Health and Care (Staffing) (Scotland) Act 2019 - draft statutory guidance: consultation
This consultation is on the statutory guidance that will be issued by the Scottish Ministers to accompany the Health and Care (Staffing) (Scotland) Act 2019. The guidance will support relevant organisations in meeting requirements placed on them by the Act and relevant secondary legislation.
12. Common Staffing Method
12.1 Which sections of the Act is this chapter about?
This chapter provides further detail on the following sections of the 1978 Act, each of which are inserted by section 4 of the Act:
section 12IJ: Duty to follow the common staffing method (referred to in the text as the "section 12IJ duty");
section 12IK: Common staffing method: types of health care; and
section 12IL: Training and consultation of staff.
A link to the Act can be found here. There are other links to useful information, including to other chapters of the guidance, embedded in this chapter; these are denoted in blue text.
12.2 Who does this chapter apply to?
The following organisations must comply with the duties contained in this chapter:
- All geographical Health Boards;
- NHS National Services Scotland (referred to in the Act as the 'Agency'),
- Special Health Boards who deliver direct patient care, i.e., NHS 24, the Scottish Ambulance Service Board, the State Hospital Board and the National Waiting Times Centre Board.
These are referred to as "relevant organisations" in this chapter.
12.3 In what settings and to which staff does this chapter apply?
Unlike other sections of the Act, the sections regarding use of the CSM only apply to the types of health care provided at the locations and by the kinds of employees listed in section 12IK. Relevant organisations must apply the CSM where they operate health care services described in 12IK and are required to report on this internally in (as a minimum) quarterly reports under section 12IF Duty to seek clinical advice on staffing and in their annual reports to the Scottish Ministers under section 12IM Reporting on staffing. The types of health care, locations and employees stated in 12IK align with the current availability of a speciality-specific staffing level tool since the use of such a tool is an integral part of the CSM. It is noted, however, that for those types of health care, locations and employees that are not currently listed in section 12IK, and therefore are not required to apply the CSM, relevant organisations will still have to ensure appropriate levels of staffing in order to comply with the section 12IA duty.
The Act allows the Scottish Ministers to amend the list in section 12IK to add, remove or change the description of a type of health care, the location where it is provided and the kind of employees who provide it, thereby adding, removing or changing those services required to apply the CSM. It is currently the intention that services covered by the CSM will be expanded in the future, as more staffing level tools are developed. However, any amendments to section 12IK of the Act will require secondary legislation to be enacted and until this happens, application of the CSM to services other than those listed in section 12IK is not mandatory. It is therefore possible that a service may have developed, and be using, a speciality-specific staffing level tool but would not be required to apply the CSM.
For those types of health care, locations and employees that are not currently listed in section 12IK, and therefore are not required by the Act to apply the CSM, the various components of the CSM may still be useful in planning appropriate staffing. There is no reason why the various aspects of the CSM cannot be used in any health care service where deemed beneficial. For example, a service may not have a speciality-specific staffing level tool available but may still find it useful to use the professional judgement tool, consider measures of quality, local context and current and funded staffing, along with comments made by patients and staff, when determining appropriate staffing. For the avoidance of doubt however, use of the CSM outside the services listed in section 12IK is not mandatory and will not be reported on in annual reports to the Scottish Ministers under section 12IM (Reporting on staffing).
The types of employees covered by the CSM in section 12IK includes all grades / bands and it is important to note that the Act makes it clear that in the application of the CSM, references to registered nurses, midwives and medical practitioners include other individuals providing care for patients and acting under their supervision or discharging duties delegated by them. This means health care support staff who support delivery of the types of services covered by the CSM are included in the requirements.
Individuals who are engaged in a course of studies in order to be admitted to the register of members maintained by the Nursing and Midwifery Council under section 60 of the Health Act 1999 or the register of medical practitioners maintained by the General Medical Council under section 2 of the Medical Act 1983 (with the exception of persons who are already provisionally registered under section 15 of that Act) are specifically excluded from the "employees" listed in 12IK. This means that these excluded groups must be supernumerary to the number of staff required to deliver care. Students are in clinical areas in a learning capacity, not to support the delivery of the service and may in fact add to the workload of staff who are directly involved in their supervision and learning. This exclusion does not extend to positions such as apprentices and 'earn and learn' models.
Accountability for all the duties covered in this chapter remains with the relevant organisation and not with individuals who may be charged with carrying out certain actions.
