Coronavirus (COVID-19) vaccine certification: evidence paper
This paper summarises the range of evidence available on vaccination certification schemes. Evidence is drawn from clinical and scientific literature, from public opinion and from international experience.
This document is part of a collection
3. Transmission in a vaccinated society
3.1 The science of transmission in a range of settings
SARS-CoV-2 can be transmitted by three main routes: close-range respiratory droplets and aerosols, longer range respiratory aerosols, and direct contact with surfaces contaminated with virus[13]. Figure 8 shows the main transmission routes.
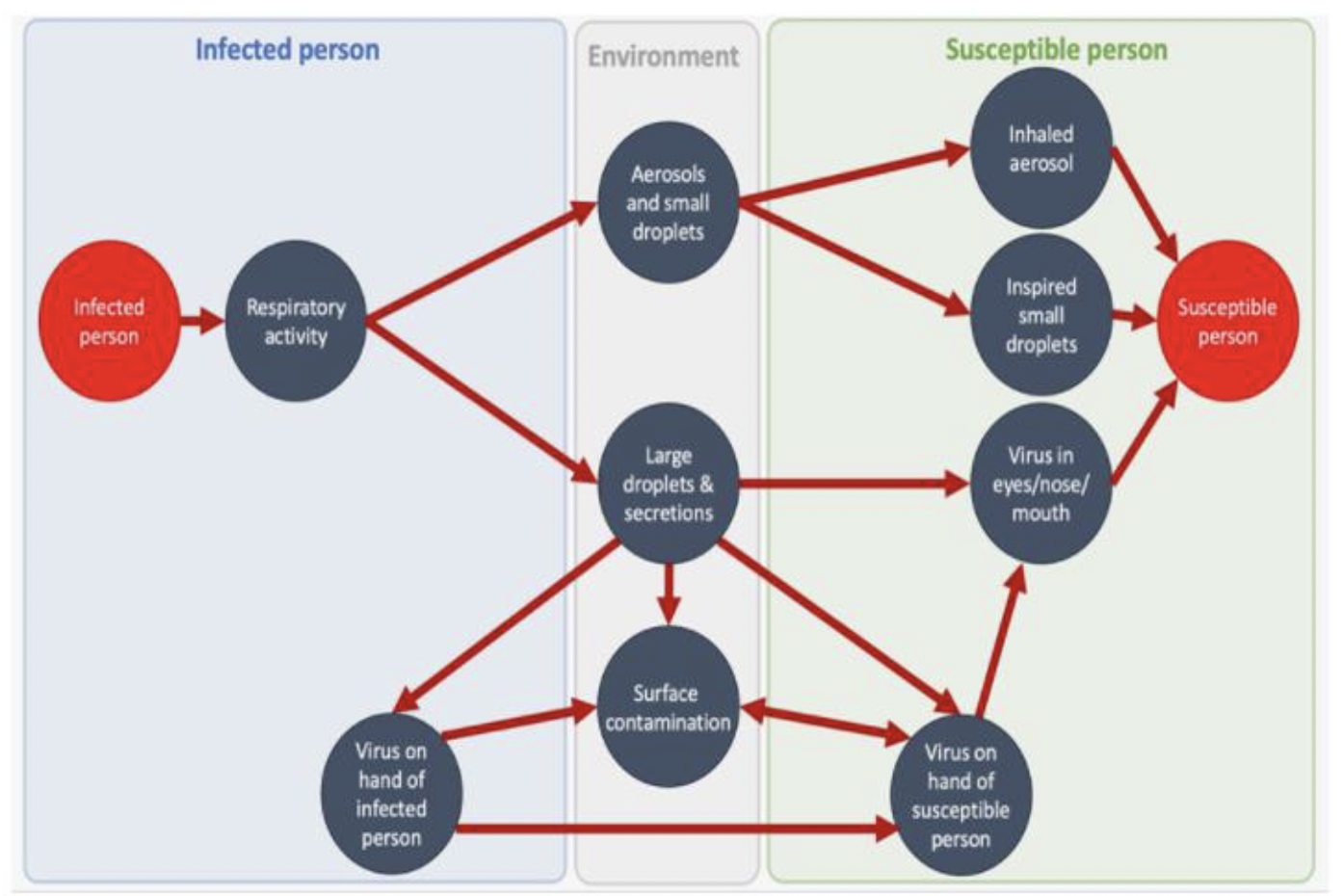
Source: Events Research Programme: Phase I findings - GOV.UK (www.gov.uk)
The PHE Transmission Group indicate that
"Transmission of the virus can take place in any setting….. It is the human behaviour, activities and interactions that occur within a setting that influence transmission. However, some settings facilitate greater transmission due to a combination of risk factors.
