Drug and alcohol services - co-occurring substance use and mental health concerns: literature and evidence review
Review of the existing evidence on co-occurring substance use and mental health concerns and the integration of mental health and substance use services relevant to a Scottish context. It forms part of a wider rapid review of co-occurring substance use and mental health concerns in Scotland.
3. Literature review
The terms "dual diagnosis", "co-existence", "co-occurrence", and "comorbidity" are all used to describe people who experience both problem substance use and mental health concerns. In this report co-occurrence is used to describe people who experience problem substance use and some form of mental health concern, which may be either diagnosed or undiagnosed.
The relationship between substance use and mental health is complex, but their co-occurrence is known to be common.[5] In some cases, substance use can lead to mental health concerns[6],[7] or existing mental health conditions may lead to problem substance use, particularly when used as a coping mechanism to manage mental health concerns.[8] There are numerous factors which can contribute to both problem substance use and mental health concerns, and to their co-occurrence. These include histories of adverse childhood experiences and trauma (including abuse, bereavement and parental imprisonment)[9],[10],[11],[12] as well as common intersecting issues, such as homelessness and offending. [13] The research literature also suggests that there may be specific considerations in relation to people with some of the protected characteristics set out in the 2010 Equality Act.[14] These include concerns that specifically affect older and younger people who use drugs or alcohol; lesbian, gay, bisexual, transgender, intersex (LGBTI) people; and those in certain ethnic groups and are highlighted within the themes throughout this review.
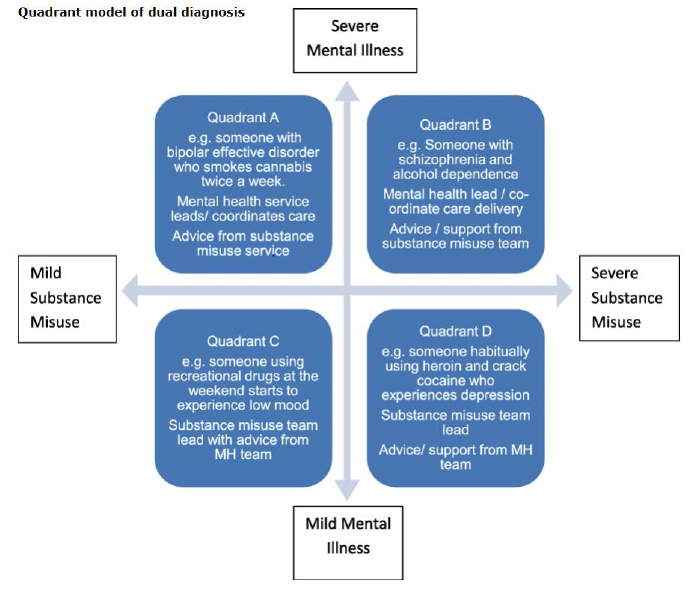
Mental health concerns and problem substance use can interact in many ways and varies according to the different circumstances, including the type and severity of substance use and mental health concerns.[15] Likewise, the support required, services accessed and care pathways required also vary. This is demonstrated in the Four Quadrant Model, which is one of several typologies developed to support understanding of the intersection between substance use and mental health.[16],[17] This is illustrated in Figure 1, which shows severity of substance use and mental health on the x and y axis, and illustrative examples of the types of challenges and potential support required in each quadrant.
There are a range of standards and approaches which have been implemented in Scotland which aim to meet the needs of people who use substances and experience mental health concerns, including the Medication Assisted Treatment (MAT) standards[19] which were published in 2021. In addition, the Scottish Government is committed to ensuring that people receive a person-centred approach to their care. Based on the Healthcare Quality Strategy for NHS Scotland, this is described as: "Mutually beneficial partnerships between patients, their families and those delivering healthcare services which respect individual needs and values, and which demonstrate compassion, continuity, clear communication and shared decision making".[20] The principles of a person-centred rather than service-centric approach are known to improve health outcomes and the advantages of involving patients as individuals and as partners in the processes of recovery through a provision of care that is personalised, coordinated, and enabling are well established.[21] Person-centred care has been shown in many settings and contexts to enhance adherence to treatment plans[22],[23] improve health outcomes and increase participant satisfaction with healthcare services.[24],[25]
In practice, however, there is mixed evidence about how standards and approaches, including person-centred care, are being implemented and experienced by those with co-occurring substance use and mental health concerns. This is highlighted in research including in the recent Mental Welfare Commission report, Ending the exclusion: care, treatment and support for people with mental ill health and problem substance use in Scotland.
People experiencing co-occurring substance use and mental health concerns are seen to be at higher risk of poor psychological health,[26],[27] high medical needs,[28],[29] sub-optimal levels of engagement in treatment[30] and a higher likelihood of engagement with the criminal justice system.[31] When interacting with the healthcare system, they also report high levels of unmet needs[32],[33] and often cite judgmental attitudes and a skills deficit among providers.[34] These issues are important from a patient-centred and ethical standpoint, but also clinically as patient satisfaction with care is associated with better outcomes.[35] The research literature highlights the complexity of issues and experiences relating to substance use and mental health concerns, where researchers and clinicians generally indicate that intervention is needed to improve both the quality of care and health outcomes.
