Realistic Medicine and Value Based Health and Care Casebook
The Realistic Medicine Casebook shows how teams across Scotland are putting Realistic Medicine into practice. It’s a practical guide offering inspiration and support for those adopting its principles and a celebration of progress in transforming care to deliver what matters to the people we care for
Reducing Waste, Harm and Variation, and Managing Risk
About 20% of spending in health and care doesn’t achieve the outcomes that matter to people. Reducing harm and waste means making the best use of our precious health and care resources and providing better care and outcomes for the people we care for.
We know that shared decision making conversations make a positive difference to the outcomes that matter. More meaningful conversations are associated with less decision regret and people are more likely to value the care they receive. In so doing, we can reduce harm and waste and focus on delivering care that truly matters. People’s attitudes to risk vary and are shaped by values, beliefs, and personal circumstances. Having meaningful conversations about risk and benefits empowers informed choices.
Unwarranted variation arises when there is variation in care which can’t be explained by the needs of the people we care for. Practising Realistic Medicine seeks to reduce unwarranted variation ensuring that we prioritise evidence based care which makes a difference and helps to ensure equity of access to care for people who are likely to benefit most. This is key to improving outcomes across Scotland.
The following case studies demonstrate how we can reduce waste and potential harm, tackle unwarranted variation and manage risk better.
Project Milkshake – Enhancing Nutrition in Care Homes
Project Milkshake, led by dedicated care home dieticians and the NHS Greater Glasgow and Clyde Care Home Collaborative, aims to combat malnutrition and improve residents’ nutritional intake through innovative and sustainable approaches.
The project emerged from a necessity to address insufficient nutritional intake among residents, despite the availability of existing milkshake provisions. Observations revealed that the offered recipes were often too rich, leading to adverse reactions and low consumption rates. Concurrently, an increase in supplement prescriptions highlighted the need for improved dietary management strategies. With updated guidelines Care Home Digest - British Dietetic Association (BDA) advocating higher protein intake for older adults, Project Milkshake sought to develop tailored interventions to meet these requirements effectively.
Rooted in the principles of Realistic Medicine and Value Based Health and Care (VBH&C), the initiative prioritises personalised, evidence based interventions to enhance wellbeing, while ensuring the most effective use of resources. Initiated by an advanced practice dietitian, the project introduces fortified milkshakes as a first-line intervention to reduce reliance on dietary supplements and enhance residents’ dietary experience.
Project Milkshake aims to improve residents’ nutritional status by creating high-protein, nutrient-dense milkshake recipes tailored to their dietary needs. By incorporating “Food First” strategies, it seeks to reduce dependency on prescribed supplements. This aims for optimal health outcomes without increasing healthcare costs and ensuring that resources are allocated effectively. Additionally, the project emphasises enhancing interdisciplinary collaboration between catering and care staff to deliver comprehensive nutritional care.
The pilot phase took place in two care homes within the Health and Social Care Partnerships (HSCPs) of Renfrewshire and East Dunbartonshire. Key steps included:
- Recipe Development – a total of 30 recipes were initially evaluated through tasting events with residents and their families. Based on feedback, 14 recipes were selected for implementation.
- Training and Engagement – two champions and two chefs per care home underwent comprehensive training, covering nutrition, recipe preparation, and strategies to enhance mealtime experiences.
- Monitoring and Feedback – a fluid balance chart-like system was introduced to track residents’ preferences and intake, ensuring recipes were well received and minimising waste.
Outcomes and Impact
Nutritional Improvement – pilot care homes demonstrated significant improvements in nutritional risk scores and BMI, with no residents requiring supplements or remaining on the Dietetic caseload after six months.
Reduction in Falls – in one home, falls decreased by 44% over 29 weeks, suggesting a link between improved nutrition and reduced falls risk.
Staff Collaboration – enhanced communication and collaboration between care and catering staff, with chefs actively participating in care planning and daily meetings.
Resident and Family Engagement – tasting events and feedback mechanisms ensured residents’ preferences were prioritised, resulting in higher acceptance of fortified milkshakes.
"My goodness, he has come on great. He stood up and gave me a hug
this morning."
Staff member talking about one of the residents
"Having the whole team trained – from domestics to nursing staff, has made them take greater interest in the nutrition of residents."
Care home manager on Project Milkshake
"The strawberry milkshake makes me think of sunny days and I like the fruit ones too."
Care home resident
"I have simple tastes and I prefer the less sweeter options."
Care home residen
Building on the pilot’s success, the project expanded to a third care home, focusing on a residential care model without nursing involvement. This phase introduced new data collection methods, including grip strength measurements, to further evaluate the intervention’s impact.
The next phase of Project Milkshake will expand across multiple HSCPs, supported by comprehensive resources on a dedicated NHS Greater Glasgow and Clyde webpage. Care homes will receive training materials, recipe books, and instructional packs, with dietitian support during setup and ongoing guidance.
In October 2024, 6 launch events trained 115 staff from 35 care homes. Of the 71 evaluations submitted, 100% reported improved confidence in identifying and managing nutritional risks, and all care homes expressed enthusiasm for continued support.
Feedback highlighted the importance of a collaborative, team-based approach to nutritional care, demonstrating the training’s success in fostering teamwork and enhancing staff capabilities. By aligning with Realistic Medicine and VBH&C principles, Project Milkshake has demonstrated that structured, personalised interventions can significantly enhance nutritional health and wellbeing while reducing waste.
