round
Remit letter and written evidence submitted to the Review Body on Doctors’ and Dentists’ Remuneration (DDRB) by the Scottish Government for the 2024 to 2025 pay round.
G. Specific Staff Groups – Pay, Terms and Conditions
General Medical Practitioners
Introduction
125. This section provides information relating to general practice (independent contractor GMPs) and the delivery of contracted services through the NHS Boards. This section provides additional background to developments with the GMS arrangements in Scotland, and the implementation of the new contract in 2018.
Background
126. The majority of GMPs working to provide primary medical services in Scotland are independent contractors, self-employed or partnerships running their own GP practices.
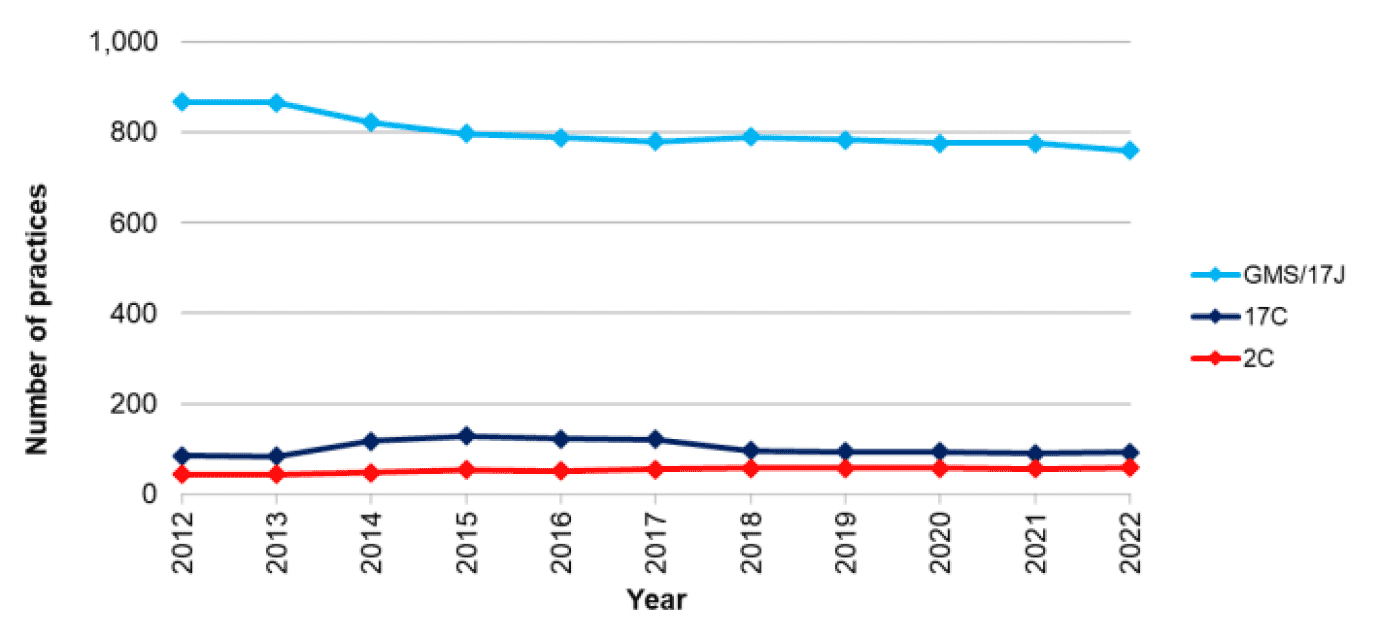
127. The General Practice – GP workforce and practice list sizes was published on 13 December 2022. As of 1 October 2022, there were 911 GP practices[18] in Scotland and 83% were on the national General Medical Services contract. The number of practices in Scotland has decreased by 9% from 997 practices in 2012, reflecting a trend towards larger practices with more GPs serving a larger number of patients. GMPs operating under Section 17C or 2C arrangements provide services based on locally agreed contracts, and any uplift in investment for these arrangements is a local matter for the Health Board.
128. As of 1 October 2022:
- 759 practices operated under the General Medical Services Contract;
- 93 practices operated under the 17C contract; and
- 59 practices operated under the 2C contract[19].
129. The headcount of GPs in Scotland is 5209. This is a slight rise of 32 GPs compared to 2021. Prior to 2018, the headcount of GPs had remained roughly constant at around 4,900 since 2012[20].
130. As of 30 September 2022, 1956 (38%) of the GP workforce were male and 3217 (62%) female[21].
131. The average (or mean) size of a Scottish GP practice in terms of numbers of registered patients was 6470 in 2021[22], however there was considerable variation, ranging from under 200 patients for practices in remote locations or practices which addressed specific health needs of patients (e.g. those with challenging behaviours or homelessness), to practices of over 20,000 patients in densely populated urban areas.
2018 GMS Contract
132. The 2018 Contract came into effect on 1st April 2018. It was agreed through a process of collaborative negotiations between the Scottish Government and the SGPC.