This report is divided into subsections reviewing policy, academic and third sector literature on co-occurring substance use and mental health concerns. The first section highlights the current progress made within policy development in Scotland and the wider UK. The report then provides an overview of the prevalence of issues around co-occurring substance use and mental health concerns, drawing from high level statistics and evidence reviews. The report then highlights the key themes in barriers to accessing treatment for people experiencing co-occurring substance use and mental health concerns and finally, provides a review of the frequently recommended interventions from the literature.
3.1 Policy developments
Over the past twenty years, the challenges experienced by people with co-occurring substance use and mental health concerns have been brought into focus.[36] This has led to the development of a range of policies aimed at supporting service provision to meet their complex needs.
3.1.1 Scottish Government Policy
The Scottish Government has made a number of commitments over the last ten years with regards to co-occurring substance use and mental health concerns. In January 2021, the First Minister announced a National Mission to reduce drug related deaths and harms. A clear focus was placed on ensuring that people are able to make an informed choice about the support and treatment they need and are able to access this when they need it through rights-based and person-centred model of care.
Prior to the announcement of the National Mission, the Scottish Advisory Committee on Drug Misuse (SACDM) and the Scottish Advisory Committee on Alcohol Misuse (SACAM) agreed in 2002 to commission a Joint Working Group to address the needs of people with co-occurring substance use and mental health concerns. Their 2003 report, Mind the Gaps, highlighted the need for improvements to promotion and prevention activities; education and awareness; efficacy of care and treatment services; and strategic planning.[37] This report was followed up by Mental Health in Scotland: Closing the Gaps in 2007,[38] which made a number of recommendations including that: frontline staff in substance use services should be trained in suicide awareness and prevention; all substance use and mental health services should have an assessment tool in place to assess comorbidity and help match care appropriate to the level and type of need; substance use services should develop skills in psychological therapies; and mental health services should take the lead on the coordination of care in the case of people with severe and enduring mental health conditions, whose needs are best met within specialist mental health care.
Following on from these key documents, both the Mental Health Strategy in 2017[39] and the Rights, Respect and Recovery: Alcohol and drug treatment strategy in 2018[40] outlined how services should treat people. This includes trauma-informed approaches that recognise the link between substance use, mental health and adverse experiences; staff and systems that do not stigmatise people who use substances; and person-centred services that wrap around the individual, not the other way around. The Scottish Government has also published a guide[41] for commissioners, managers, trainers and practitioners on implementing a number of the ambitions in the Scottish Government's Mental Health Strategy,[42] particularly those around integrated treatment for mental health and problem substance use.
The Mental Health Transition and Recovery Plan, published in 2021, states that the Scottish Government will work with partners to explore opportunities for integrating addiction and general mental health services. The plan aims to provide better co-ordination of support for people with co-occurring substance use and mental health concerns. It is supported by The Mental Health Strategy 2017-2027, which details two actions relating to co-occurring substance use and mental health concerns . These are to:
Action 27 – "Test and learn from better assessment and referral arrangements in a range of settings for dual diagnosis for people with problem substance use and a mental health condition."
Action 28 – "To offer opportunities to pilot improved arrangements for dual diagnosis for people with problem substance use and an associated mental health diagnosis."[43]
The Medication Assisted Treatment (MAT) standards were published in 2021 and provide a framework of clearly defined principles that all services and organisations responsible for the delivery of care must adhere to in order to meet the needs of people who use substances. Standard nine[44] focuses on mental health and states that "all people with co-occurring drug use and mental health difficulties can receive mental health care at the point of MAT delivery". It highlights numerous criteria for both mental health and substance use services which aim to support people with co-occurring substance use and mental health concerns, with the aim of avoiding sequential treatment and limiting dropout between services. Standard 10[45] also focuses on trauma informed care, with the acknowledgement that the majority of people accessing MAT are likely to have histories of complex trauma which may be intrinsically linked to the individual's drug use. Trauma informed services aim to promote recovery and improve outcomes for individuals, their families, staff and services.
The final report of Scotland's Drug Deaths Taskforce Changing Lives in 2022 continued this theme of improving care through more integrated working between mental health and substance use services. This report[46] includes a number of key principles specifically relating to mental health and problem substance use. The "No Wrong Door" message is particularly strongly made. This acknowledges that problem substance use can be a result of or lead to support needs that cross multiple sectors and services. People with multiple needs may not necessarily fit within the existing systems that are in place, however, they should not be rejected on these ground. All services to which people with co-occurring substance use and mental health concerns present should ensure no one is turned away without making sure that supportive contact is made. The report also highlights that mental health support should not be conditional on people receiving treatment for their dependency, recovery or abstinence. The Taskforce also recommends for a single lead professional to take a coordinating role in developing and overseeing a holistic care package, with the patient's consent and involvement.
In addition to these Scottish Government publications, the literature includes published public sector policy and third sector policy reports on co-occurring substance use and mental health concerns, which are explored in the next section.
3.1.2 Wider UK Policy
Outwith Scotland, other UK nations also have policy developments which contribute to our understanding of how to provide support and services for people with co-occurring substance use and mental health concerns.
