The Scottish Health Survey 2021 - volume 1: main report
Presents results for the Scottish Health Survey 2021, providing information on the health and factors relating to health of people living in Scotland.
This document is part of 2 collections
Chapter 3 Respiratory Conditions Including COVID-19
Chapter Summary
Among all adults in 2021:
- 16% reported that they had doctor-diagnosed asthma
- 14% reported having wheezed in the last 12 months, lowest in the time series
- 26% reported ever having wheezed
Among all children in 2021:
- 9% reported that they had doctor-diagnosed asthma
- 11% reported having wheezed in the last 12 months
- 20% reported ever having wheezed
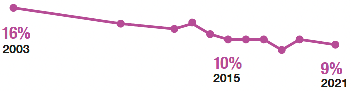
The prevalence of doctor-diagnosed asthma in children has decreased since 2003.
Boys were more likely to have doctor-diagnosed asthma than girls in 2021.
- 11% boys
- 6% girls
While prevalence of doctor-diagnosed asthma in adults did not vary significantly by deprivation in 2021, wheezing in the last 12 months was more common in more deprived areas.
In 2021, doctor-diagnosed chronic obstructive pulmonary disease increased with age.
In 2021:
- 5% of all adults reported having long COVID
The proportion of adults who reported having long COVID differed with age.
- 1% of adults reported that long COVID limited their activities a lot
The most common symptoms of long COVID amongst adults were:
In 2021, the vast majority of adults reported that they had or were willing to take up the COVID vaccine, while a few said that they were not and the least that they were unsure or preferred not to say.
- 96% willing
- 3% not willing
- <0.5% unsure or preferred not to say
In 2021, the most common reasons for not taking up the COVID vaccine were:
- 43% 'I need more information about the safety of the vaccines'
- 33% 'I'm concerned about how quickly the vaccines have been approved'
- 28% 'I'm concerned about how quickly the vaccines have been developed'
- 24% 'I don't think COVID would be a serious illness for me'
In 2021, mental wellbeing was lower amongst adults with long COVID compared with those who did not have long COVID.
- Mean WEMWBS3 score of 44.7 with long COVID
- Mean WEMWBS3 score of 48.8 without long COVID
Mental wellbeing was also lower in 2021 amongst adults who had been advised to shield compared with those who had not.
- Mean WEMWBS3 score of 47.1 had been advised to shield
- Mean WEMWBS3 score of 48.8 had not been advised to shield
1 - no observations (zero value)
2 0 non-zero values of less than 0.5% and thus rounded to zero
3 WEMWBS scores range from 14 to 70. Higher scores indicate greater wellbeing.
Respiratory Conditions including COVID-19
Rachel Whitford
3.1 Introduction
Infectious respiratory disorders and long-term respiratory conditions, such as asthma and chronic obstructive pulmonary disease (COPD), are a considerable challenge for the individuals that live with them and for health services in Scotland. These respiratory conditions are currently incurable, with particular concerns about asthma over- and under-diagnosis.[1],[2],[3]
The UK has one of the highest rates of asthma in the world.[4],[5] This illness is characterised by variable and recurring symptoms of breathlessness, wheezing, coughing and chest tightness. Around 1 in 14 people in Scotland are currently receiving treatment for asthma, a fifth of whom are children.[6] The reasons for the high prevalence of asthma in the UK are not certain; however, the risk factors identified include environmental (house dust mites, pollen, animals, specific foods, viral infections, moulds, fungi, environmental tobacco smoke and air pollutants) and genetic disposition, obesity, and lifestyle/stage (diet, drug use, caesarean sections, and breastfeeding).[7] Occupational exposure also accounts for around 10% of cases of adult-onset asthma.[8]
The prevalence of COPD means that it is now the third leading cause of mortality worldwide.[9] Not only does this reinforce the importance of monitoring and, where possible, tackling the causes and symptoms of this condition, the ageing population along with the additional complication of older COPD patients being more likely to have other long-term conditions presents a further challenge in managing COPD.[10] Due to Scotland's health inequalities, the associations of long-term conditions like COPD with deprivation, lifestyle risk factors and wider social health determinants are increasingly important.[11] Smoking is the main cause of COPD with up to 25% of long-term smokers estimated to develop COPD and an estimated 8 out of 10 of those with the condition having either smoked or continue to smoke.[12] This smoking associated risk is higher for women compared to men.[13]
