Population Health Framework: evidence paper
This report accompanies the Population Health Framework (PHF). It provides an overview of evidence on population health in Scotland, highlighting key challenges and opportunities for improvement. It also includes a technical note on the development of the PHF aim.
2. Setting the scene: population health in Scotland
This section provides an overview of population health in Scotland. It begins by explaining how population health is defined and understood, before describing the drivers which underpin the PHF. It then summarises recent trends in Scotland’s population health and considers evidence on the factors which have contributed to these, before setting out future projections.
Key points
- The strongest influences on health are the conditions in which people are born, grow, work, live and age. These are collectively known as the social (or wider) determinants of health, and include social, cultural, political, economic, commercial, and environmental factors.
- After decades of improvement, Scotland’s health is worsening. Since around 2012, mortality improvements have stalled, death rates have risen among the most deprived communities, and health inequalities have widened. Scotland’s life expectancy is the lowest of all UK countries and remains the lowest in Western Europe.
- A strong body of evidence has identified the implementation of UK Government austerity policies during the 2010s as one of the principal drivers of these trends.
- Beyond austerity, Scotland has longstanding inequalities in income, wealth, and power, known as the ‘fundamental causes’ of health inequalities.
- There has also been limited progress across several key social determinants of health in recent years, such as housing, education, and employment.
- These factors, along with the impact of the Covid-19 pandemic, Brexit, and the cost-of-living crisis, provide further context for Scotland’s stalling health improvements.
- Analyses project a 21% increase in the overall burden of disease in Scotland over the next 20 years. While such a rise would have significant implications for public health and the health and social care system, it is not inevitable. Effective policies and interventions have the potential to alter trends and improve health outcomes.
2.1. Understanding population health
Key definitions
The World Health Organisation (WHO) (1948: p1) defines health as “a state of complete physical, mental and social wellbeing and not merely the absence of disease or infirmity”. This highlights that health includes physical, social and emotional wellness rather than simply the absence of ill health.
Population health is a broader concept that considers the health of an entire population, and how social, economic, biological, and environmental factors influence that health. While there is no single accepted definition of population health, it can be usefully defined as “the health outcomes of a group of individuals, including the distribution of such outcomes within the group” (Kindig and Stoddart, 2003: p381).
Health inequalities are defined by McCartney et al. (2019: p28) as “systematic, avoidable and unfair differences in health outcomes that can be observed between populations, between social groups within the same population or as a gradient across a population ranked by social position”.
Health equity is defined by WHO (2025a) as “the absence of unfair and avoidable or remediable differences in health among population groups defined socially, economically, demographically or geographically”.
The King’s Fund defines a ‘population health approach’ as:
“An approach aimed at improving the health of an entire population. It is about improving the physical and mental health outcomes and wellbeing of people within and across a defined local, regional or national population, while reducing health inequalities. It includes action to reduce the occurrence of ill health, action to deliver appropriate health and care services and action on the wider determinants of health. It requires working with communities and partner agencies” (Buck et al., 2018: p18).
This definition, which is adopted in the PHF, focuses on the health of the broader population rather than the health of individuals. It highlights the importance of both physical and mental health and wellbeing, while emphasising the need to reduce inequalities in health as well as improve health overall. It also recognises that achieving improvements in population health requires input from a wide range of sectors and organisations, such as national and local government, the third sector, business, communities, and political leaders (Holmes, 2022).
Models of population health
Health is shaped by a wide range of complex and interconnected factors, including the physical, social, cultural, commercial, and economic environment, alongside individual characteristics and behaviours, which are influenced by wider structural conditions (WHO, 2024a). Recognising this complexity, different models have been developed to help explain the various factors that determine a population’s health, the connections between these, and where action is needed to improve population health.
The King’s Fund framework for population health (Buck et al., 2018) centres on four interlinked pillars:
- The wider determinants of health, which include factors such as income, education, housing, and transport.
- Health behaviours, and the contexts that produce them. These include, for example, smoking, alcohol consumption, diet, and physical activity. The wider determinants of health, as well as commercial influences, play a significant role in shaping these factors.
- The places and communities we live in and with, such as our local environment, community networks, and social relationships.
- An integrated health and care system, viewed as essential for meeting the growing demand for complex and longer-term care.
Models have also been developed that specifically focus on addressing health inequalities. In 2010, Sir Michael Marmot chaired an independent review aimed at identifying the most effective, evidence-based strategies to reduce health inequalities in England. The resulting report (Marmot, 2010) outlined six key policy objectives to reduce health inequalities, with a further two added in 2022 (Marmot, 2022). These are described as the Marmot Eight principles (Institute of Health Equity (IHE), 2025):
1. Give every child the best start in life.
2. Enable all children, young people and adults to maximise their capabilities and have control over their lives.
3. Create fair employment and good work for all.
4. Ensure a healthy standard of living for all.
5. Create and develop healthy and sustainable places and communities.
6. Strengthen the role and impact of ill health prevention.
7. Tackle discrimination, racism and their outcomes.
8. Pursue environmental sustainability and health equity together.
Central to both the King’s Fund model and Marmot Eight principles is the recognition that health is shaped by factors that extend beyond how the health service is funded and functions, or genetics and behaviours. Rather, health is intrinsically linked to the circumstances and environments in which people are born, grow, live, work, and age, such as our childhood experiences, employment, housing, education, and social networks. These are collectively known as the social (or wider) determinants of health (Dahlgren and Whitehead, 1991; Marmot, 2010; WHO, 2010a). In the PHF, these are referred to as the ‘building blocks’ of health.
Research shows that the social determinants have a greater impact on population health than healthcare or individual behaviours (WHO, 2010a; Buck et al., 2018). While precise measurement is challenging, studies examining the factors influencing health have broadly indicated that social, economic, and environmental factors are the primary driver of health (50% collectively), followed by health behaviours (30%), and health services (20%) (e.g. McGinnis et al., 2002; Booske et al., 2014; Bunker et al., 1995). The relative impact of each of these factors is illustrated in Figure 1.
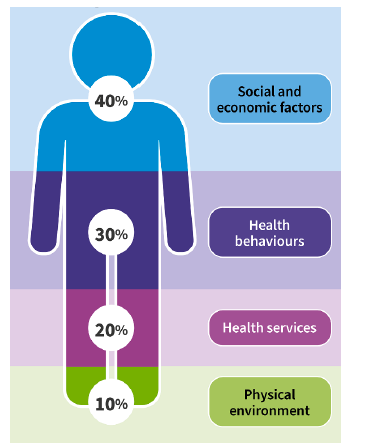
Source: PHS (2024a)
Also key to understanding population health is the unequal distribution of income, power, and wealth between groups in society, which is caused by political, economic, and social decisions and priorities (Tweed et al., 2017). Inequalities in income, power, and wealth are widely recognised as the ‘fundamental causes’ of health inequalities (Link and Phelan, 1995). These fundamental causes result in inequalities in the social determinants of health described above, leading different groups to experience different levels of physical and mental health, illness, and death (Tweed et al., 2017).