12.4 What is this chapter about?
This chapter is about the use of the CSM to help determine what changes (if any) are needed to the "staffing establishment" and / or the way in which a particular type of health care / location provides its services.
The purpose of the CSM is to ensure a consistent approach to decision-making across NHS Scotland which:
- uses all available evidence within the context in which the service is being delivered;
- ensures that clinical advice is sought and had regard to; and
- ensures that any risk associated with staffing is identified and mitigated as far as possible when determining staffing requirements, with a clear escalation process in line with the section 12ID Duty to have risk escalation process in place.
The use of staffing level and professional judgement tools is a key component of the CSM. The appropriate tools to use and the frequency at which the CSM should be used in relevant areas are defined in Regulations.
12.5 What is the common staffing method?
The CSM is illustrated in figure 1 below:
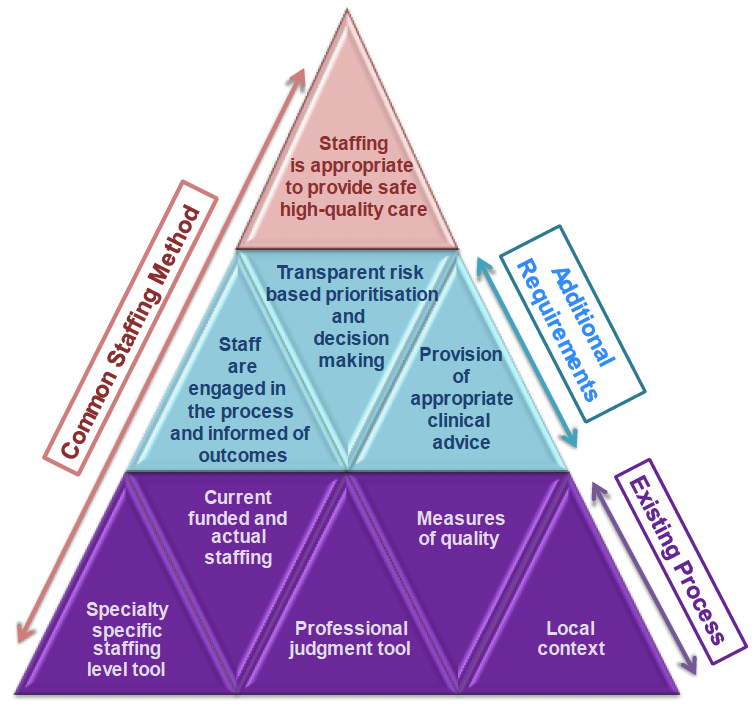
The CSM sets out a process, including the use of speciality-specific staffing level and professional judgement tools and a range of other considerations, which must be applied rigorously and consistently. The application of the CSM will support relevant organisations to ensure appropriate staffing for the health, wellbeing and safety of patients and the provision of safe and high-quality care. It will form part of the evidence that relevant organisations submit to demonstrate how they have complied with the Act. Section 12IK lists each type of health care that is covered by the CSM. For each type of health care covered, the Act specifies for which employees and in which locations the CSM must be used.
The CSM is composed of a number of parts that should be used together to make staffing decisions. Staff at all levels should be engaged in the CSM and there should be a culture of decision-making based on a shared understanding of the workload and the need to balance quality of care, staffing, and other resource considerations. As with all parts of the Act, the CSM needs to be applied alongside the guiding principles and the section 12IA Duty to ensure appropriate staffing.
12.6 Do I have to use the common staffing method?
Section 12IK of the Act lays out in table format the types of health care, the locations and the employees for which the CSM must be applied. The CSM should be applied in each setting that falls within the definitions in this table. As explained earlier in this chapter, the CSM can be used in types of health care, locations and employees not listed in the table in section 12IK but this is not mandatory.
12.7 How do I use the common staffing method?
The CSM is a five-part process which needs to be followed when making decisions about staffing in each of the types of health care that are covered by the CSM:
- the relevant speciality-specific staffing level and professional judgement tools need to be used by the relevant organisation and the results taken into account;
- any measures for monitoring and improving care which are published by the Scottish Ministers as standards and outcomes need to be taken into account, so far as relevant;
- the range of factors listed in the Act need to be considered, namely:
- current staffing levels and vacancies;
- different skills and levels of experience of employees;
- role and professional duties, in particular, of any individual with lead clinical professional responsibility for the particular type of health care;
- effect that decisions about staffing and the use of resources taken may have on the provision of other types of health care including, in particular, those to which the CSM does not apply;
- local context;
- patient needs;
- appropriate clinical advice;
- any assessment by HIS, and any relevant assessment by any other person, of the quality of health care which it provides;
- experience gained from using the real-time assessment arrangements under section 12IC and the risk escalation processes under sections 12ID and 12IE;
- comments by patients, and individuals who have a personal interest in their health care which relate to the duty imposed by section 12IA; and
- comments by employees which relate to the duty imposed by section 12IA.