Much of the recent UK Government and devolved government policy addressing services for people with co-occurring substance use and mental health concerns resonates with Scottish Government policy and aims to address some of the same challenges, such as the need for service integration and increased staff training (see sections below).[47],[48],[49] A 2017 Public Health England commissioning guide[50] highlights that people with co-occurring substance use and mental health concerns often found themselves excluded from services,[51],[52] and emphasises aims of Everyone's Job (where all providers of mental health and substance use services have a joint responsibility to meet the needs of individuals with co-occurring conditions) and No Wrong Door aims (as highlighted in the Scottish Drug Deaths Taskforce Changing Lives report[53] above).
On 8 February 2019 Professor Dame Carol Black was appointed to lead a UK government-commissioned independent review[54] that looked into treatment, recovery and prevention. The review focused solely on England but has had a key influence on the development of drugs policy across the devolved administrations. The report highlighted the need for radical reforms in leadership, funding and commissioning for Commissioners of substance use services and NHS mental health services to ensure that individuals do not fall between the cracks. Specifically highlighted was the need to improve the provision of mental health services.[55]
3.1.3 Key points
- Scottish Government policy has increasingly addressed the challenges facing those with co-occurring substance use and mental health concerns. These aim to embed holistic, person-centred approaches within guidelines and standards and target mechanisms for improved referrals and service integration for people with co-occurring substance use and mental health concerns.
- Where other aspects of drug policy may diverge across the UK and devolved governments, there appears to be a consensus towards greater service integration and staff training needs (see barriers to accessing services and recommended interventions sections below). Service user-centred ambitions are also expressed via values such as values such as "Everyone's Job" and "No Wrong Door" which, even where not named directly, can be identified to some extent as core principles.
3.2 Prevalence of co-occurring substance use and mental health concerns
Understanding the prevalence of mental health and problem substance use co-occurrence and the level of need for support and treatment is methodologically complex. Exact figures for the number of people who experience co-occurring substance use and mental health concerns are not collected systematically, however some academic research, local audits and policy work provide estimates, combined with figures from the wider UK. The current lack of evidence in the Scottish context is an area for potential further research.
Data from the 2021 Scottish Health Survey[56] indicated that adults who had used drugs in the previous 12 months reported lower mental wellbeing scores on average than those who had not used drugs (mean Warwick-Edinburgh Mental Wellbeing Scale of 45.4 and 49.1 respectively). Similar patterns were recorded among both men and women. Evidence provided in the 2021 National Confidential Inquiry into Suicide and Safety in Mental Health[57] found that it was estimated that problem substance use was a factor in between 48% and 56% of all suicides between 2008 and 2018 in Scotland. This indicates both the prevalence of intersecting problem substance use and mental health concerns, as well as the severity of consequences for people who are unable to access appropriate care and support.
From a clinical perspective, research undertaken[58] in 2014 in general adult inpatient wards of a city hospital in Scotland found that use of Novel Psychoactive Substances (NPS) was identified in 22.2% of psychiatric admissions over a period of six months, contributing to psychiatric symptoms in 59.3% of patients. These admissions were more likely to be young, male and having had contact with the criminal justice system.
A study[59] based on evaluating the impact of public health interventions in reducing harms related to substance use in Scotland linked administrative data to measure the risks of mortality related to problem drug use in Scotland between 2010 and 2020 for a cohort of 46,960 individuals. It found that 14.3% of those in the sample had a past mental health disorder hospital admission. It also found that those with a past hospital admission for a mental health disorder had higher mortality rates both based on deaths from all causes (mortality rate of 28.05 per 1000 person years, compared to an overall mortality rate of 22.00 per 1000 person years) and drug-related deaths (mortality rate of 17.71 per 1000 person years, compared to an overall mortality rate of 12.91 per 1000 person years).
The survey published alongside this literature review also indicates a high prevalence of co-occurring substance use and mental health concerns. It found that around three quarters (76%) of respondents working across 79 different drug and alcohol services in Scotland said that the majority of services users who attend their service presented with co-occurring substance use and a current mental health concern (either diagnosed, self-defined or that the respondent believed the service user could benefit from mental health support). However, 42% of respondents also estimated that less than half of their service users presented with a formal diagnosis of a mental health condition at their service.
Evidence from the UK Government based on statistics from England[60] shows that in 2021, nearly two-thirds (63%) of adults starting treatment for substance use said they had a mental health treatment need, which is part of a rising trend. Those with a mental health treatment need ranged from 57% in the opiate group to 71% of the non-opiates and alcohol group.
Research from an evidence review[61] undertaken in 2009, looking primarily at studies undertaken across the UK, estimated that between 20% and 37% of people using mental health services experience problem drug or alcohol use. However, figures of people accessing mental health services from substance in substance use services settings were less clear, partly due to a lack of psychiatric diagnostic testing performed in these settings. Based on a small number of studies, between 6 and 15% of people accessing substance use services were estimated to have been diagnosed with psychiatric disorders were. This review[62] also indicated higher rates of co-occurrence in inner city areas, as well as differences by ethnicity. People from Afro-Caribbean backgrounds were over-represented among clinical populations of people with co-occurring mental health and substance use. White people were over-represented compared with Asian and mixed groups.
3.2.1 Homelessness
People experiencing homelessness or who are at risk of homelessness are identified in the literature as experiencing a higher rate of health inequalities across a wide range of conditions, including co-occurring mental health and substance use.[63]
Research conducted by the Scottish Government from 2001 to 2016[64] compared 435,853 people who had been assessed as homeless or threatened with homelessness with control groups from the most and least deprived areas of Scotland. The study found that 19% of the people who had been assessed as homeless or threatened with homelessness had evidence of substance use during the study period, with 94% of these having evidence of co-occurring mental health concerns. The data showed that people experiencing homelessness were more likely to have evidence of problem substance use or a mental health concern (though not necessarily co-occurring) compared to the control groups, which was even more likely for people who had experienced repeated periods of homelessness.