Over the last two years, there has been an increase in public and clinical awareness of the longer-term effects of COVID-19 infection usually referred to as long COVID or post-COVID-19 syndrome. The overlapping long COVID symptoms sometimes experienced can affect body systems including the respiratory system. Recent evidence suggests that a sizeable proportion of people who report to have long COVID have long-term rehabilitation and support needs.[14]
3.1.1 Policy background
The Respiratory care – action plan: 2021 to 2026[15] sets out the vision for improvement in the prevention, diagnosis, care, treatment and support of people living with respiratory conditions. This is supported by other key policy initiatives including the Scottish Access Collaborative & Modernising Patient Pathways Programme, which aims to improve patient journeys through sustainable changes that facilitate person-centred care and the Framework for supporting people through Recovery and Rehabilitation during and after the COVID-19 Pandemic.[16]
One of the Scottish Government's National Performance Framework National Outcomes is for people in Scotland to 'live longer, healthier lives',[17] which includes a National Performance Indicator to 'reduce premature mortality' (deaths from all causes in those aged under 75).[18]
Within the Scottish Government National Indicators, health risk behaviours linked to respiratory disease, including smoking, harmful drinking, low physical activity and obesity, are monitored against an outcome of reducing the percentage of adults exhibiting two or more of these behaviours.[19]
In September 2021, the Scottish Government published Scotland's Long COVID-19 Service[20] paper. The paper sets out the key elements that underpin the approach to care and support for people with long COVID.
The Scottish Government's approach is based on four key elements: supported self-management, primary and community-based support, rehabilitation support and secondary care investigation and support.
A long COVID Strategic Network has been established and brings together clinical experts, NHS Boards, third sector organisations and those with lived experience to guide, plan and design the ongoing care for people living with long COVID.
The Scottish Government consider it vital for the COVID-19 vaccination programme to reach everyone and that no one is left behind, both for individual health and our collective community wellbeing.
A range of outreach activities and partnerships with community and third sector organisations, and frontline local authority staff have supported the building of trust and enabled the removal of barriers for people who might not otherwise take up the vaccination offer. For example, vaccinating at community venues, places of worship and food banks. Recent research commissioned by Scottish Government shows that having a local and more flexible service is welcome.[21]
Mobile outreach units have been provided by the Scottish Ambulance Service (SAS) and some Health Boards partnered with local transport providers to use their vehicles to go into community settings. Pop-up and drop-in clinics were used across the country for those who are unable to access the mass vaccination clinics. Local communities were often consulted on the location of mobile clinics.
3.1.2 Reporting on respiratory conditions including COVID-19 in the Scottish Health Survey
This chapter updates trend data on adults' self-reported doctor-diagnosed asthma, COPD prevalence, and respiratory symptoms (wheezing). Data on long COVID prevalence, symptoms and impact on daily life and mental wellbeing (measured with WEMWBS – Warwick-Edinburgh Mental Wellbeing Scale) are reported as well as figures on reasons for not taking up the offer of the COVID-19 vaccination.
The area deprivation data are presented in Scottish Index of Multiple Deprivation (SIMD) quintiles. To ensure that the comparisons presented are not confounded by the different age profiles of the quintiles, the data have been age-standardised. For a detailed description of both SIMD and age-standardisation as well as definitions of other terminology used in this chapter and for details on the data collection methods for respiratory conditions and long COVID, please refer to Chapter 2 of the Scottish Health Survey 2021 - volume 2: technical report.
