Drug and alcohol services - co-occurring substance use and mental health concerns: survey
This report presents the results of a survey of individuals working within services that provide support to people who use drugs or alcohol. It forms part of a wider rapid review of co-occurring substance use and mental health concerns in Scotland.
3. Main findings
3.1 Response rates and respondent information
Of the 349 individuals who were approached to complete the survey, 93 (27%) responded. Two respondents from criminal justice services have been excluded from the overall analysis as these services were outside the scope of the survey. Therefore 91 respondents (26% of those approached) are included in the overall analysis.[3]
It should be stated that the sample is not representative of all services that provide support for people who use substances in Scotland. The respondents self-selected to participate in the survey meaning that there may be some bias in the results. The survey results should therefore be treated with caution throughout and be regarded as indicative only of the views of the respondents that completed the survey. Despite this, it provides a useful insight into the provision and availability of care for people who experience co-occurring substance use and mental health concerns in Scotland.
The respondents worked across 79 different drug and alcohol services in Scotland. The majority of respondents (71) were from different services. However in 20 cases, a response was submitted by more than one member of staff from the same service. One service had four related responses, two services had three responses each and five services had two responses each. There were also two services that had two respondents who worked within different NHS Health Boards. It is important to note that responses have not been consolidated where multiple responses from the same service have been received. Data is presented from the point of view of the respondents, not the services.
The largest number of responses came from respondents working within the Alcohol and Drug Partnership areas of Aberdeen City (12%) and Glasgow City (12%) (see Table 1). There were also several respondents working within Edinburgh (11%), Dumfries and Galloway (8%) and Highlands (7%). The rest of the partnership areas had a few respondents working within them. There were no responses from Falkirk, Orkney and Shetland.
| Alcohol and Drug Partnership Area | Number of respondents | % of respondents |
|---|---|---|
| Aberdeen City | 11 | 12% |
| Glasgow | 11 | 12% |
| Edinburgh | 10 | 11% |
| Dumfries and Galloway | 7 | 8% |
| Highland | 6 | 7% |
| Falkirk | 0 | 0% |
| Orkney | 0 | 0% |
| Shetland | 0 | 0% |
| Other[4] | 46 | 51% |
Base: 91 respondents
Relating to the National Health Service (NHS) Health Board areas, the largest number of respondents worked within NHS Greater Glasgow and Clyde (23%) (see Table 2). NHS Grampian (18%) and NHS Lothian (16%) were the next most common health boards that the respondents worked within. NHS Orkney and NHS Shetland were the only health boards that did not have any responses.
| NHS Health Board | Number of respondents | % of respondents |
|---|---|---|
| NHS Ayrshire and Arran | 5 | 5% |
| NHS Dumfries and Galloway | 7 | 8% |
| NHS Grampian | 16 | 18% |
| NHS Greater Glasgow and Clyde | 21 | 23% |
| NHS Highland | 7 | 8% |
| NHS Lothian | 15 | 16% |
| NHS Orkney | 0 | 0% |
| NHS Shetland | 0 | 0% |
| NHS Tayside | 5 | 5% |
| Other[5] | 15 | 15% |
Base: 91 respondents
Most respondents (98%) described their services as community based. Just over half (51%) self-described as a community addiction service, while 13% of respondents said that their service was a residential community service. Some respondents reported that they provided multiple services in the community (7%), such as a combination of community addiction and primary care. The remaining respondents stated their services were based in primary or emergency care, counselling, employability, harm reduction, homelessness support, housing recovery, stabilisation units, rehabilitation, social housing, young people and social work.
The largest number of responses were received from those in leadership positions within a service (e.g. Chief Executive Officers, managers, team leaders), which accounted for 48% of the respondents (see Table 3). Respondents' professions also included clinical staff (37%), such as consultants, doctors, nurses, paramedics and medical officers. The remaining respondents were support workers, social workers, mental health counsellors and housing officers.