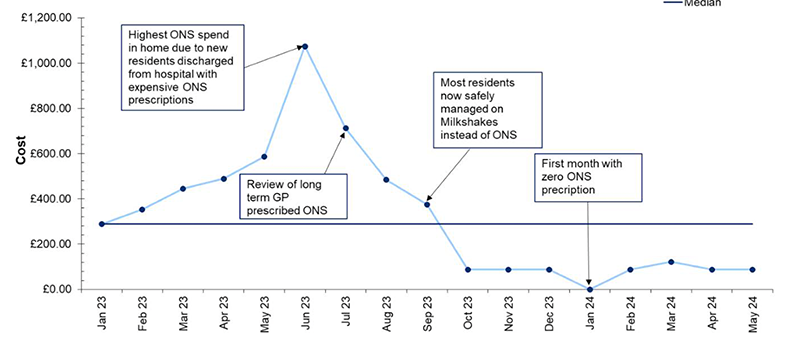
The cost of Oral Nutritional Supplements has significantly decreased over time, dropping from £1,085 in January–March 2023 to just £174.72 in April–May 2024. By leveraging national channels to share insights and resources, Project Milkshake aims to shape more sustainable and effective nutritional care practices across Scotland’s care home sector.
Further resources can be accessed on Food First and Project Milkshake | Right Decisions (scot.nhs.uk)
Figure 2: GP ONS Spend for residents in pilot home 2 on Project Milkshake
In conclusion, this initiative highlights the significant benefits of listening to and understanding what matters to people, resulting in care that is personalised and impactful. For residents, this approach has led to better outcomes, such as improved strength and reduced risk of falls, enhancing their quality of life. Care homes have also seen advantages, including reduced waste and cost savings, demonstrating the value of aligning care with residents’ needs and preferences.
Additionally, staff have experienced increased wellbeing and job satisfaction, as they witness firsthand the positive difference their care makes. The project has also strengthened relationships between residents, chefs, and carers, fostering a collaborative environment built on meaningful conversations and shared goals. Together, these benefits underline the transformative potential of this approach for everyone involved.
Incremental Haemodialysis in Inverness
Nearly 2,000 people in Scotland currently receive haemodialysis, a life-sustaining treatment for individuals whose kidneys have stopped working, involving connection to a dialysis machine that cleans the blood, typically for three-to-five hours per session. While this treatment is lifesaving, it carries significant costs for patients, the healthcare system, and the environment. Each dialysis session uses around 400 litres of water, with two-thirds going to waste, and it is calculated that 7.1 tonnes of CO2 are emitted per year for each dialysis patient.
NHS Highland have introduced Incremental Haemodialysis, an approach that begins with twice-weekly dialysis instead of the standard three sessions per week. Their approach was featured in the Chief Medical Officer’s 2024 report Realistic Medicine – Taking Care, but here we are revisiting it to update on the significant impact of this change.
By starting dialysis incrementally, we can make the most of the kidneys remaining function in the early stages, reducing the treatment burden for people while maintaining safe, effective and personalised care.
NHS Highland was the first UK centre to apply this evidence based approach to all new dialysis patients, with ongoing monitoring to guide the transition to more frequent sessions when clinically necessary. Taking an evidence informed approach, the specialist renal team in NHS Highland has transformed the service being delivered – establishing an incremental dialysis pathway.
Now around 35% of all of NHS Highland dialysis patients receive twice weekly dialysis reducing the total number of haemodialysis treatments by 12% every week.
People dialysing with incremental haemodialysis have one more day to themselves every week instead of travelling to and from hospital and being attached to a dialysis machine, giving them more time to enjoy their usual activities. It has reduced the need for transport to and from dialysis. It has cut down on the plastic waste produced by every dialysis treatment which uses a dialyser, needles, blood lines etc. It has reduced the amount of nursing time needed so it has been possible to close one entire dialysis shift.
The first two-and-a-half years of this approach saved:
- 2,923 haemodialysis treatments avoided.
- 6.5 tonnes non-recyclable waste.
- 132 tonnes of CO2 emissions saved.
- 67,111 miles travelled saved.
- £153,772 taxi costs saved.
- £5,297 travel reimbursements saved.
- £50,000 haemodialysis consumables saved.
- £2,957 waste disposal costs saved.
94% of patients felt that starting dialysis twice weekly was better than starting three times weekly.
People reported:
"It reduces my travelling time by four hours a week."
"It allows me to work an extra day at my local charity shop."
"I was able to keep working."
"I can walk the dogs, see my grandchildren and get some work done in the garden."
It has been a huge success for NHS Highland, delivering better value healthcare by returning time to people, reducing overtreatment and waste and reducing NHS costs. This method has been adopted in 50% of units in Scotland, the wider UK and farther afield such as New Zealand.
Incremental Haemodialysis in NHS Highland is a great example of the practice of Realistic Medicine to deliver Value Based Health and Care with benefits for people, our healthcare system and the environment.
Varicose Veins: Analysing Variation to Reduce Waste and Harm
Realistic Medicine aims to reduce unwarranted variation in health and care practices, particularly where variation cannot be explained by clinical, or population need. Unwarranted variation may indicate over – or under-treatment, potentially leading to harm and inefficient use of resources. In NHS Lothian, an analysis of procedures for varicose veins in February 2024 revealed an unusually high number of surgeries being performed compared to other Scottish Health Boards, even after adjusting for population size. Varicose veins surgery is considered a Procedure of Limited Clinical Value (PLCV) in NHS Scotland, with strict national referral criteria designed to ensure appropriate treatment.
