Moray Maternity Services Review: report
Report of the independent review into maternity services for the women and families of Moray, commissioned by Cabinet Secretary for Health and Sport, Jeane Freeman in March 2021.
7 Key considerations
When considering all the proposed models of service delivery for maternity services in Moray, and reviewing these against identified criteria, a number of factors were considered. These included patient safety and quality; patient experience and feedback; as well as the deliverability of the models under consideration.
Further information on key factors considered are set out below:
7.1 Human Factors
Human factors play a key role in any organisation, and their importance to the safety and wellbeing of all involved in those services are crucial. Within Health, this link has been well recognised, initially in the work of The Institute of Healthcare Improvement, and now through the work of Healthcare Improvement Scotland (HIS) and the Scottish Patient Safety Programme (SPSP).
This work is based on learning from other sectors, including the Nuclear and Aviation industries.
'Human factors' is the scientific discipline concerned with the understanding of interactions among humans and other elements of a system. These human factors include leadership, team working, and communication, such as handover, briefing and debriefing. It is well documented that these factors are a crucial element in delivering safe patient care. For example, the SPSP supports care services to learn together to improve the safety and reliability of healthcare to reduce harm whenever care is delivered. They encourage Health Boards to share learning in a safe environment which supports learning and development. The Maternity and Children's Quality Improvement Collaborative (MCQIC) works with maternity services across Scotland to improve outcomes for mothers and babies.
Human factors have also been specifically referenced in a number of reviews into maternity services across the UK, including the high profile "Morecambe Bay" report: Morecambe Bay Investigation Report published - GOV.UK (www.gov.uk)
The Royal College of Obstetricians and Gynaecologists (RCOG) state "Positive working place cultures are underpinned by kindness, civility and respect. And staff need to feel part of a common goal." Jointly with the Royal College of Midwives (RCM), they have undertaken work to improve and support positive work-place environments.
With respect to Dr Gray's, the Expert Group Review into services in Dr Gray's commissioned by the CMO in 2018 noted that "staff morale was low and communication was poor".
Again in 2019, the culture and working relationships were highlighted as an issue as part of the information provided to NHS Grampian's Clinical Governance Committee report into Maternity Services at Dr Gray's Hospital on 21 February 2020. This information references the review by Professor Alan Cameron undertaken in 2019. In the report of that review, it is stated:
"Working relationships in the Dr Gray's Maternity Services are dysfunctional and damaged to the extent they may impact upon patient safety"
The following comments also appear in the report:
"examples of blame, alleged bullying, unprofessional behaviour and the desire for Dr Gray's to be 'left alone' – none of these are conducive to a multidisciplinary team working in an open and honest culture, where everyone's contribution, irrespective of role or location, is equally valued"
"incidences of staff displaying paternalism in respect of compassionate discussions"
"The current culture within the unit appears to be one where the medical model was dominant with communication to the Review team of a paternalistic culture and a current hybrid model of care that does not fully meet the needs of anyone, women or staff."
During this review, working relationships and culture, both internally in Dr Gray's as well as between staff in Dr Gray's, Aberdeen Maternity Hospital and NHS Grampian, have again been identified as an ongoing concern. This was expressed by a number of professionals and stakeholders; and has, on occasion, led to a loss of confidence by service users and the wider community.
For example, staff mentioned that poor working relationships had hampered development in the unit, and multi-disciplinary meetings were described as "difficult to attend". Mothers and families also referenced communication issues between professionals and across sites.
It is also noted that guidelines appear to differ between Dr Gray's, Aberdeen and Raigmore, which lead to confusion for women and their families. Whilst the Review Group accept that some variations may be required, the core of guidelines should be built on evidence-based practice. Variations in any guidelines require to be clearly articulated to all staff and service users.
It will, therefore, be important that work is progressed to address these relationships, and the overall safety culture within the service.
Notwithstanding the above, it is however, extremely important to emphasise that during the work of the Review Group, there was no evidence that the clinical outcomes for women and babies in Moray were any way impacted by this.
As described below, on the whole, women and families were also extremely positive about the care and support they had been given by individual members of staff.
7.2 Mothers' and Families' Voices
During the course of this independent Review, we met with mothers from Moray, and local action groups representing mothers, both virtually and in person. We felt that it was very important that we heard their stories from mothers to fully understand the lived experience of those directly affected by changes to the Maternity Service in Moray.