The Population Health Framework drivers
The PHF has been structured around four overlapping drivers of health and wellbeing (Figure 2). These drivers align with the King’s Fund population health pillars and link to the Marmot Eight principles:
- Social and Economic Factors – Improve the social and economic factors that support better health and reduce inequalities.
- Places and Communities – Create healthy and sustainable places by working in and with communities.
- Enabling Healthy Living – Develop supportive environments that promote health and wellbeing and reduce health harming activities.
- Equitable Health and Care – Foster a health and social care system that delivers equity, prevention and early intervention.
A fifth overarching driver considers ‘how’ the system needs to change to bring greater focus to population health and support a shift to a more prevention-based system through coordinated activities across all drivers:
- Prevention Focused System – Strengthen collective accountability for population health outcomes and inequalities.

2.2. The current status of Scotland’s health
Recent evidence has highlighted concerning shifts in the health of Scotland’s population, including stalled improvements in mortality, worsening health outcomes, and widening inequalities (Miall et al., 2022). Several reports have set out these trends and explored inequalities in detail (McCartney et al., 2022; Walsh and McCartney, 2023; Finch et al., 2023; Miall et al., 2022; Catalano, 2024). This section draws on these reports, as well as more up-to-date data, to present a summary of the current status of Scotland’s health.
Trends in mortality and health outcomes
In 2022, Glasgow Centre for Population Health (GCPH) published a report which set out changes that had been seen in population health in Scotland and across the UK since around 2012 (McCartney et al., 2022). An update to this report was published in 2023 (Walsh and McCartney, 2023). These reports focus on mortality rates and other related indicators, such as life expectancy[1], as key markers of a population’s overall health.
McCartney et al. (2022) outline that with a few notable exceptions (for example, during periods of war or pandemic) mortality rates in high-income countries had been improving since the mid-nineteenth century, reflecting improvements in living and working conditions, public health interventions, and medical advances. However, around 2012-2014[2] these improvements stalled in many countries, including all the UK nations. By 2018, life expectancy in the UK was significantly lower than what would have been expected if the improving trends seen from 1990 to 2011 had continued. In Scotland, this resulted in life expectancy being 1.3 years lower for females and 1.4 years lower for males than anticipated.
More recent data show that life expectancy fell further over the course of the Covid-19 pandemic. While between 2020-2022 and 2021-2023 life expectancy increased by 4.8 weeks for females and 12.8 weeks for males, it remains below the pre-pandemic years at 80.8 years for females and 76.8 years for males (National Records of Scotland (NRS), 2024a; Figure 3). However, 2023 figures are likely to align more closely with pre-pandemic trends.
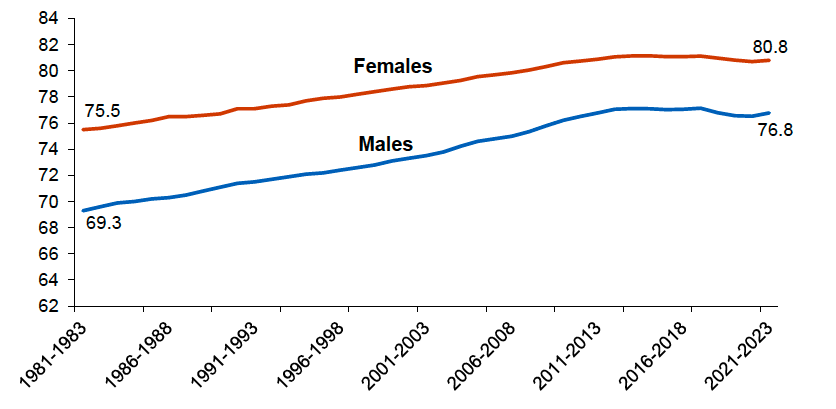
Source: NRS (2024a)
Healthy life expectancy (HLE)[3] has also declined in Scotland. Analysis by Walsh et al. (2022) showed a striking fall in HLE, with a drop of around two years of HLE observed between 2011 and 2019. This trend was also mirrored for the UK overall, where there was a marked decline in HLE between 2013-2015 and 2017-2019. In 2019-2021, healthy life expectancy at birth was 60.4 (± 0.5*) years for males and 61.1(± 0.6) years for females in Scotland (NRS, 2022; Figure 4)[4].
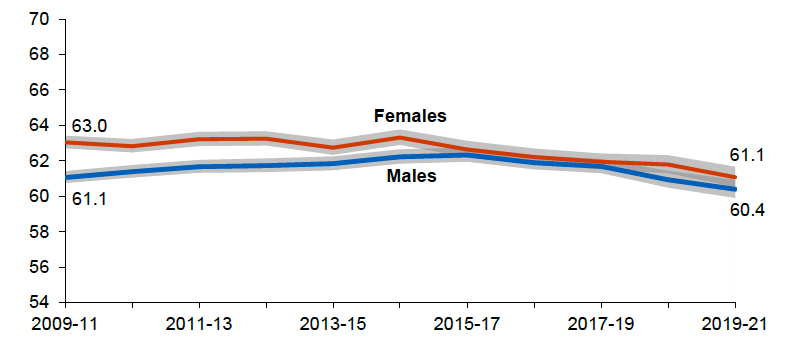
Source: NRS (2022)
Trends in mental health are also important to consider. McCartney et al. (2022) note that while trends in mental health outcomes are less clear, there is some evidence that mental health problems, particularly among younger adults, worsened between 2015 and 2019 in Scotland and England. This trend was also evident in research conducted by Zhang et al. (2023), which found that psychological distress worsened among working-age adults in Scotland, England and Great Britain as a whole between 2015 and 2019. They state that their findings indicate “a widespread mental health crisis that predates the Covid-19 pandemic” (ibid.: 468).
Scotland’s Census (2024) found that the percentage of people reporting a mental health condition increased from 4.4% in 2011 to 11.3% in 2022. This increase was largely driven by a significant rise among younger individuals, with the largest increase seen in the 16 to 24 age group. In 2022, 15.4% of those aged 16 to 24 reported a mental health condition, up from 2.5% in 2011.
The Scottish Health Survey (SHeS)[6] measures mental wellbeing using the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS), with higher scores indicating greater wellbeing. The most recent data show that while average levels of mental wellbeing for adults increased to 48.9 in 2023 from 47.0 in 2022 and 48.6 in 2021, the mean score remains below that typically recorded in pre-pandemic years, which ranged from 49.4-50.0 between 2008 and 2019 (Scottish Government, 2024a). Younger adults also reported lower mental wellbeing than older adults, with mean WEMWBS scores in the range 49.3-50.8 for adults aged 55-74 and 51.9 for those aged 75 and over (ibid.).