Supplementary tables on respiratory conditions including COVID-19 are also published on the Scottish Government website: Scottish Health Survey.
3.2 Respiratory Conditions Including COVID-19
3.2.1 Doctor-diagnosed asthma, wheezed in the last 12 months, and ever wheezed, 2003 to 2021, by age and sex
Adults
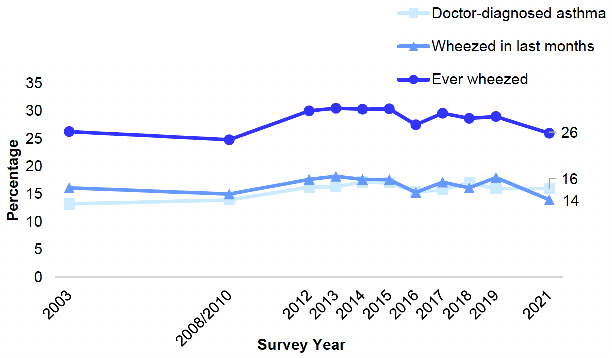
Doctor-diagnosed asthma of adults increased over time from 13% in 2003 to 16% in 2021 but has remained relatively stable since 2012 (16%). A similar pattern was observed for both women and men during this time. While there was a difference in the proportion of men and women who had doctor-diagnosed asthma in 2021, it was not statistically significant (15% and 17% respectively).
In 2021, the proportion of adults who had wheezed in the last 12 months was 14%, the lowest proportion since the time series began in 2003. Before 2021, the proportion of adults who had wheezed in the last 12 months fluctuated between 15% and 18% since 2003. Men followed the same pattern, seeing the lowest prevalence rate in 2021 (12%) since the time series began, which was also a five-percentage point decrease since 2019. In 2021, the proportion of women who had wheezed in the last 12 months (16%) was more reflective of previous survey years, with prevalence ranging between 15% and 19% since 2003.
In 2021, the proportion of adults who had ever wheezed was 26% (28% of women and 25% of men). This proportion was consistent with previous years in the time series, with prevalence remaining between 25% and 31% since 2003. Figure 3A, Table 3.1
Children
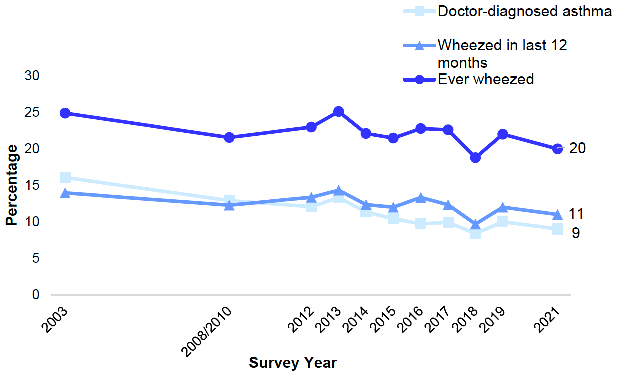
In 2021, the prevalence of doctor-diagnosed asthma among children (aged 0-15) was 9%. The proportion of children diagnosed with asthma has almost halved since 2003 (16%), but prevalence has remained relatively stable since 2015 (10%). Boys were significantly more likely than girls to have doctor-diagnosed asthma in 2021 (11% compared with 6%).
The proportion of children who had wheezed in the last 12 months in 2021 was 11%. This was consistent with previous years in the time series, with proportions of children who had wheezed in the last 12 months fluctuating between 10% and 14% since 2003.