133. The contract includes:
- Improving access for patients;
- Addressing health inequalities and improving population health, including mental health;
- Providing financial stability for GPs;
- Reducing GP workload through the expansion of the primary care multidisciplinary team;
- Increasing support for GPs and GP infrastructure;
- Increasing transparency on general practice funding, activities and workforce to assist strategic planning, commissioning and delivery of primary care services; and
- Making general practice a more attractive profession for existing GPs, junior doctors and undergraduate medical students.
134. One of the core aspects of the new Contract is the new funding model as the Scottish Government recognises that an appropriate and secure level of income is a prerequisite to attracting GPs to the profession and ensuring the future sustainability of general practice.
135. The new contract will be introduced in two phases. Phase One included:
- A new workload formula to better match resource to demand;
- Additional investment of £23 million to allow most practices to gain from the new funding formula, whilst the remaining practices have received an income guarantee to protect their income level to ensure no practice was destabilised; and
- From April 2022, a GP Partner whole-time-equivalent minimum earnings expectation. This means that no GP will receive less than £93,824[23], NHS income per year (including pension contributions) for a whole-time post. This is due to be uplifted in line with DDRB recommendations.
136. These initial changes will be followed by Phase 2 dependent on a further vote from the profession. Phase 2 will include:
- Introducing an income range for GP Partners that is comparable to consultants; and
- Directly reimbursing practice expenses.
137. These proposals are based on evidence from the 2017 Review of GP Earnings and Expenses[24].
Pay and Contractual Uplift 2022/23
138. For 2023/24 the Scottish Government implemented the DDRB recommendation to uplift GP pay net of expenses by 6%. In total the Scottish Government uplifted the GP contract by £60.4 million. This also included a 6.5% uplift to practice staff expenses, and a 6% uplift to wider practice expenses. This also included £8.3 million funding to cover population growth in 2022/23.
139. The contractual uplift was applied consistently across all general practices.
Investment in General Practice
140. Investment figures for 2018/19 were published on 19 September 2019[25]. They show that for the period 2018/19 the total spend on General Practice (including the reimbursement of drugs dispensed) was £992.5 million in Scotland, an increase of 6.53% from 2017/18. Total spend on General Practice 2018/19 (excluding the reimbursement of drugs dispensed) was £967.5 million in Scotland, an increase of 6.81% from 2017/18. From 2020, this series of publication has been discontinued.
Agreement to Publish GP Earnings
141. Following an agreement between Scottish Government and SGPC NHS payments to practices have been published since May 2015 beginning with the publication of 2013/14 data.
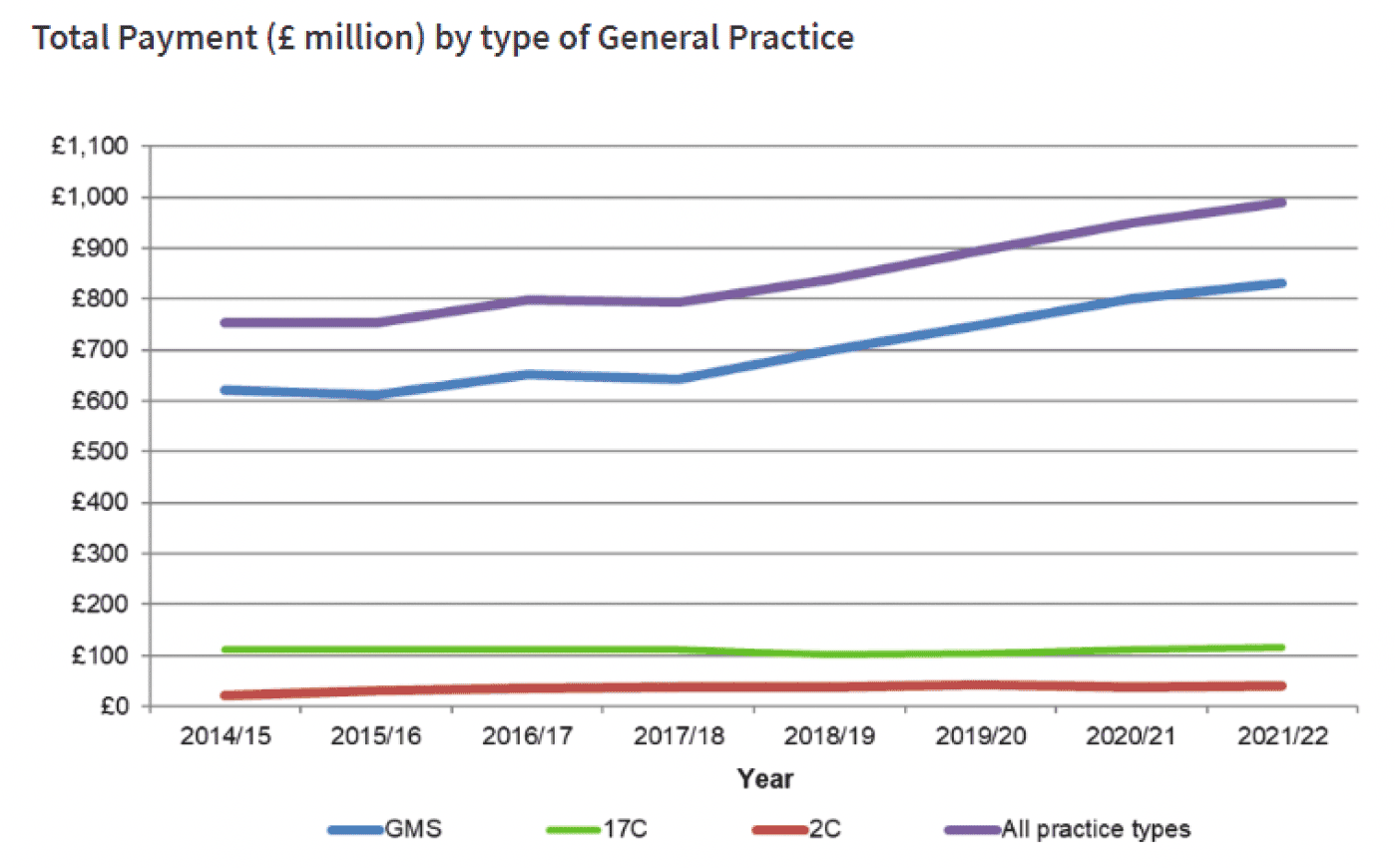
142. In 2021/22 the sum of NHS Scotland non-dispensing payments made to 923 General Practices was £989.4 million[26]. Investment had increased by £38.9 million (4.1%) when compared to 2020/21.