- risks must be identified and all reasonable steps taken to mitigate against them taken; and
- the relevant organisation needs to decide what changes, if any, are needed to its "staffing establishment", and the way in which it provides care.
For each type of health care covered, the Act specifies for which employees in which locations the CSM must be used. The CSM must be used in each individual clinical ward or team within that type of health care, for example for Adult Inpatient Provision, in relation to nursing workload, it would be run separately in every adult inpatient ward which has 17 or more occupied beds on average. In a community setting it would be run in each separate team.
12.8 Staffing level and professional judgement tools
The first step of the CSM is the application of the relevant speciality-specific staffing level tool. A staffing level tool requires individuals to input certain information about the location in which it is being used, such as a ward or a community service. The tool then outputs quantitative information about staffing, to assist in determining appropriate staffing levels.
A professional judgement tool requires individuals to assess staffing requirements based on their professional opinion of the current workload and the local context. Again, the tool outputs quantitative information about staffing, to assist in determining appropriate staffing levels. The outputs of the two types of tools should be compared with each other and any differences considered, along with the other parts of the CSM.
Details of the tools that must be used for the specific type of health care, location, and employees can be found in these Regulations {link will be added to final guidance once Regulations enacted}. These tools have been designed and tested with the specific setting in mind and should not be used outside these designated settings.
Tools should be applied in accordance with the appropriate user guide. Relevant organisations may also have their own procedures which should be followed as appropriate.
12.9 Measures for monitoring and improving the quality of care
Relevant quality measures published as standards and outcomes by the Scottish Ministers under section 10H of the 1978 Act must be considered, such as the Health and Social Care Standards.. This provides an overview of the quality of care being provided, and allows exploration of whether current staffing levels are a factor in this. Alongside these measures, organisations may also have their own internal measures of quality which they may wish to also consider.
Following the use of the speciality-specific staffing level and professional judgement tools and the consideration of quality measures, the Act then goes on to list a number of factors (listed in 12.7 of this chapter) that also need to be taken into account when determining the "staffing establishment" and the way it which it provides health care. These are further considered below.
12.10 Current staffing levels and any vacancies
Current staffing levels in that type of health care and any vacancies that exist need to be taken into account, along with any impact this has on quality of care. Associated risks should be assessed and mitigating actions identified. This may include, but not necessarily be limited to, assessment of rosters/rotas, absence (including the use of Predicted Absence Allowance – PAA – as applicable), vacancy and supplementary staffing levels.
12.11 Skills and level of experience of employees
Skill mix and the level of knowledge and experience of staff needs to be taken into account, and any impact this has on quality of care needs to be considered; with any associated risks and mitigating factors identified.
12.12 Role and duties of individuals with lead clinical professional responsibility
As part of the CSM process, the role and professional duties of individuals with lead clinical professional responsibility for a type of health care covered by the CSM must be considered when determining staffing levels. More detail is provided about this in chapter 10. Currently, no staffing level or professional judgement tool automatically takes into account the time required for clinical leaders to undertake their leadership role, so it is important that this is factored in.
12.13 Effects of decisions on other areas of health care
The CSM is only required to be used in relation to the types of health care, locations and employees listed in section 12IK of the Act. Nevertheless, it is important to remember that other types of health care, locations and employees still need to be considered, as they may be impacted by decisions made in the types of health care covered by the CSM.
Those services required to use the CSM must consider the effect that decisions taken about staffing in that particular area may have on other areas, particularly those areas who are not required to use the CSM. An example may be where a decision to increase or decrease the nursing establishment having followed the CSM could have a direct impact on staffing requirements in AHP or medical provision in a type of health care not covered by the CSM.