This may be that the setting enables particular activities or behaviours that are more risky (e.g. singing, aerobic activity, close interactions), in a place where people spend a long period of time (e.g. homes, workplaces, education), or that a setting does not apply certain mitigation measures (e.g. no use of face coverings in some settings)."[14]
High-risk settings, tend to have the following characteristics[15] [16]:
- close proximity with people from other households
- settings where individuals stay for prolonged periods of time
- high frequency of contacts
- confined shared environments
- poor ventilation
Activities such as dancing, singing and exercise where more particles are breathed out increase the risk of transmission[17].
The Environmental and Modelling Group (EMG) of Scientific Advisory Group for Emergencies (SAGE) have high confidence that the highest risks of transmission are associated with poorly ventilated and crowded indoor settings[18].
3.2 High risk settings
There are a number of higher risk settings currently suggested to be included in the vaccination certifications scheme[19]:
- Late night venues with music, alcohol and dancing
- Live events: indoors unseated 500+ in the audience
- Live events: outdoors unseated 4,000+ in the audience
- All live events: 10,000+ in the audience
Late night venues and live indoor events are considered high risk due to the high likelihood of aerosol emission and low probability of physical distancing and face coverings being worn. These are places where people come together from different households to spend prolonged periods of time (more than 15 minutes) in close proximity, enabling the virus to spread easily from person to person. Risks are further compounded by speaking loudly and the effects of alcohol consumption[20]. Depending on the venue, issues of ventilation (with recirculation of air being particularly problematic), crowding (where it is hard to regulate the distance between people), and pinch points (at areas such as toilets) all contribute to risk. Keeping surfaces clean and regulating movement throughout the setting is a further challenge.
Large outdoor events are considered a risk as even though transmission risk is lower outdoors in general, the risk will be higher where close interactions happen such as in crowded pinch points[21]. Other risks are due to large numbers of people travelling to and from events, leading to crowded public transport and crowded local hospitality venues.
The UK Events Research Programme (ERP) aims to assess the risk of transmission of COVID-19 associated with attending large events as well as to look at whether testing and other measures (non-pharmaceutical interventions) can be used so that people can attend events safely[22]. Information on the outcomes of the programme is in section 5.5 of this report.