Overall, the recent changes in key population health indicators have sparked alarm among public health experts. As stated by McCartney et al. (2022: p12): “This is hugely worrying. Put simply, we should not see such trends in a wealthy society such as the UK”.
Health inequalities
While the rate of improvement in mortality has slowed across all socioeconomic groups in Scotland, the trends have been worst for those living in more deprived areas. This has led to a widening of health inequalities across a range of key measures. The latest data on life expectancy show a gap of 13.2 years for males and 10.5 years for females between the most and least deprived areas in Scotland in 2021-2023, up from 12.2 and 8.6 years in 2013-2015 (NRS 2024a; NRS 2022; Figure 5).
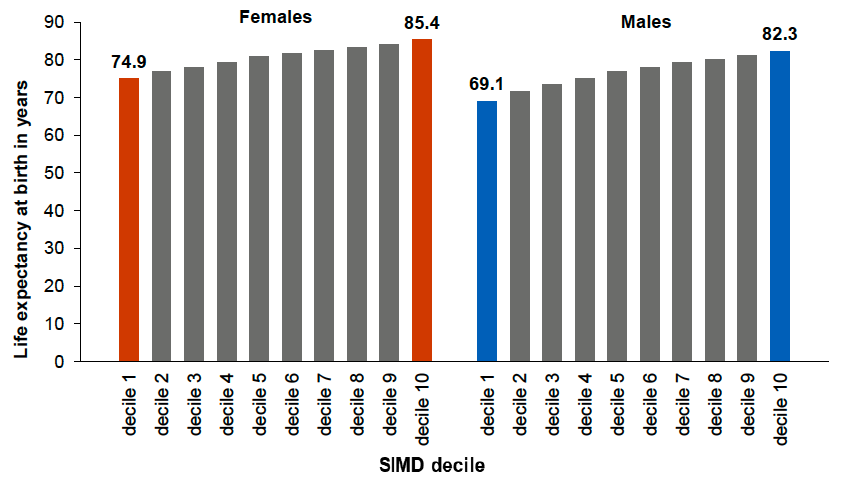
Source: NRS (2024a)
Socioeconomic inequalities in HLE are even starker. Walsh et al. (2022) demonstrate that while overall HLE declined by approximately 2 years between 2011 and 2019, a greater decline (of around 3.5 years) was observed among the most deprived fifths of areas. The most recent NRS (2022) data show that males and females in the most deprived areas are spending more than a third of their life in poor health compared with around 15% in the least deprived areas.
Health inequalities in Scotland have also been recently examined elsewhere, including by researchers at the University of Glasgow as part of a review by the Health Foundation (Miall et al., 2022) and by the Scottish Health Equity Research Unit, which was established in 2024 to provide insights and analysis on the socioeconomic factors that shape health (Catalano et al., 2024). In addition to life expectancy and HLE, these reports consider a range of other indicators of health, and demonstrate that health consistently worsens as deprivation increases, with the most deprived areas experiencing particularly poor outcomes. For example, over the period 2016-2020 those in the most deprived fifth of areas were five times more likely to die from alcohol-specific causes, while in 2023 the rate of drug-related deaths in the most deprived fifth of areas was 15 times as high as that in the least deprived fifth (Miall et al., 2022; Catalano et al., 2024; NRS, 2024b). Miall et al. (2022) also highlight that socioeconomic inequalities emerge early in life, for example in the prevalence of low birthweight, early child developmental concerns and risk of overweight or obesity at the start of school.
The Chief Medical Officer’s (CMO) 2024 Annual Report highlighted the reality of health inequalities in Scotland, stating that: “On average, by the time people in our poorest communities have died, people in our most affluent communities are only just beginning to experience ill-health” (Scottish Government, 2024b: p45).
Comparisons with other countries
Although declines in life expectancy have also been seen elsewhere in the UK and across Europe (Steel et al., 2025), Scotland’s health outcomes lag behind those of the rest of the UK and other Western European nations. Scotland has the lowest life expectancy of the UK nations (Office for National Statistics (ONS), 2024) and a lower HLE than the UK average (NRS, 2022). Life expectancy in Scotland also ranks amongst the lowest in Western Europe (NRS, 2024a). International data show that Scotland has a higher prevalence of largely preventable, non-communicable conditions relative to comparable European countries, as well as the widest socioeconomic inequalities in health in Western Europe (ScotPHO, 2023a).
2.3. What is causing recent trends?
Trends in social and economic factors
The impact of austerity
A changed health trajectory has therefore been identified in Scotland, with the population health improvements of previous decades stalling and then moving into reverse. A strong body of evidence has identified the implementation of UK Government austerity policies during the 2010s as one of the principal drivers of the changes in mortality rates in Scotland and the wider UK (McCartney et al., 2022; Walsh and McCartney, 2023; Finch et al., 2023). As part of these measures, funding for many public services, including health and social care, declined in real terms. While reduced spending on health is likely to have contributed to the stalling of mortality improvements by limiting access to, and the quality of, care for people with acute health needs (Finch et al., 2023), Seaman et al. (2023) argue that the two principal mechanisms through which austerity had adverse effects were cuts to local government spending and social security.
Local government spending was one of the largest areas of budget reduction resulting from the imposition of economic austerity in the 2010s (McCartney et al., 2022). Evidence indicates that cuts to local government spending can adversely affect population health and wellbeing, including negatively affecting mortality and life expectancy, due to local governments’ reduced capacity to fund essential services such as housing, education, leisure, and social care services (Broadbent et al., 2024). Moreover, because local authorities which are more dependent on central government funding are systematically more deprived, cuts to services have disproportionately affected more disadvantaged areas (McCartney et al., 2022).
Austerity policies also resulted in reductions in the real-term value of many social security benefits, as well as increased constraints on their conditionality and eligibility (McCartney et al., 2022). Seaman et al. (2023) examined the relationship between all social security cuts fully implemented by 2016 and life expectancy at the UK local authority level and found that they were associated with lower life expectancy. Other research has shown detrimental effects that social security cuts had on mental health outcomes such as increased prevalence of depression and anxiety (Reeves et al., 2021).
The detrimental impacts of austerity on population health are well-documented not only in Scotland but also across the UK and Europe (Stuckler et al., 2017; Toffolutti and Suhrcke, 2019). For example, drawing on data from across Europe, Stuckler et al. (2017) demonstrate that austerity has had important consequences for health and health services. They highlight that those already vulnerable were most adversely affected, such as those with precarious employment or housing, or with existing health problems. They also note that countries with strong social protection systems, such as Iceland and Germany, fared better than those with weaker social protection systems, such as Greece.
As summarised by GCPH (2024: p5), austerity led to an “adverse and rapidly impactful shift in the pattern of economic and social development determining access to positive determinants of health for key groups in the population”. They also highlight that this policy response has since been compounded by other factors, including Brexit, the Covid-19 pandemic, the war in Ukraine, and the cost-of-living crisis.