| Occupation | Number of respondents | % of respondents | |
|---|---|---|---|
| Leadership Positions | Manager | 31 | 34% |
| Team Leader | 9 | 10% | |
| CEO | * | * | |
| Clinical Staff | Consultant Psychiatrist | 13 | 14% |
| Nurse | 9 | 10% | |
| Doctor | 6 | 7% | |
| Medical Officer | * | * | |
| Paramedic | * | * | |
| Other | Support Worker | 8 | 9% |
| Counsellor | * | * | |
| Social Worker | * | * | |
| Housing Officer | * | * |
* low bases >5 responses have been suppressed for anonymity
3.2 Profile of the service users with co-occurring substance use and mental health concerns attending substance use services
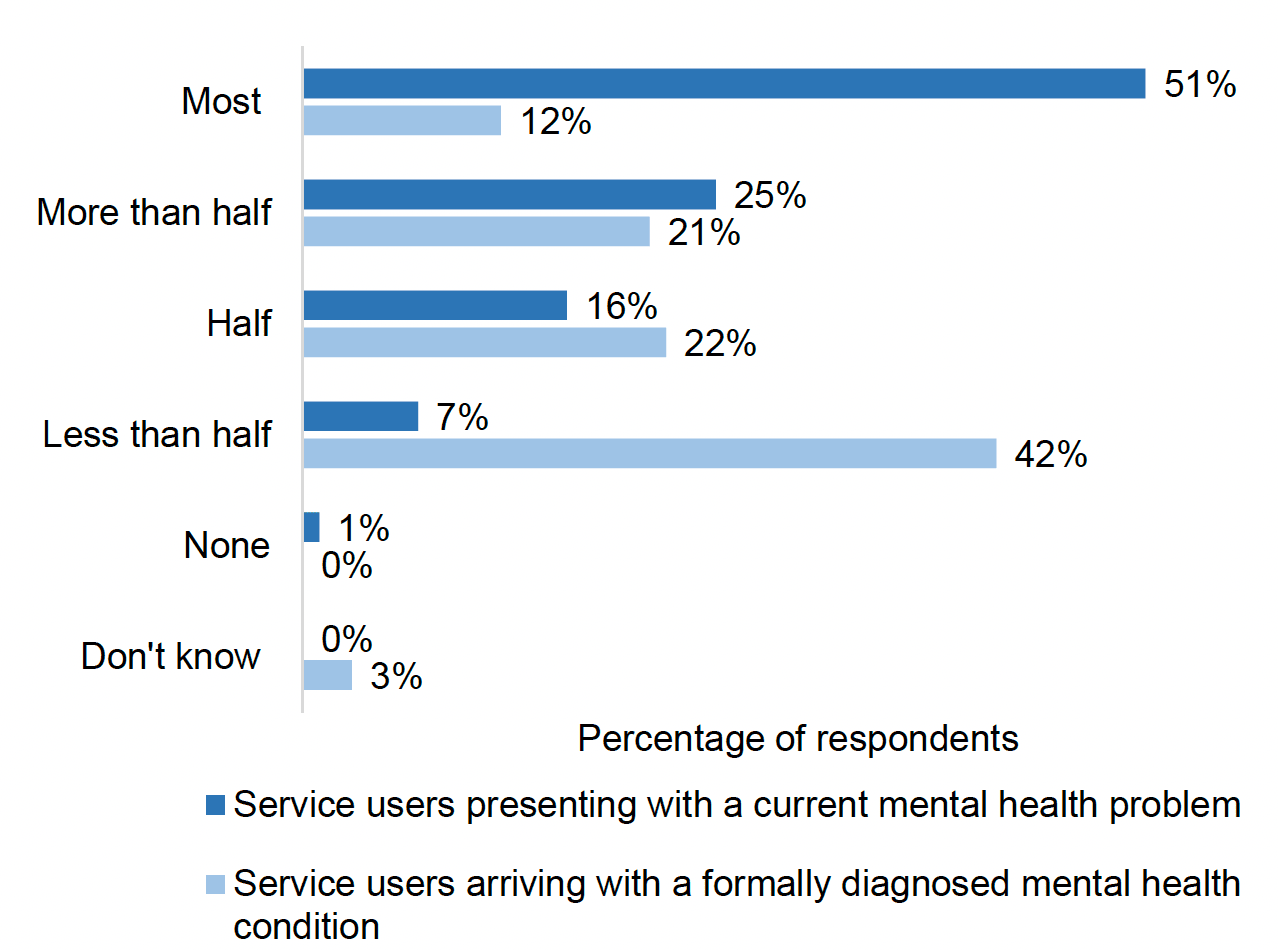
Respondents were asked to gauge what proportion of service users presented with co-occurring substance use and a current mental health concern at their service[6]. They were also asked to estimate the proportion of service users that arrived at their service with a formally diagnosed mental health condition.