Work focusing on homelessness in Glasgow also shows the prevalence of co-occurring substance use and mental health concerns. A retrospective five year study conducted in Glasgow from 2000 found that being homeless resulted in a sevenfold increase in the risk of a drug-related death.[65] More recently, a study[66] linked a population register of adult residents in Glasgow to administrative datasets from homelessness and criminal justice services; community pharmacies, a clinical psychosis registry with data from 2010 to 2014, and death registrations from 2014 to 2019. It was found that homelessness, opioid dependence, justice involvement and psychosis were commonly occurring and were each associated with an increased risk of poor health and high rates of premature mortality, with risk increasing with the number of co-occurring factors.
These findings are echoed in research undertaken in a wider UK context, including by organisations working directly with people affected by homelessness. Research published in a 2020 report[67] by St Mungo's, a homelessness charity based in London and the South-East of England, highlighted that that drug and alcohol related causes accounted for more than half of the 726 deaths in 2018, where 12,000 people "rough sleeping" or at risk of doing so went without vital drug and alcohol treatment in England in 2019.[68] The report provides qualitative insight into the experiences of homelessness and highlights the close association between drug and alcohol and experiences of trauma and exclusion prior to and while a person is homeless, the impacts of which are often self-medicating using drugs and alcohol.
3.2.2 Key points
- There is currently a lack of systematically collected evidence on the exact prevalence of co-occurring substance use and mental health concerns in Scotland. There is also a lack of recent evidence pertaining to equalities groups, including about different genders, ages, minority ethnic communities and LGBTI people.
- Overall, co-occurring substance use and mental health concerns are thought to be common, with lower mental wellbeing reported for adults who use drugs. Problem substance use was a factor in 48%-56% of all suicides between 2008 and 2018 in Scotland. Based on evidence from England, nearly two-thirds of adults starting treatment for substance use said they had a mental health treatment need.
- There is significant evidence around the disproportionate level of co-occurring substance use and mental health concerns amongst people experiencing or at risk of experiencing homelessness.
3.3 Barriers to accessing treatment
Across the literature there are reports of the barriers that people with co-occurring substance use and mental health concerns face when trying to access support and treatment. The Scottish Government's 2007 Closing the Gaps review provided foundational insight into many of the issues faced in accessing treatment, and found that at the time "of the 44% of mental health service users misusing substances, less than 5% satisfied eligibility criteria for drug treatment programmes in their area".[69] Substance use services were also set up to support opiate dependence, as opposed to more predominantly used substances including alcohol, cannabis, sedatives and stimulants. The review found that personality disorders and mild to moderate depression and anxiety were the main diagnosed mental health conditions experienced by people who use drugs and alcohol, all of which were considered to have "low potential for referral" to mental health services.[70] This section explores research undertaken subsequently into the barriers to accessing treatment for people with co-occurring substance use and mental health concerns.
3.3.1 Lack of integrated services
Many sources highlight the barriers presented by the lack of availability of integrated care, with estimates for the proportion of people receiving integrated care for co-occurring substance and mental health concerns in the UK being as low as 4%.[71] The recent Mental Welfare Commission report also highlighted that 90% of the general practitioners surveyed in their research reported difficulties in referring patients to both mental health and substance use services, including when the patient presented in crisis.[72]
The Dundee Drugs Commission conducted a review[73] of the impact of drug use in Dundee and of the support available to people who use drugs. Following a call for evidence, the most common and consistent finding was that there was "a lack of mental health support for those who experience problems with drugs".[74] This was usually expressed as either: a reluctance of statutory drug treatment services to address mental health (i.e. where people presenting to substance use services were told "we only deal with drug problems, not mental health"); or the perceived refusal of mental health services to work with individuals unless they addressed their substance use first.
Alongside the Dundee Drugs Commission's work, NHS Tayside commissioned an independent inquiry[75] to assess the accessibility and quality of care at all mental health services in the area. It found that services in Dundee that were established to address substance use and mental health did not operate jointly to complement each other's work and that there was a lack of services available that could take responsibility for individuals who presented with mental health symptoms and under the influence of drugs or alcohol. The inquiry found evidence that patients who needed to be referred to substance use services were discharged without a relevant referral and that in the event of an overdose, some patients were discharged from mental health services and were referred to the Integrated Substance Misuse Service (ISMS), which provides both substance use and mental health services.
The lack of appropriate services is echoed by findings from research undertaken by third sector organisations working across the UK. In 2015, ADFam – the families and substance use charity – and the Recovery Partnership published its State of the Sector report[76] which highlighted the challenges of providing joined-up support to service users across England with multiple and complex needs, such as co-occurring substance use and mental health concerns. One hundred and seventeen respondents completed this survey, of which 37% were service managers and 63% worked within a service in another role. A fifth of the respondents reported that access to mental health provision had worsened over the previous year, with only 9% reporting an improvement. The consistency with which access to mental health services was flagged as an issue suggests that it remained a key challenge.[77]
The Association of Mental Health Providers, the leading representative body for voluntary and community sector mental health organisations in England and Wales, published its report on co-occurring substance use and mental health concerns in 2016.[78] It noted that joint commissioning was rare despite government initiatives and policy guidance to develop more integrated services for people with co-occurring substance use and mental health concerns. The report also highlighted some of the challenges to effective service delivery including: the lack of a joined up approach, failure to diagnose or recognise need, and lack of access to services.