- £832.1 million was paid to General Medical Services (GMS) contracted practices run by GPs[27];
- £116.7 million was paid to locally negotiated contracted practices (17C) run by GPs[28]; and
- £40.5 million was paid to NHS Board run practices (2C)[29].
143. Of the £989.45 million paid in 2021/22: The Global Sum was the largest payment amounting to £670.4 million to 923 General Practices[31].
144. In addition to the £989.4 million, £22.2 million was paid to 85 General Practices for dispensing services in 2021/22, an increase of £0.3 million, paid to 88 General Practices for these services in 2020/21[32].
145. The new contract means an increase of data collection. This will include requiring all practices to provide data on earnings, expenses, hours and sessions. This data will be held confidentially and processed by NHS National Services Scotland Practitioner Services. Only anonymised, non-identifiable data will be provided to the government and NHS Boards for the purpose of analysis.
Vacancy, Turnover and Attrition Rates
146. According to the General Practice Workforce Survey Scotland 2022[33], 37% of GP Practices reported that they had vacant GP sessions from 1 April 2021 to 31 March 2022, in comparison with 32% of practices in 2019[34]. The overall vacancy rate was 8.7 vacant GP sessions for every 100 total GP sessions. The vacancy rate varied by NHS Board. Discounting the Island Boards rates which are subject to volatility due to small numbers, the vacancy rate ranged from 5.6 vacancy sessions per 100 GP sessions in Greater Glasgow and Clyde, to 113.7 vacancy sessions per 100 GP session in Lanarkshire.
| NHS Board | Percent of Responding Practices Reporting a Vacancy | Vacancy Rate2 |
|---|---|---|
| Ayrshire & Arran | 45% | 8.5 |
| Borders | 67% | 10.1 |
| Dumfries & Galloway | 26% | 8.8 |
| Fife | 47% | 10.7 |
| Forth Valley | 30% | 6.3 |
| Grampian | 52% | 12.5 |
| Greater Glasgow & Clyde | 21% | 5.6 |
| Highland | 24% | 7.2 |
| Lanarkshire | 44% | 13.7 |
| Lothian | 52% | 9.1 |
| Orkney | 25% | 7.4 |
| Shetland | 67% | 25.5 |
| Tayside | 44% | 7.8 |
| Western Isles | 33% | 11.9 |
| Scotland | 37% | 8.7 |
1. Figures for Island boards may be impacted by small numbers.
2. Vacancy rate is the number of vacancy sessions per 100 total GP sessions.
| NHS Health board | Sick Leave | Maternity Leave | Parental Leave | Special Leave | Self isolation |
|---|---|---|---|---|---|
| Scotland | 27,296 | 35,744 | 2,422 | 1,974 | 20,579 |
1. The estimated number of absent sessions (in the absence of a 100% survey response rate) was based on scaling the sample headcount from the survey to match the national headcount from NPCCD.
Recruitment and Retention
147. Between 2008 and 2017 the headcount of GPs remained roughly constant at around 4900. In 2017, Scottish Government committed to increasing numbers by at least 800 over the next ten years.
148. In 2023, we continue to make good progress towards this commitment with the number of GPs increasing by 106 over the last two years, to a total of 5209, as at 1 October 2022, which was a record number of GPs working in Scotland.
149. As we strive to meet our 2027 recruitment challenge, we have significantly improved fill rates for GP Speciality Training. GPST fill rates have achieved close to 100% over the previous five years, with 35 additional posts being approved last year for 2023 recruitment. This will help towards meeting the Scottish Government’s commitment to have 800 more GPs in Scotland by 2027.
150. We are also taking forward a number of initiatives to make general practice a more exciting and attractive specialism. This includes -
- Continuing to offer the £20,000 bursaries for GPST posts in “hard to fill areas” in 2023.
- Expanding training opportunities within Primary and Community-based practices.
- Enhancing roles of GPs via Fellowships.
- Reviewing the trainee selection criteria to ensure it is fit for purpose.
