Short Life Working Group for Mental Health in Primary Care: report
The Mental Health in Primary Care Short Life Working Group recommended the establishment of Mental Health and Wellbeing in Primary Care Services within areas served by a group of GP practices, providing assessment, advice and support for people who require a mental health or a wellbeing response.
Discussion
Mental Health in Primary Care
12. General Practice are long-standing anchor institutions of their communities providing ongoing care for the mental and physical health across the whole lifespan. Practices provide universal, comprehensive and accessible care to all individuals offering continuity of care, particularly important for those who are socioeconomically disadvantaged, and oversee care from a range of service providers.
13. GPs are increasingly working as part of Multidisciplinary Teams (MDT) within their practice, based in the community or alongside specialist colleagues. The vast majority of patients are cared for in Primary and Community Care close to their homes, especially when supported by an MDT. To reduce stigma and encourage the creation of mental health communities, there has to be acceptance that the responsibility for Mental Health is for everyone and not only for specialist services.
14. GPs are usually the first port of call for people seeking professional help for mental health issues and the vast majority of mental health consultations occur in Primary Care, covering a diverse range of needs. Approximately 1/3 of GP consultations (c8million / year) have a mental health component. GPs may diagnose, treat and monitor the individual themselves or they may refer the individual to specialist services for further investigation, and / or treatment. People can present with mental health issues to other members of the General Practice team, however, this data is less formally captured.
15. The management of people who present with mental health problems in the Out of Hours (OOHs) period varies across health boards and their associated partnerships. A study has shown that people who present with mental health concerns have on average five contacts before they reach the most appropriate person in the OOHs period compared to physical health concerns which have on average two contacts. As OOHs is an urgent care service, the majority of these presentations will be in crisis. This means that timely and easy access to secondary care services for all age groups is essential. It is imperative therefore that when considering people who present with mental health concerns in Primary Care, a 24/7 view is taken of service delivery.
Current Challenges in Service Provision
16. The range and complexity of mental health presentations in Primary Care do not all fit existing pathways of care. While GPs can refer to specialist services, those services may reject that referral on the basis that the condition does not meet the criteria for specialist care, or where people require mental health and substance misuse support, resulting in a referral back to the GP. This means GPs become the primary clinical support for individuals with complex needs that they are not always trained to deal with. Having only general practice involvement in this range of complex needs is unsatisfactory for the person and can have a high impact on GP workload, therefore looking to a multidisciplinary response will ensure the best outcomes for people. It is also important to have strong connections with secondary care mental health services in order to be able to “step up” treatment if needed, as seamlessly as possible.
17. Another concern for GPs is management of less complex mental health issues, often associated with other social stressors. This may require little clinical input and while that is important, it will not address the underlying issues. Links to alternative supports in the community, including social services, community groups and those services delivered by third sector organisations is vital for this group.
18. Patients with severe and enduring symptoms of mental illness need referral to specialist services for diagnosis, treatment and for advice about managing risk including those whose presentation is complex or for whom there is diagnostic uncertainty. They may also require ongoing access to support in Primary Care.
19. GPs are often satisfied with the response such patients receive once they have an established place in secondary care services. But any delay in assessment and care planning may lead to a significant reliance on unscheduled presentations, including to crisis and out of hours’ services. Improved access to prompt scheduled care therefore has the potential not only to improve the patient experience, but also to reduce the overall resource burden on the system.
20. Specialist services also have an important role to play in providing peer-to-peer decision support for the care of people with complex illnesses in the community. This works best in areas that are able to invest in relationships between clinicians across the health and social care interfaces and where access is available to the electronic patient records such as Clinical Dialogue.
21. There are significant challenges with obtaining access to mental health specialist service provision for children and adolescents. Contributing factors to this include long waiting times and high levels of rejected referrals. Primary Care mental health teams that are able to offer crisis intervention and support to young people early in their journey, significantly limit potential future damage for young people and their families.
Where Primary and Community care fits into an integrated mental health care system
22. Primary and Community Care Teams have a pivotal role within an integrated mental health system and are key in developing and sustaining a system that supports the population with improved mental health and wellbeing. The services provided by such teams is necessary, but not sufficient: they depend on a wider system of care to function optimally. The Scottish Government Mental Health Transition and Recovery[1] plan sets out the range of areas where improvements are required to deliver an improved mental health and wellbeing service to the wider population.