We heard the mothers describe spending their pregnancy concerned as to whether they would meet the criteria for a "Moray birth" or require to be transferred in advanced labour to Aberdeen, a journey of 65 miles. Mothers from the West of the Moray area spoke of having to drive past Dr Gray's to make the journey to Aberdeen whilst in labour, despite Raigmore in Inverness being the closest Obstetric Maternity Unit. Mothers also expressed concern regarding the journey to Aberdeen along the A96, a single carriageway road, perceived to be prone to accidents; and which can, on occasion, be closed in winter due to prevailing weather conditions. Mothers described the stress this caused on themselves and their partners making the journey home, relatively soon after giving birth, with a new-born baby in an infant car seat.
The stories they told, whilst all individually distinct, had several common themes running through them, and we have decided to relate their stories via these themes which will hopefully give a flavour of what we heard whilst maintaining confidentiality. We recognise that we only heard a small fraction of the voices from Moray, and that many mothers and their families will have more positive experiences to relate, and this has to be taken into consideration when reading these stories; however, this does not detract from the emotional impact they had upon us. We would like to thank and commend all of the mothers, women and families who contacted us to explain how their experiences of the maternity services in Moray had impacted them; and we would especially like to thank those who came forward and spoke to us. Telling their stories in person was clearly distressing for a number of them, yet they persisted, and their courage and fortitude is commendable.
As an integral part of the synthesis of evidence gathered, the Service Design Hub established a series of personas[13] for each homogeneous[14] group with whom the Review Group engaged, based on shared 'pain points' and similar 'needs' identified.
Key themes recognised as emerging from experiences shared by the various stakeholders, and outlined below, are: communication, community impact and anxiety, travel, staff, and partners.
7.2.1 Communication
It is recognised that communication is vital to the efficient working of any system, never mind one as complex as the NHS, but it was evident from the stories we heard that communication issues were a major factor. This may have been communication with the mothers by either of the three Maternity Units, communication between those units at a professional level, or communication with the community as a whole. Many mothers felt that the links between Dr Gray's and Aberdeen Maternity Hospital were poor.
- "I am not sure who is talking to who between the two units, but when I turned up at Aberdeen Maternity Hospital, they didn't have a clear idea of what my problem was and were so busy struggled to find out."
- "I felt that the staff in Dr Gray's were frightened to raise any issues with Aberdeen Maternity Hospital."
- "It was clear that the staff in Aberdeen Maternity Hospital had no understanding of where we had come from and the distance involved. It was quite common to be told to go away and come back later, or the next day. If they spoke to each other (Dr Gray's and Aberdeen) then surely they would understand how difficult this was?"
- "When I arrived at Raigmore, I was terrified; but I could feel, simply by the looks and murmured conversations, that I was deemed a bit of a nuisance. They hadn't expected me, and had no free space. It really clouded what I hoped would be a more positive experience."
- "The unit was downgraded very suddenly, in our eyes anyway, and we were told it was temporary, for a year at most. This was three years ago and nothing has changed. We need to hear from NHS Grampian and have more chance to speak to them and let them hear us. The silence just increases all our anxiety. The fear of the unknown."
7.2.2 Community Impact and Anxiety
The move from a Consultant-led Unit to a Community Maternity Unit at Dr Gray's in 2018 led to an understandable reaction from the community, which has led to local groups and politicians discussing this issue regularly, and in as many forums as possible. Stories have been relayed and shared, and one consequence of this has been a growing anxiety amongst women about what quality of service they may receive if they are having a baby in Moray.
- "I am very aware of women who wish to have a baby, but are making the awful decision not to, based on the local services available. Some have left the area due to their concerns, which is a real blow to an area like Moray which is desperate to grow its community, not shrink it!"
- "Some of my friends have discussed timing their pregnancy to ensure that they deliver in the summer months, so that they don't have to contemplate travelling to Aberdeen in the winter. We shouldn't have to do this."
- "Ever since I fell pregnant, I have noticed a background anxiety, a nervousness, that I didn't have in my first pregnancy. I have heard these stories of mothers travelling all the way to Aberdeen in labour and in pain, and the thought terrifies me."