This is supported by research conducted by Douglas et al. (2022), who assessed the likely impact of the rising cost of living on health and identified a range of adverse effects on individuals and households through, for example, increased problem debt, food insecurity, fuel poverty, poor housing condition, and mental distress. They stated that while many of these will have adverse impacts on health and health inequalities in the short term, they are also likely to reduce population resilience and increase health inequalities in the longer term. These factors disproportionately affect those already on low incomes, so are likely to further increase inequalities in income, wealth, and health. In line with the significant and growing body of evidence which demonstrates the impact of early life experiences on long-term mental and physical health (WHO, 2020), Douglas et al. (2022) also highlight how the impacts on children and young people, such as potential developmental effects from poor nutrition, cold, damp homes, and potential increases in adverse childhood experiences, could have lifelong effects on their life chances and health.
Inequalities in income, wealth, and power
In addition to the impact of austerity, Scotland has longstanding inequalities in income, wealth, and power – the ‘fundamental causes’ of health inequalities (Link and Phelan, 1995). A substantial body of evidence demonstrates the links between income and health, and wealth and health, respectively. Higher income generally leads to better health, as it gives access to essential resources such as food, quality housing, transport, and leisure opportunities (PHS, 2024b). Similarly, greater wealth – i.e. financial assets amassed over the lifetime – is associated with improved health outcomes (Baciu et al., 2017). Pollack et al. (2013) demonstrate that wealth influences health through mechanisms that are not necessarily monetary, such as power and prestige, attitudes and behaviour, and social capital, in addition to offering resources and a safety net unavailable to those without the same level of financial resilience.
However, central to fundamental cause theory is that income and wealth inequality can negatively affect population health over and above the negative impacts of individuals lacking income and wealth. In other words, greater income and wealth inequality are associated with higher health inequalities, with health worse across the social spectrum in countries with higher income and/or wealth inequality (PHS, 2024b). The process by which the fundamental causes translate into health inequalities at the individual level is shown in Figure 6 below.

Source: Adapted from PHS (2024b)
Fundamental causes
Global economic forces
Macro socio-political environment
Political priorities and decisions
Societal values to equity and fairness
Unequal distribution of income, power and wealth
Poverty, marginalisation, and discrimination
Wider environmental influences
Economic and work
Physical
Learning
Services
Social and cultural
Individual experience
Economic and work
Physical
Learning
Services
Social and interpersonal
Effects
Inequalities in:
Wellbeing
Healthy life expectancy
Morbidity
Mortality
In Scotland, the Gini coefficient for income – a measure of income inequality which ranges from 0 to 1, where 1 stands for total inequality – rose sharply in the 1980s from a low of around 0.25 to around 0.35 (PHS, 2024c). Since then, it has fluctuated at this high level, measuring at 0.32 in 2021-2024 (Scottish Government, 2025a). Importantly, Eiser et al. (2022: piii) highlight that while household inequality across most of the population has remained largely unchanged in recent years, inequality has increased at the upper and lower ends of the distribution, meaning that “the very poorest have become poorer than everyone else, and the very richest have become richer than everyone else”. They also note that income inequality in Scotland is relatively high in an international context, which is a legacy of the large increase seen in the 1980s.
High levels of wealth inequality also exist in Scotland, with the wealthiest 2% of households owning 18% of the total wealth (made up of physical wealth, financial wealth, property wealth, and pension wealth) in 2018-2020 (Scottish Government, 2022a). Eiser et al. (2022) note that, despite a substantial increase in the overall value of wealth held by households over the last 10 years, there is little evidence that its distribution has become more dispersed.
Catalano et al. (2024) also highlight that average household incomes have stagnated in Scotland since the financial crisis, with median incomes around 20% lower in 2019-2022 than they would have been if the pre-financial crisis trend had continued. Further, compared with pre-pandemic levels, average incomes have decreased, both before and after accounting for housing costs. Over the same period, the proportion of households in relative poverty[8] has increased. Catalano et al. (ibid.) outline qualitative research that illustrates how low incomes and poverty negatively affect health and wellbeing through four key interlinked pathways, including material impacts (such as not being able to afford to eat or live in a decent quality home), aspects of the physical environment (such as high air pollution, traffic accidents, and having fewer amenities), experiences of stigma and discrimination, and mental health impacts (such as anxiety and stress).
Wider trends in the social determinants of health
Trends relating to other key determinants of health are also relevant in explaining Scotland’s stalling health improvements. Eiser et al. (2022) examine trends in the social determinants of health in Scotland since 1999 – the year of the establishment of the Scottish parliament – and highlight that there has been little evidence of improvement in several key areas during this period. They state that while it cannot be said that these socioeconomic trends are the sole cause of the concurrent health slowdown, they have ‘undoubtedly’ contributed to the recent stalling in improvements in health.
For example, Eiser et al. (ibid.) explore trends relating to housing. They demonstrate that there has been growth in the share of households in the private rental sector in Scotland in recent years, and that in general, this sector is associated with higher costs and lower quality compared with owner occupation and social housing. They also highlight a clear income gradient with regards to housing quality in Scotland, with lower-income households more likely to live in houses with damp and mould and less likely to be able to keep their home warm in the winter, for instance. Catalano et al. (2024) also outline trends of concern relating to housing, including that fuel poverty and insecurity have increased since 2019, while homelessness applications have risen.
Looking at trends in education, Eiser et al. (2022) note that socioeconomic inequalities in educational attainment in Scotland are high, exist at all levels of education, and have remained persistent over time. They also highlight low levels of intergenerational social mobility in Scotland (a measure of the extent to which people’s education, income or jobs are associated with those of their parents), noting that the occupations that people have as adults are strongly associated with those that their parents had.
Other employment-related trends outlined include the rise in some forms of insecure work in Scotland since 2010, such as zero-hours contracts and low-paid self-employment, and that the poverty risk for families with at least one adult in work has increased since 1999 (ibid.). Trends in employment are also explored by Catalano et al. (2024), who highlight the wide gap in weekly earnings between the highest and lowest-earning full-time workers in Scotland.
These examples demonstrate that in addition to the harmful effects of austerity and long-standing inequalities in income, wealth, and power in Scotland, there has been limited progress in several key social determinants of health in recent years. As Eiser et al. (2022: p149) summarise, the dramatic stagnation of earnings and living standards, combined with the effects of austerity in public services, mean the slowdown in mortality improvement “is less of a puzzle”.