In 2021, 20% of children had ever wheezed, a figure which had not changed significantly since 2003 (fluctuating between 25% and 19%). Prevalence of boys ever having wheezed in 2021 was 22%, not significantly different from the 18% of girls. Figure 3B, Table 3.1
3.2.2 Doctor-diagnosed asthma, wheezed in last 12 months, and ever wheezed (age-standardised), 2021, by area deprivation and sex
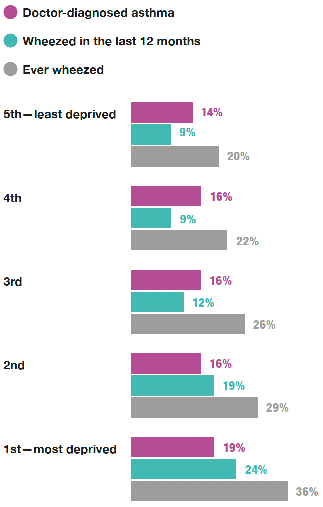
In 2021, prevalence of doctor-diagnosed asthma did not vary significantly by levels of area deprivation. Proportions of age-standardised doctor-diagnosed asthma were between 14% and 19% in each of the SIMD quintiles.
There was, however, a significant difference in the proportion of adults who had wheezed in the last 12 months by level of deprivation, with 24% of those in the most deprived areas and 9% of those in the least deprived areas reporting this in 2021. Figure 3C, Table 3.2
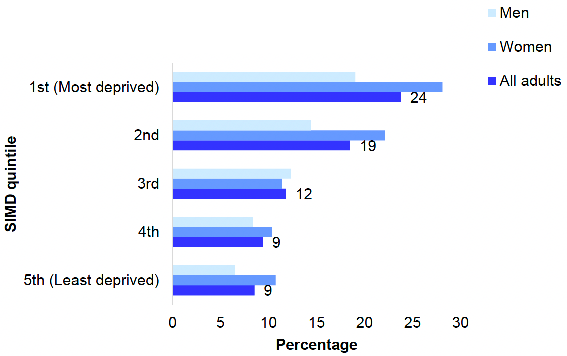
In 2021, the proportion of those who had ever wheezed also varied significantly by SIMD quintile. The proportion of adults who had ever wheezed increased with deprivation (20% in the least deprived areas compared with 36% in the most deprived areas). There were no significant differences between men and women by areas of deprivation. Table 3.2
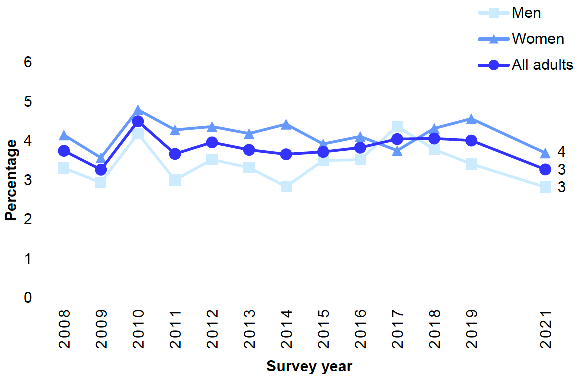
3.2.3 Doctor-diagnosed COPD, 2008 to 2021, by sex
The proportion of adults with doctor-diagnosed COPD was 3% in 2021 which was not significantly different from the stable trend of 4% since 2011.