Around three quarters of respondents (76%) said that the majority[7] of service users who attend their service presented with co-occurring substance use and a current mental health concern. Over half of respondents (51%) estimated that "most" of their service users did and a quarter (25%) of respondents estimated that "more than half" did so. There were 15 respondents (16%) that stated "half", and 6 respondents (7%) said "less than half". Only one respondent estimated that "none" of the current service users presented with co-occurring substance use and a current mental health concern.[8]
Two fifths (42%) of respondents estimated that "less than half" of service users service users with co-occurring substance use and mental health concerns presented with a formal diagnosis of a mental health condition. Around one in five respondents in each case estimated that "half" (22%) or "more than half" (21%) did so. Figure 1 shows the contrast between the respondents' estimates on the proportion of service users with co-occurring substance use and mental health concerns and those that had a formal diagnosis of a mental health condition on arrival to their service.
The majority of respondents (62%) reported that their service uses some form of mental health screening tool (see Table 4). Almost half of respondents (46%) reported using the General Health Questionnaire. Eleven respondents (12%) said they used the Beck Depression Inventory, while the remaining screening tools were reported as being used by less than 10% of respondents. Other examples of mental health screening tools used were GAD-7, PHQ-9, Mental Health Assessment for Nurses and the Core 10. Of the 56 respondents that reported using a screening tool, around three quarters (76%) said their service used a single assessment measure. There were also 13 respondents (14%) that indicated their service used two or more screening tools.
Just under a third of respondents (32%) said they did not use a mental health screening tool within their service. Despite not using a tool, the majority (76%) of these respondents said that "most" or "more than half" of the service users presented with a co-occurring substance use and mental health concern, and around half (52%) said that "less than half" presented with a formally diagnosed mental health condition.
| Type of mental health screening tool | Number of respondents | % of respondents |
|---|---|---|
| Beck Anxiety Inventory | 7 | 8% |
| Beck Depression Inventory | 11 | 12% |
| Hamilton Anxiety Rating Scale | 8 | 9% |
| General Health Questionnaire | 42 | 46% |
| None | 29 | 32% |
| Other specified | 13 | 14% |
| Don't know | 6 | 7% |
Base: 91 respondents
3.3 Substances involved in co-occurring substance use and mental health concerns
Respondents were asked about the types of substances used by people presenting at their service with co-occurring substance use and mental health concerns. Table 4 shows how commonly respondents reported different types of substances being involved in co-occurring substance use and mental health concerns.
| Type of Substance | Very common | Common | Occasionally | Never | I don't know |
|---|---|---|---|---|---|
| Alcohol | 77% | 22% | 1% | 0% | 0% |
| Amphetamines | 20% | 18% | 54% | 4% | 4% |
| Benzodiazepines (prescription/street) | 70% | 16% | 9% | 1% | 3% |
| Cannabinoids (including synthetic) | 57% | 29% | 12% | 0% | 2% |
| Cocaine (powder/crack) | 57% | 27% | 12% | 1% | 2% |
| Gabapentinoids | 25% | 45% | 22% | 2% | 5% |
| Methadone | 41% | 25% | 24% | 4% | 5% |
| Opiates | 48% | 29% | 16% | 3% | 3% |
| Prescription-only medicines | 22% | 40% | 34% | 0% | 4% |
Base: 91 respondents
Almost all of the respondents (99%) reported that alcohol was "commonly" or "very commonly"[9] used by people presenting at their service with co-occurring substance use and mental health concerns. Only one respondent answered that alcohol use was "occasionally" implicated. The majority of respondents also said that benzodiazepines (87%), cannabinoids (86%), cocaine (85%), opiates (77%), gabapentinoids (70%), methadone (66%) and prescription-only drugs (62%) were "commonly" or "very commonly" used by service users with co-occurring substance use and mental health concerns.