- "Moray can seem a bit of a deprived area, but it has lots going for it, not least the two military bases; but I keep hearing about families asking for transfers or refusing to be posted here purely down to the Maternity Services."
- "There is fear: I fear not knowing exactly where I will deliver my baby; will I have to travel a long distance? / on a poor road? / in pain? only to arrive somewhere unknown to me and so busy that it struggles to deal with me."
7.2.3 Travel
Women, early on in their pregnancy, due to complications or underlying health conditions, may be placed on what is commonly referred to as a "Red Pathway". This means they will be booked to give birth in Aberdeen (or Raigmore; although numbers suggest very few women are offered this option). However, of the women planning to give birth in Dr Gray's, for appropriate clinical reasons and safety whilst in labour, they may have to be transferred intrapartum to Aberdeen or Raigmore. This can often lead to a poor experience, uncontrolled pain, and safety issues from the journey itself. However, it should be stressed that many mothers in Moray have made this journey with no adverse clinical outcomes, and accept that (at the time) this was the best and safest option for them and their unborn baby. It is also worth noting that it is not uncommon for mothers in other rural areas of Scotland to have to travel similar distances for their maternity care.
- "When my contractions started, I went to Dr Gray's as planned, but it was apparent early on that they were not happy. Quite suddenly, I was told I needed to go to Aberdeen, and I had to make my own way there. Thankfully, my husband was free and able to get time off work to drive me, although this could have been much harder in different circumstances. He often works away from home and we haven't family nearby. Anyway, we started the journey; but, after about 10 minutes, my contractions got significantly worse. I had to take my seatbelt off as the pain was unbearable. I spent the next hour of the journey like this with my husband sometimes driving too fast as he was so worried about me. I couldn't stop thinking about what would happen if we had an accident. It was terrifying."
- "I had been deemed a high risk but there had been agreement that I could still have my baby in Dr Gray's. However, after 35 hours of labour, it was decided that I was not progressing and that I had to go to Aberdeen. My husband had to drive me and I was in so much pain that the only way I could achieve any level of comfort was to kneel in the back seat facing backwards holding the headrest. I had no seatbelt on the whole way."
- "I had been told that if I had a bleed before giving birth, the chances were slim that I would survive, and consequently neither would my baby. I spent months in constant fear that I would bleed. Then the worst happened, and I started bleeding at home. I was transferred, initially to Dr Gray's, then to Aberdeen in a blue-light ambulance. The bleeding did initially stop, and I was told my baby had a heartbeat; but, when the bleeding started again, on the way to Aberdeen, I was told the heartbeat had gone. I therefore thought that my baby was dead, and it was likely I was next. It has taken me over a year to talk about this as the experience was so traumatic. Thankfully, my baby (and I) did survive."
7.2.4 Staff
It goes without saying that all interaction of the women and their families described above involved staff members from Dr Gray's and Aberdeen, NHS Grampian and Raigmore, NHS Highland. It is possible that some of the experiences shared may give readers a sense that staff could perhaps be rather uncaring or unhelpful. However, it is important to stress that women, almost without fail, would sing the praises of the staff they interacted with. Often mothers recognised that both Aberdeen and Raigmore were busy; and described feeling like they were an 'extra' on top of the maternity staff's already heavy workload; yet compassion and kindness in how they were treated were expressed as the norm.
- "Before I tell my story, I want to say that all staff that I have been involved with over my two pregnancies have been amazing. Nothing I say is in any way a criticism of their care."
- "The staff in Aberdeen Maternity Hospital may not realise at times that we have great distances to cover (and this is understandable when you realise the number of mothers they are dealing with), but they were always extremely kind and caring. I couldn't have asked for more, other than to have got all that in Elgin!"
- "I feel genuinely sorry for the staff at Dr Gray's. They are amazing, and delivered my first baby (prior to 2018) with kindness and a care that made every moment memorable, even the painful parts! I hope they can get back to this soon."
7.2.5 Partners
In recounting their stories, many women and their representatives were at pains to tell us how their experience had affected their partners. There was a combination of fear, anxiety, inconvenient and uncomfortable travel, and helplessness in these stories; and we feel it is important to recognise this in the report.