For most years since 2008, prevalence of COPD has been slightly higher for women than for men, but not significantly so. In 2021, 4% of women and 3% of men reported having doctor-diagnosed COPD. Figure 3D, Table 3.3
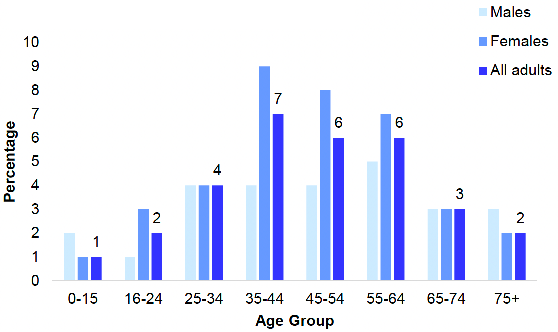
3.2.4 Doctor-diagnosed COPD, 2021, by age and sex
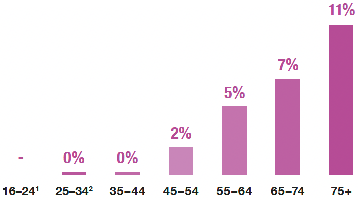
In 2021, the proportion of those with a diagnosis of COPD increased with age. Around one in ten (11%) of those aged 75 and above had doctor-diagnosed COPD, compared with less than 0.5% of those aged 16-44. A similar pattern was observed for both men and women. Table 3.4
3.2.5 Whether has long COVID and whether limiting ability to carry out day-to-day activities due to long COVID, 2021, by age and sex
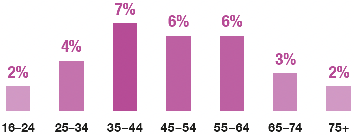
In 2021, one in 20 people (5%) reported having symptoms of long COVID at least four weeks after first developing COVID-19. The proportion of those who had long COVID was highest amongst those aged 35-64 (6 - 7%). Prevalence was lowest amongst the youngest and oldest age groups (1% of children, 2% of those aged 16-24 and 2% of those aged 75+). Women were slightly more likely than men to experience symptoms of long COVID (5% of women compared with 4% of men). Figure 3E, Table 3.5
One per cent of adults reported that long COVID limited their activities a lot. Women were slightly more likely than men to report that they had symptoms of long COVID which limited their activities a lot (2% and 1% respectively). Table 3.5
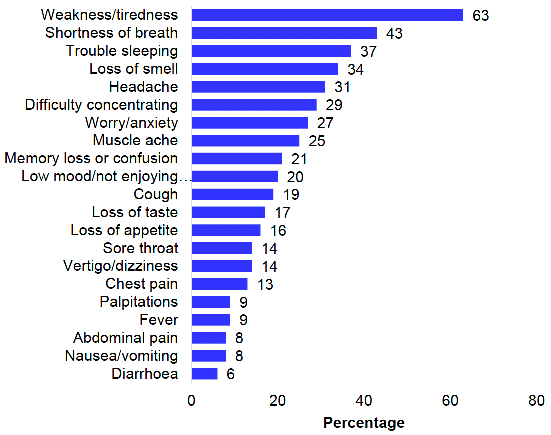
3.2.6 Long COVID symptoms, 2021, by age and sex
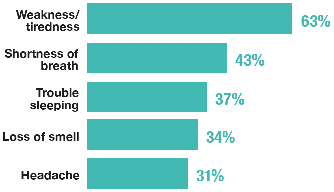
In 2021, the most common symptom amongst adults who were experiencing long COVID was 'weakness / tiredness', with 63% of those with long COVID reporting this. This was followed by 'shortness of breath' (43%), 'trouble sleeping' (37%), 'loss of smell' (34%), 'headache' (31%), 'difficulty concentrating' (29%) and 'worry / anxiety' (27%). Figure 3F, Table 3.6
3.2.7 Whether have had or would be willing to have the COVID-19 vaccine, 2021, by age and sex
In 2021, the vast majority of adults (96%) reported that they had or were willing to take up the COVID-19 vaccine, while 3% said that they were not and less than 0.5% that they were unsure or preferred not to say. There were no significant differences between men and women.