- Enhancing the GP Returners Programme to encourage those who have left the profession to return.
- Increasing exposure to primary care at undergraduate level
151. The high level of trainee recruitment has been maintained in 2023 with 100% of GP training posts advertised so far this year filled successfully.
152. To help retain current workforce, the GP Retention Working Group has just established a set of recommendations to continue our work to develop effective approaches to supporting the GP career pathway and retaining our valued GPs in service. We will be working at pace with partners to take these new recommendations forward.
153. Seniority Payments for Scottish GPs are set out in chapter 10 of the annual Statement of Financial Entitlements (SFE)[35]. Seniority Payments reward experience, based on years of reckonable service adjusted for superannuable income factors. Seniority Payments are made to the practice for payment to individual GPs.
154. Presently a GP has to work for six years before any seniority payment is made; for 6 years to achieve a payment of £600 per annum, for 21 years to achieve a payment of £5,129 per annum, for 36 years to achieve £10,258 per annum, with the maximum of £13,900 per annum payable being made at the 47 year point[36]. The contractor has to have been in an eligible post for more than 2 years in order to be able to apply.
155. The Scottish Government’s annual bill for seniority payments to GPs was £16.9 million in 2021/22[37]. There is no change on the £16.9 million in the previous year 2020/21[38].
156. ‘Golden Hellos’ for Scottish GPs are set out in chapter 11 of the annual Statement of Financial Entitlements (SFE). Golden Hellos are a lump sum payment to doctors who are starting out as GP performers in their first eligible post. Posts are considered to be eligible if they are attracting payments for remoteness, rurality or deprivation. Golden Hellos can also be paid to new GP performers if the local Health Board believes the practice is experiencing significant difficulties around recruitment and retention. These are just for GPs in GMS practices with the exception of Golden Hellos for remoteness and rurality which are for all practices regardless of contractual status.
| Reason | Payment |
|---|---|
| Recruitment Difficulty | £5,000 (minimum) |
| Remoteness or Rurality | £10,000 |
| Deprivation | £7,500 - £12,500 |
157. The rate of payment for part time GPs, with a time commitment fraction of less than 4 sessions per week is 60% of the full payment.
Salaried GPs
158. The General Practice Workforce Survey Scotland 2022 estimated that 72% of GPs were Independent Contractors[39]. It estimated that there were around 1221 salaried GPs (27%) and 61 GP retainees (1%).
159. The survey also found that Performer GPs, who had an average of 0.82 WTE per GP. Performer Salaried (0.67 WTE per GP) and Performer Retainer (0.44 WTE per GP) were more likely to work part time.
160. The document sets out a breakdown of the GP workforce by gender, however we do not have current data to indicate whether these GPs were independent contractor or salaried GPs.
GP Expenses
161. Data on GP income and expenses data is provided annually by NHS Digital on behalf of the four countries[40], and which, for the tax year 2021/22, was published on 31 August 2023. We invite DDRB to consider this report in its entirety, but for the purposes of independent contractor GPs in Scotland the report showed that:
162. The average taxable income for contractor GPs in General Medical Services in the UK was £153,400 in 2021/22. In Scotland the average taxable income for contractor GPs was £119,500. Ahead of Phase 2 of the GP contract, this is the only data the Scottish Government has about general practice expenses.
| Contract Type | Year | Report Population | Gross Earnings | Total Expenses | Income Before Tax | Expenses to Earnings Ratio |
|---|---|---|---|---|---|---|
| GPMS | 2020/21 | 3,250 | £255,666 | £140,200 | £115,400 | 54.9% |
| 2021/22 | 3,250 | £269,000 | £149,500 | £119,500 | 55.6% | |
| Change | 0 | +5.2% | +6.6% | +3.5% | +0.7 Percentage Points | |
| GMS | 2020/21 | 2,900 | £251,400 | £136,600 | £114,800 | 54.3% |
| 2021/22 | 2,850 | £265,100 | £146,000 | £119,100 | 55.1% | |
| Change | -50 | +5.4% | +6.9% | +3.7% | +0.8 Percentage Points | |
| PMS | 2020/21 | 350 | £290,400 | £170,100 | £120,300 | 58.6% |
| 2021/22 | 350 | £300,200 | £177,400 | £122,700 | 59.1% | |
| Change | 0 | +3.4% | +4.3% | +2.1% | +0.5 Percentage Points |
163. During 2017 the Scottish Government commissioned Deloitte to undertake a Review of GP Earnings and Expenses[42]. It found that 70% of practice costs (on average) were staffing costs, followed by premises which accounted for 16% of practice costs.
164. There was some evidence indicating that partners in urban practices earned on average more than partners in remote practices. No correlation between average net income and deprivation was found. There was also some limited evidence that larger practices had a higher net income per partner GP than smaller practices.
Workforce Data for Scotland
165. The General Practice Workforce Survey Scotland 2022 captures aggregate workforce information from Scottish general practices and each of the NHS Board-run GP Out of Hours services. It provides the most comprehensive information available on the staffing cohort of general practice, both in hours and out of hours, but does not provide the cost. The costs of running a practice are a matter for the GP partners, including what pay they award employees. The 2022 survey was published in November 2022[43].