3.3 The impact of vaccination
3.3.1 Vaccinated individuals are less likely to catch the virus
Vaccines help prevent transmission of the virus as vaccinated people are less likely to become infected and ill than unvaccinated people (and only infected people can transmit the virus). A diagram to show how vaccines help prevent infections in a group of people is in Figure 9 below.
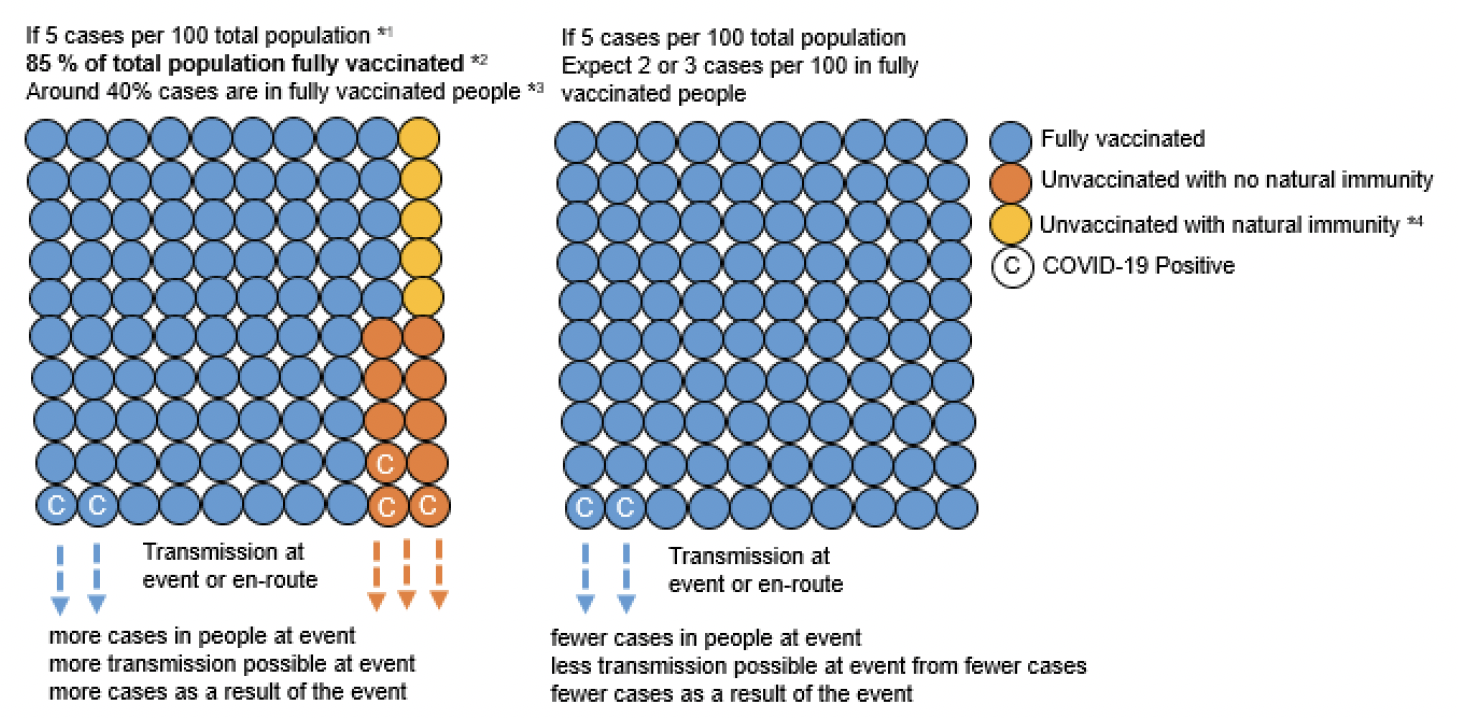
Assumptions from:
*1 Estimated average ratio of the population that had COVID-19 in week ending 3 September 2021 - 1/45for Scotland Coronavirus (COVID-19) Infection Survey, UK - Office for National Statistics
*2 Data up to 15 September COVID-19 Daily Dashboard - PHS COVID-19 | Tableau Public
*3 As on 6 September COVID-19 Statistical Report - 8 September 2021 - COVID-19 statistical report - Publications - Public Health Scotland
*4 As of 1 September - 5% have natural immunity and not vaccinated(assumption based on 85% adults are vaccinated and 90% have antibodies) Coronavirus (COVID-19) Infection Survey, antibody and vaccination data, UK - Office for National Statistics
The UK Vaccine Effectiveness Expert Panel (VEEP) is a group of scientific and analytical specialists from academia and government in the UK who provide a consensus view on vaccine effectiveness, split by variant, vaccine and dose. They have recently published estimates for vaccine effectiveness based on an assessment of the evidence at the time of writing and as new evidence or data emerges, SAGE will update its advice[23]. The current estimates are described in Annex B. For a summary, see Table 1 below[24].
| Infection | Symptomatic disease | Hospitalisation | |
|---|---|---|---|
| Oxford AstraZeneca | 65% (two dose) | 70% (two dose) | 80% (one dose), 95% second dose |
| Pfizer/BioNTech | 75% (two dose) | 85%(two dose) | 80% (one dose), 95% second dose |
| Moderna | 85% (two dose) | 75% (one dose) | Not included |
Source: Vaccine Effectiveness Expert Panel - consensus narrative, 27 August 2021[25]
Vaccine effectiveness is estimated by comparing rates of disease in vaccinated
individuals to rates in unvaccinated individuals and is generally measured as the percent reduction in the frequency of COVID-19 among vaccinated people compared to people not vaccinated. More analysis can be found in a number of large studies including EAVE-II (Early Pandemic Evaluation and Enhanced Surveillance of COVID-19) in Scotland[26] [27], REal-time Assessment of Community Transmission (REACT-1) in England[28] [29] [30] and the Office for National Statistics (ONS) COVID-19 Infection Survey ONS study[31] [32] [33], which are described in Annex B.