Trends in health harms
Health behaviours, such as smoking, poor diet, physical inactivity, and harmful alcohol use, are leading risk factors that drive preventable ill health and premature mortality in Scotland. Given their importance in shaping population health outcomes, recent trends in a number of health risks and behaviours in Scotland are set out below. It is important to note, however, that each has its root causes in the social determinants of health described above, with people’s exposure to health-harming products and environments, and ability to access healthy options, strongly influenced by their circumstances (Everest et al., 2022). As will be covered further in later sections of this report, evidence shows that addressing these risks and behaviours requires population-based, equity-focused interventions, as opposed to a focus only on individual behaviours.
Weight
Overweight and obesity increase the risk of illnesses such as type 2 diabetes, cardiovascular disease, and some cancers (WHO, 2024b). People with higher weight can also experience discrimination and stigma, which can have negative effects on their mental and physical health and create barriers to accessing services (Arora et al., 2019; Westbury et al., 2023). While the factors that influence overweight and obesity are varied and complex, evidence shows that many are associated with the social determinants of health (Williams et al., 2024). For example, having access to affordable and healthy food, green spaces to be physically active in, and the density of local out of home (OOH) food provision all play an important role in shaping health behaviours (Everest et al., 2022). Commercial factors, such as the way in which foods are marketed, priced, and labelled, also have a significant influence (Kalra et al., 2023; Gilmore et al., 2023). These are explored in more detail in section 3.5 of this report.
The SHeS asks a range of questions relating to health and health behaviours, as well as collecting height and weight measurements. The most recent SHeS showed that in 2023, two thirds (66%) of adults in Scotland were classed as living with overweight or obesity (Body Mass Index (BMI) 25 kg/m2 and over) (Scottish Government, 2024a), with no significant difference between males and females.
Almost a third (32%) of adults were living with obesity (BMI 30 kg/m2 and over) in 2023, which is the highest level in the time series and an increase from 24% in 2003 (ibid.; Figure 7). The increased prevalence of obesity has been identified as an additional factor that may have contributed to deteriorating mortality rates in Scotland, including through a contribution to the stalling of improvements in cardiovascular mortality (Walsh and McCartney, 2023). Nesta (2023) estimated the full cost of obesity in Scotland at £5.3 billion in 2022, £4.1 billion of which is in value lost to people through reduced quality of life.
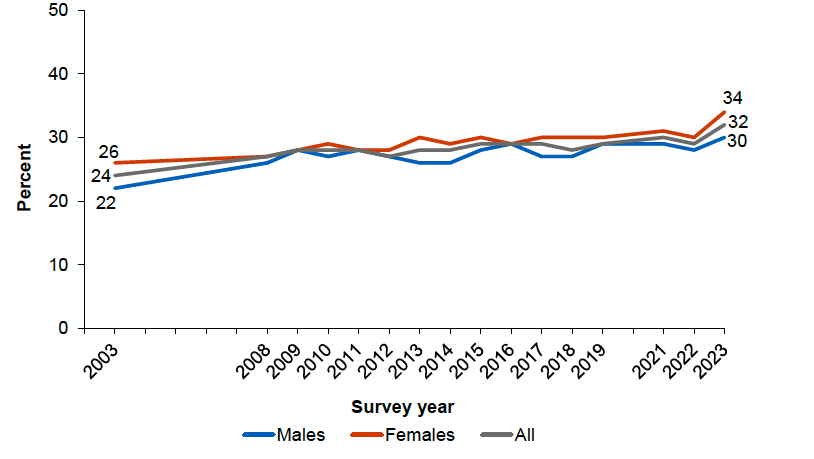
Source: Scottish Government (2024a)
Levels of overweight and obesity in Scotland are also patterned by inequality. In 2023 the proportion of adults in the most deprived areas living with overweight or obesity was 69%, compared with 58% in the least deprived areas (Scottish Government, 2025b).
Childhood overweight and obesity are also significant concerns in Scotland. In 2023, 30% of children were at risk of overweight (including obesity) (ibid.). Evidence highlights that having a higher weight in childhood and adolescence affects immediate health, is a reliable predictor of overweight and obesity into adulthood, and is linked with the early emergence of associated health problems (WHO, 2024b).
PHS (2024d) statistics on the BMI of Primary 1 school children (aged around five years old) in Scotland also show that in the school year 2023/24, 76.5% of those measured had a healthy weight, while 22.3% were at risk of overweight or obesity and 1.2% were at risk of underweight. This report highlights marked socioeconomic inequalities in child healthy weight, particularly in the percentage of children at risk of obesity. In 2023/24 14% of children living in the most deprived areas were in this category, compared with 6.4% of those living in the least deprived areas.
Diet
Poor diet, including regular overconsumption of foods high in calories, fat, sugar, and salt, is one of the key factors leading to weight gain and obesity (Swinburn et al., 2004). Beyond its role in obesity, having a poor diet also contributes to conditions such as coronary heart disease, high blood pressure, stroke, type 2 diabetes, dental decay, and some types of cancer (Food Standards Scotland (FSS), 2020). In Scotland, the average diet is too high in calories, total fat, saturated fat, sugar and salt and too low in vegetables, fruit, fibre, and other key nutrients (ibid.).
Research by Scheelbeek et al. (2020) highlights that significant health and environmental benefits could be realised by adherence to the national dietary recommendations outlined in the Eatwell Guide. The Eatwell Guide is the main source of consumer facing advice on maintaining a healthy and sustainable diet across the UK (FSS, 2025), including Scotland, where the Scottish Dietary Goals are also in place for scientific monitoring purposes and to underpin policy (Scottish Government, 2016a). Scheelbeek et al. (2020) found that greater adherence to the recommendations was associated with both reduced mortality and lower dietary greenhouse gas (GHG) emissions.
Despite these potential benefits, current food environments do not support healthy food choices. For example, the food environment heavily incentivises and promotes low-cost, energy-dense, and nutrient-poor foods (Pineda et al., 2024) which disproportionately contribute to intakes of calories, fat, saturated fat, sugar, and salt (FSS, 2023). Furthermore, people living in more deprived areas face particular challenges in consuming a healthier diet due to a lack of access to healthy, affordable food (PHS and FSS, 2024; PHS, 2024e). Research shows that those living in the most deprived areas would need to spend around half of their disposable income on food to meet the cost of the Eatwell Guide, while those in the least deprived areas would only need to spend around a tenth (PHS and FSS, 2024). Those living in more deprived areas are therefore more likely to experience the adverse health outcomes associated with a poor diet and, in some cases, food insecurity.
Findings from the most recent SHeS showed that 14% of adults reported experiencing food insecurity (being worried they would run out of food) in Scotland in 2023, an increase from 9% in 2021 and the highest level since the time series began in 2017 (Scottish Government, 2024a). This proportion increased with deprivation, rising from 6% in the least deprived areas to 23% in the most deprived areas (Scottish Government, 2025b).