3.3.2 Abstinence requirements for mental health care
A barrier identified in the literature is the requirement on the part of some mental health services that individuals stop using substances prior to receiving treatment for their mental health. This is found to be the case in a number of UK-wide and Scottish based reviews.[79],[80],[81]
The Simon Community, a charity working on homelessness in Northern Ireland, published a report[82] in 2022 which acknowledged that substance use was a barrier to accessing services for homelessness, mental health and substance use. While many of their clients were receiving help for substance use, qualitative feedback highlighted difficulties in accessing services where there were co-occurring mental health concerns. In these cases, clients were told to manage their substance use prior to mental health services providing support, or that their poor mental health was a result of problem substance. Ultimately, this lead to people disengaging with all services.
The literature also highlights instances of self-medicating, whereby people use substances as a coping mechanism to manage mental health concerns. Where they are then required to stop using substances in order to access mental health services, this can present significant challenges. This complexity was highlighted in a 2021 study[83] based on interviews with drug treatment and mental health professionals working in England. It also noted that Scottish and UK quality standards recommending that substance use should not be a reason to exclude people from psychiatric treatment were not always followed, highlighting a divergence between policy and practice.[84],[85]
3.3.3 Quality of care
The literature frequently identifies barriers to people with co-occurring substance use and mental health concerns receiving a high quality of care. This often relates to staff attitudes and perceptions of substance use and mental health. Effective therapeutic relationships are known to be key determinants in the success or failure of treatment strategies for patients with substance use disorders[86] while negative attitudes by health professionals may detract from patients' sense of empowerment and self-efficacy and may lead to worse treatment outcomes.[87],[88]
Following a retrospective case-note review of patients admitted to inpatient psychiatric wards in England, Williams et al. [89] found that substance use disorders were commonly comorbid with anxiety and depressive disorders and were associated with a lower quality of care and poorer treatment outcomes. The study found that discrepancies in care quality may contribute to the poor treatment outcomes experienced by patients with problem substance use, and strategies to reduce this inequality are necessary to improve the wellbeing of this patient group.
Staff attitudes can have a negative impact on how patients or service users feel about accessing services, particularly those with certain mental health concerns. A review[90] published in 2011 looked at the interlocking factors that can contribute to poor responses to people with multiple and complex needs from a range of front line services (including health, social care, welfare, housing and criminal justice agencies). As well as drawing attention to the service user's experience of these services, the review highlighted individual, organisational and structural challenges that staff within these services negotiate. The review identified poor relationships and lack of trust between clients and staff, as well as poor continuity of care and fragmented service response. This was echoed in the 2022 Mental Welfare Commission report[91], which noted the impact of staff shortages on delivery of care, and particularly how this can cause a lack of continuity. For services users, this can mean having to re-tell their story repeatedly to multiple different staff members and relive past trauma.
In literature relating to protected characteristic groups, the need for more inclusive care was emphasised. Qualitative research[92] undertaken with substance users in Glasgow highlighted experiences of racism and stereotyping experienced by people from minority ethnic groups within substance use services, which was seen as a barrier to accessing these services. The survey published alongside this report also highlights the challenges for non-English speakers in accessing services with appropriate interpreters.
There can also be specific difficulties in accessing treatment services for mental health and substance use issues for people in the LGBTI community. One study[93] looking specifically at LGBTI people's mental health (but not substance use) found that stigma and a lack of staff knowledge and understanding of the needs of LGBTI individuals acted as barriers to accessing services. The researchers identified a need for mental health care that promotes the principles of equity, inclusion and respect for diversity, thus understanding that the LGBTI community is not a homogenous group, and faces unique challenges when dealing with their mental health needs.
3.3.4 Stigma
The stigmas attached to both mental health concerns and problem substance use are highlighted in the literature around accessing treatment, and were echoed in the results of the survey released alongside this report. Concerns of stigma are particularly prominent in relation to specific groups, such as certain age groups and minority ethnic groups. The Scottish Drug Deaths Taskforce 2022 report[94] particularly highlights the impact of the stigma around substance use on reinforcing trauma and having mental health impacts in and of itself. Related to staff attitudes, numerous sources[95],[96] highlight service user perceptions of stigma from service providers to people experiencing co-occurring substance use and mental health concerns, and particularly those also experiencing homelessness. Evidence from a study[97] undertaken in Canada highlights gendered dynamics of stigma, where women reported higher levels of perceived stigma than men.
