Coronavirus (COVID-19): ONS Infection Survey – antibody data - 21 July 2021
Antibody data from the ONS COVID-19 infection survey published on 21 July 2021.
This publication presents an analysis of antibody prevalence, which can be used to identify individuals who have had COVID-19 in the past or who have developed antibodies as a result of vaccination. The findings presented in this publication are based on data from the Office for National Statistics (ONS) COVID-19 Infection Survey.
The COVID-19 Infection Survey aims to measure:
- how many people test positive for COVID-19 infection at a given point in time, regardless of whether they report experiencing coronavirus symptoms
- the average number of new infections per week over the course of the study
- the number of people who test positive for antibodies, to indicate how many people are ever likely to have had the infection or have been vaccinated
All results are provisional and subject to revision.
The Office for National Statistics (ONS) publish estimates for England, Wales, Northern Ireland and Scotland on their website.
The underlying data displayed in the charts in this publication is available in the reference tables on the ONS website.
Main points
In Scotland, it is estimated that almost 9 in 10 adults, or 88.6% of the adult community population (95% credible interval: 86.7% to 90.3%) would have tested positive for antibodies to SARS-CoV-2 from a blood sample in the week beginning 28 June 2021, suggesting that they had the infection in the past or have been vaccinated.
In the most recent week, antibody positivity has continued to increase in Scotland.
The percentage of adults testing positive for antibodies continued to increase in those aged between 16 and 34 years; it remains high for those aged 35 and over.
The percentage of adults in the community population testing positive for antibodies aged 16 to 24 years was 57.3% (95% credible interval: 48.2% to 65.7%). The percentage testing positive for antibodies in those aged 25 and over ranged from 89.1 to 96.4%; the highest percentage of people testing positive for antibodies was in those aged 65 to 69 at 96.4% (95% credible interval: 94.8% to 97.5%).
There is a clear pattern between vaccination and testing positive for COVID-19 antibodies but the detection of antibodies alone is not a precise measure of the immunity protection given by vaccination. Having antibodies can help to prevent individuals from getting the infection, but it does not guarantee that an individual cannot be infected with COVID-19.
Information on this release
In this publication, the following terminology is used:
- antibodies – the presence of antibodies to SARS-CoV-2 is measured in the community population to understand who has had COVID-19 in the past, and the impact of vaccinations. It takes between two and three weeks after infection or vaccination for the body to make enough antibodies to fight the infection. Having antibodies can help to prevent individuals from getting the infection. Once infected or vaccinated, antibodies remain in the blood at low levels and can decline over time. The length of time antibodies remain at detectable levels in the blood is not fully known
- community population – in this instance community population refers to private residential households, and excludes those in hospitals, care homes and/or other institutional settings
- SARS-CoV-2 – this is the scientific name given to the specific virus that causes COVID-19
It is not yet known how having detectable antibodies, now or at some time in the past, affects the chance of becoming infected as other parts of the immune system (T cell response) will offer protection. Antibody positivity is defined by a fixed amount of antibodies in the blood. A negative test result will occur if there are no antibodies or if antibody levels are too low to reach this threshold.
It is important to draw the distinction between testing positive for antibodies and having immunity. Following infection or vaccination, antibody levels can vary and sometimes increase but are still below the level identified as “positive” in this test, and other tests. This does not mean that a person has no protection against coronavirus (COVID-19) since an immune response does not rely on the presence of antibodies alone. We also do not yet know exactly how much antibodies need to rise to give protection. A person’s ‘T cell’ response will provide protection but is not detected by blood tests for antibodies. A person's immune response is affected by a number of factors, including health conditions and age. Additional information on the link between antibodies and immunity and the vaccine programme can be found in the latest ONS blog.
The daily official government figures provide the recorded actual numbers of vaccines against SARS-CoV-2 issued; the vaccination estimates from the COVID-19 Infection Survey are likely to be different from the official figures and should not be used to track the progress of the vaccine rollout. Please see the latest daily official government figures on vaccination data on the UK coronavirus dashboard to understand the progress of the vaccination programme across the UK. This is because they are estimates based on a sample survey of reported vaccine status and are provided for context alongside antibodies estimates. Importantly, the survey collects information from the population living in private households and does not include people living in communal establishments such as care homes, hospitals or prisons. Those that live in care homes were one of the priority groups identified by the Joint Committee on Vaccination and Immunisation (JCVI). The value of showing estimates of vaccines alongside estimates of people testing positive for antibodies is to illustrate the relationship between the two.