This Realistic Medicine project focused on investigating the referral and triage processes to identify any unnecessary or inappropriate variation. The aim was to ensure that only people who meet the national referral criteria for varicose veins surgery receive treatment, reducing both potential harm and waste.
The Realistic Medicine team conducted a review of 93 varicose veins referrals over an eight-week period in 2024. The findings revealed that 25% (n=24) of the referrals did not meet the established national criteria for treatment. Of those 25%, 33% were appropriately excluded during the triage process. However, 66% (n=16) of referrals that did not meet the NHS Scotland criteria were still seen in outpatient clinics. Of those not meeting the national criteria seen in outpatient clinics, 33% (n=8) underwent an ultrasound, and 25% (n=6) were listed for surgery.
These results suggested that the referral criteria were not being consistently applied, potentially resulting in unnecessary surgeries and inefficient use of NHS resources. It could also present risks to patient safety by exposing people to unnecessary procedures.
To address this unwarranted variation and improve the referral and triage process, several key actions were initiated:
- Collaboration with Patient Expert Group – NHS Lothian’s Realistic Medicine Patient Expert Group collaborated to create patient-facing information on Varicose Veins. This was designed to support people who did not meet the referral criteria in managing their condition without requiring a specialist referral. The information aimed to help people self-manage, empowering them to make informed decisions about their care.
- Automation of Referral Process – to streamline the triage process and reduce the administrative burden on consultants, NHS Lothian automated the process of returning inappropriate referrals to GPs at the triage stage within the Trak system. This allowed consultants to focus more on clinical decision making rather than administrative tasks.
- Vascular Team Education – the vascular team was tasked with delivering a RefTalk to primary care professionals in November 2024. This session focused on reinforcing the importance of adhering to national referral criteria fairly and equitably for all patients, ensuring that only those who met the necessary criteria were referred for specialist care.
To assess the effectiveness of the actions taken, a follow-up review of referrals and triaging was carried out in February 2025. This review showed an improvement (9%) in the number of referrals not meeting national criteria being rejected at triaging stage and an 8% reduction in the number being seen in clinic. These patients will continue to be followed to determine if they go on to receive ultrasound or treatment.
Total Varicose Vein Referrals |
Referrals not meeting criteria |
Referrals not meeting criteria removed at triaging |
Referrals not meeting criteria seen in clinic |
Referrals not meeting criteria receiving ultrasound |
Referrals not meeting criteria receiving surgery |
|
|---|---|---|---|---|---|---|
Baseline |
93 |
25% (n=24) |
33% (n=8) |
66% (n=16) |
33% (n=8) |
25% (n=6) |
Follow-up |
53 |
23% (n=12) |
42% (n=5) |
58% (n=7) |
Not available yet |
Not available yet |
The investigation into the referral and triaging practices for varicose veins surgery in NHS Lothian highlighted significant variation in how the national criteria was being applied. By collaborating with patient groups, automating administrative processes, and educating primary care providers, the Realistic Medicine team aimed to reduce unnecessary referrals and ensure a fairer, more efficient system.
Hospital @ Home in NHS Shetland
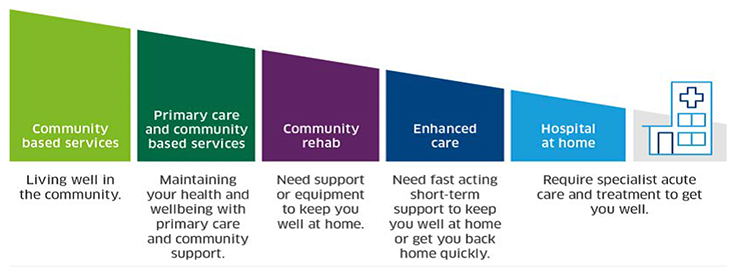
Hospital at Home (H@H) provides urgent short-term hospital level care in people’s homes. H@H care may be provided from one day to several weeks–time which would otherwise be spent in hospital.
In June 2023, NHS Shetland applied to be part of the Hospital at Home (H@H) expansion programme to develop, test and refine a local H@H service. H@H has been shown to be a safe, personalised alternative to hospital admission where care is delivered by a multi-disciplinary team across the community they serve.
Figure 3. Definition of Hospital at Home
The H@H pilot launched in NHS Shetland in September 2023, beginning with the formation of a dedicated multi-disciplinary team that met regularly to coordinate care efforts.
A key priority for the H@H team was to develop locally appropriate processes to facilitate integration between Primary and Secondary Care, including accessible patient notes, prescribing, onward referrals, the establishment of a virtual ward, and data collection for evaluation. The ultimate goal was to design a sustainable H@H model suited to Shetland’s unique health and care needs.
The first stage of the pilot demonstrated that delivering H@H services in Shetland was feasible and welcomed by people, and the foundations were established to look to expand this further. However, it was evident that there was a need to recruit staffing specific to H@H to allow for this further expansion. This was evidenced when staff unavailability in June / July 2024 led to no patients being treated.
Figure 4.
Recruitment of dedicated H@H staff included:
- Consultant Geriatrician
- Band 7 Team Leader
- Band 6 Nurse
- Band 7 Pharmacist
- Band 7 Physiotherapist
This team expansion allowed for the pilot to include referrals from primary care services and admission avoidance from the Emergency Department, a dedicated Pharmacist facilitated test of Hospital Electronic Prescribing and Medicines Administration (HEPMA) system for prescribing, pharmacy oversight and a new process for generating timely discharge letters.