A death involving COVID-19 occurring in someone who has received both vaccine doses, and had a first positive PCR test at least 14 days after the second vaccination dose, is known as a "breakthrough death". In total, there were 256 breakthrough deaths in England between 2 January and 2 July 2021[34]. In people who received their second dose at least 21 days before their date of death, 0.8% of all deaths involved COVID-19. Over one-third (37.4%) of all deaths in unvaccinated people involved COVID-19[35].
Therefore, we have strong evidence that vaccines are effective at preventing disease, hospitalisations and deaths. However, vaccine effectiveness decreases over time for both Pfizer-BioNTech and Oxford-AstraZeneca vaccines due to waning immunity[36] [37] [38].
The latest estimates included in COVID-19 vaccine surveillance report
(Week 38) indicate that in England as a result of the COVID-19 vaccination programme, 230,800 hospitalisations have been prevented, and between 119,500 and 126,800 deaths and 23.7 to 24.1 million infections have been prevented, up to 17 September[39].
3.3.2 Vaccination prevents hospitalisations
We can observe in real data from Scotland the pivotal effect vaccination has had in preventing hospitalisations.
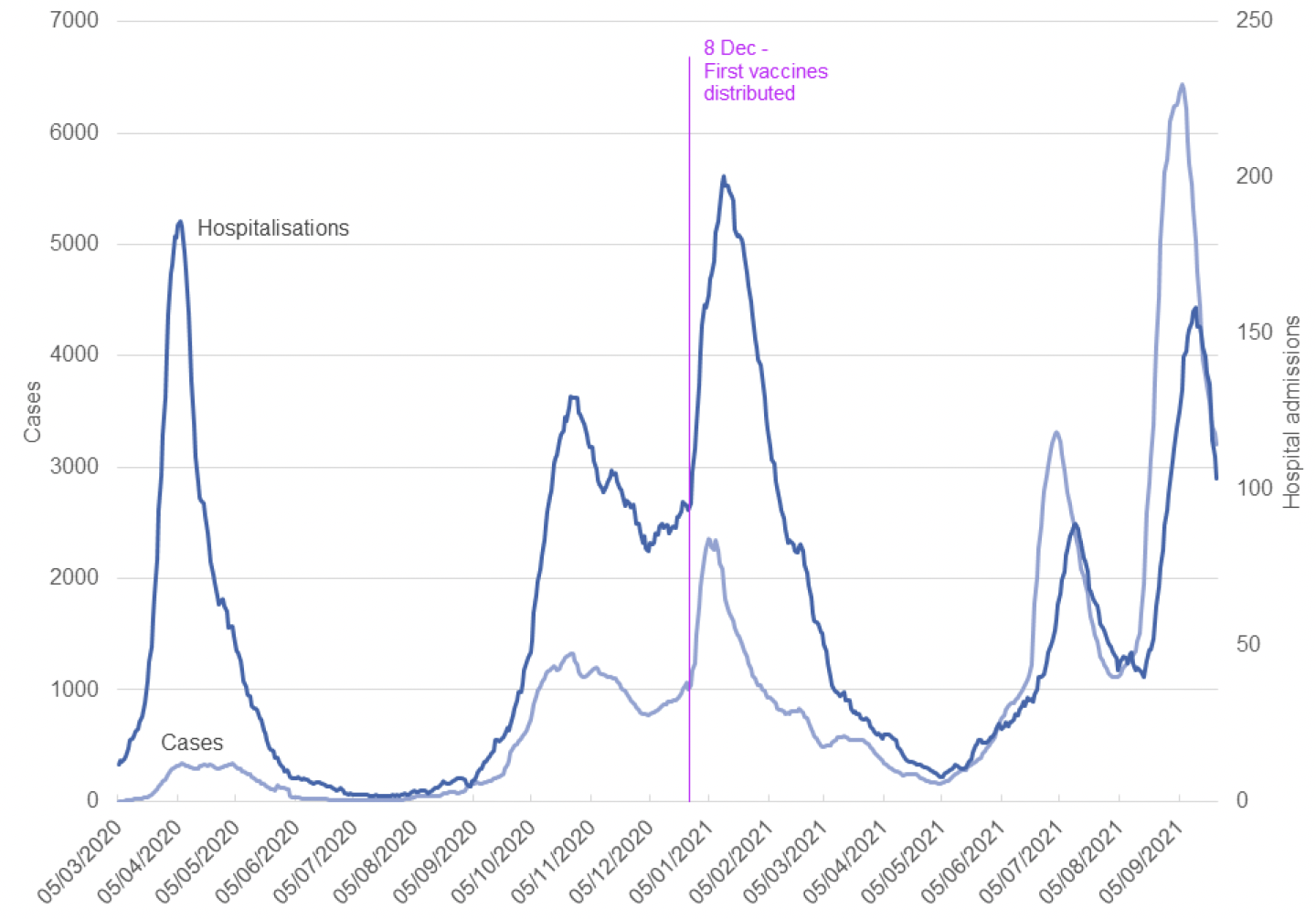
Note: It takes 21 days for protection to develop after the first dose
Source: Daily COVID-19 Cases in Scotland - Daily Case Trends By Health Board - Scottish Health and Social Care Open Data (nhs.scot). Updated 28 September 2021 with data up to 24 September 2021.