Although not required under the Act it could be beneficial to consider the converse situation, i.e. the effects changes made in other services would have on the service using the CSM. This may require an increase or decrease in staffing dependent on the situation. Some examples where this may apply are listed below (this is not an exhaustive list):
- changes to allied health profession support in a clinical area;
- changes to support services e.g. administration support or portering services in a clinical area;
- changes to medical support in a clinical area; or
- changes in access to multi-agency support e.g. social workers, child protection services.
12.14 Local context
The local context in which the type of health care is being delivered can also have an impact on staffing requirements and it is therefore important this is considered as part of the CSM. The calculators behind the staffing level and professional judgement tools are based on a range of service delivery models and are flexible enough to be adapted to most situations. Therefore the factors which should be considered are those where there is something distinct in that clinical area that differs from the majority of areas providing a similar service. Examples of situations where the local context will be important include, but are not restricted to:
- very remote and rural areas;
- the clinical environment e.g. single rooms;
- significantly different service models;
- additional clinical activity e.g. clinics in ward environments;
- hub and spoke models of care e.g. satellite units; and
- demographic factors, e.g. areas of deprivation and marginalised groups.
12.15 Patient need
Patient need, beyond what has already been considered as part of the staffing level and professional judgement tools, must also be considered. No two service users are the same and the outcomes that matter to a particular service user will vary. When using the CSM, consideration must be given to the service users themselves, rather than just their needs in isolation. Patient need in this context must include consideration of both current provision and unmet need.
12.16 Appropriate clinical advice
Relevant organisations must also ensure that appropriate clinical advice is sought as part of the CSM. Chapter 9 contains further guidance on this.
12.17 Quality assessments
The CSM requires relevant organisations to take into account any assessment by HIS (Healthcare Improvement Scotland), and any other relevant assessment, of the quality of care being provided in that type of health care. This means that the effect of staffing on the outcome of any HIS assessment of quality, or other relevant internal or external quality measures/assessment should also be considered when determining staffing requirements as part of the CSM. This may include, but is not restricted to, outcomes from any Healthcare Improvement scrutiny, specialty specific national measures of quality or audits.
12.18 Experience gained from real-time staffing assessment and risk escalation
Any trends or issues identified as part of the section 12IC Duty to have real-time staffing assessment in place, section 12ID Duty to have risk escalation process in place and section 12IE Duty to have arrangements to address severe and recurrent risks under the Act should also be considered when determining staffing requirements as part of the CSM. For example, if a particular clinical area has regularly identified a staffing shortfall during real-time assessment, further exploration is required to identify the root cause and to ensure a sustainable solution is sought as part of decisions made following use of the CSM.
12.19 Feedback from service users
Any feedback from patients, service users, their families or carers regarding the provision of safe, high quality health care should be considered. It will be important that processes are in place to ensure that this information is collated consistently across the organisation. In practice this will mean that where comment has been made and investigation has revealed there is a correlation with staffing levels and skills, this must be considered when decisions are made following use of the CSM.
12.20 Staff engagement
Any comments made by staff regarding whether there is appropriate staffing should be taken into account. It is important there are processes in place to ensure this information is collated consistently across the organisation. In practice this will mean that where comment has been made and trends are identified there is a requirement for this to be considered when staffing decisions are made as part of the CSM.
These comments may be made by staff using existing opportunities, such as daily handovers, team huddles, adverse event reporting, or during team or individual meetings with line managers, senior managers or partnership organisations. Relevant organisations may feel it more appropriate for a dedicated forum or procedure to be established for staff to feel psychologically safe to provide comments about staffing levels / workload to inform the CSM. There must also be a mechanism for feedback to be provided to staff about the use of the CSM, and staffing decisions made as a result (see 12.25 of this chapter for further detail).
12.21 Identify and mitigate risks
Once all this information for an individual area has been gathered it is important that each of the factors is considered so that there is a detailed understanding of what the staffing requirement is and how that relates to the current staffing levels. Having gained this understanding the Act then goes on to describe the steps that should be taken using this information.
There is a requirement to identify any risks that exist with the current staffing levels and to put in place all "reasonable steps" to mitigate these risks. It may be that risks have been identified, but they are of an acceptable level or nature that they can be managed locally and no action is required. A risk may also be mitigated in a number of ways, dependent on the level of risk. For example, issues with staffing may be mitigated by proactively reducing clinical activity within an area, but could also be mitigated by providing additional administrative support to clinical staff, or increasing the levels of relevant clinical staff. If after taking mitigating action the level of risk is still not at an acceptable level, then consideration of this risk would be escalated in line with the relevant organisation's processes under the section 12ID Duty to have risk escalation process in place and the section 12IE Duty to have arrangements to address severe and recurrent risks.