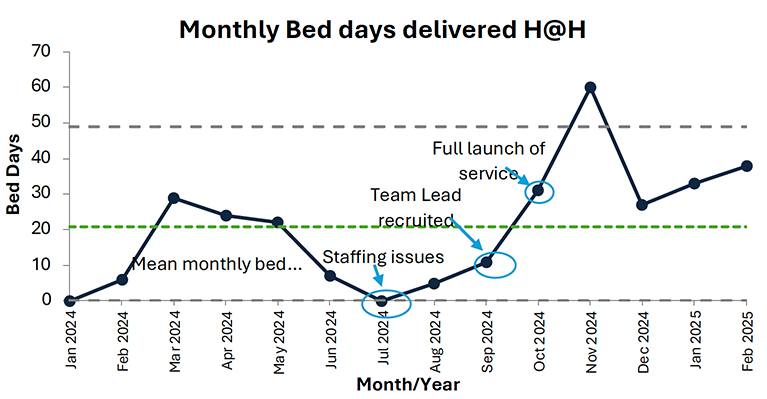
The recruitment of dedicated staff and expansion of referral routes has led to an increase in patient referrals and bed days delivered by the team. The month of November peaked at 60 bed days demonstrating the potential of the service.
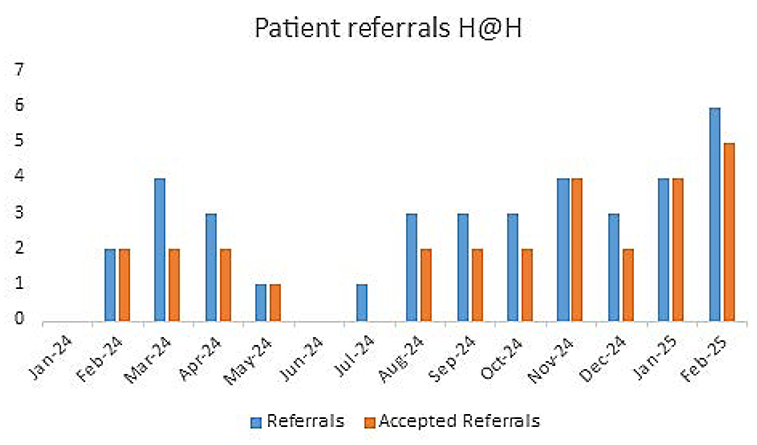
Between January 2024 and end-February 2025, a total of 293 H@H bed days were delivered, with an average length of stay at home of seven days. Referral acceptance was influenced by factors such as staffing availability and individuals’ suitability for the H@H service.
Figure 5.
Figure 6.
H@H is Realistic Medicine in action. It promotes a personalised approach to care. By listening to what matters to the people we care for and those closest to them, we now have clear referral pathways that have been developed and are continuously improving and refining processes.
H@H also improves risk management and ensures timely, appropriate care in the right place for the people in our care. Furthermore, the emphasis on shared decision making empowers people, the H@H team and the health and care professionals to collaborate and support the people we care for to choose the care that is right for them. Through these efforts, the H@H service is not only achieving the outcomes that matter to people, but also fostering a more sustainable health and care system by ensuring those who don’t want or do not need to go to hospital are cared for at home.
"I have nothing but praise for this service and the care and attention I received. Spending long periods in hospital can get on top of you at times but H@H made it possible to be treated and recover in my own home environment among my family and friends, and for that I am extremely grateful to H@H for giving me that opportunity"
"From a colleague perspective I found the whole process slick and brilliant for patients. Thank you for setting this up. I hope it can be rolled out to patients in rural areas too!"
"I’m just so grateful that you were here to help."
"[The H@H team] has removed the burden of having to co-ordinate getting investigations completed and supported us in safely avoiding another admission."
"I’m immensely grateful to the H@H team for supporting me in getting my partner home and supporting us in keeping them at home."
Ongoing efforts focus on expanding the roles of Allied Health Professionals (AHPs) and pharmacy staff within the H@H service, particularly in relation to frailty care. Additionally, work is underway to establish a clear referral pathway from the Scottish Ambulance Service (SAS) to H@H, ensuring seamless patient transitions. Continuous testing and refinement of processes remain a priority to improve service efficiency, with a focus on delivering care that people really value.
Enhancing Blood Management Accuracy: A Value Based Health and Care Improvement Initiative
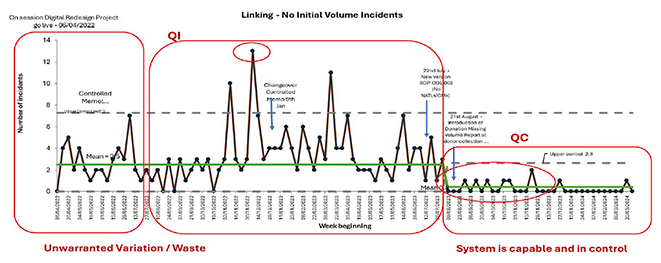
During the implementation of a redesign project within blood collection services, an issue emerged regarding discrepancies between the recorded and actual donation volumes. The new process introduced unwarranted variation, resulting in 4-13 incorrect blood volume recordings per week.