23. An integrated system requires strength across all components, including public health messaging for the whole population, provision of information to assist self-management, third sector provision of community services and Primary and Community care as well as highly specialised aspects of care and treatment.
24. The role of Primary and Community care is central to this system, as illustrated in the diagram below:
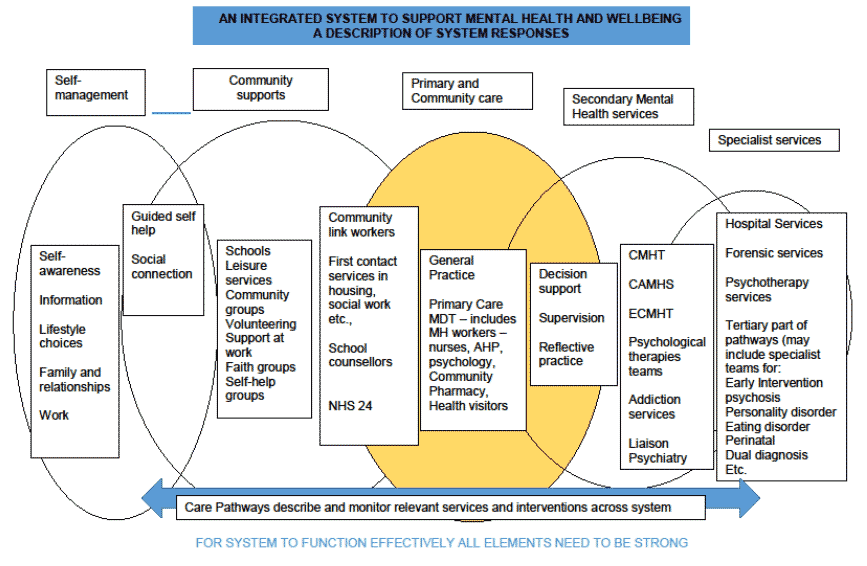
The figure above, provides a diagram overview which reflects an Integrated System to support Mental Health and Wellbeing; Mental Health Care Pathways.
The Care Pathways describe what services are available from Self-Management, Community Supports, Primary and Community care, Secondary Mental Health services through to Specialist services. To ensure all elements within the Care Pathway system functions are effective and strong, ongoing monitoring and interventions are needed.
The diagram shows the pivotal and central role, Primary and Community Care Teams have within an integrated mental health system and are key in developing and sustaining a system that supports the population with improved mental health and wellbeing.
The teams and services provide on a wider system of care to function optimally and an Integrated system requires strength across all components, including highly specialised aspects of care and treatment.
25. Primary Care provides support and care to the majority of those that seek help but also provides the link into secondary and more specialist services where required.
26. There is widespread recognition that the Primary Care part of the Mental Health system requires attention and development. A range of local initiatives have been supported through recent Primary Care Improvement Funding and/or funding via Action 15 of the Mental Health Strategy for Scotland[2]. Many of these initiatives to date are described in the evidence paper that accompanies this report. Further evidence can be found in ‘Exploring Distress & Psychological Trauma’ research commissioned by NHS Greater Glasgow and Clyde[3] and ‘Mental health and Primary Care networks - Understanding the opportunities’ a report published jointly by the King's Fund and the Centre for Mental Health[4]. These reports highlight both the concerns and the opportunities that exist to improve this aspect of the system.
27. Whist the distress/crisis response element within mental health is very important, it is part of the wider multi-disciplinary system and at the moment services are being developed in silos, without the overview of how different aspects of care and treatment will connect with each other. For the Primary Care team, it is really important that they can understand the system to navigate appropriately on behalf of their patients, with whatever form of mental health problems/symptoms they are experiencing.
28. This report and its recommendations focus on early clinical intervention by MDTs, supporting ‘key priority 5’ in the Memorandum of Understanding (MoU) between Scottish Government, British Medical Association, Integration Authorities and NHS Boards.[5] This priority requires that additional professional roles will provide services for groups of patients with specific needs that can be delivered by other professionals as first point of contact in the practice and/or community setting. These additional roles should include community clinical mental health professionals (e.g. nurses, occupational therapists, psychological therapists and enhanced practitioners) based in general practice. The MoU envisages that “by 2021 specialist professionals will work within the local MDT to see patients at the first point of contact, as well as assessing, diagnosing and delivering treatment, as agreed with GPs and within an agreed model or system of care. In line with the recommendations in this report, it provides for service configuration to vary dependent upon local geography, demographics and demand.” Current system configuration/demands present significant challenges to implementation. This report seeks to describe the kind of system changes which would be required to make this possible.