In 2016, a literature review[98] from the Scottish Centre for Crime and Justice Research (SCCJR) considered the response of services to the specific needs of people aged 35 and over who use drugs, including tackling social isolation, shame and stigma issues. Older individuals who used drugs were more likely to consider substance use a moral failing[99] and felt stigmatised due to having a mental health condition or using psychotropic medicines.[100] As such, while stigma is a barrier regardless of age, self-stigmatising views create an additional barrier to seeking and accessing support. Respondents who identified experiencing the multiple stigmas of drug addiction, being on methadone treatment, and ageing, also reported having fears about seeking drug treatment. They discussed not wanting to seek drug rehabilitation services because of their perception of being stigmatised due to their age by their peers and staff. They were also worried they would be the oldest service user in the methadone clinic, and that they would not fit in. The report concluded that there were few models of care internationally that could be mapped onto Scottish service provision without issue and that creative solutions would be needed to design services to meet the needs of older people who use drugs.
There has been limited work on the specific issues affecting ethnic minorities who use drugs in Scotland. However, Khan et al.[101] found that stricter attitudes to recreational drug use were common among Asian Scottish families and that this could encourage greater secrecy concerning their use out of fear of their parents discovering their use of drugs. Participants in this study also reported that they felt service staff from the same ethnicity as them would judge them more harshly than white Scottish service users given the shared social and cultural attitudes towards drugs, creating a barrier to accessing services.
3.3.5 Homelessness
There is a significant overlap between homelessness and co-occurring substance use and mental health concerns and homelessness provides its own, additional, challenges for those seeking access to services or treatment.
A recent review of reviews of the effectiveness of treatments and services for people who are homeless and use substances found many barriers to accessing healthcare and treatment. These included perceived stigma and discrimination by staff, strict appointment times and complicated administration procedures.[102] A 2021 report[103] from the University of Liverpool explored the experiences of people who have been homeless and used drugs or alcohol in accessing statutory or voluntary support services, based on interviews and focus groups with people with lived experience. The research found that the longer people were homeless, the harder they felt it was to get support from services, including the police; and that this wore down their physical and mental health. They reported that consistent rejection and disappointment led to feelings of hopelessness which often led to a continued or increased use of drugs and alcohol.
Research[104] undertaken with frontline staff working in homelessness support services in Scotland also highlighted the experiences of those supporting people experiencing homelessness. It described the varying interactions between service users and staff, noting that service users who were withdrawn or angry evoked feelings of frustration for staff, resulting in job dissatisfaction and acting as a barrier to staff engagement. This was perceived to increase the likelihood of some service users falling through the net in accessing support.
Research by Adams et al.[105] noted that people experiencing homelessness have higher rates of mental health concerns and problem substance use and lower access to health services compared to the general population. They specifically focussed on the changes in delivery across health and social care services as a result of the COVID-19 pandemic, with many adopting virtual or telephone alternatives to face-to-face support for service users. Such reactive changes to service provision often led to inadvertent exclusion. Barriers to access reported by those with lived experience of homelessness included: physical locations, repetition of recovery stories, individual readiness, and limited availability of appointments and treatments. Participants suggested creating services reflective of need and providing opportunities for choice and empowerment. They felt that community mental health and substance use support for people experiencing homelessness should ensure the support is personalised, responsive to need, inclusive, and trauma-informed.
3.3.6 Key points
- One of the most commonly highlighted barriers was the lack of integrated services to support both problem substance use and mental health needs. In many cases, accessing mental health support is dependent on abstaining from substance use, which particularly presents a barrier for those using substances as a means of coping with mental health concerns.
- Stigma and the variation in quality of care are widely reported as barriers to accessing services. There is a general consensus that effective care should be judgement free and reflect an awareness of specific individual needs above and beyond those relating to their mental health or substance use. The importance of continuity of care was highlighted.
- Some groups experience additional barriers to accessing services, including additional types stigma highlighted within some minority ethnic groups and for older substance users. Discrimination and a lack of inclusive services for LGBTI people and some minority ethnic groups are also noted.
- Heightened barriers were faced by people experiencing homelessness, which include increased stigma, fear of rejection faced when seeking support from services, varied interactions with frontline staff, limited availability of services and individual readiness to access services.
3.4 Recommended interventions
A number of interventions for co-occurring substance use and mental health concerns are recommended across the literature. These range from suggested approaches such as harm reduction and case management, to examples of specific interventions undertaken to improve staff knowledge of co-occurring substance use and mental health concerns, integration between services and outcomes for service users.
3.4.1 Person-centred and trauma-informed approaches
As highlighted above, person-centred approaches to care have significant benefits in supporting people with substance use and mental health concerns. Both academic and third sector literature echo this, and advocate for its implementation throughout mental health and substance use services. Trauma-informed approaches to care are also emphasised within the literature as being essential to providing person-centred support.
In 2015, the Revolving Doors Agency – a third sector organisation focused on the relationships between crime and unmet social and health care needs – published series of literature reviews[106] on severe and multiple disadvantage, which include concepts for recovery and desistance across the fields of mental health, substance use and criminology. It highlighted the need to focus on individual service users' journeys, which emphasise integrating personal meaning and agency into support and treatment services. As such, they advocated for service user involvement in the design of services and for greater peer and community support networks for individuals with co-occurring substance use and mental health concerns, arguing that eliminating discrimination, stigma and inequality will support people's journeys of recovery and desistance.