Incorrect or incomplete blood volume recordings led to downstream waste, including rework and additional low-value tasks such as raising support calls with the duty manager, digital and security teams and quality assurance teams, who then had to investigate individual incidents. Additionally, these errors delayed the processing of donated blood, which, in some cases, led to breaches in time-sensitive limits. This, in turn, reduced the availability of certain blood products for hospitals and the people we care for. In extreme cases, these disruptions impacted overall blood product supply and availability.
To address this, a comprehensive evaluation of the donation volume linking process was conducted, focusing on system integration and internal quality control.
Key actions included:
- Quantitative Analysis – tracking the number of process incidents per week using Statistical Process Control (SPC) charts to identify and monitor process variations.
- Qualitative Assessment – gathering insights from incident meetings and improvement forums to assess staff satisfaction and process improvements.
- Technical Process Enhancements – implementing changes to the system linking donation volumes, ensuring errors were minimised and process stability was achieved.
The improvements led to an 86% reduction in donation volume errors, decreasing from an average of seven errors per week to just one error per week.
Figure 7.
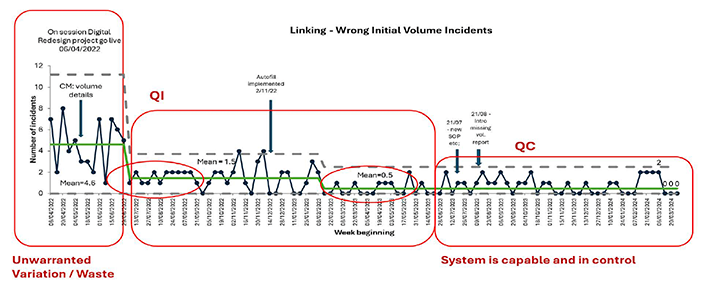
Figure 8.
The system transitioned from one of inconsistency and waste (low value) to a controlled and efficient process, enhancing the value of health and care delivery by:
- reducing unnecessary investigations and administrative burden.
- preventing delays in blood product processing.
- ensuring timely availability of critical blood products.
The sustained success of these improvements was validated through SPC evidence, leading to formal approval from Scottish National Blood Transfusion Service Clinical Governance and Safety in the summer of 2024 to discontinue continuous monitoring—demonstrating that the solution remains effective without ongoing intervention. This approach is providing better value care for our system and the people we care for.
Lido caine 5% Medicated Plasters
The Scottish Government: Achieving Value and Sustainability in Prescribing guideline states that lidocaine 5% medicated plasters have been identified as a medicine of limited clinical value. These items should only be prescribed for an exception named in the guidance, or if no other item or intervention is clinically appropriate or available. Exceptions stated for lidocaine are:
- prescribe to individuals who have been treated in line with SMC guidance and are still experiencing neuropathic pain associated with previous herpes zoster infection (post-herpetic neuralgia, PHN).
- where the decision to prescribe is in line with the Scottish Palliative Care guideline.
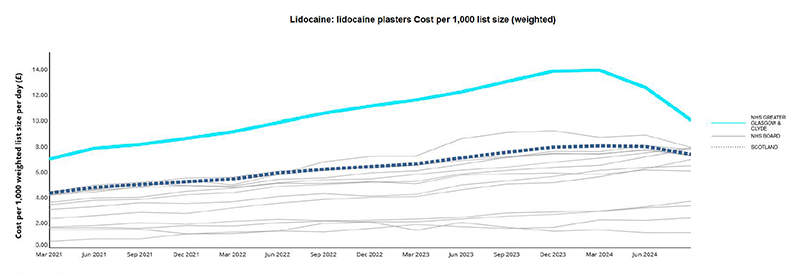
In May 2024, NHS Greater Glasgow and Clyde’s prescribing rate of lidocaine plasters was more than double the rest of Scotland and more than 20 times the rate in NHS England, suggesting unwarranted variation in their use. The cost of lidocaine 5% medicated plaster in NHS Greater Glasgow and Clyde had more than doubled from March 2018 to March 2022. This was higher than any other health board in Scotland.
Key Actions
Following the creation of a Scottish Government short life working group focused on achieving value and sustainability in prescribing, NHS Greater Glasgow and Clyde wrote to all prescribers in May 2024 and October 2024. These letters from medical, nursing and pharmacy leads highlighted the variation in prescribing of lidocaine plasters and asked clinicians in primary and secondary care to review their prescribing practice.
A Prescribing Indicator Implementation Guide was produced focused on review of people prescribed lidocaine 5% medicated plasters with the support of the GGC Chronic Pain Managed Clinical Network (MCN).
The aim was to review everyone who had been prescribed lidocaine 700mg (5% w/w) medicated plasters for more than six months, with a view to stopping use where inappropriate or reducing prescription quantities and/or switching to the most cost-effective plaster.
A 5-step approach was used:
- Stage 1 – Planned Work Discussion – discuss and agree a plan with the GP practice. Explain the aim and process of the review, gain support from all prescribers and reduce inappropriate initiation of lidocaine 5% medicated plasters.
- Stage 2 – Run Search / Data Collection – to identify people using lidocaine 5% medicated plasters.
- Stage 3 – Review – screen list and agree which people were eligible to include. This allows prescribers in the practice to use their clinical discretion and exclude a person who may not fit the above criteria on clinical grounds.
- Stage 4 – Actions - lidocaine plasters not ordered in the last three months were inactivated from repeat prescribing. People who had been using them for more than six months were advised to trial stopping their lidocaine patch by letter or text message and offered a conversation with the practice pharmacist.