- "My husband does not like driving and, because of this, has never driven to Aberdeen. When he had to do this, at short notice, with a crying, panting wife beside him it was a pretty terrible experience. Then we arrived and he was asked to 'go home and come back later'. Home was nearly 80 miles away; but he did this without question. He made this journey every day for three days in a row, which was exhausting."
- "I feel traumatised by our journey, but I know my husband feels the same. He has flashbacks about possible accidents and their consequences. Whatever would've happened would've been his fault…which is so unfair."
- "I think it is really unfair that my partner had to witness what he did. This is an important time for him too, but he felt excluded and often ignored simply due to all the uncertainty and moves. It shouldn't be like this."
The quotes used above are a small sample of what we heard; to relate all the stories in their entirety would be inappropriate, and likely to breach privacy and confidentiality agreements.
We, the Review Group, wish to express our sincere gratitude to all of the mothers for your honest contribution to this review process; and we would like to assure you that we did listen, and we heard what you told us.
7.2.6 Staffing levels and challenges
Maternity and Obstetric care requires the support of a multi-disciplinary team to deliver high-quality and safe services. This includes, depending on the model of service provided:
- Midwives
- Obstetricians and junior doctors
- Anaesthetists
- Paediatricians and neonatal staff to support newborn babies
- Theatre staff (to support the provision of specific procedures – i.e. caesarean sections, assisted deliveries, etc.)
- Laboratory and pharmacy staff
- Non-clinical support staff (e.g. porters, domestics, etc.)
The make-up of the North region is quite unique; and therefore, we cannot underestimate the challenges that exist around the workforce and in the maintenance of skills for the multi-disciplinary team referenced above.
There are currently recruitment challenges for both medical and midwifery posts across health services in the UK. This is exacerbated in rural Health Boards in Scotland, and has been a particular challenge in the North of Scotland. This reflects the fact that communities are often more remote and the nature of service provision requires staff who are willing to work in more generalised roles and on out of hours ('on-call') rotas with greater frequency of work. For example, in Dr Gray's, the obstetrics and gynaecology consultants have always worked a single on-call rota, 1:4 covering both obstetrics and gynaecology. In Aberdeen, consultants will often specialise in either obstetrics or gynaecology; the current on call rota there is 1:11.
While there are definite benefits to be described in working within services such as Dr Gray's, it is essential that Health Boards in the North of Scotland look at innovative ways to recruit, train and retain staff. This is being explored as part of the "Best Start North" Programme, between NHS Grampian, NHS Highland, NHS Orkney and NHS Shetland. This will be critical to the ongoing sustainability of any future model of care in Dr Gray's.
This includes options to have joint appointments between Health Boards, and agreement is being explored to provide a service network. An indication for further work from phase one of this programme is in relation to clinical supervision, education, training, and sustaining people skills. This is shown as an example of something that can more effectively be achieved collectively than it could within a single Board. The Best Start North Programme has noted innovative examples of recruiting and retaining staff which warrant further exploration. While the progression of this work has been impacted by the pandemic, and is currently paused awaiting the outcome of this Review, we would strongly support this being taken forward as a priority.
We also heard from representatives at RAF Lossiemouth that opportunities may exist to recruit partners of military staff arriving in Moray for a tour of duty, who currently work in clinical roles elsewhere in the UK. This should also be progressed as a matter of priority for joint work.
It is recognised that solutions for the North need to be unique and provide resilience for these services. There are examples of Scottish Island Boards who have recruited obstetricians and gynaecologists on a rotational basis from other parts of the UK and beyond. The benefit of this is that while they may be carrying out lower volumes of work while on the Islands, they are doing high volumes of activity elsewhere; as a result, this sustains their clinical skills, and is a key factor in ensuring they can continue to sustain a service in remote areas that do not provide an adequate level of activity to maintain their skills.
Within any extended model of obstetric care in Dr Gray's, the availability of junior medical staff, who are still in training to become consultants in their relevant speciality, is essential. This was demonstrated with the gap in paediatric junior staff in 2018 that led to the initial change in obstetric service provision.
It is also well recognised that the teaching of junior medical staff is beneficial to services both in terms of improvements in quality of services, but also as a factor in the recruitment and retention of staff. It is, therefore, important that work is progressed to improve the experience and retention of trainees in Dr Gray's.