Willingness to take up the COVID-19 vaccine varied significantly by age. Those aged 16-44 were most likely to be unwilling to take up the COVID-19 vaccine (5%) compared with 1% of those aged 65 and over. Table 3.7
3.2.8 Reasons for not taking up COVID-19 vaccine, 2021, by age and sex
Adults who had not taken up the COVID-19 vaccine, or who said they were unsure or unlikely to do so when offered one, were asked the reason why. In 2021, the most common reasons for not taking up the COVID-19 vaccine were:
- 'I need more information about the safety of the vaccines' (43%);
- 'I'm concerned about how quickly the vaccines have been approved' (33%);
- 'I'm concerned about how quickly the vaccines have been developed' (28%);
- 'I don't think COVID-19 would be a serious illness for me' (24%);
- 'I am concerned about having an allergic reaction, even though I do not have a medical history of allergies' (22%); and
- 'I have heard that some people don't feel well after being vaccinated' (18%)
Table 3.8
3.2.9 Adult WEMWBS mean score (age-standardised), 2021, by whether had COVID-19/long COVID and sex
In 2021, mental wellbeing was not significantly associated with ever having had COVID-19. The mean WEMWBS score (age-standardised) for adults who had had COVID-19 was 48.1 compared with 48.7 for those who had not had COVID-19.
The mean WEMWBS score for those with long COVID, however, was 44.7 compared with 48.8 for those who did not have long COVID, indicating significantly lower mental wellbeing for those with long COVID. Table 3.9
3.2.10 Adult WEMWBS mean score (age-standardised), 2021, by whether received a letter that advised to shield and sex
In 2021, those who had received a letter or text advising them to shield during the COVID-19 pandemic tended to have lower mental wellbeing than those who had not (WEMWBS score of 47.1 and 48.8 respectively). Table 3.10
Table list
Table 3.1 Doctor-diagnosed asthma, wheezed in last 12 months, and ever wheezed, 2003 to 2021, by age and sex
Table 3.2 Doctor-diagnosed asthma, wheezed in last 12 months, and ever wheezed (age-standardised), 2021, by area deprivation and sex
Table 3.3 Doctor-diagnosed COPD, 2008 to 2021, by sex
Table 3.4 Doctor-diagnosed COPD, 2021, by age and sex
Table 3.5 Whether has long COVID and whether limiting ability to carry out day-to-day activities due to long COVID, 2021, by age and sex
Table 3.6 Long COVID symptoms, 2021, by age and sex
Table 3.7 Whether have had or would be willing to have the COVID-19 vaccine, 2021, by age and sex
Table 3.8 Reasons for not taking up COVID-19 vaccine, 2021, by age and sex
Table 3.9 Adult WEMWBS mean score (age-standardised), 2021, by whether had COVID-19/long COVID and sex
Table 3.10 Adult WEMWBS mean score (age-standardised), 2021, by whether received a letter that advised to shield by sex
The tables can be found on the main report page under supporting files.
References and notes
1. See Asthma: key points.
2. See Chronic obstructive pulmonary disease (COPD): key points.
3. See Asthma 'over-diagnosed and trivialised'.
4. To, T, Stanojevic, S, Moores, G, Gershon A S , Bateman, E, Cruz, A A, Boulet L-P (2012). Global asthma prevalence in adults: findings from the cross-sectional world health survey.
5. Beasley, R (1998). Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis and atopic eczema: ISAAC. The Lancet; 351(9111): 1225-32.
6. See Asthma deaths in Scotland highest this century.
7. See Asthma: risk factors.
8. See Occupational asthma.
9. See Chronic obstructive pulmonary disease (COPD).
10. Chronic Obstructive Pulmonary Disease (COPD): best practice guide. Edinburgh, Scottish Government, 2017.
11. See Impact of deprivation on health.
12. See COPD.
13. See Chronic obstructive pulmonary disease (COPD): key points.
14. Respiratory care – action plan: 2021 to 2026. Edinburgh, Scottish Government, 2021.
15. Respiratory care – action plan: 2021 to 2026. Edinburgh, Scottish Government, 2021.
16. Framework for reporting people through Recovery and Rehabilitation during and after the COVID-19 Pandemic. Edinburgh, Scottish Government. 2020.
17. See National Performance Framework.
18. See National Indicator Performance.
19. See National Indicator Performance.
20. Scotland's Long COVID Service.
21. See Coronavirus (COVID-19) and flu vaccination programme: user journeys and experiences.
Contact
There is a problem
Thanks for your feedback