Primary care improvement plans - implementation progress summary: March 2021
Summary of the current progress towards implementation of the Memorandum of Understanding (MoU) between the Scottish Government, the SGPC, Integration Authorities and NHS Boards.
Primary Care Improvement Plans Summary of implementation progress at March 2021
1. Introduction
The 2018 GP Contract Offer ("the Contract Offer") and its associated Memorandum of Understanding ("MoU") between the Scottish Government (SG), the Scottish General Practitioners Committee of the British Medical Association (SGPC), Integration Authorities (IAs) and NHS Boards was a landmark in the reform of primary care in Scotland. The Contract Offer refocused the General Practitioner (GP) role as expert medical generalists to enable GPs to do the job they train to do and deliver better care for patients. It committed to a vision of general practice being at the heart of the healthcare system where multidisciplinary teams come together to inform, empower and deliver services in communities for those people in need of care. It recognised the statutory role of IAs in commissioning primary care services and service redesign to support the role of the GP as an expert medical generalist. It also recognised the role of NHS Boards in service delivery and as NHS staff employers, and parties to General Medical Services (GMS) contract.
In 2021 the MoU was refreshed (the MoU2) to cover the period 2021-2023 between the same Parties. The key aim remains expanding and enhancing multidisciplinary teams working to help support the role of GPs as expert medical generalists, to improve patient outcomes. The MoU Parties recognised a great deal has been achieved however there is still a way to go to fully deliver the GP Contract Offer commitments originally intended to be delivered by April 2021.
The original MoU sets out the six priority service areas where it has been agreed that IAs, in partnership with Health Boards and GPs, will focus:
- Vaccination Transformation Programme (VTP);
- Pharmacotherapy;
- Community Treatment and Care Services (CTAC);
- Urgent Care;
- Additional Professional Roles;
- Community Links Workers (CLW).
All of these services are currently available to patients, however in most cases these had historically been provided by individual GP practices. Following the joint SG/SGPC letter of December 2020, the focus for 2021-22 has been on Pharmacotherapy, CTAC and VTP services. More information about what these services include and the anticipated new models of delivery are provided in Section 4.2.
Funding to support the implementation of the MoU has been allocated to IAs through the Primary Care Improvement Fund (PCIF), and locally agreed Primary Care Improvement Plans (PCIPs) covering all 31 IA areas of Scotland were developed by the end of July 2018. The PCIPs set out in more detail how implementation of the six priority service areas will be achieved. IAs are required to provide updates on their PCIPs on an annual basis, and data on increases in workforce numbers and spread of services every six months through an agreed standard tracker template. The trackers also include space for free text comments to provide context to the data provided.
The delivery of primary care transformation is occurring within a complex local landscape. IAs must work closely with local communities and other stakeholders to ensure that PCIPs address specific local challenges and population need. They must also agree where the local priorities lie for the services being reformed. As a result of this, there is geographical variation in service design and delivery models.
The pace of service redesign has been impacted by the COVID-19 pandemic across all areas, with some services and recruitment paused during 2020. This included the reduction of appointment times, reduction to programme management capacity, restrictions to patient capacity and workforce reallocation. Many appointments shifted to telephone or Near me video consultations, with face-to-face appointments offered following telephone triage where necessary.
All IAs are now working on remobilisation of services, which includes implementation of the MoU.
This publication provides a national summary of the current progress towards implementation of the MoU, as submitted by IAs in May 2021 for the period up to the end of March 2021. The data at a local level is available in the spreadsheet accompanying this publication.
2. Workforce numbers
Table 1 shows the number of whole time equivalent staff who have been recruited to support to implementation of the six priority services agreed in the MoU. The tables do not include existing staff within NHS Boards or IAs who were delivering these services prior to the MoU.