Relevant organisations should ensure they have a risk assessment process so that across all types of health care covered by the CSM there is a consistent approach to mitigation and escalation of risk. In addition, subsequently there should be a consistent approach to prioritisation of any changes to staffing required across the organisation.
12.22 Decide what changes are needed
Once these steps have been completed, an evaluation is required to consider whether changes to "staffing establishments", or the way in which that type of health care is provided are required. It is important that the impact on staffing requirements of each aspect of the steps is considered and any differences, for example in output from the speciality-specific staffing level tool, the professional judgement tool and feedback, are investigated to enable a detailed understanding of the staffing requirement and how that relates to current staffing levels. The short-term aim is for risks to be mitigated, and, on the longer term, for relevant organisations to consider service redesign or to staffing, to ensure staffing levels are appropriate and sustainable.
The CSM is required to be followed in each setting in the type of health care to which this Act applies, for example a ward or a community team. It is important that each relevant organisation to which this duty applies has a consistent process to ensure that every setting providing health care of a type covered by the CSM applies the CSM at minimum at the frequency defined in Regulations {a link will be added to the Regulations once they have approved by Parliament}, and that the outputs, including decisions about service redesign, are considered on an organisational basis
Following the use of the CSM in each setting in which it applies, relevant organisations should use existing governance processes to make staffing decisions and implement changes as determined by the use of the CSM.
12.23 Frequency of application of the common staffing method
The Act provides for Regulations {a link will be added to the Regulations will be added once they have been approved by Parliament] to determine the minimum frequency with which the CSM should be used and relevant organisations must adhere to this. This can differ for different types of health care and can be altered over time. Frequency of application will also be determined for any new type of health care covered by the CSM in the future (i.e. those added to the table in section 12IK of the Act). It should be noted that this is a minimum frequency and good practice would dictate that the CSM should be run more frequently in certain circumstances. It should also be noted that regardless of the frequency of the application of the CSM, a real-time staffing assessment, risk escalation process and process to address severe and recurrent risks still needs to exist and be applied on an ongoing basis.
Circumstances in which the CSM could be run more frequently include but are not limited to:
- following service redesign;
- significant policy change in the type of health care;
- reduction in quality of care being provided identified through analysis of quality outcome indicators, including patient and staff feedback;
- where there has been a significant change in client group being cared for in that type of health care;
- where, in the professional judgement of the clinical leader there has been a change to workload impacting on staffing requirements; or
- where a risk has been escalated in an area to which the CSM applies or a severe or recurrent risk has been identified.
In some types of health care and / or locations, workload tools outside those required to be used for the CSM may be used and / or measures of patient acuity/dependency assessed and recorded. This may provide information on staffing requirements, the usual purpose of which is to assess requirements in real-time. This is not sufficient to meet the requirements of the CSM as it does not take all the information described in the method into account when planning staffing requirements, for example taking into account assessment of quality, comments from employees or the local context in which the service is being delivered. An example of this would be a workload tool which is applied daily and provides information in real-time; in this case the entire CSM including all other aspects, should still be applied at the frequency provided for by the Regulations as a minimum.
Relevant organisations are expected to have a clear timeline for running the CSM in all areas required at the minimum frequency required.
12.24 Who should apply the common staffing method?
Legal responsibility for applying the CSM sits with the relevant organisation. In practice, it is expected that the relevant clinical team leaders will be responsible for applying the CSM in their clinical area. The clinical team leader must then be supported through time and resources to assess the output from the tools and all other data and aspects associated with the CSM. Decisions on staffing establishments will then be made by the appropriate decision-makers in the organisation, having followed the section 12IF Duty to seek clinical advice on staffing prior to making those decisions.
The relevant organisation must ensure that staff involved in the application of the CSM have the necessary and sufficient clinical expertise and knowledge of the process to properly assess and analyse the outcomes in order to identify staffing requirements. For the current types of health care covered by the CSM, which are primarily nursing and midwifery settings, this is likely to be the Senior Charge Nurse/Midwife or a more senior Nurse/Midwife, supported via the organisation's managerial and professional structures.
It is important that the team is fully engaged in the running of the CSM and the output and decisions made as a result are discussed with them.