The need for non-discriminatory, comprehensive and needs-led approaches were also highlighted in a 2018 report[107] from the Royal College of Psychiatrists specifically focusing on older substance users. They advocated for services to share best practices as a means to achieve this. International reviews also highlighted the importance of viewing those accessing services as whole people with unique circumstances.[108]
Evidence also highlights the importance of trauma-informed approaches,[109] which acknowledges previous histories of adverse childhood experiences and trauma, and the impact they have on people accessing mental health and substance use services.[110] These approaches aim to recognise that people who use mental health and substance use services may have experienced trauma and that this may have an impact on them. Trauma-informed services aim to offer people the kind of relationships that promote recovery and do not cause further trauma or harm.[111] The need for trauma-informed care is highlighted by many sources,[112],[113],[114] and is also key to the Scottish Government Quality Principle and the MAT standards.[115],[116]
3.4.2 Staff training
There is a significant body of literature highlighting the role of training as a factor affecting staff attitudes, and inter-agency and interdisciplinary working. The 2006 Closing the Gap report[117] provides a framework for working effectively with people with co-occurring substance use and mental health concerns. The report suggests that one of the main issues leading to insufficient or poor responses to service users with co-occurring substance use and mental health concerns is the lack of skills and knowledge in the workforce to address their complex needs in an integrated and effective way. Other sources note that responsibility for many activities and service user groups is now being passed to lower graded staff who may not have benefited from professional training (such as housing support workers) because other higher-cost services have been withdrawn.[118]
Scottish and UK Government reports have also highlighted the role of training in enabling practitioners to work more effectively with people experiencing co-occurring substance use and mental health concerns.[119],[120] UK Government guidance[121] also states, however, that training in isolation will have limited benefits and that practice development and supervision are required to support staff in transferring their learning into practice. Practice development is also understood as a continuous journey of developing and innovating in care settings, so that patients, residents, families and the team engage with each other in person-centred ways.
A scoping review undertaken in 2020[122] explored the effect that the education and training nurses received had on the quality of service provided to patients with co-occurring substance use and mental health concerns. The authors argued that education could be used as an intervention to improve attitudes and increase confidence and knowledge, and that this had great promise in improving care and treatment outcomes for people with co-occurring substance use and mental health concerns. This is exemplified in Louie et al.'s 2018 research,[123] which explored the implementation of a multimodal training programme that was developed specifically to encourage an integrated service approach, and improve clinicians' capacity to identify and manage co-occurring substance use and mental health outcomes within drug and alcohol treatment settings. They concluded that services such as these could facilitate effective and integrated care for service users with multiple and complex needs.
Williams et al.[124] undertook research based on case note review of patients admitted to inpatient psychiatric wards in England, and suggested that training and support for clinicians and health service providers may help reduce inadvertent discrimination and improve care for this population. They noted that several studies have described the positive effects of targeted education to improve the knowledge and skills of professionals working with people with problem substance use.[125],[126] Additionally, other organisational support systems such as supervision and opportunities to consult with experts have also been shown to enhance knowledge and confidence among health professionals, contributing significantly to an increased willingness to engage in collaborative care with these service users.[127],[128]
However, while professional training can provide valuable skills in supporting services users with co-occurring substance use and mental health concerns, in some cases it can also foster a narrow response in the support provided. The 2011 review[129] by Revolving Doors sought to understand the poor frontline responses to adults with multiple needs and highlighted that a service user's concerns were often viewed in terms of a single frame of reference determined by the individual professional's training. As a result, a service user's other concurrent needs and the wider context influencing those needs were frequently ignored. This also had a negative effect on service user involvement. Williams[130] argued that integration of health and social care across organisations and sectors relies on the transfer of tacit knowledge between professional groups, with staff preferring learning from colleagues on an informal basis to more formally structured learning formats.
3.4.3 Service integration & networks
As highlighted in the previous sections, lack of service integration remains a barrier to accessing care as well as a key focus for policy makers.[131] This includes integration between mental health and substance use services, but also in many instances with wider physical health, housing and other social services.[132] The existing literature explores how service integration may be achieved in practice, either formally or informally.
The need for integration is also recurrent theme in both Scottish Government and UK Government policy recommendations,[133],[134] which include the development of integrated mental health and substance use teams,[135] as well as the mainstreaming of combined substance use and mental health care approaches.[136]
Several studies have identified "well networked services"[137] or "service linkages"[138] as core components of good practice when working with people with co-occurring substance use and mental health concerns or other multiple and complex needs. This suggests that services working with these service users may benefit from actively developing such linkages or networks, in particular where this is focused on shared learning to develop the knowledge and skill base of practitioners.
In a Scottish context, a 2019 report[139] from the Glasgow Centre for Population Health and NHS Greater Glasgow and Clyde highlighted the synergies and differences in the role and remit of organisations (including Police Scotland, Community Safety Glasgow and third-sector organisations) working with vulnerable people in Glasgow city centre. This included people experiencing homelessness and those who were at risk of poor health and substance use, with histories of trauma and complex needs. Organisations participating in the study acknowledged the need to act collaboratively and highlighted evidence that this approach was working and being further developed. However, the activities of organisations were mostly driven by their own primary remit, which was sometimes considered contradictory or not conducive to collaborative working. The report suggested widening the access that organisations had to each other's resources, systems and networks; which would in turn allow them to focus more of their own resources on active support.