The data returned shows that there has been a sustained increase in recruitment across all areas of the MoU. While increases in workforce may be indicative of progress towards delivery of the MoU, there is in general[1] no expectation of specific workforce levels which are required across Scotland. It should be recognised that there may be variation in appropriate staffing numbers depending on the clinical model developed, the skills mix of the workforce and local population needs.
| Year ending 31 March | 2018 | 2019 | 2020 | 2021 | |
|---|---|---|---|---|---|
| Pharmacotherapy | Pharmacist | 132.0 | 289.0 | 439.1 | 543.1 |
| Pharmacy Technician | 38.4 | 87.9 | 169.1 | 248.6 | |
| Vaccinations / Community Treatment and Care Services | Nursing | 24.7 | 77.2 | 232.3 | 401.9 |
| Healthcare Assistants | 13.7 | 107.6 | 193.0 | 305.5 | |
| Other [a] | 2.0 | 38.7 | 63.1 | 92.2 | |
| Urgent Care (advanced practitioners) | Advanced Nurse Practitioners | 18.0 | 67.0 | 129.6 | 202.5 |
| Advanced Paramedics | 3.1 | 11.1 | 13.6 | 14.4 | |
| Other [a] | 2.6 | 13.5 | 22.6 | 37.7 | |
| Additional professional roles | Mental Health workers | 13.9 | 53.6 | 102.7 | 215.7 |
| Musculoskeletal Physiotherapists | 11.1 | 46.2 | 114.5 | 169.5 | |
| Other [a] | 2.2 | 19.7 | 41.0 | 43.2 | |
| Community link workers | 51.4 | 98.6 | 165.6 | 189.3 | |
| Total Staff Recruited | 313.1 | 910.1 | 1686.1 | 2463.4 | |
(a) including but not limited to: midwives; community mental health nurses; out of hours staff; programme managers; administrative support.
Many areas reported in their tracker returns that the pace of recruitment has been impacted by the COVID-19 pandemic across all MoU areas, with pauses in recruitment lasting 4-6 months. Following this, many Multi-Disciplinary Team (MDT) members were redeployed to support the pandemic response and vaccine roll-out, directing resources away from services listed in the MoU. Most services are now back into remobilisation phase with recruitment complete or underway.
3. NHS Board provided services
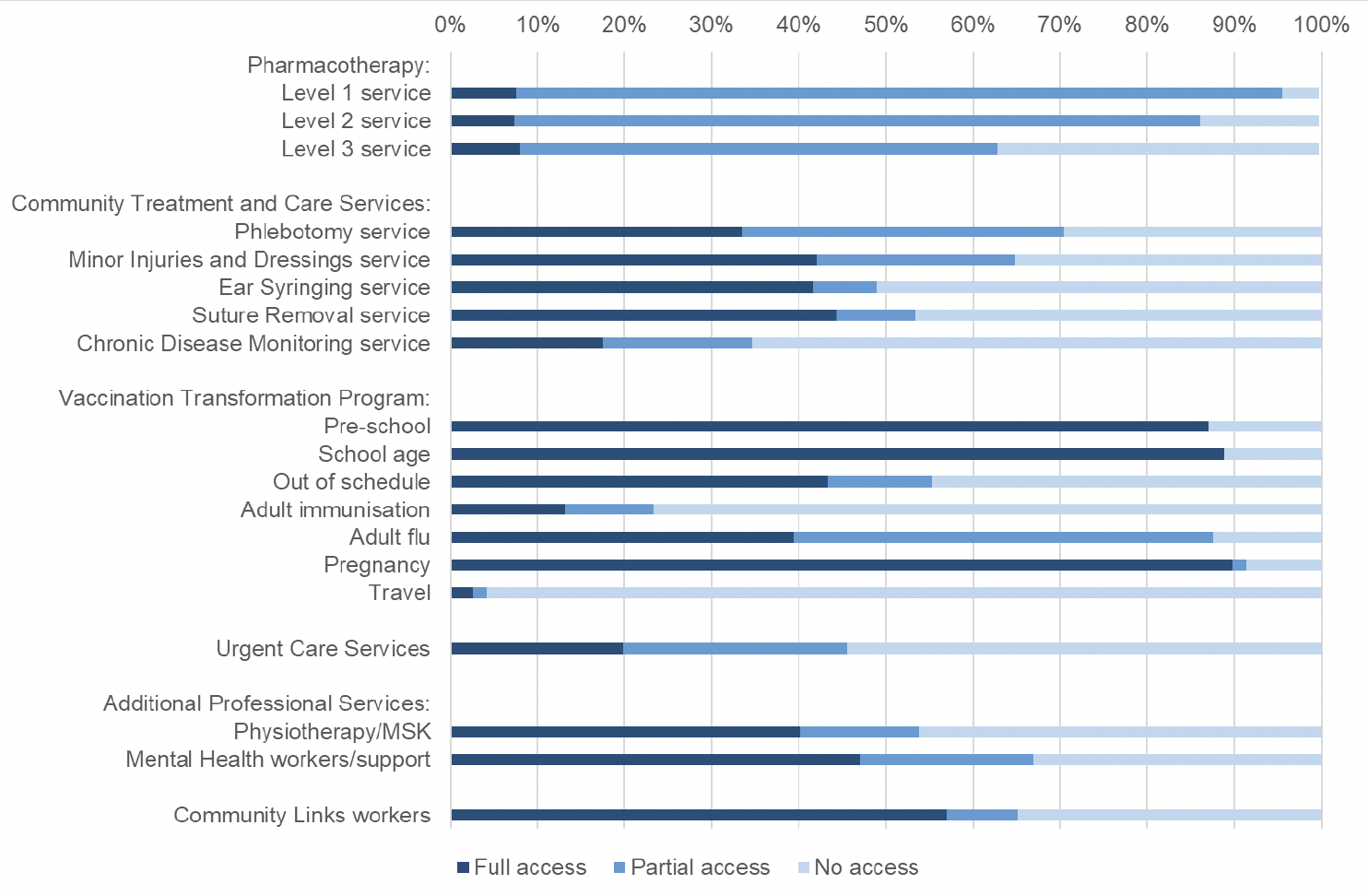
The additional staff described in section 2 above enable NHS Boards to provide an increased range of services, in accordance with the MoU. All of these services are currently available to patients, however in most cases these had historically been provided by individual GP practices. Chart 1 illustrates the percentage of GP practices whose patients can now access these services directly from their NHS Board.
It is not expected that all GP practices in Scotland will take up these NHS Board provided services. Because service delivery models are designed specifically according to local population needs, there are variations in approach across the country. For example, there may be some GP Practices where there is no defined need for a particular professional role (such as Community Links Workers) and the list of CTAC's services is not prescriptive. These services may therefore never reach 100% coverage. There may also be local circumstances where local Primary Care Improvement Programme Boards determine it is necessary for one or more local GP practices to continue delivering one or more services intended to transfer to board-employed MDT under the MoU.