The CSM will be run across a large number of locations and teams. The information should be collated in a consistent manner across the organisation and taken into consideration, alongside existing governance processes, when staffing decisions are made at board level. The information should form the basis of staffing decisions at all levels of the organisation, for the types of health care covered by the CSM.
12.25 Training and consultation of staff
Section 12IL of the 1978 Act places an additional responsibility on relevant organisations to encourage and support employees to give views on staffing arrangements, for the types of health care covered by the CSM, and to take account of and use such views. This will enable identification of areas of best practice and areas for improvement in staffing arrangements in areas where the CSM applies. In practice this will mean that a process will need to be in place for staff to provide their views on staffing, for any areas of good practice to be shared across the organisation, any challenges identified, and for this information to feed in to decisions made as a result of applying the CSM. This process should make links to existing governance, professional and partnership structures.
This requirement should be read in conjunction with existing responsibilities on the training and consultation of staff, most significantly the Staff Governance Standard — NHS Scotland Staff Governance. Relevant organisations are already responsible for the implementation of the Staff Governance Standard at a local level. As such this existing requirement requires that staff are well informed, appropriately trained and developed and involved in decisions that affect them.
Staff who are using the CSM must be trained in its use. This training requirement covers all the staff involved in applying the CSM, including those who apply the staffing level and professional judgement tools and individuals who may be providing clinical advice. The training required will be dependent on the level of involvement in the process and current knowledge and understanding.
Staff must also receive adequate time to use the CSM process when determining staffing requirements. Again, this applies to all employees who are involved in its application, including those identifying and mitigating risks and those making staffing decisions. It is likely that the individual running the staffing level and professional judgement tools will require the most time.
User guides are available for application of the staffing level and professional judgement tools at Staffing (workload) tools and methodology. In addition, an educational resource toolkit is provided by Healthcare Improvement Scotland as a training resource for staff at Health and Care Staffing in Scotland | Turas | Learn. Healthcare Staffing Programme staff at Healthcare Improvement Scotland are also available to provide organisations with support and advice on complying with the requirements in the Act.
Relevant organisations will also be required to provide information to staff working in areas where the CSM applies about how the method has been used in the area. This includes the results from using the staffing level and professional judgement tools, the other factors taken into account, and what decisions have been made as a result. As required by the Staff Governance Standard, staff should be engaged and involved in decision-making which affects them. There must be a mechanism for accessible and timely feedback to be provided to staff about the use of the CSM, and staffing decisions made as a result.
In practice, relevant organisations need to ensure that they have governance processes in place which follow the Staff Governance Standard and which therefore will contribute to:
- application of the CSM in all areas where it applies at the minimum frequency determined in Regulations;
- provision of appropriate clinical advice at all levels of decision-making (this will include at board level);
- identification, mitigation and escalation of risk on an organisation-wide basis;
- identification of redesign opportunities;
- internal reporting and risk assessment processes; and
- appropriate staff engagement, training and communication.
12.26 How does a relevant organisation evidence compliance?
Like the other duties contained in this Act, the provisions of the CSM are about ensuring safe and high-quality care. While ensuring the right processes are in place is important, the main purpose of these processes is to ensure appropriate staffing and that should be the focus.
In meeting the CSM, the relevant organisation needs to set out:
- the arrangements it has for ensuring the CSM is used in all clinical areas (individual wards or teams) to which it applies;
- the governance arrangements it has for deciding on staffing levels required as a result of applying the CSM, including provision of appropriate clinical advice;
- the arrangements it has in place for the identification and reporting of risk, mitigation, and escalation relating to staffing requirements as a result of applying the CSM;
- the arrangements it has in place for seeking staff views and feeding back to staff about decisions made as a result of applying the CSM; and
- the arrangements for ensuring staff have appropriate time and training to apply the CSM.
12.27 Other relevant guidance and legislation
Carers (Scotland) Act 2016 (legislation.gov.uk)
Staff Governance Standard — NHS Scotland Staff Governance
Healthcare quality strategy for NHSScotland - gov.scot (www.gov.scot)
Clinical and care governance framework: guidance - gov.scot (www.gov.scot)
Excellence in Care (healthcareimprovementscotland.org)
Standards - The Nursing and Midwifery Council (nmc.org.uk)
Ethical guidance - GMC (gmc-uk.org)
Quality improvement | NHS Education for Scotland
CEL 32 (2011) - Revised workforce planning guidance 2011 (scot.nhs.uk)
Contact
Email: hcsa@gov.scot
There is a problem
Thanks for your feedback