Physical activity
Physical activity is a broad term describing any form of activity performed by the human body, including everyday activities like walking, gardening and DIY, as well as active recreation and sport (PHS, 2022a). It is effective in the prevention, early intervention, and management of many long-term conditions and noncommunicable diseases (NCDs) such as heart disease, stroke, diabetes, and breast and colon cancer (WHO, 2024c). Being active also helps to prevent hypertension, overweight and obesity, and can improve mental health, quality of life, and wellbeing (PHS, 2024f). It can also reduce the risk of overall mortality, including in those already diagnosed with some NCDs (Geidl et al., 2020). In addition to the multiple health benefits of physical activity, populations that are physically active can generate additional social, environmental, and economic benefits (PHS, 2024f).
Many different factors can determine how active people are and the overall levels of physical activity across different population groups. People’s ability to be active is strongly shaped by their circumstances and surroundings, such as aspects of the built environment (e.g. the existence of active travel infrastructure and green space), as well as social and cultural factors (Smith et al., 2017).
In 2023, 63% of adults in Scotland reported meeting the guidelines for moderate or vigorous physical activity (MVPA)[12], which is within the range of 62-69% recorded between 2012 and 2022 (Scottish Government, 2024a; Figure 8). However, there are significant inequalities between different groups and their engagement in physical activity. For example, in 2023 males were more likely than females to adhere to the guidelines across most age groups, most notably among those aged 25-34 (80% and 63% respectively) and those aged 75 and over (45% and 30% respectively) (ibid.).
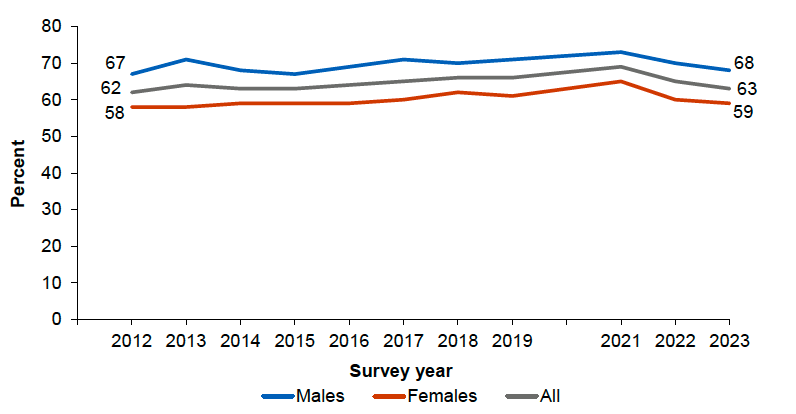
Source: Scottish Government (2024a)
Adherence to the MVPA guidelines also tends to be higher among those living in the least deprived areas compared with those in the most deprived areas. While over seven in 10 (72%) of those living in Scotland’s least deprived areas met the recommended level of physical activity in 2023, among those in the most deprived areas the equivalent proportion was one in two (50%), marking one of the lowest proportions in the 2012-2023 timeseries (ibid).
PHS (2024g) estimated the burden of disease attributable to physical inactivity in Scotland and found that an estimated 3,185 deaths and over eleven thousand (11,474) disability-adjusted life years (DALYs) are attributable to physical inactivity in Scotland. More than 80% of these deaths and DALYs are due to the 'very low' physical activity category (those doing less than 30 mins/week of moderate physical activity per week).
Tobacco and vaping
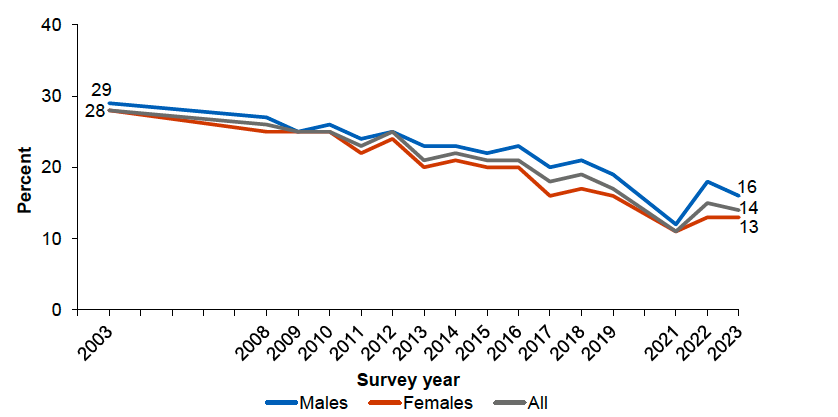
Tobacco dependency remains the leading preventable cause of mortality in Scotland, with tobacco a major risk factor for diseases such as cardiovascular disease and lung cancer (WHO, 2023a; PHS, 2023a; PHS 2024h). The most recent SHeS showed that in 2023, 14% of adults in Scotland were current tobacco cigarette smokers (Scottish Government, 2024a; Figure 9). Tobacco smoking prevalence was similar among males and females (16% and 13% respectively), although significantly more females than males indicated that they had never smoked (66% and 59% respectively) (ibid.).
While tobacco smoking rates have declined steadily since 2008 (ibid.), in 2022 it still accounted for an estimated 8,942 deaths (271 deaths per 100,000 population) among those aged 35 and over in Scotland (21% of all deaths) (PHS, 2023a).
Source: Scottish Government (2024a)
A wide body of evidence shows that the more disadvantaged a person is the more likely they are to be dependent on tobacco, with smoking associated with various indicators of deprivation and marginalisation (Action on Smoking and Health (ASH), 2019a). Higher smoking rates in specific population groups are influenced by a range of interacting social, economic, and cultural factors that shape smoking initiation, patterns, and behaviours, as well as attempts to quit (PHS, 2024i). For example, those in more deprived circumstances are more likely to be exposed to high availability of tobacco products, to experience stress and mental health issues, and are less likely to have encouragement, social support, or access to information about where to get help to quit smoking (ibid.).
Data from SHeS illustrates the strong association between smoking and deprivation in Scotland. In 2023, smoking prevalence was highest among adults living in the most deprived areas (26%) and lowest among those living in the least deprived areas (6%) (Scottish Government, 2024a). This trend has been observed since 2003, when smoking prevalence was 45% in the most deprived areas and 17% in the least deprived areas (ibid.).
Smoking in pregnancy, which increases the risk of stillbirth, preterm birth and low birthweight, follows a similar pattern. Data from PHS (2024j) show that in 2023, women reported smoking in 11% of pregnancies with a known smoking status. This proportion has decreased slightly each year since antenatal booking data collection began. However, women from the most deprived areas reported being a current smoker in 20.4% of pregnancies where smoking status was known, compared with 2.4% in the least deprived areas.
Among adolescents, smoking prevalence is at its lowest level since 1990 (Inchley et al., 2023). In 2022, the Health Behaviour in School-Aged Children (HBSC) study reported that just under one in ten (9%) adolescents reported having ever smoked cigarettes, with the prevalence increasing with age: 1% of 11-year-olds, 6% of 13-year-olds, and 20% of 15-year-olds (ibid.). More recent data from the 2024 ASH SmokeFree GB Youth survey[15] indicated that 17% of Scottish adolescents aged 11-17 reported having ever tried smoking, with 4% identifying as current smokers (Scottish Government, 2024c).