The majority of practices have at least partial access to NHS Board provided pharmacotherapy services, with 8 per cent having full access and 88 per cent partial access to level 1 services at March 2021.
Around a third of practices had full access for most of the CTAC services listed, as at March 2021. 17 per cent had full access to Chronic Disease Monitoring.
The VTP workstream was delayed for one year to focus on COVID-19 vaccination and seasonal flu vaccinations. The roll out of pre-school, school age and pregnancy vaccinations are relatively well advanced, with services in place for nearly 90 per cent of practices. There is currently lower coverage for adult immunisation, with 13 per cent of practices having full access to this service. Some areas reported that full transfer of all vaccinations to NHS Boards was not appropriate e.g. for the vulnerable and elderly. Most areas are operating a blended model of GP and NHS Board delivery, with community nurses, pharmacies, schools and maternity wards all playing an important role.
Twenty per cent of practices are fully supported with urgent care services, and a further 26 per cent have partial access to this service.
Forty per cent of practices currently have full access to a musculoskeletal physiotherapist and 47 per cent have full access to a mental health worker. 57 per cent of practices have full access to a community links worker, whose services are not intended to be universal but allocated on the basis of need.
4. Background notes
4.1 Data quality
The data included in this report is provided by IAs. Information on workforce numbers is sourced from local systems which are dynamic and primarily used for operational purposes. The data can therefore change over time and the figures presented here are the best available estimate. The Scottish Government is working with IAs to improve data quality and previously published information may change from one publication to the next to reflect these refinements.
4.2 Definitions
The services included in the MoU are defined as follows. As indicated above, there may be geographical and other limitations to the extent of any service redesign and local needs which need to be determined as part of the PCIP.
Vaccination Transformation Programme The Vaccination Transformation Programme was announced in March 2017 to review and transform vaccine delivery in light of the increasing complexity of vaccination programmes in recent years, and to reflect the changing roles of those historically tasked with delivering vaccinations.