166. The 2022 results for Scottish general practices are based on survey data received from 707 responding practices. Of these, 123 did not fully complete the survey, 25 practices did not return individual staff data, and 42 practices were excluded due to poor data quality. The results include information on:-
- Estimated WTE numbers of GPs in post in Scottish general practices, along with information on patterns of sessional commitment by age and gender (a GP's week is typically defined in terms of sessions rather than hours, with a working day generally being comprised of two or sometimes three sessions).
- Estimated headcount and WTE numbers of nurse practitioners and other registered nurses employed by Scottish general practices, along with information on the age profile of these staff.
- Use of locum GP time and extra nurse time by Scottish general practices.
- Known vacancies for these professional groups in general practices from 1 April 2021 to 31 March 2022.
167. The Primary Care Out of Hours workforce survey 2022 was published in 2023 and the main points from that survey were:
- The number (headcount) of GPs working for Primary Care Out of Hours (OoH) services in Scotland in the year ending 31 March 2022 was 1,392, equating to an estimated Whole Time Equivalent of 232.
- Within Primary Care OoH services, 9% of the GPs worked 1,000 hours or more over the year and their total annual hours accounted for nearly half (45%) of the total GP hours worked.
- Eight NHS Boards had to take additional action at least weekly to ensure shifts are filled, either by extending shifts, having nurses cover GP shifts or vice versa, or by offering additional financial incentives.
- As observed in previous surveys, GPs aged over 55 years worked a higher average number of hours per week in Primary Care OoH services than younger GPs.
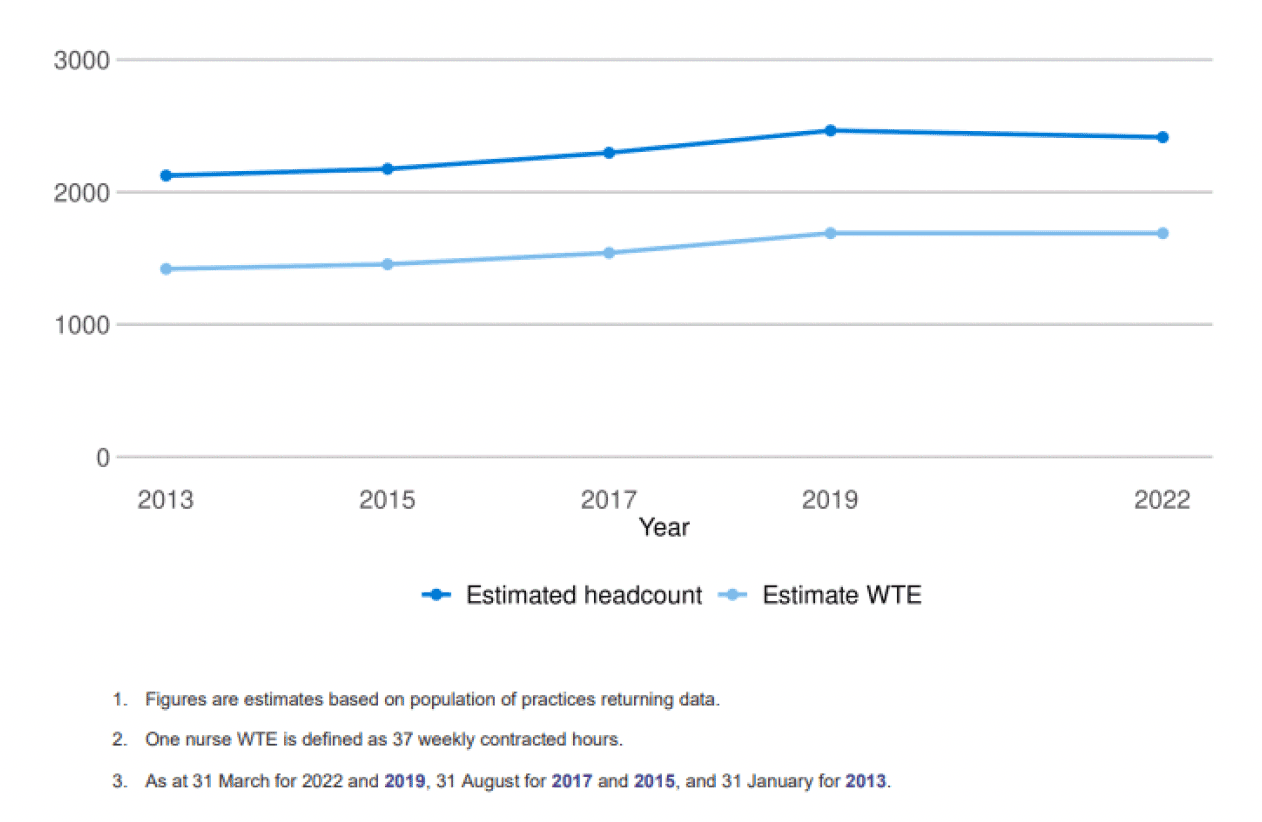
168. The estimated number (headcount) of registered nurses working in GP practices in Scotland in 2022 was 2414, a decrease of 51 from the 2019 survey. The estimated WTE for all nurses was 1,690 (based on 37 hours or more per week being full time), representing the same estimated WTE as the 2019 survey.