Differences between official figures and the estimates from this survey differ in scale across each of the four nations (some survey estimates are closer to the official reported figures than others) due to differences in reporting dates and the inclusion of National Immunisation Management System (NIMS) data for England. In addition, the sampling method for Northern Ireland is different to the other nations, inviting only people that have previously participated in a Northern Ireland Statistics and Research Agency (NISRA) survey, which could result in a sample of individuals that are more likely to get vaccinated. This should be taken into consideration if comparing vaccine and antibody estimates across the four nations, since vaccine status and antibody positivity are related. In addition, as the analysis develops, the survey-based estimates will enable possible future analysis of people who have received a vaccine with other characteristics collected in the survey. ONS have recently published a blog which provides more information on what the ONS can tell you about the COVID-19 vaccine programme.
There is high uncertainty around COVID-19 Infection Survey estimates due to the relatively small number of people included in this analysis, so caution should be taken in interpreting the results.
The weekly modelled estimates use standard calendar weeks starting on a Monday. To provide the most timely and accurate estimates possible for antibody positivity, the model will include data for the first four to seven days of the week, depending on the availability of test results. The antibody and vaccination estimates for the most recent week in this publication include data from 28 June to 4 July 2021.
Further information on the methodology can be found at the end of this release.
Antibody estimates: likelihood of testing positive for antibodies to SARS-CoV-2
In Scotland, it is estimated that almost 9 in 10 adults, or 88.6% of the adult community population (95% credible interval: 86.7% to 90.3%) would have tested positive for antibodies to SARS-CoV-2 from a blood sample in the week beginning 28 June 2021, suggesting that they had the infection in the past or have been vaccinated. Antibody positivity has continued to increase in Scotland.
Modelled weekly estimates of the percentage of people testing positive for antibodies to SARS-CoV-2 from a blood sample, are displayed in Figure 1 as estimates for the midpoint of the week.
Figure 1: Modelled weekly percentage of people in the adult community population testing positive for antibodies to SARS-CoV-2 from a blood sample, from 7 December 2020 to the week beginning 28 June 2021, including 95% credible intervals
Antibody estimates by age group: likelihood of testing positive for antibodies to SARS-CoV-2, by age group
The percentage of adults testing positive for antibodies to SARS-CoV-2 (the specific virus that causes COVID-19) continued to increase in those aged between 16 and 34 years; it remains high for those aged 35 and over.
The percentage of adults in the community population testing positive for antibodies aged 16 to 24 years was 57.3% (95% credible interval: 48.2% to 65.7%). The percentage testing positive for antibodies in those aged 25 and over ranged from 89.1 to 96.4%; the highest percentage of people testing positive for antibodies was in those aged 65 to 69 at 96.4% (95% credible interval: 94.8% to 97.5%).
Figure 2: Modelled percentage of people in the community population testing positive for antibodies to SARS-CoV-2 from a blood sample, by age group, in the week beginning 28 June 2021, including 95% credible intervals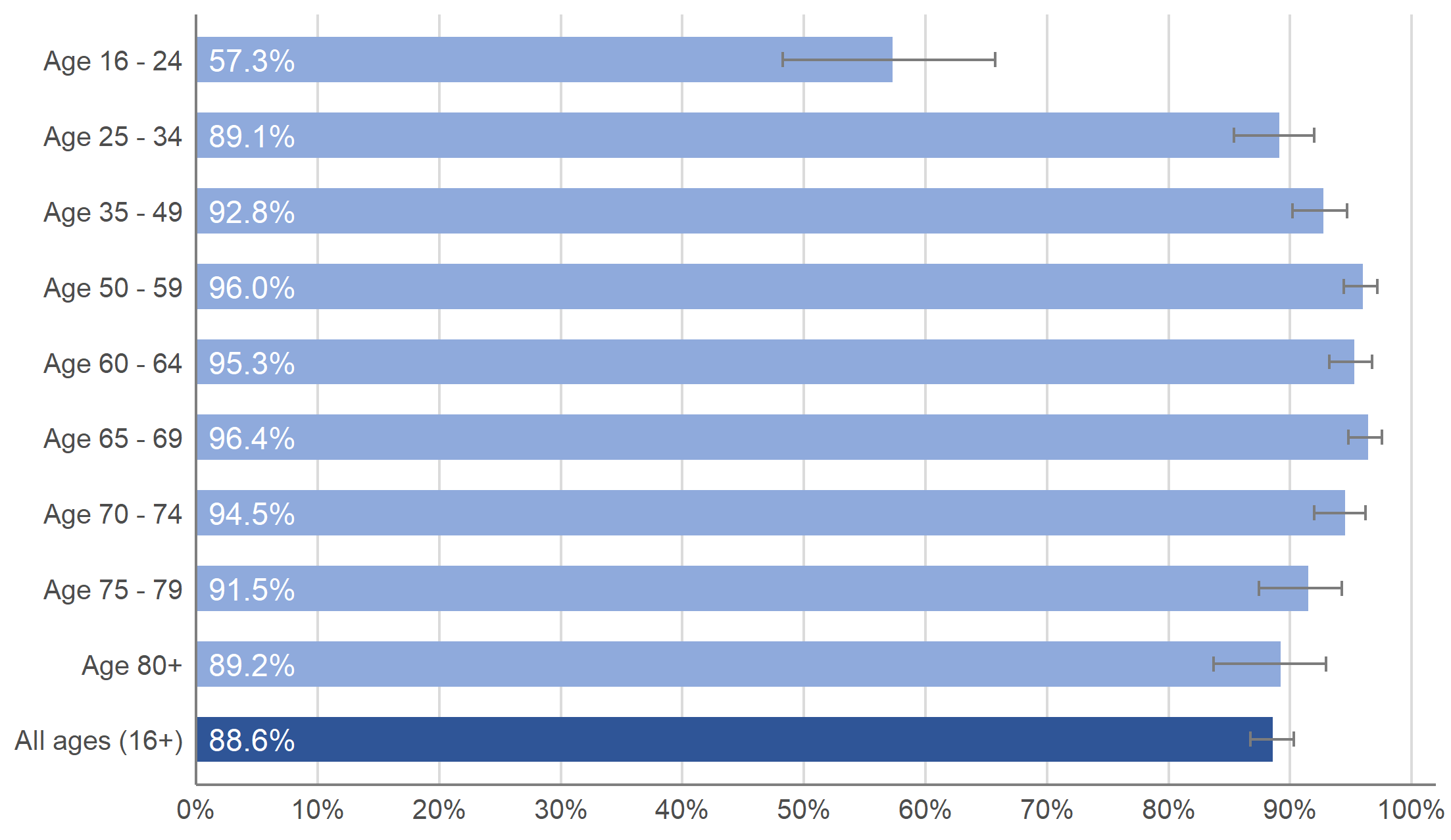