The distribution, employment and supervision of junior medical staff is the responsibility of National Education Scotland (NES) through the Scotland Deanery (the Deanery). The Deanery is also responsible for monitoring the quality of training and making recommendations on the approval of training places. This also includes input from the relevant Royal Colleges and the General Medical Council (GMC). It should also be noted that while the primary reason for a junior doctor placement is education and training, they are also integral to the safe staffing and delivery of a service.
As part of the Review Group's evidence gathering, we met with representatives of the Deanery who indicated there are insufficient medical trainee numbers in the North of Scotland in obstetrics, anaesthetics and paediatrics to provide an adequate number of doctors at either junior or middle grade level to support a standard consultant-delivered maternity model in Dr Gray's. Indeed, with current trainee numbers, and the difficulty of recruiting to even these posts, there are real challenges in supplying trainees to Aberdeen and Raigmore, let alone to three consultant-led units in the North of Scotland. Any attempt at redistributing trainees from Aberdeen or Raigmore would create a significant risk to the sustainability of these services. Alternatively, a redistribution would be required to the North of Scotland, which would equally run the risk of destabilising services in the rest of Scotland. It should also be noted that the unit in Dr Gray's is not currently approved as a training location for obstetric trainees.
Midwifery staffing provision was also noted to be a challenge in the North of Scotland. Whilst during the Review it had been noted that the midwifery team in Moray has been stable for a significant period of time, recruitment and retention for qualified midwives remains challenging in NHS Highland and NHS Grampian. This meant, at times, that midwives working in Moray would be working in Aberdeen; there were some benefits to this model though, with increased staff integration and collaboration through relationship-building. With the move to continuity of midwifery care, it is likely flexible movement of staff between sites will become the norm and should be promoted.
Other elements of service provision and supporting infrastructure were noted, which will also require to be taken into consideration, as follows:
- The gestation at which women can safely give birth at Dr Gray's will need to be agreed locally. This needs to reflect the recommendations in Best Start regarding where and how Neonatal services can be delivered. The decision will need to take account of recommendations regarding transitional care to keep mothers and babies together. This will require discussion around the staff and training required to provide these services safely.
- ScotSTAR (Scottish Specialist Transport and Retrieval) is a division of the Scottish Ambulance Service that exists to provide a national service for the safe and effective transport and retrieval of critically ill neonates and children in Scotland. The service provides a safe and dedicated transport service for a particular patient group who, because of their clinical condition, require an augmented clinical team during retrieval/transport, and represent the most vulnerable of patients transported in Scotland.
The ScotSTAR team have a multi-professional staff complement of consultant and fellow grade medical staff and experienced transport nurses, who work in tandem with the regional Paediatric Intensive Care (PICU) teams. While it is not suggested that in the near future there will be any significant change in impact on the ScotSTAR service, it will be important, as development of local maternity services progresses, that continued engagement takes place with ScotSTAR to address any further impact.
- The Scottish Ambulance Service (SAS) is central to providing intrapartum transfers of mothers (who are currently mainly transferred to Aberdeen from Dr Gray's). This can reportedly take a crew out of area for up to six hours at a time. Ongoing discussions will be need to be taken forward between NHS Grampian, NHS Highland and SAS to ensure the sustainability of the service, to support future transfer requirements, as the maternity service in Moray evolves.
- Appropriate laboratory services are available to support maternity care at Dr Gray's. It is understood that Dr Gray's utilises "O Negative" blood for emergency situations, as cross-matching services are not available out of hours. We recognise this could have an impact on the level and sustainability of maternity services provision. We are aware, with the development of new technologies, there are alternative models of blood supply. As maternity services are developed in Dr Gray's, consideration should be given to the appropriateness of alternative solutions to bolster availability of blood to support the maternity services in Moray.