169. The largest group of nurses working at General Practices were General Practice Nurses, accounting for 63% of the estimated Nurse headcount and 60% of the estimated Nurse WTE. The next largest group are Advanced Nurse Practitioners (ANPs) and Nurse Specialists, accounting for 27% of the estimated Nurse headcount and 31% of the estimated Nurse WTE.
170. The figures from this survey do not represent the entire registered nurse workforce working in Scottish general practices. They exclude nurses who are employed by NHS Boards but who work in independent contractor practices.
171. Overall, 86% of all responding practices reported the use of a locum GP during 2021/22, with the estimated use of 292 Locum GP WTEs. This is higher than the 273 WTE estimated from the 2019 survey.
Figure 3: Number of internal locum sessions required over 12 months, Scotland; 2013 - 2017[44]
| NHS Board | Percent of Responding Practices Using a Locum GP | Estimated Locum WTE |
|---|---|---|
| Ayrshire & Arran | 82% | 10 |
| Borders | 100% | 11 |
| Dumfries & Galloway | 78% | 9 |
| Fife | 84% | 16 |
| Forth Valley | 79% | 8 |
| Grampian | 88% | 34 |
| Greater Glasgow & Clyde | 85% | 63 |
| Highland | 80% | 29 |
| Lanarkshire | 85% | 34 |
| Lothian | 97% | 53 |
| Orkney | 75% | 6 |
| Shetland | 100% | 16 |
| Tayside | 93% | 18 |
| Western Isles | 67% | 2 |
| Scotland | 86% | 292 |
1. Locum GP WTE calculated as the total number of locum sessions filled during 2021/22 divided by 416 (the eight sessions that make up a weekly WTE multiplied by the 52 weeks in the financial year).
2. The estimated WTE (in the absence of a 100% survey response rate) was based on scaling the sample headcount from the survey to match the national headcount from NPCCD. For more details see the Methodology section.
3. The WTE for Scotland has been estimated separately from the WTE for each board, so the Scotland total is slightly different than the sum of the boards’ WTE.
172. There were an estimated 479 Health Care Assistants with an estimated WTE of 317 working in Scottish general practice in 2022 (as at March 31). This shows a 24% decrease in headcount (estimated 627 in 2019) and a 23% decrease in estimated WTE (410 in 2019) compared with the previous survey. For phlebotomists, there were an estimated 103 working at General Practices in Scotland in 2022 with an estimated WTE of 59.6. This shows a similar estimated headcount as in 2019 (104), but with a 5% higher estimated WTE (54 in 2019) compared with the previous survey.
173. The 2018 GP Contract mandates the provision of workforce data to be made mandatory. This will facilitate workforce planning in the future.
Working Hours
174. The Primary Care Out of Hours Workforce Survey Scotland 2022[45] gathered information on GPs working in GP Out of Hours services.
175. Results from the 2022 survey showed that younger GPs were more likely to input fewer hours with the average for under 35s being 3 hours and for 35 to 44 year olds, 5 hours per week on average. This contrasts to those aged 45 to 54, contributing 8 hours, 55 to 59 year olds contributing 9 hours, 60 to 64 year olds contributing 11 hours and those aged 65 years and over contributing 10 hours per week on average.
176. GPs aged under 35 years made up 20% of the OoH workforce, but their combined hours accounted for just 10% of the total hours. Likewise, for GPs aged 35 to 44 years, while they made up 37% of the workforce, their combined hours accounted for only 31% of the total GP hours worked in Primary Care OoH services. GPs aged 45 years and over made up 43% of the OoH workforce, but their reported combined hours accounted for 60% of the total GP hours worked in Primary Care OoH services.
177. During 2017 the Scottish Government commissioned Deloitte to undertake a Review of GP Earnings and Expenses[46]. Like the workforce survey this was also based on a sample of GP practices, and found that GP commitment ranged from under 10 hours per week to over 60 hours per week.

General Dental Practitioners (GDPs)
NHS Dentistry - General Dental Service (Independent Contractors)
Overview
178. The Public Dental Service (PDS) is a NHS Board employed service formed in 2013 two predecessor services that were directly provided by NHS Boards; these being the Community Dental Service (CDS) and the Salaried General Dental Service (SGDS). It was designed to help secure the adequate provision of dental services to the whole population, covering where General Dental Services do not provide sufficient provision in, for example, areas of rurality or for patients with complex needs. The PDS also provides a dental public health function through dental inspection services to educational establishments; undertakes an oral health improvement role (Childsmile); and carries out epidemiological research on behalf of Health Boards to assist in monitoring oral health over time and in planning services.
179. The PDS continues to be managed and delivered directly by Boards which are required to balance and reconcile several important factors
180. Complementarity: general dental services delivered by independent contractors is the preferred vehicle of Scottish Government for delivery of primary dental care to the population of Scotland. It is recognised that independent contractor services are not always viable in all parts of Scotland. Therefore NHS Boards should only provide routine dental care by the PDS where there is a gap in such provision.
- Sustainability: Boards should ensure the continued viability of the services provided, given their often specialised nature as well as the vulnerable sectors of the population served, by working collaboratively with their neighbouring boards to achieve economies of scale.