- Stage 5 – Face-to-Face Review and Further Actions – all people continuing therapy with lidocaine 5% medicated plasters were switched to the most cost-effective preparation. Facilitated education with prescribers was encouraged to reduce inappropriate initiation of lidocaine.
The Prescribing Indicator Implementation Guide was included to support staff with implementation of reviews and to ensure a personalised approach was taken. This contained:
- a facilitation guide;
- sample GP Practice Protocol for Medication Review and Initiation in Primary Care;
- lidocaine Plaster Monitoring Form;
- example patient letters;
- patient Consultation Aid for trial stops of lidocaine;
- considerations for older people and care home patients.
Further considerations
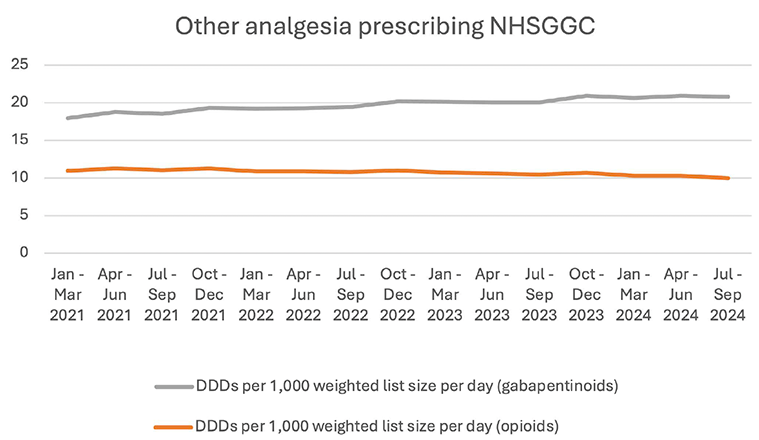
Reducing prescribing of lidocaine used for pain conditions outside of the licenced indication can reduce inappropriate prescribing where there is a lack of evidence for their clinical effectiveness. The potential for increased demand for alternative analgesia or high-risk medication such as opioids or gabapentinoids was assessed using data from the National Therapeutic Indicators (NTIs), where no significant increase in prescribing was identified (see Figure 10). There was also no corresponding increase identified in people receiving high dose opioids (>50mg Morphine Equivalent Dosing) or high dose gabapentinoids (dosing equivalent to >3600mg gabapentin) during that period.
Figure 9: DDDs per 1,000 list size (weighted) per day for opioids and gabapentinoids
Outcomes
Following the review to improve the appropriateness of lidocaine plaster prescribing there has been a reduction in the number of lidocaine 5% plasters prescribed. This has led to a reduction in prescribing variation, improved appropriateness of prescribing in line with national guidance and allowed individuals the opportunity to have a holistic pain review with the practice pharmacist. There was a 28% reduction in cost from March 2024 to October 2024 (see figure 10) with further improvements expected as additional practices engage with the work.
Figure 10: Lidocaine plaster costs per 1,000 list size (weighted)
Five-Day Antibiotic Treatment Courses for Respiratory Tract Infections
Antimicrobial resistance (AMR) is a natural consequence of using antibiotics, but overuse and inappropriate use can increase the likelihood of adverse events and unnecessarily increase the rate of antimicrobial resistance. The link between antimicrobials and Value Based Health and Care was recently highlighted in Achieving Value and Sustainability in Prescribing.
The scale of the threat of AMR and the case for action is set out in the UK AMR Action plan: Confronting antimicrobial resistance 2024 to 2029. This follows on from the previous UK publication 20-year vision for antimicrobial resistance, which set the ambitious goal of ensuring AMR will be controlled and contained by 2040, and the first five-year national action plan for antimicrobial resistance, ‘Tackling antimicrobial resistance 2019 to 2024’.
An important element of antibiotic stewardship is making sure that when antibiotics are clinically indicated, they are not used for longer than required, with advice to people to “complete the full course”. Respiratory infections are the main infection related consultation in NHS Scotland and the most common reason for antibiotics prescribed in the community. Where prescribing is indicated, guidance recommends an initial five-day antibiotic treatment course for community acquired pneumonia.
Key Actions
The Scottish Antimicrobial Prescribing Group (SAPG) promotes the safe and effective use of antibiotics across hospital and community settings to improve antibiotic stewardship and tackle the risks of antimicrobial resistance. They are supporting reduced courses of respiratory antibiotics in a number of ways:
1. Targets
The UK AMR Action plan has a target to reduce total antibiotic use in human populations by 5% by 2029 from the 2019 baseline. SAPG have developed a supplementary target - By 2029, 90% of prescriptions of amoxicillin and 60% for doxycycline will be for a 5-day course. This will allow benchmarking at board and practice level, identifying areas that may need support to improve their prescribing of respiratory antibiotics.
2. Guidelines
SAPG supports local empirical prescribing policies which include a clear duration of five days’ treatment for community acquired pneumonia. Scottish Government worked with SAPG to develop an antimicrobial resistance section within the recent national publication Achieving Value and Sustainability in Prescribing.
3. Update of the default dosing and duration in General Practice IT system (Vision)
SAPG’s website hosts step by step instructions to change the default dose and duration of medications within our clinical system, making it easier for prescribers to select the correct duration of respiratory antibiotics.