29. Below are examples of existing models demonstrating how mental health support services are integrated in Primary Care settings:
30. In Lanarkshire, Occupational Therapists (OTs) are working in Primary Care settings offering open access appointments to patients requiring prevention and early intervention solutions. This enables patients to self-manage their condition and build resilience. OTs are skilled in assessing components of everyday occupations and roles that matter to people, identifying the impact of development, physical and mental health conditions on these occupations and devising intervention plans to enable people to overcome such impacts and engage fully in their day to day lives. OTs use scientific bases, and a holistic perspective to promote a person's ability to fulfill their daily routines and roles.
31. Mental Health Liaison Nurses are also used in Lanarkshire, providing triage, assessment and short term intervention to people experiencing mild to moderate mental health problems of a short term nature.
32. In Lothian, Dumfries & Galloway and Lanarkshire, Mental Health Nurses have been recruited to meet the needs of patients with mild to moderate mental health difficulties. Their interventions consist largely of clinical advice/triage, crisis management, case management of those with complex mental health needs, general psychological support, brief intervention, treatment for addiction, independent prescribing and signposting to local services. In Lanarkshire, they have built on this to develop a stepped/matched Mental Health & Wellbeing Service model, using Action 15 funding. It has continued to expand, with the service being rolled out to 40 GP practices.
33. In Ayrshire and Arran, they are increasing mental health provision within Primary Care Teams/Clusters by embedding Community Link Workers and Mental Health Practitioners within Primary Care Teams to assist with sign-posting, access, and provision of time limited interventions. They have seen great value in having Mental Health and Psychological Therapy aligned with Primary Care.
34. In Grampian and Lanarkshire, the Accessible Depressions & Anxiety Psychological Therapies model increases access to psychological therapies and interventions in Primary Care adult mental health and develops the specialist mental health workforce in secondary care. This is achieved through expanding the competencies of the existing workforce to deliver the most effective treatments, developing Primary Care Teams with multiple disciplines and providing guidance and support on the model of service delivery. This enables cost-effective stepped care, patient choice, quality assurance and increases capacity.
35. In Fife, a comprehensive matched care model offers a wide and flexible range of early intervention, self-help, groups and one to one psychological therapy including integrating web based, remote and face to face interventions.
36. In Scottish Borders, a recent development is a partnership between GPs/Primary Care and Mental Health utilising funding from PCIP and Action 15. This is a collaborative Primary Care service that is currently operating completely remotely, offering a wide range of interventions.
37. The most important common factor is that each of these approaches are moving towards a reframing of the ‘task’ for Mental Health and support workers in Primary Care settings. The traditional model prioritises triage and diagnosis, with a view to identifying people who will be accepted for care by specialist Mental Health services on the basis of ‘mental illness’.
38. A more useful model in Primary Care settings is a prompt and compassionate response to all forms of distress, which is provided at a local level using community assets and peer networks wherever possible. Specialist Mental Health input must be available whenever indicated, but should not be the default response for all presentations.
39. Other common factors in the success of these services are:
- Where available, regular reflective practice (or other wellbeing support) to deliver a sustainable, timely and compassionate mental health service.
- Taking a person centred approach to meet the needs of the person in a timely way.
- Integration with digital/remote Primary Care mental health and wellbeing resources, increasing access to resources such as NHS inform, interactive self-care guides, NHS 24’s 24/7 mental health hub, Breathing Space crisis line and computerised CBT.
- Alignment with Primary Care and the use of the wider multi-agency team.
- Close linkage with Social Work and addiction services in the locality.
- Raising GP Awareness about the role and availability of the wider multi-agency team.
- Providing continuity of care.
- Highlighting the importance of providing training, standardised operational procedures and opportunities for feedback.
- Increased GP cluster working.
- Integration of psychological therapy pathways, reflective practice, training and supervision.
- Utilising a stepped/matched care model of evidence based treatment. Fidelity to an evidence based model has been shown to consistently improve outcomes.
- Access is available to the electronic patient records.
40. These factors have resulted in people accessing the correct support quickly, leading to better outcomes for them. This in turn leads to a reduction in GP, GP Practice and clinical attendance rates.
Contact
Email: MHWPCServices@gov.scot