7.3 Births Data and Analysis
Analysis of data regarding births by Induction of labour and Caesarean Section:
7.3.1 Moray and Banff Births 2017/8 to 2020/Sep 2021[15]
Number of births in Moray and Banff split by location of delivery
| Location / Year[16] | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|
| Dr Gray's | 869 | 596 | 280 | 178 |
| Aberdeen | 125 | 321 | 618 | 714 |
| Raigmore | - | 38 | 33 | 16 |
| CMU | 7 | 0 | 3 | 6 |
| Home | 7 | 16 | 8 | 13 |
| Born before arrival (BBA) | 4 | 9 | 5 | 11 |
| Total | 1023 | 1014 | 1041 | 1032 |
Number of births by type of delivery in Dr Gray's 2018 - 2021 (Jan-Sep)
| Dr Gray's[17] | 2018 | 2019 | 2020 | 2021 (Jan-Sep) |
|---|---|---|---|---|
| Induction of labour | 215 | 0 | 1[18] | 2[19] |
| Birth without obstetric intervention | 416 | 215 | 191 | 132 |
| Breech | 4 | 1 | 0 | 1 |
| Ventouse | 25 | 6 | 2 | 0 |
| Forceps | 23 | 1 | 0 | 1 |
| Elective caesarean section | 35 | 52 | 0 | 0 |
| Emergency caesarean section | 49 | 5 | 5 | 0 |
| Caesarean section grade not recorded | 14 | 0 | 0 | 0 |
| Babies born before arrival at hospital | 7 | 3 | 8 | 7 |
Number of births by type of delivery in Aberdeen 2018 - 2021 (Jan-Sep)
| Aberdeen | 2018 | 2019 | 2020 | 2021 (Jan-Sep) |
|---|---|---|---|---|
| Induction of labour[20] | 156 | 337 | 335 | 265 |
| Birth without obstetric intervention [21] | 182 | 312 | 325 | 210 |
| Breech | 1 | 5 | 5 | 1 |
| Ventouse | 7 | 17 | 13 | 10 |
| Forceps | 52 | 92 | 83 | 86 |
| Elective caesarean section | 32 | 69 | 126 | 88 |
| Emergency caesarean section | 65 | 138 | 186 | 153 |
| Caesarean grade not recorded | 23[22] | 0 | 0 | 0 |
| Babies born before arrival at hospital | 1 | 1 | 3 | 3 |
7.3.2 Moray Population Projections
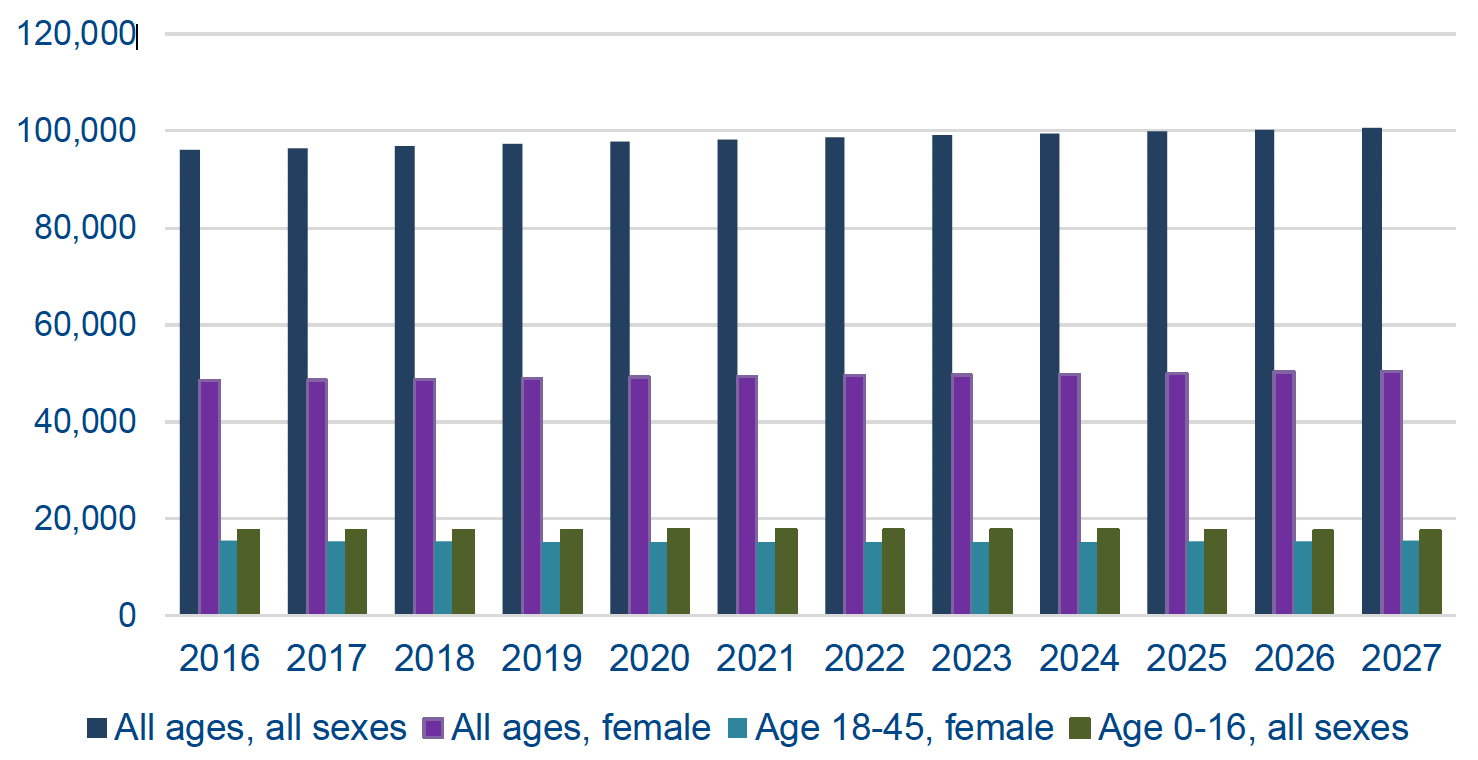
While these projections show a small increase in the overall population in Moray of nearly 5% over the period from 2016 to 2027, within this, the proportion of women in the 18-45 cohort is broadly stable.
7.4 Best Start North
NHS Grampian, NHS Highland, NHS Orkney and NHS Shetland have come together to develop a sustainable plan for the future service delivery.
Best Start North, a programme report published in December 2020, sets out their ambition and the challenges they face in delivering on this ambition.
The Best Start North Steering Group had the following objectives:
- To support a multi-professional and cross Board culture of excellence in Maternity and Neonatal Services.
- To provide senior leadership and direction from each of the relevant Boards for a strategic review and planning process.
- To provide senior clinical input and leadership on the services provided across the relevant Boards.
- To ensure that any planning processes or data gathering undertaken as part of the review is supported at Board level.