- Equity: NHS Boards are required to ensure that NHS dental services are available for those who wish to access them in their area. This requirement includes vulnerable groups of people who may be unable to access general dental services, and the CDS traditionally had an important role in enabling NHS Boards to meet this obligation. Boards should ensure that the PDS continues to reduce such inequalities.
- Compliance: the PDS of a NHS Board must comply with the all relevant legislation and regulations.
181. Scottish Government is focused on the delivery of NHS dental reform – which will come into force on 1 November 2023. This is a major payment system reform, with changes being made to both Item of Service and Capitation arrangements.
182. In Scotland the blended payment model also includes a range of allowance payments that were put in place under 2005 reform, these reflect a range of expenses type payments, such as General Dental Practice Allowance and rent (among others). These payments have not been considered as part of the current reforms, however, it is Scottish Government’s intention to undertake bilateral discussion with BDA over the coming year to better inform a discussion through DDRB about expenses – crucially in the light of the reformed NHS dental landscape.
Landscape
183. The payment reform is intended to support the Scottish Government’s ambition to sustain NHS dental services and provide equitable access to services for all patients in Scotland. This has been looked at primarily through the fee per item structure and the introduction of a single capitation payment for all registered patients. There is a major change to the levels of trust that the new system expects from dental contractors, through a move away from a prescriptive range of fees towards a modernised clinical approach and lower bureaucracy.
184. It is important that the committee notes that payment reform is not contract reform – this is because there are no contractual arrangements between Scottish Government and independent dental contractors in Scotland. The method of payment under this reform is the blended model, which under reform includes Item of Service, Capitation and a wide range of Allowances. The payment reform is mainly focused on the Item of Service fees, which was subject to intensive discussion and negotiation with BDA Scotland. Alongside this a single capitation payment replaces the previous capitation and continuing care arrangements to streamline the overall structure.
185. Reform builds on the long-term Scottish Government policy to deliver preventive care, improve periodontal treatment and streamline payment systems that was set-out, in detail under the Oral Health Improvement Plan (OHIP) (2018). The delivery of OHIP commitments is central to the overall approach that has been taken by Scottish Government towards the delivery of NHS dental services through the independent contractor model.
186. In streamlining the payment fees, there is now improved provision of preventive and periodontal treatment alongside providing clinicians with the capability to provide the full suite of NHS treatment to patients. In summary, the new payment model reduces the number of care and treatment items from approximately 700 to 45, allowing improved clinical freedom that supports clinical discretion and delivery of care based on patient need for treatment.
Allowances and Expenses Exercise
187. The intention is to consider allowances through bilateral discussion with BDA through the course of the next year to enable evidence to be provided to DDRB in the context of the reformed payment system. Scottish Government does not consider that it is the right time at present to consider further changes in this connection under robust and rigours assessment of the impact of reform on the sector – including the crucial requirement to sustain equitable access to care for patients.
188. In discussion with BDA over the coming year Scottish Government will seek to agree the overall landscape and scope of future ongoing bilateral discussion space with BDA on these matters. These discussions are clearly defined as being exploratory in nature and state clearly that Ministers remain responsible for decisions relating to government spend on matters around pay and expenses. This process may include an open books exercise, if a suitable approach can be agreed with BDA to take this forward.
Policy approach and engagement
189. The priority for payment reform has been to ensure that fee levels are more reflective of the wider economy costs of delivering modern dentistry through the Item of Service fees. The associated impacts for dental contractors are that improved fees provide an enhanced incentive to remain within the NHS. It should be noted that Item of Service fees feed directly into the allowances system through the relationship between these earnings and the General Dental Practice allowance – which supports the overall operability of businesses to maintain NHS services.
190. The Scottish Government has set out the guiding principle post pandemic to deliver sustainable NHS dental services that are equitable to all patients who wish to use the NHS. There are important financial drivers associated with the provision of NHS services and DDRB will wish to note that value for money spending is key to both the delivery and sustainability of NHS services in the long term, with pay and expenses a key consideration in the light of significantly enhanced Item of Service fees.
191. The development of the reform builds on the extensive sectoral engagement during the development of OHIP and more recent consultation, including a sector-wide survey of dentists, Chief Dental Officer’s Advisory Group and regular engagement with British Dental Association (BDA) Scotland. The reforms address many of the concerns and representations that have been identified and Scottish Government is clear that the conditions are in place through reform to deliver in the majority of areas a consistent level of NHS dental care across Scotland within the independent contractor model.
192. There may be some further interventions required in some areas, for instance remote and rural areas. Scottish Government is working closely with Health Boards where systemic issues, such as availability of workforce may not be sufficient to meet local demand.
Clinical improvement
193. As noted above, the clinical amendments under the reform are highly significant and modernise the delivery of NHS care and the treatment received by patients. The reform is based on moving the sector to a high-trust/low bureaucracy model of payment that reduces the administrative burden for dental teams, and affords far greater levels of clinical discretion to practitioners. The reform also provides greater visibility of NHS care to patients through the reduced number of fee codes, meaning the new system will be much easier for patients to understand.