Figure 3 shows the modelled weekly estimate of the percentage of people in the community population testing positive for antibodies to SARS-CoV-2 from 7 December 2020 to the week beginning 28 June 2021 by age group, showing the trend over time.
When antibodies are measured over time by age, it is possible to see the impact of the vaccination programme between first and second doses. Antibody positivity is generally increasing with age, with the highest percentage testing positive for antibodies in the older age groups and lowest among the youngest groups. This reflects the age prioritisation in vaccination programmes in place. The percentage of adults who reported they have received at least one dose of a coronavirus (COVID-19) vaccine is lowest in the younger age groups but is increasing.
In March, antibody positivity decreased among people aged 80 and over and has since increased, likely as a result of second doses. A similar decrease and subsequent increase can be seen in those aged 70-79 at the end of March 2021. For those aged 60-69 and 50-59, antibody positivity flattened before increasing again from April and May 2021 respectively.
Modelled weekly estimates of the percentage of people in the community population testing positive for antibodies to SARS-CoV-2 from a blood sample by age group are displayed in Figure 3 as estimates for the midpoint of the week.
Figure 3: Modelled weekly percentage of people in the community population testing positive for antibodies to SARS-CoV-2 from a blood sample, by age group, from 7 December 2020 to the week beginning 28 June 2021, including 95% credible intervals
Modelled daily estimates of antibody positivity by single year of age in the most recent weeks can also be found in the accompanying dataset and visualisation published by the ONS in their antibody data bulletins.
The methodology used to produce the daily modelled estimates is different to that used to produce the weekly estimates and as such, these figures are not directly comparable. This more granular analysis shows a similar pattern to our grouped age analysis.
Antibody and vaccination estimates: comparison of the likelihood of testing positive for antibodies to SARS-CoV-2 with vaccination estimates
It is important to note that this section contains estimates based on self-reported vaccines from the ONS COVID-19 Infection Survey and should not be used to track the progress of the vaccine rollout. Please see the latest daily vaccination data on the UK coronavirus dashboard to understand the progress of the vaccination programme across the UK.
Survey estimates refer to the community population, by which we mean private households only and excludes those in hospitals, care homes or other institutional settings. This data does not include those that live in care homes, one of the priority groups identified by the Joint Committee on Vaccination and Immunisation (JCVI).
Differences between official figures and the estimates from this survey differ in scale across each of the four nations due to a number of factors referenced in the ‘Information on this release’ section above. This should be taken into consideration if comparing vaccine and antibody estimates across the four nations, since vaccine status and antibody positivity are related.
There is a clear pattern between vaccination and testing positive for antibodies to SARS-CoV-2 (the specific virus that causes COVID-19) as shown in Figure 4, but the detection of antibodies alone is not a precise measure of the immunity protection given by vaccination.