4. QI work
SAPG have developed a range of interventions to support the reduction of unnecessary use of antibiotics for self-limiting respiratory tract infections, including a national audit tool for primary care management of commonly encountered infections.
The audit tool is intended to provide prescribers with qualitative information on their prescribing of antibiotics. This information complements existing quantitative information available via the Prescribing Information System for Scotland (PRISMS). It is intended to facilitate reflective learning on the use of antibiotics. The results allow prescribers to compare their own prescribing decisions with local guidance and support identification of areas for quality improvement.
Outcomes
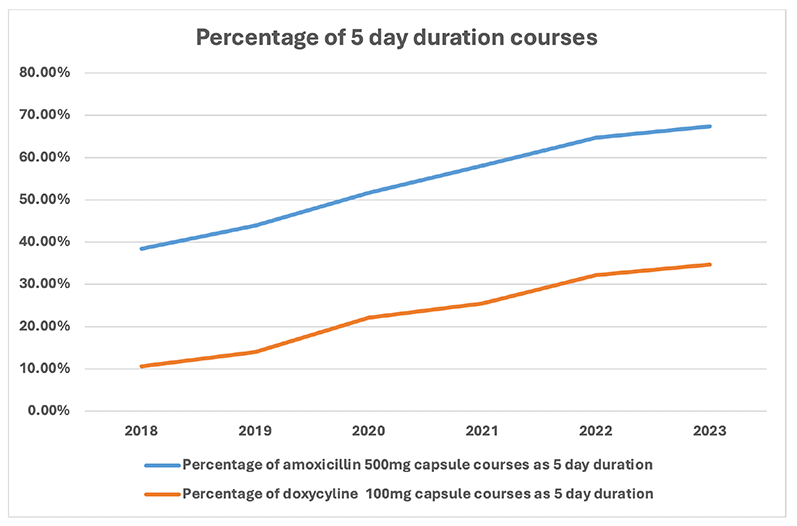
The yearly Scottish One Health Antimicrobial Use and Antimicrobial Resistance (SONAAR) reports show there has been a year on year increase in 5-day courses of amoxicillin and doxycycline (see Figure 11 and Figure 12 below). Improvements have been particularly notable in NHS Boards which have embedded 5-day prompts within electronic prescribing platforms. Unification of prescribing platforms and better use of clinical decision support will be crucial to reduce unwarranted variation, as well as helping to address other important prescribing targets.
Appropriate use of antibiotics is helping to reduce unwarranted variation in prescribing, reduce the impact of antibiotics on our planet and maximise the value of healthcare, achieving better outcomes for people and contributing to a more sustainable health and care system.
Figure 11: Percentage of amoxicillin 500mg capsule courses and doxycycline 100mg capsule courses prescribed as 5-day duration in Primary Care
Year |
Percentage of amoxicillin 500mg capsule courses as 5-day duration |
Percentage of doxycyline 100mg capsule courses as 5-day duration |
|---|---|---|
2023 |
67.40% |
34.70% |
2022 |
64.70% |
32.20% |
2021 |
58.10% |
25.50% |
2020 |
51.70% |
22.10% |
2019 |
43.90% |
14.00% |
2018 |
38.40% |
10.60% |
Improving Asthma Outcomes and Reducing Environmental Impact of Asthma Treatments: Addressing Short-Acting Beta Agonists (SABA) Over-Reliance, and Optimising Asthma Care
The Quality Prescribing Strategy for Respiratory: A Guide for Improvement 2024-2027 and the BTS/NICE/SIGN guideline Asthma: diagnosis, monitoring and chronic asthma management provide recommendations on optimising asthma care, recognise the importance of reducing the over-reliance on short-acting beta 2 agonists (SABA) in asthma care and reducing the environmental impact of inhalers.
Over-reliance on SABA inhalers is an indicator of poor asthma control. Use of more than three of these inhalers per year is associated with an increase in asthma exacerbation rates and healthcare utilisation. The level of SABA use in the UK is amongst the highest in Europe with 38% of asthma patients potentially over-reliant on SABA inhalers.
One SABA, salbutamol, accounts for two thirds of the total carbon footprint from pressurised metered-dose inhalers (pMDIs). These contain hydrofluorocarbon propellants which are potent greenhouse gases and alone account for 22% of the primary care carbon footprint. Dry-powder inhalers (DPI) or soft mist inhalers (SMI) do not contain propellant gases and are more climate friendly. In addition, well-controlled asthma, using appropriate treatment such as inhaled corticosteroids, has a third of the carbon footprint of poorly-controlled asthma. Therefore, a holistic review optimising asthma management, and reducing SABA over-reliance, will improve asthma outcomes for people and reduce the environmental impact of treating asthma.
The NHS Greater Glasgow and Clyde (NHSGGC) Clinical Sustainability and Primary Care Climate Change Group identified eighteen “early adopter” GP practices who agreed to undertake Quality Improvement work around sustainable respiratory care. A Greener Respiratory Care Quality Improvement tool was used in many practices to collate data and outcomes. The aim was to improve asthma care and outcomes whilst reducing the environmental impact of asthma treatments by addressing SABA over-reliance.
Practices undertook to complete facilitated education regarding Greener Respiratory Care and identify a cohort of patients who had been dispensed six or more SABA inhalers per year. They planned a holistic clinical review of each person’s respiratory long-term needs, optimised asthma treatment and considered, where appropriate, a lower global warming potential inhaler. Greener disposal of inhalers was encouraged by returning them to community pharmacies for disposal.