- To agree and support relevant communications and messages related to the review.
- To consider and contribute to the outputs from the review process, including interim and final reports.
- To provide and optimise Board level leadership for the redesign of services.
- To consider and provide feedback and direction on proposals or developments arising from the planning process.
- To provide information and advice to the programme of work on any issue posing a risk to deliver ability using appropriate escalation or reporting processes.
- To respond to direction from the Chair and Chief Executives Group, taking
- appropriate actions.
7.4.1 Best Start North Approach
The group has undertaken a mapping exercise of the resources available in the North of Scotland, and Shetland and Orkney Health Boards.
The group comments that:
"NHS Grampian has been committed to a phased return of maternity services to Dr Gray's, with phase one seeing the re-introduction of elective caesarean sections already in place. However, the second phase of the reintroduction has not been realised as concerns were raised about the workforce required particularly from an anaesthetic standpoint. This would mean that a substantial capital investment was required to meet national standards, as currently Dr Gray's do not have around the clock resident anaesthetist. This temporary model of care has now been in place for over two years and there is a growing need to move to a sustainable long-term model of maternity care at Dr Gray's."
To support this work, an interim report was commissioned with the Department of Health Innovation (DHI)[23] as an output from a series of workshops; and in this report, key themes were identified in looking at Dr Gray's.
DHI reported that: "These emerging themes are acutely represented within the challenges in establishing a sustainable long-term model for maternity care at Dr Gray's".
(1) Right People, Right Skills, Right Place, Right Time
Medical staffing was a significant reason for the shift to a hybrid model of maternity care at Dr Gray's Hospital. The current model was not designed to be a long-term solution and the phased re-introduction of obstetric-led maternity services has been hindered by the economic and workforce resource required. Therefore, a long-term solution that is safe, equitable and economically viable may involve taking a tailored approach to ensuring the right people with the right skills are available in an appropriate location to deliver care in a timely manner.
It is beyond the remit of this study alone to suggest what the appropriate future model for maternity care at Dr Gray's may be. However, ensuring that a frank, receptive approach is taken towards future conversations, that include the input of the full range of stakeholders and that are done in an efficient, albeit considered manner, will be integral.