Modelled weekly estimates are displayed in Figure 4 as estimates for the midpoint of the week. The ‘one or more doses’ category also includes those that are fully vaccinated.
Figure 4: Modelled weekly estimate of percentage of people in the community population that have received one or more doses of a COVID-19 vaccine and modelled weekly percentage of people testing positive for antibodies to SARS-CoV-2 from a blood sample, from 7 December 2020 to the week beginning 28 June 2021, including 95% credible intervals
Modelled weekly estimates of the percentage of people that have received one or more doses of a COVID-19 vaccine, or who have been fully vaccinated by age group can also be found in the full bulletin published by the Office for National Statistics on 21 July 2021, which can be accessed here.
Methodology and further information
The analysis presented in this publication is based on blood test results taken from a randomly selected subsample of individuals aged 16 years and over, which are used to test for antibodies against SARS-CoV-2. This can be used to identify individuals who have had the infection in the past or have developed antibodies as a result of vaccination.
It takes between two and three weeks after infection or vaccination for the body to make enough antibodies to fight the infection. Antibodies remain in the blood at low levels, although these levels can decline over time to the point that tests can no longer detect them. Having antibodies can help to prevent individuals from getting the infection, but it does not guarantee that an individual cannot be infected with COVID-19.
The presence of antibodies is measured to understand who has had COVID-19 in the past and the impact of vaccinations. Once infected, the length of time antibodies remain at detectable levels in the blood is not fully known. It is also not yet known how having detectable antibodies, now or at some time in the past, affects the chance of becoming infected or experiencing symptoms, as other parts of the immune system (T cell response) will offer protection.
The full bulletin on antibody and vaccination data published by the Office for National Statistics on 21 July 2021, which includes antibody information for England, Wales and Northern Ireland, can be accessed here.
More information about the COVID-19 Infection Survey in Scotland can be found on the information page on the Scottish Government website, and previous COVID-19 Infection Survey data for Scotland can be found in this collection.
ONS have changed from presenting antibody and vaccination data in a fortnightly article to a fortnightly bulletin series, with the last fortnightly article being published on 13 May 2021. Previous articles presenting antibody and vaccination data are still available.
Additional methodology notes not covered in main body of publication:
-
The model used to provide these estimates is a Bayesian model: these provide 95% credible intervals. A credible interval gives an indication of the uncertainty of an estimate from data analysis. 95% credible intervals are calculated so that there is a 95% probability of the true value lying in the interval. A wider interval indicates more uncertainty in the estimate.
-
National Immunisation Management System (NIMS) administrative data is used to validate COVID-19 Infection Survey self-reported records of vaccination for England. The equivalent of this is currently not included for other countries, meaning the estimates for Wales, Northern Ireland and Scotland are produced only from COVID-19 Infection Survey self-reported records of vaccination.
- The first COVID-19 vaccination was administered on 8 December 2020, but vaccination rates were too low to model until 14 December 2020. The estimates of the percentage of people vaccinated are based on modelling of the people visited in the COVID-19 Infection Survey in the community in a particular time period. These estimates are then adjusted (post-stratified) using population estimates to be representative (in the same way as for the antibody analysis). ONS present data on the estimated percentage of people aged 16 years and over who have received one or more doses of a COVID-19 vaccination since 14 December 2020 and the percentage of people aged 16 years and over who are fully vaccinated since 15 February 2021.
- The denominators used for vaccinations are the total people in the sample at that particular time point, which are then post-stratified by the mid-year population estimate.
- There is high uncertainty around COVID-19 Infection Survey estimates due to the relatively small number of people included in this analysis, so caution should be taken in interpreting the results.
- Previously, published estimates of antibody positivity were weighted estimates for 28-day periods of antibody positivity for England, Wales, Northern Ireland and Scotland, with fortnightly updates on antibody data. The first article using this new methodology was published on 30 March 2021. Estimates are now based on a model where England, Wales and Scotland are included together in a spatial-temporal model with Northern Ireland being modelled separately. This reflects the geography of the four countries with Northern Ireland not sharing a land border with Great Britain. The geo-spatial model incorporates physical land distance between regions.
- The data is modelled on standardised Monday-Sunday surveillance weeks and data from 7 December 2020 is presented. The latest week’s modelled estimate is subject to more uncertainty as it is an incomplete week of data and therefore more likely to change when more data become available. Further information on this method to model antibodies can be found in ONS updated methods article.
- The sampling method for Northern Ireland is different to the other nations, inviting only people that have previously participated in a Northern Ireland Statistics and Research Agency (NISRA) survey, which could result in a sample of individuals that are more likely to get vaccinated. This should be taken into consideration if comparing vaccine and antibody estimates across the four nations, since vaccine status and antibody positivity are related.