Also explored was the role of communities of practice and professional networks as mechanisms to facilitate interdisciplinary and inter-agency collaboration and knowledge transfer, as well as to provide peer support and shared experiences. Anderson et al.[140] found that communities of practice provided a forum for peer support and supervision for mediating feelings of role or service isolation, and to sustain the motivation of those working with people with co-occurring substance use and mental health concerns, or other multiple and complex needs. They highlighted that while communities of practice can facilitate inter-disciplinary and inter-agency knowledge transfer, the limited resources available to local networks act as a barrier to developing their capacity to improve support for people with multiple and complex needs.
A 2012 systematic review[141] of empirical literature on health professional networks supports this conclusion. It identified several studies that suggest that positive networks within health organisations may increase health professionals' job satisfaction and resilience to job stressors and burnout. It concluded that establishing cohesive and collaborative networks of professionals or agencies may have a positive effect on care coordination, quality and safety. The review emphasised the need to understand the structure and characteristics of such networks and to attend to network functionality. The authors proposed that bridging divides is important for networks to improve quality and safety of care. Moreover, active development of links between professions and across other commonly occurring organisational divides was considered crucial for the development of larger and more resilient professional networks.
Manley et al.[142] considered co-occurring substance use and mental health concerns networks as one of a number of approaches taken to improve and develop the support provided by practitioners to these service users. They identified four good practice features of these networks:
- Provision of a model for multi-agency and multi-professional working which engenders understanding of issues within and between services and is able to resolve conflicting views regarding treatment;
- Sharing of good practice in a non-hierarchical environment;
- Promotion of cross-boundary networking, supervision and learning;
- Encouragement of service user and carer participation and collaboration.
An evaluation[143] of the UK's first network of practitioners involved in co-occurring substance use and mental health concerns in the North of England found that the majority of network members reported high levels of self-efficacy and confidence in engaging service users in both their problem substance use and mental health domains.
3.4.4 Support for people experiencing homelessness
A 2021 systematic "review of reviews"[144] investigated the effects of interventions in primary care, mental health and drug treatments for people who are homeless and who use drugs. Evidence was included from a range of interventions including specialist housing interventions, residential and community based programmes for people with co-occurring substance use and severe mental health concerns, case management (the provision of a single case manager responsible for linking users with multiple relevant services[145]), abstinence-based and harm reduction orientated substance treatment, healthcare interventions, peer support programmes, eating disorder interventions and sexual health promotion.
While the evidence was mixed; integrated care for people experiencing homelessness and problem substance use appeared to be associated with better outcomes. Harm reduction approaches, which include pragmatic interventions, policies, and programmes, but do not require a person to stop using drugs as a condition of support,[146] had positive effects on drug-related risks, overdose, and other substance use outcomes; as well as on hospital visits and admissions. Case management had positive effects on problem drug use, housing and mental health outcomes. Housing interventions – including Housing First, which offer individuals housing unconditionally as quickly as possible – were associated with improvements in physical health, but had little impact on problem drug use. Permanent supportive housing was effective in reducing mental health symptoms for people experiencing co-occurring substance use and severe mental health concerns. Assertive outreach was associated with positive physical and mental health outcomes for people with co-occurring substance use and severe mental health concerns. Overall, the review found that treatment approaches needed to be flexible, person-centred, supportive and integrated. In addition, a longer treatment duration was recommended in the literature reviewed, although the authors emphasised the need for more research into optimal treatment lengths and more qualitative insights from people experiencing or at risk of homelessness.
3.4.5 Youth substance use
The literature focusing on substance use amongst young people highlights this demographic as a specific area of concern, and makes distinct recommendations for prevention, treatment and management of problem substance use. Echoing recommendations for more joined-up approaches made more generally, research[147] highlights the need for this to be done to embed support for young people with co-occurring substance use and mental health concerns within a range of services, including housing agencies, mentoring programmes, social services and charitable organisations.
A study based on interviews conducted by peer researchers with participants aged between 16 and 20 in the North East of England[148] found that access to housing and social and mental health support were perceived as having the potential to prevent a worsening in an individual's circumstances with regard to problem substance use. Participants suggested that removing barriers to accessing support for mental health, housing and welfare and financial support could help with managing problem substance use and wider issues. They also felt that services should be judgement free and provided by staff who are educated about multiple complex needs and related adversity.
Research[149] based on a survey of UK academic and clinical experts in the field of youth substance use disorders tried to establish consensus for the prevention, treatment, and management of high-risk substance use and overdose among young people (aged 10 to 24 years old). Respondents agreed that screening in primary care and other clinical settings should be recommended for all young people. They also agreed that the needs and preferences of the service user should be central to the treatment and support provided, with the objective of reducing harm and mortality while promoting resilience and healthy development. The researchers felt that a continuum of care was needed, from lifestyle mentoring, harm reduction, and targeted prevention to early crisis response, with a clinical trajectory that addresses all major developmental challenges.
3.4.6 Key points
- Principles of person-centred care and trauma-informed approaches are highlighted across academic, third sector and policy literature.
- Research on interventions focuses heavily on the role of staff training, including to implement person-centred and trauma-informed approaches. The importance of diverse and integrated staff networks is emphasised as a way to support transfer of knowledge and development of practice.
- Literature highlights both formal and informal mechanisms for improving service integration across mental health services and substance use services.
- Harm reduction and case management approaches were found to have benefits for people experiencing homelessness. For young people using substances and experiencing mental health concerns, screening in primary care and other clinical setting was highlighted as being important, along with housing and welfare and financial supports.
Contact
Email: socialresearch@gov.scot