(2) Patient Expectations and Choice
Patient expectations and choice of location of birth are central to the challenge faced by Dr Gray's. The work undertaken by DHI will be supported by engagement undertaken by SenseMaker® which focuses on the public/patient perspective, experience and expectations. Therefore, SenseMaker®'s work will be better positioned to highlight patients/public perceptions on expectations and choice in greater detail.
However, the DHI has had extensive engagement with clinical and midwifery staff, as well as patient representatives contributing to co-design workshops. It has been indicated that local public campaigns fervently advocate the resumption of a consultant-led maternity service at Dr Gray's.
(3) Emergency and Retrieval Services
As highlighted previously, it is important that good communication and consultation on changes in models of service delivery takes place, including with the SAS and ScotSTAR who are critical to the safe transfer of mothers and babies between maternity units and to neonatal care when this is clinically required.
With the pace at which the shift in service model had to be implemented in 2018, it is clear that the opportunity for joint planning and consultation was limited. However, it has also been suggested that clarity of guidelines and transfer arrangements can remain an area of continued challenge. It has been suggested, for example, that there have been delays in timing of transfers, and the remit of the service at Dr Gray's resulting in "SAS arriving on site with women that fall out with the remit of current services."
7.5 Wider implications for Dr Gray's beyond Maternity Services
In discussions with a range of stakeholders, including members of the public, NHS Grampian and the local maternity services, it has been acknowledged that the future of maternity services in Dr Gray's is closely linked to the future of Dr Gray's Hospital as a whole.
This would be the experience of similar services in other district general hospitals across the UK and Scotland, where the vibrancy of services in a hospital has a positive knock-on effect on all the services being provided. This reflects the interconnected nature of services in the Health Service with all services, including maternity and obstetric services, being dependent on the range of clinical and non-clinical services available on the site. As already indicated, obstetric services are particularly dependent on services in anaesthetics, theatres and paediatrics. The sustainability, scale and capacity of these services are also then linked to the wider services provided on the site.
In turn, this impacts on the way in which a hospital is perceived, and will impact on the overall ability to recruit to and retain staff at the hospital.
It was clear from much of the feedback we received from local staff and the public that they were unsure about, and concerned for, the future of Dr Gray's. This is despite NHS Grampian stating their support for services at Dr Gray's, and confirming that Dr Gray's is an essential part of NHS Grampian's future service provision. The Review Group is clear that the future plans for Dr Gray's as a whole will be critical to the successful ongoing provision of obstetric and maternity services there.
7.6 Travel to Access Maternity Services
The women and families of Moray raised concerns regarding the distances they had to travel for elements of their antenatal care, or indeed whilst they were in labour. Their perception was that staff in Grampian did not always appreciate the distances that were required to be travelled and the challenges presented by the rurality of the area. This resulted on occasions with women being contacted to attend Aberdeen without adequate notice. If attending for a review out with core hours, the women found themselves being discharged home late in the evening. In this context, it has to be acknowledged that this is not unique to the women of Moray, and that, in other areas of rural Scotland, women also find themselves in similar situations. The information below offers some context to the women's concerns.
Travelling from Elgin to Aberdeen:
- By train, this can take in the region of two hours, and costs can vary from £16 to £47 depending on the time of day when the journey is made.
- By bus, this journey can take in excess of two and a quarter hours, and costs can range from £14 up to £21.
- By car, Aberdeen is approximately 65 miles from Elgin which generally takes between an hour and twenty minutes to just over an hour and a half to drive to, depending on traffic and road conditions. Fuel costs would be in the region of £15, and with fuel price rises this can fluctuate.
It should be noted that women and their partners and/or families may have to make this journey on more than one occasion, which can be inconvenient, uncomfortable and costly.
Having this number of women travelling via personal transport does not align with the Scottish Government plan to cut carbon emissions to net zero in the Health Service.
Utilising NHS "Near Me" digital technology, reducing the need for women and families to travel in person to Aberdeen or Inverness should be enhanced as a result of this Review. Consultant anaesthetic and obstetric services can successfully be delivered via digital technology moving forward. This reduces the amount of time spent travelling for women, ensuring they continue to have thorough assessment in collaboration with their midwife, offering a more convenient, less costly, and more comfortable experience.
Contact
Email: Kirstie.Campbell@gov.scot