Results
There has been a reduction in the number of people prescribed six or more SABA inhalers per annum as a percentage of all people prescribed SABAs from 27.99% in October 2021 to September 2022 to 24.16% in October 2023 to September 2024.
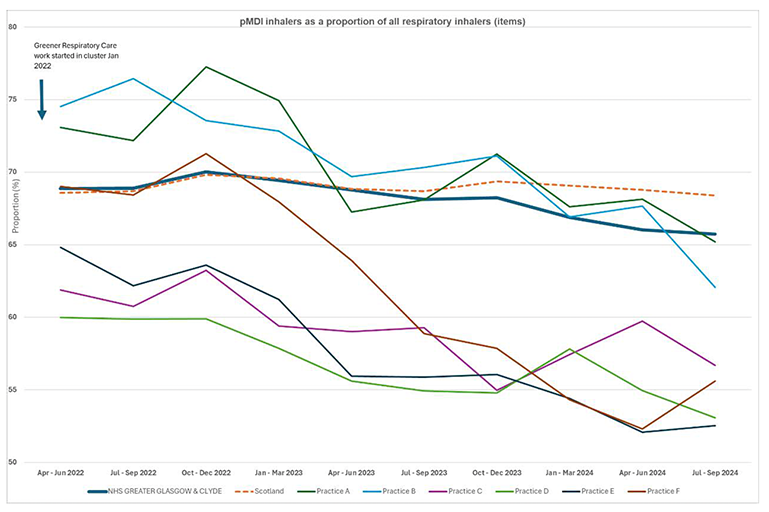
There has also been a reduction in pMDIs as a proportion of all inhalers in all of the practices in NW cluster A, as shown in Figure 13 below. (Data accessible via National Therapeutic Indicators.)
The graphs below show the impact of the work for practices in one primary care quality cluster (NW- A), comprising some of the first GP practices to undertake this project. The first practice started the Greener Respiratory Care (GRC) work in January 2022.
Figure 13.
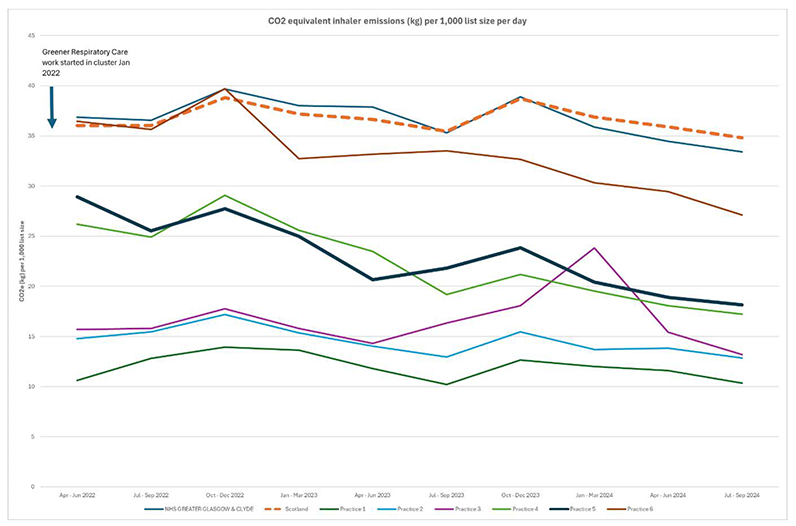
The reduction in pMDI prescribing has led to a reduction in the carbon dioxide equivalent inhaler emissions for all practices in NW cluster A, as shown in Figure 14 below (National Therapeutic Indicators).
Figure 14.
The impact of this initiative on the cost of inhalers was also assessed, looking at prescribing costs and volume of bronchodilator metered dose inhalers (MDIs) and dry-powder inhalers (DPIs) in GP practices. There was a larger proportional decrease in the number of people prescribed more than six SABA inhalers per annum in the early adopter practices compared to other practices (Table 1).
Patient Count |
Bronchodilator Inhalers >6 |
|
|---|---|---|
NHSGGCEarly Adopter Practices |
Jun20-May21 |
2,349 |
Jun23-May24 |
1,836 |
|
Shift |
-513 (-27.9%) |
|
Other Practices |
Jun20-May21 |
39,124 |
Jun23-May24 |
33,620 |
|
Shift |
-5504 (-16.4%) |
|
The overall impact on cost for the early adopter practices was neutral, see Table 2.
Sum of Paid Gross Cost |
Early Adopter Practices |
Early Adopter Practices |
Early Adopter Practices Total |
Other Practices |
Other Practices |
Other Practices Total |
|---|---|---|---|---|---|---|
DPI |
MDI |
DPI |
MDI |
|||
Jun20-May23 |
£23,843 |
£61,544 |
£85,388 |
£401,363 |
£1,066,354 |
£1,467,717 |
Jun23-May24 |
£35,145 |
£50,515 |
£85,661 |
£480,146 |
£1,044,207 |
£1,524,354 |
Shift |
£11,302 |
-£11,029 |
£273 |
£78,783 |
-£22,147 |
£56,636 |
Overuse of SABA inhalers indicates poor asthma control and has a negative impact on the environment. Early adopter GP practices reduced reliance on these inhalers improving care, increasing the proportion of more environmentally friendly inhalers and reducing the carbon emissions attributed to inhalers. These changes achieved cost effective asthma care which is better for people and the planet.
Contact
Email: realisticmedicine@gov.scot