Less than half of respondents (37%) said that amphetamines were "commonly" or "very commonly" used by people presenting at their service with co-occurring substance use and mental health concerns. No respondents reported that alcohol, cannabinoids or benzodiazepines were "never" used by service users presenting with co-occurring substance use and mental health concerns. Other substances respondents reported were ketamine, nitrous oxide, crystal meth, mephedrone, novel psychoactive substances (NPS), gamma hydroxybutyrate (GHB) and solvents such as gamma butyrolactone (GBL).
3.4 Availability of mental health support and treatment within substance use services
Respondents were asked if their service is able to offer specific mental health support for service users who present with an undiagnosed mental health concern.
The majority of respondents (63%) reported that their service offers mental health support for service users who present with an undiagnosed mental health concern. Some of these respondents provided details on the type of support provided, which ranged from support from specialist staff (such as mental health nurses and psychologists) to specific interventions (such as consultant psychiatry and cognitive behavioural therapy).
Of the respondents who said their service offered mental health support[10], most (91%) said it was "common" or "very common" for their service to offer treatment for anxiety disorders (see Table 5). The majority of these respondents reported it was also "common" or "very common" for their service to offer treatment for mood disorders (86%) and post-traumatic stress disorder (75%). Less than half of the respondents said that their service commonly or very commonly offered treatment for attention deficit hyperactivity disorder (40%), alcohol-related brain damage (30%) and psychotic disorders (25%). Some respondents also commented that their service offered treatment for other mental health concerns including eating disorders, conversion disorder, learning disabilities, organic brain disorders and adverse childhood experiences.
| Mental Health Condition | Very Common | Common | Occasionally | Never | I don't know |
|---|---|---|---|---|---|
| Alcohol-related brain damage | 7% | 23% | 54% | 14% | 2% |
| Anxiety disorders (including general anxiety, obsessive compulsive disorder) | 60% | 32% | 2% | 5% | 2% |
| Mood disorders (including bipolar disorder, depression) | 51% | 35% | 7% | 5% | 2% |
| Personality disorders | 51% | 23% | 16% | 9% | 2% |
| Psychotic disorders (including schizophrenia) | 12% | 12% | 60% | 12% | 4% |
| Attention deficit hyperactivity disorder[11] | 12% | 28% | 46% | 11% | 2% |
| Post-traumatic stress disorder | 47% | 28% | 16% | 5% | 4% |
Base: 57 respondents
3.5 Referrals arrangements for mental health support
Over a third of respondents (37%) said that their service did not provide mental health support. The majority of these (85%) reported that they referred these service users to another service. There were 5 respondents (15%) that reported their service did not offer referrals. The majority of respondents who indicated that their service made referrals reported that the referral did not mean that the service user had to leave their service (90%).
Respondents noted different criteria for referral at their service. Some respondents said that their service referred individuals if they had any mental health concern, while others specified that the severity of the mental health concern would determine whether an individual was referred or not. Measures of severity were reported to include suicidality, survival of an overdose, or if a service user was experiencing a mental health crisis. A number of respondents commented that referrals were often initiated at the request of the service user seeking support. Other respondents said that a lack of expertise, resources and staff within their services meant that they had "limited time to offer psychological interventions", requiring them to refer service users to other services.
Most of the respondents who said that their service referred individuals to other services for mental health support referred them to community mental health teams (86%) (see Table 6). Respondents also reported referrals to general practitioners (66%), local third sector support organisation (62%) and online tools and resources (62%). A small number of these respondents (10%) said their service referred service users to an intensive home treatment team.[12] There were 26 respondents (90%) that selected more than one referral service. A few respondents also provided examples of referring service users to accident and emergency (A&E) mental health teams, community mental health nurses and mutual aid or peer support services.
| Services to which referrals are made | Number of respondents | % of respondents |
|---|---|---|
| Community mental health team | 25 | 86% |
| General practitioner | 19 | 66% |
| Local third sector support organisation | 18 | 62% |
| Online tools and resources | 18 | 62% |
| Crisis teams | 16 | 55% |
| Intensive home treatment team | 3 | 10% |
Base: 29 respondents
3.6 Protocols for coordinating care between multiple services
Respondents were asked whether a protocol was in place for coordinating the care of service users supported by more than one service and how protocols were improved upon.