Wider Context
194. NHS dental services across the UK have been significantly impacted through the COVID-19 – from complete closure, through gradual remobilisation of services to the present position where reform has been implemented. Alongside the pandemic, factors such as EU withdrawal and wider economic conditions have provided specific local and general challenges, such as remote and rural workforce and cost of laboratory made treatment items.
Conclusion
195. Scottish Government is clear that payment reform is a necessary first step to secure the provision of NHS dental services in Scotland, and while it is not a cure-all reform aims to puts the sector into a more stable long-term footing. It is essential to ensure that the reform is given sufficient time to stabilise in the real-live environment, reflecting the financial pressures faced by government across the Primary Care landscape.
196. In connection with the wider issues around expenses these can be aired in the BDA Scotland discussion forum, which will better inform future Ministerial consideration of these matters.
Consultants, Specialty Doctors and Associate Specialists (SAS) and Junior Doctors) including Improving working lives
Pay
197. The BMA Scotland Consultant and Specialty Doctors and Associate Specialists (SAS) have indicated to Scottish Government that they are not willing to participate in the DDRB process for the current pay round as there has been a loss of confidence in the independence of the DDRB and the operation of the pay review process amongst their committees. They believe it has moved away from its original principles and wish to see a reformed DDRB. This is similar to the position that has been adopted by BMA committees in other parts of the Home Nations.
198. As you will be aware the BMA Scottish Junior Doctor Committee have also stated they have lost confidence in the process, which resulted in direct negotiations in 2023/24 which agreed pay deal for Junior Doctors and Dentists as follows:
- A single year pay uplift in 2023/24 of 12.4%.
- For 2024/25, 2025/26 and 2026/27 a guaranteed minimum uplift of inflation for the financial year to which that pay deal relates.
- Agreement to enter full contract negotiations from Autumn 2023 with implementation by April 2026: outcomes to include contract reform and a new Pay Review mechanism.
199. The Scottish Government has consistently supported the DDRB process and the independent recommendations that the pay review body sets. Whilst we are seeking recommendations for all Medical Crafts with the exception of Junior Doctors, we are cognisant of the views of our stakeholders and believe that the time is right for a 4 countries review of the process so that we can seek to work collectively to address the concerns of our stakeholders, and bring back faith in the DDRB from the profession.
Engagement
200. We have recently established a Joint Negotiation Committee comprising of with MSG (NHS Scotland employers/Scottish Government) and BMA Scotland Consultants, Juniors and SAS committees.
201. This fora has replaced the previous tripartite arrangements that we in place with individual BMA committees and it is intended to create a space for the consideration of strategic terms and conditions issues of importance to these medical professions so that discussions on areas of common concern can be conducted in a more holistic and strategic manner. The group meets regularly and, where appropriate, it will produce joint guidance to support the medical workforce in Scotland.
Distinction Awards and Discretionary Points for Consultants
202. It is still the position in Scotland that no new Distinction Awards have been made as these do not align with progressive pay principles of the Scottish Government. There are Consultants who received awards priory to the freeze who are still in receipt. It remains the case that extant arrangements for DAs and DPs will remain in place.
203. Although DAs are frozen to new Consultants, the availability of new DPs increases in line with the number of Consultants in post. Scotland continues to offer an attractive pay package for Consultants along with the continued guarantee of No Compulsory Redundancy. There is no evidence to suggest that an adverse impact has resulted from the freezing of the value of DADPs.
204. We are therefore not seeking any recommendations from DDRB on distinction awards and discretionary points.
Improving the working lives of Acute Hospital Medical Grades
205. The Scottish Government remains committed to the Expert Working Group report on a maximum 48 hour working week for junior doctors with no averaging. In partnership with the BMA and employers, we continue to work to identify specific areas where actual operational improvements can be made to working lives of Junior doctors.
206. BMA and Employers have worked closely with Scottish Government in recent month to produce joint proposal that will seek to improve the process whereby Junior Doctors receive appropriate advance sight of rotas before any rotations.
207. In addition the Scottish Government has worked in collaboration with stakeholders to identify and consider action that may need to be addressed to support Consultants in the latter stages of their career and who were considering peri-retirement. The reports governance arrangements sit within the Shape of Training Transition Group and Scottish Government Health Workforce Directorate, thus ensuring alignment of work on retention with wider work on medical workforce supply/demand, and to longer term medical workforce planning.
Contract Implementation for Speciality and Associate Specialist Doctors and Dentists in NHS Scotland
208. In the autumn of 2022, after many months of negotiation, the Scottish Government came to an agreement with employers and the BMA on the creation of a new contract for both the Speciality and Associate Specialist Doctors and Dentists in NHS Scotland.
209. These new contracts were accepted by BMA members at ballot, and the contracts were implemented on 1 December 2022.
210. Uptake of the new arrangements has been excellent, with over 80% of current Specialty Doctors choosing to move to the new contract. In relation to the new Specialist role we are still in the early days of introducing this grade. A number of posts have been created and filled and indications are that NHS Board are planning to utilise this grade further. NHS Boards continue to explore the use of these roles and the potential service delivery benefits. Over the course of the next year NHS employers intend to monitor the uptake of this grade across NHS Scotland and continue to promote the use of this new role.