While smoking prevalence among adolescents has declined over time, there have been substantial increases in e-cigarette use since 2018. In 2022, the HBSC reported that 3% of 11-year-olds, 10% of 13-year-olds and 25% of 15-year-olds said they had used an e-cigarette in the past 30 days, and almost one in five (18%) said they had used an e-cigarette at least once in their lifetime (Inchley et al., 2023). In 2024, results from the ASH SmokeFree GB Youth survey showed that 19% of Scottish adolescents aged 11-17 had ever tried vaping, of which 7% identified as current vapers (Scottish Government, 2024c). Both the HBSC and ASH SmokeFree GB Youth surveys show that current and ever use increase with age.
Although not as significantly as for adolescents, e-cigarette use has also been increasing among adults in Scotland. Current use of e-cigarettes reached 12% in 2023, an increase from 10% in 2022 and 7% in 2019 (Scottish Government, 2024a; 2025b). While current research indicates that vaping is less harmful to health than smoking when smokers completely switch to e-cigarettes, evidence shows that vaping causes health harms (such as due to addiction or exposure to toxicants) in non-smokers to which they would not otherwise have been exposed (Scottish Government, 2024d). To date there are insufficient data on a number of clinical outcomes (e.g. cardiovascular or respiratory disease, and cancer) caused by vaping, including in pregnancy, and biomarkers of potential harms to health cutting across several diseases (Royal College of Physicians, 2024).
Alcohol
Alcohol is a significant problem in Scotland in terms of mortality, morbidity and social harm. Its detrimental impacts on health include causing liver disease, cardiovascular disease, type 2 diabetes, and cancer (ScotPHO, 2025a). Harmful alcohol use also has a significant negative social impact, for example increasing the likelihood of accidents and violence (Commission on Alcohol Harm, 2021). Research by McVie and Morales-Gomez (2024) shows that violent incidents in Scotland are concentrated in places with higher availability of alcohol premises. Manca et al. (2021) also demonstrate the significant burden alcohol consumption places on emergency services, particularly ambulance services. Their analysis of data from 2019 showed that one in six ambulance callouts (16.2%) in Scotland were alcohol-related, rising to over one in four (28%) during weekend nights (6pm to 6am).
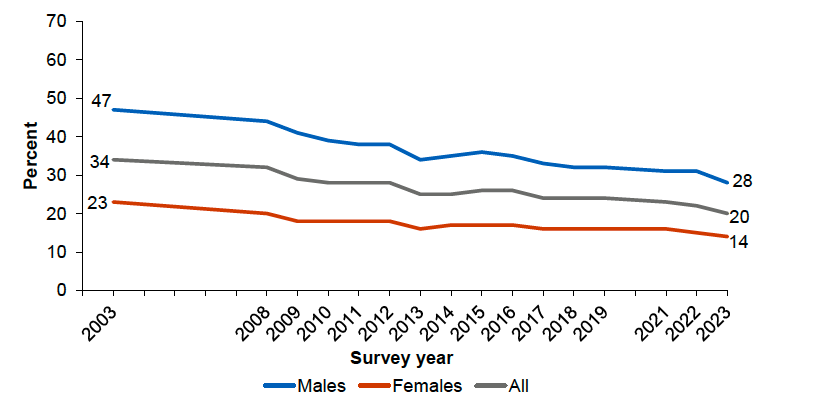
The prevalence of hazardous or harmful drinking has decreased over time in Scotland, with the latest SHeS showing that levels have fallen from 34% in 2003 to 20% in 2023 (Scottish Government, 2024a; Figure 10). Hazardous or harmful weekly alcohol consumption is twice as high for men (28%) as for women (14%).
Source: Scottish Government (2024a)
The prevalence of hazardous or harmful drinking is also patterned by deprivation. Unlike smoking and overweight and obesity, which are more prevalent in more deprived areas, levels of hazardous or harmful drinking tend to be higher among those living in the least deprived areas. In 2023, the prevalence of hazardous or harmful alcohol consumption was 23% in the least deprived areas compared with 17% in the most deprived areas (ibid.).
Despite lower levels of hazardous or harmful drinking, evidence shows that those in the most deprived areas experience higher levels of alcohol harm. For example, in 2023 alcohol-specific deaths were 4.5 times as high in the most deprived areas of Scotland compared with the least deprived areas (NRS, 2024c). There were 1,277 alcohol-specific deaths in total, the highest number registered in a year since 2008 (ibid.).
This is known as the alcohol harm paradox (Jones et al., 2015; Smith and Foster, 2014). While it is difficult to conclude the mechanisms and pathways that underlie this, possibilities presented in the literature include compounding due to clustering of health risk behaviours in more deprived areas, and differences in drinking patterns rather than differences in intake (e.g. ‘bingeing’ and heavy episodic use; drink-type preference) (Jones et al., 2015).
Research by Katikireddi et al. (2017) showed that disadvantaged social groups experience greater alcohol-attributable harms compared with individuals from advantaged areas even after accounting for different drinking patterns, obesity, and smoking status. Their findings showed that the risk of alcohol-attributable harms among moderate alcohol consumers of low socioeconomic status was greater than for those who drink heavily but are socioeconomically advantaged. They discuss how lived experiences of poverty shape the emergence of health outcomes, not only through health-related behaviours but also as a result of poor material circumstances and psychosocial stressors. For example, poverty can reduce resilience to disease and impact access to high quality treatment, predisposing drinkers of low socioeconomic status to greater health harms despite exposure to similar levels of risk factors as drinkers of high socioeconomic status.
Looking at alcohol consumption in younger people in Scotland, HBSC shows that the proportion of adolescents (11, 13, and 15-year-olds) reporting having been drunk at least twice has steadily declined since 1998 and was at its lowest level in 32 years in 2022 (Inchley et al., 2023). Nevertheless, two-fifths (41%) of adolescents reported that they had drunk alcohol at least once in their lifetime and 12% reported having been drunk two or more times in their life (ibid.). Alcohol use in adolescence is associated with more regular and higher rates of alcohol use and dependence in adulthood, as well as additional mental health problems and wider social harms (Marshall, 2014).
Drugs
Scotland has one of the highest drug death rates in Europe. In 2023, there were 1,172 drug deaths[16] registered in Scotland, an increase of 12% (121 deaths) compared with 2022 (NRS, 2024b). Drug deaths have been increasing in Scotland over the last two decades, with the rate of drug deaths 4.2 times higher in 2023 than 2000 after adjusting for age (ibid.). The use of drugs, and particularly opioids, benzodiazepines, and stimulants, is associated with a range of health and social harms. The loss of life due to drugs, particularly amongst those aged 35-55 years, means that drug deaths are impacting on overall life expectancy trends for Scotland and are exacerbating health inequalities (PHS, 2024k). Other health harms include risk of blood-borne viruses and injuries relating to injecting, while broader social harms associated with drug use include an increased risk of homelessness, stigma, and social isolation (ScotPHO, 2025b).