Over half of respondents (55%) reported that there was a protocol in place for coordinating the care of individuals supported by more than one service[13]. A further 36% of respondents answered that their service did not have a protocol in place[14], while a few responded that they did not know (8%).
Where a protocol was reported to be in place, the majority of respondents (86%) reported that it was used[15]. A number of these respondents described how often the protocol was revised at their service. Some noted that their service revised their protocol "continually" or "as needed". Others detailed different timeframes, with most respondents reporting that protocols were reassessed annually, although monthly and quarterly were also mentioned. There were also respondents that stated it occurred every 2 years, with some noting it was "very overdue" and one commenting that it hadn't been revised since 2014.
Good communication and collaboration between services and service users were identified as key determinants to understanding whether a protocol was functioning appropriately. Service users were often "encouraged to be actively involved in their own care and support", with many respondents commenting that the service users' engagement was integral to understanding if a protocol was working. Engagement could take place, for example, through meetings between staff and service users to discuss individual cases or by service user feedback questionnaires. Some respondents said that clinical outcomes, measures, and other mental health indicators of the service user were used to understand if a protocol was working. Some respondents emphasised that good communication, collaboration and feedback between staff at their own service and that of the other service providers allowed them to evaluate and understand if a protocol was working.
Where no formal care management protocol was in place, respondents stressed communication with service users and between services as key to ensuring continuity of care.
3.7 Challenges experienced by and support offered to different groups of service users
Respondents were asked what the particular challenges experienced by different groups of service users were, and how the specific needs of these service users were supported.
There were a number of challenges that respondents highlighted for their services in meeting the needs of people experiencing homelessness. These included difficulties around attending appointments, a loss of contact with them, issues registering these service users at local general practitioner practices, and limited availability of secure housing when discharging them back into the community. To help overcome these challenges some respondents indicated that they worked collaboratively with other services to help provide support to service users who are experiencing homelessness by offering them housing. Respondents also said that some services have specific staff that provide to people experiencing homelessness, such as officers and nurse teams.
Non-English speakers were also identified as a group of service users that experience specific challenges. Many respondents at services where non-English speakers were service users said that they offered interpreters. Most statutory services, and larger third sector organisations, had access to interpreters via the NHS or similar services, but some smaller organisations reported making use of Google Translate. However some noted that it was difficult to have an interpreter there for the duration of a person's involvement with the service stay due to the availability of the interpreter and the associated costs. In addition, some noted that interpreters could act as a barrier for effective treatment in a therapeutic community environment.
Respondents said that there were particular challenges faced by women who attended their services. They said that these women could be at risk from experiencing trauma, sexual exploitation, and issues relating to family relationships and the fear of losing custody of children. Respondents said that services supported female service users by offering women-only groups and separate gender specific services such as female trauma groups and whole family approach teams that bring together adult and children services. They also emphasised providing privacy and security within their facilities.
Stigma around drug use or mental health was said to have made accessing treatment more difficult for some groups. A small number of responses also mentioned addressing the specific needs of the LGBTI community and those of young people. In addition, the issues services users with disabilities can experience in relation to their physical access to services were mentioned.
3.8 Suggested improvements to mental health support
Respondents were invited to report any further comments they had on how services could be improved to meet the needs of people with co-occurring substance use and mental health concerns.
A number of respondents discussed the issue around difficulties in referring individuals to mental health services and that once a referral had been made, this was often rejected on the basis that substance use was still an issue for that individual. Specifically, some felt that there were cases where an individual seeking support at a substance use service, should in principle have their primary support provided by a specialist mental health service. It was felt by some that lack of resources in mental health services contributed to care being focused on substance use, despite this not being where the focus should lie.
Respondents also highlighted the issue of resourcing within substance use services. It was felt that the limited numbers of support staff in services contributed to increased waiting times. Some respondents reported that they often feel like they were "firefighting" and dealing with issues reactively instead of taking the required time to develop relationships with service users and take a more holistic therapeutic approach. This was also felt to contribute to staff being less able to take a person centred approach, where multiple services provide support and care to an individual.
Specific suggested areas of improvement include flexibility in service delivery; increased scope for outreach (e.g. home visits); improved referral pathways between services, and the creation of local "hubs" where substance use and mental health services are located in the same place, allowing individuals to be jointly assessed and treated.
Contact
Email: socialresearch@gov.scot