IAs have delivered phased service change based on locally agreed plans as part of the PCIP to meet a number of nationally determined outcomes including shifting of work to other appropriate professionals and away from GPs. This has already happened in many parts of the NHS system across Scotland for Childhood Immunisations and Vaccinations. In October 2021, regulation change removed vaccinations from the GMS contract.
Pharmacotherapy These services are in three tiers divided into core and additional activities, to be implemented in a phased approach.
In 2021, phase one included activities at a general level of pharmacy practice including acute and repeat prescribing and medication management activities. This is to be followed by phases two (advanced) and three (specialist) which are additional services and describe a progressively advanced specialist clinical pharmacist role.
Regulations will be amended by Scottish Government in early 2022 so that NHS Boards are responsible for providing a pharmacotherapy service to patients and practices by April 2022. The use of medicines to treat and care for patients will remain an important part of GP work. The delivery of electronic prescribing is an essential requirement for all involved in prescribing, which will be prioritised by the ePharmacy Programme Board, supported by National Services Scotland and the NES Digital Service.
Community Treatment and Care Services These services include, but are not limited to, basic disease data collection and biometrics (such as blood pressure), chronic disease monitoring, the management of minor injuries and dressings, phlebotomy, ear care, suture removal, and some types of minor surgery as locally determined as being appropriate.
Scottish Government are currently in the process of drafting regulations for the delivery of CTAC Services so that Boards are responsible for providing a Community Treatment and Care service from April 2022. These services will be designed locally, taking into account local population health needs, existing community services as well as what brings the most benefit to practices and patients.
Urgent Care These services provide support for urgent unscheduled care within primary care, such as providing advance practitioner resource (a nurse or paramedic) for GP clusters and practices as first response for home visits, and responding to urgent call outs for patients, working with practices to provide appropriate care to patients, allowing GPs to better manage and free up their time for more complex cases.
The Scottish Government will make regulations so that Boards are responsible for providing an Urgent Care service from 2023-24. Evidence from the Primary Care Improvement Plans suggests there is variation in how this service is being delivered. Further guidance will be provided by the National GMS Oversight Group on delivery of this commitment in advance of April 2022. Consideration in particular will be given to how this commitment fits into the wider system Redesign of Urgent Care work currently in progress.
Additional Professional Roles Additional professional roles will provide services for groups of patients with specific needs that can be delivered by other professionals as first point of contact in the practice and/or community setting (as part of the wider MDT). These roles could include, but are not limited to:
- Musculoskeletal focused physiotherapy services
- Community clinical mental health professionals (e.g. nurses, occupational therapists) based in general practice.
Specialist professionals will work within the local MDT to see patients at the first point of contact, as well as assessing, diagnosing and delivering treatment, as agreed with GPs and within an agreed model or system of care. Service configuration may vary dependent upon local geography, demographics and demand.
MoU Parties will consider how best to develop the additional professional roles element of the MoU. In particular with Mental Health, there is a need to consider how PCIF funded posts interface with Action 15 funded posts as well as new policy commitments for mental health. The Primary Care Mental Health Development group in Scottish Government is taking this consideration forward. Separate to this MoU and the arrangements in place to fund it, the commitment of additional Mental Health Link Workers is currently being considered in the context of the locally led model proposed by the Mental Health in Primary Care Short Life Working Group.
Note that the numbers presented in these tables include Mental Health workers funded through PCIF as well as those funded through other routes. The numbers presented here may be different from those published in the Mental Health worker quarterly performance reports, which focuses on recruitment through Action 15 of the Mental Health Strategy.
Community Links Worker is a generalist practitioner based in or aligned to a GP practice or Cluster who works directly with patients to help them navigate and engage with wider services, often serving a socio-economically deprived community or assisting patients who need support because of (for example) the complexity of their conditions or rurality. The roles of the CLWs will be consistent with assessed local need and priorities and function as part of the local models/systems of care and support. Consideration will be given by April 2022 as to how the Link Worker workforce interfaces with the Scottish Government's commitment to delivering 1,000 Mental Health Link Workers by the end of this Parliament.
Spread of Services have been categorised by IAs as: GP practices having full access; partial access; or no access. These definitions have been locally determined. Work is underway to provide clarity on expectations and consistency of reporting.
5. Contact
For more information or queries on the information presented here please contact the Primary Care Policy Team at PCImplementation@gov.scot
Contact
Email: PCImplementation@gov.scot