Drug-related deaths are more prevalent among people who lived in socioeconomically disadvantaged communities. People in the most deprived areas of Scotland were more than 15 times as likely to die from drug use compared with people in the least deprived areas in 2023 (NRS, 2024b). For deaths of all causes, people in the most deprived areas are around twice as likely to die as those in the least deprived areas. The links between problematic drug use and experiences of deprivation are complex, but evidence highlights the role of poverty and disadvantage, alongside increased exposure to trauma and poor mental health, amongst other historical and demographic factors (Sweeney, 2020; Linton et al., 2017; Walsh et al., 2016; Pinderhughes et al., 2016). Reducing deprivation and its consequences removes barriers that impede recovery, good health, and full participation in society.
The effects of inequality such as deprivation, homelessness, trauma, and co-occurring mental health problems on a person are known to be compounding factors that can greatly impact quality of life and the harms associated with substance use (Bramley et al., 2020). The stigma associated with drug use and the additional stigmatisation of people because of the criminalisation of drug use increases discrimination and drives inequality. Stigma and discrimination reduce the availability, accessibility, and acceptability of the fundamental building blocks of health (Scher et al., 2023). This increases the risk of poor health and adverse social outcomes, and limits opportunities for reducing harm amongst those at the highest risk.
Multiple risk factors
While the above health risks and behaviours are often considered in isolation, it is often the case that multiple risk factors occur together. For example, there is strong evidence of clustering between alcohol misuse and smoking, and poor diet and smoking (Meader et al., 2016). These risk factors can interact, so that two or more risk factors can have a greater effect than may be expected of each factor individually (ScotPHO, 2024a). A systematic review, which investigated the joint risks of alcohol consumption, smoking, and excess weight across all major health outcomes, found that alcohol and smoking together were strongly associated with head and neck cancer, while alcohol and excess weight jointly increased the risk of liver disease (Burton et al., 2023).
It is possible to analyse the presence of multiple risk factors within the Scottish population using SHeS data. In 2023, the proportion of adults with two or more risk behaviours (current smoker, harmful or hazardous drinker, low physical activity, obesity) was 27% (Scottish Government, 2025b). The percentage of the population with multiple risk factors increases with deprivation, with the percentage of adults with two or more health risk behaviours in the most deprived areas (39%) over double that of those in the least deprived areas (18%) in 2023 (ibid.).
The impact of Covid-19
As noted above, the Covid-19 pandemic exacerbated the issues of stalling and worsening life expectancy in Scotland. The impacts of Covid-19 on health were profound and included the direct effects of the virus itself and indirect effects through reduced access to care, the health impacts of response measures, and wider impacts on the economy, such as changes to employment and income (ScotPHO, 2023b).
Being older, male, from an ethnic minority background, and having lower socioeconomic status were all associated with a higher risk of Covid-19 mortality (Mikolai et al., 2023). These inequalities were driven by individual- and community-level factors, including underlying morbidity and vulnerability to Covid-19, vaccination rates, and the broader social determinants of health (Bambra et al., 2020; McGowan and Bambra, 2022). The indirect impacts were also felt most acutely by those on lower incomes, those living in more deprived areas, and those in ethnic minority groups (Douglas et al., 2020).
Recent analysis of the Global Burden of Disease (GBD) Study 2021 showed that European countries who experienced the greatest slowdown in life expectancy improvements before the Covid-19 pandemic – including Scotland, the other UK nations, Italy and Greece – were generally the most severely affected by Covid-19 and had some of the largest decreases in life expectancy in 2019-21 (Steel et al., 2025).
2.4. Future projections
Predicting future health trends is inherently uncertain. However, the Scottish Burden of Disease Study (SBoD) – a national, and local, population health surveillance system which monitors how diseases, injuries and risk factors prevent the Scottish population from living longer lives in better health – offers valuable insights by forecasting the burden of disease in Scotland. Findings from the SBoD show that despite an overall decline in the projected population, the annual disease burden is forecast to increase by 21% over the next 20 years (PHS, 2022b). The most significant increases are expected in cardiovascular diseases, cancers, and neurological diseases, which together are anticipated to account for two-thirds of this rise (ibid.).
The SBoD study has recently been updated to forecast how demographic and population health trends might interact, providing a more comprehensive view of future public health challenges (PHS, 2025a). These projections incorporate historic trends on disease prevalence alongside projected changes in the Scottish population. Based on both demographic changes and historical trends, PHS projects the following:
- Diabetes (type 1 and type 2 combined): The number of people with diabetes in Scotland is estimated to increase by 36% from 2019 to 2044, from 307,800 prevalent cases to 419,200 prevalent cases. This equates to an additional 111,400 people living with diabetes in 2044, compared to 2019.
- Ischaemic heart disease (IHD): The number of people with IHD in Scotland is estimated to decrease by 15% from 2019 to 2044, from 252,600 prevalent cases to 215,500. This equates to 37,100 fewer people living with IHD in 2044, compared to 2019.
- Cerebrovascular disease: The number of people with cerebrovascular disease in Scotland is estimated to increase by 35% from 2019 to 2044, from 106,000 prevalent cases to 143,000. This equates to an additional 37,000 people living with cerebrovascular disease in 2044, compared to 2019.
- Atrial fibrillation: The number of people with atrial fibrillation is projected to increase by 56% from 2019 to 2044, from 113,700 prevalent cases to 177,600. This equates to an additional 63,900 people living with atrial fibrillation in 2044, compared to 2019.
- Chronic obstructive pulmonary disease (COPD): The number of people with COPD is estimated to increase by 63% from 2019 to 2044, from 134,300 prevalent cases to 219,000. This equates to an additional 84,700 people living with COPD in 2044, compared to 2019.
- Chronic liver disease: The number of people with chronic liver disease is estimated to increase by 54%, from 43,200 prevalent cases to 66,300. This equates to an additional 23,100 people living with chronic liver disease in 2044, compared to 2019.
PHS (ibid.) highlights the significant implications of these projections for public health and the health and social care system, with any increases in disease prevalence and burden likely to impact the sustainability of services in the future. However, these projections are not inevitable. Policies and interventions have the potential to alter these trends and improve health outcomes, with PHS (ibid.) emphasising that prioritising prevention is the most effective way of reducing the rate of new disease cases. The next section explores the benefits of shifting to a system focused on prevention, examines other opportunities to make progress in improving population health in Scotland, and sets out key challenges that the PHF must address.
Contact
Email: socialresearch@gov.scot