Figure 10 above shows that, prior to the deployment of vaccinations, a spike in cases resulted in a steep surge in hospitalisations. At the start of the year, daily reported cases peaked at around 2,600 and at that time (pre-vaccines) around 13% of cases ended up in hospital. In the current wave, daily cases peaked at 7,521 on 2 September resulting in around 2-3% of cases being hospitalised[40].
Public Health Scotland data shows that, in the four weeks from 21 August to 17 September, 34.1% of COVID-19 related acute hospital admissions were unvaccinated individuals[41]. For context, 91.8% of adults aged 18+ have had at least one dose of the vaccine and vaccinated figures include the elderly and vulnerable groups. Overall, individuals in the oldest age groups were most likely to be hospitalised. In all age groups, the rate of admissions per 100,000 was higher in unvaccinated individuals compared to fully vaccinated individuals in the week to 17 September. Unvaccinated individuals were 3 to 4 times more likely to be in hospital with Covid-19[42].
3.3.3 Vaccinated people who are infected can transmit the virus
Once infected a person may transmit the virus, even if they are vaccinated. However, evidence is limited for whether vaccinated people that test positive are less infectious or infectious for a shorter period of time compared to non-vaccinated people.
The most recent consensus view of The Vaccine Effectiveness Expert Panel (VEEP) was considered at SAGE 95 on 9 September 2021[43].
VEEP say that "for the Alpha variant, there is ~40% reduction in onward transmission from vaccinated but infected people after one dose of the AstraZeneca vaccine, and ~45% for the Pfizer vaccine"[44].
Data from Scotland has also shown that household contacts of vaccinated healthcare workers are at reduced risk of becoming a case, at a time when Alpha variant was dominant[45]. Data from Israel also indicate vaccine helped prevent transmission in breakthrough cases at a time when Alpha variant was circulating[46] [47].
VEEP state that there is no direct evidence available for vaccine effectiveness against transmission for the Delta variant[48].
However, there is some indirect evidence discussed below and in Annex B to suggest vaccine effectiveness against transmission may be lower for Delta than for the Alpha variant. Delta infection is thought to result in more infectious viral particles than the original wild type and alpha strain (reflected by a lower Ct value in PCR testing) and is more transmissible[49] [50] [51] [52] [53] [54] [55] [56].
A number of studies comparing Ct values (giving an indication of viral load and infectiousness) in vaccinated versus unvaccinated people are outlined in Annex B. Looking at the limited evidence available, some studies show that fully vaccinated people with Delta variant breakthrough infections have similar levels of viral RNA as unvaccinated people at the time of testing, such as the larger studies from the ONS COVID-19 infection survey[57] [58] [59] and PHE study[60] as well as other studies[61] [62] [63] [64] [65].
However, the level of viral RNA may decrease quicker in fully vaccinated people, meaning that they could spread the virus for a shorter period than unvaccinated people[66] [67]. Also the large UK REACT-1 study found a difference in viral load between vaccinated and non-vaccinated people with a positive PCR test, but the difference between median Ct values for vaccinated and unvaccinated individuals became smaller when only stronger positives were included in the analysis[68].
Contact
There is a problem
Thanks for your feedback