Attend Anywhere / Near Me video consulting service evaluation 2019-2020: report
This report presents the findings of an external evaluation of the Attend Anywhere / Near Me video consultations service used across health and care services in Scotland
3. Findings
3.1 Uptake and use of Attend Anywhere
By the time of writing this report (early 2020) all 14 local Health Boards and the Golden Jubilee National Hospital were enrolled on the scale-up programme. The uptake and use across Health Boards and clinical areas are presented in Appendix A, based on activity data collected through the Attend Anywhere system during Jan-Dec 2019.
During this period, 6719 Attend Anywhere consultations were conducted across all health boards. Most of this activity (91%) was within secondary (i.e. hospital) care and other community health services (excluding GP practices). This included approximately 180 clinical departments with 'active' waiting areas ('active' meaning used at least once during this period) across all health boards. These were all at different stages of implementation, and there was great variation in the level of video clinic activity across clinical departments. The graph in Appendix B presents the spread of video clinic activity across services.
Approximately 130 clinical departments (70%) had conducted five or more video appointments during the collection period.
The activity included approximately 35 different clinical specialties. Gastroenterology presented the highest frequency of appointments, but was only routinely used within two Health Boards (Highland and Grampian). Haematology was the second highest specialty, but was mainly focused within one Health Board (Highland). Psychiatry and psychology related services presented the highest uptake rate across Health Boards, and was the third highest area with regard to frequency of video appointments overall. The full list of specialties and associated activity are presented in Appendix C.
The remaining 9% of Attend Anywhere activity across health and social care was through 64 GP services. Similarly, these were all at different stages of implementation, with 23 (36%) of these services having conducted five or more video consultations.
Around 62% of consultations via Attend Anywhere were conducted within two Health Boards; NHS Highland (42%) and NHS Grampian (20%). Although it is important to note that many clinicians based within these two Health Boards also run remote consultations with the patients based in the NHS Western Isles, NHS Shetland and NHS Orkney. This meant that the appointment activity was captured within the Attend Anywhere accounts at the hub sites where the clinician was based, even though the patient was based at an island site (either at home or at the hospital)
Furthermore, 50% of the GP activity was concentrated within NHS Grampian, where there is a specific TEC-funded programme to support scale-up within community and primary care across Aberdeenshire.
The activity data was captured through the Attend Anywhere platform, as opposed to NHS systems, and so it was not possible to establish the proportion of video in relation to other appointments types (i.e. face to face and telephone appointments). However, based on preliminary analysis conducted by local teams within some health boards, it would appear that the proportion of Attend Anywhere activity was a relatively low proportion of overall outpatient activity. For example, In NHS Highland, it was estimated that Attend Anywhere constituted 1-2% of outpatient clinic activity across the Health Board. Similarly, within NHS Grampian it was estimated that 16-18% of patients opted to use video for their consultation within one of the most established services that routinely offers video appointments. However, it is important to note that these estimates were based on preliminary analyses, and there are other aspects of outpatient activity to account for (e.g. new versus return appointments). This highlights the value of being able to access routinely collected data from the patient administration systems, rather than relying solely on the Attend Anywhere platform, to monitor use of video consultations in relation to wider clinic activity. Whilst this type of data collection was beyond the scope of this evaluation, we recommend utilising these sources of data for future evaluations going forward (see Discussion section, below)
In addition to the use of Attend Anywhere for clinical appointments within the Health Boards, a number of third sector organisations have been using video for counselling, advice services and hospice care. Two organisations in particular have been using it on a routine basis with service users: Rape Crisis Grampian (conducting 159 consultations during Jan-Dec 2019) and MS Revive (which supports people affected by multiple sclerosis: conducted 120 consultations).
3.2 User experience surveys
During Jan-Dec 2019, 679 online patient surveys were completed immediately after the video consultation, representing about 10% of consultations (see full details in Appendix D). Of these, 98% of the patients stated that they would choose the video option again.
When asked what mode(s) of transport they would have used if travelling to the clinic, most patients (61%) said they would have used a private car and 11% would have used train/bus. Other forms of transport included plane (6%), ferry (5%), taxi (4%), hospital transport (3%) and cycling (1%). For some patients (10%) the journey would have involved a combination of these different modes of transport. Only a small minority of patients said they would have walked (4%) or cycled (1%) to the clinic (graph in Appendix D).
According to the surveys, the average (estimated) distance they would have travelled (one-way) if going to the clinic was 51 miles, ranging greatly from less than one mile to 1300. (See full graph in Appendix D.) It was also reported by some (17%) that the Health Board would have paid for the journey; of these the average distance travelled was 104 miles.
The benefits and disadvantages perceived by patients are presented in Table 4. The main benefits included saving travel (stated by 72% of the sample), convenience (62%), saving time (57%) and saving money (39%). Relatively few negatives were reported by patients. The main negative was not being able to hear the clinician properly (7% of respondents) and not being able to see the clinician properly (4%), with some saying that a face to face appointment would have been better (3%).
| Benefits | % reported |
|---|---|
| Saved travel | 72% |
| Convenience | 62% |
| Saved time | 57% |
| Saved money | 39% |
| Did not have to wait as long for the appointment | 29% |
| Did not have to take time off work | 28% |
| Did not need someone to take me | 23% |
| Because of my condition it was safer/easier | 23% |
| Did not have to arrange child care | 13% |
| Other* | 2% |
| Disadvantages | % reported |
| Could not hear the person properly | 7% |
| Could not see person properly | 4% |
| Face to face would have been better | 3% |
| Had to have another appointment face to face anyway | 2% |
| Could not find somewhere private to conduct the call | 1% |
| Took longer to arrange | 1% |
| Use mobile data allowance | 1% |
| Cost money to do | <0% |
| Was too complicated | <0% |
| Other** | 3% |
* examples of 'other' benefits included feeling more comfortable at home and less stress from journey
** the majority of 'other' disadvantages related to the technical connection or duration in the virtual waiting area.
In most cases (76%), patients reported that consultations ran with no technical problems. Of those reporting technical problems, the issues mainly related to audio-video quality (e.g. moments of sound loss, lack of synchronisation between video and audio), as opposed to complete technical failures that prevented use. However, some did report delays in establishing a connection or the call dropping out during the consultations.
During Jan-Dec 2019, 755 clinician surveys were completed, representing about 11% of consultations (see full details in Appendix D). Of these, the majority (71%) reported that the consultation ran with no technical problems. Around 17% of the clinicians felt that such technical issues impaired the consultation.
The benefits and disadvantages perceived by clinicians are summarised in Table 5. The main benefits reported by clinicians included avoidance of travel for patients (56%) and themselves (38%). It was also felt that the video option made it easier and safer for patients with mobility problems due to their health condition (10%). Another perceived benefit was reduction in appointment duration (20%). Although, in some cases (2%), it was felt that video actually made the consultation longer.
| Benefits | % reported |
|---|---|
| Saved service user travel | 56% |
| Saved clinician travel | 38% |
| Took less time | 20% |
| Avoided patient travel by plane/ferry | 14% |
| Avoided use of patient transport | 11% |
| Safer/easier because of patient's condition | 10% |
| Other* | 8% |
| Disadvantages | % reported |
| The video and audio quality impaired the consultation | 17% |
| Face to face would have been better | 8% |
| Could not do everything via video, needed to arrange another appointment | 2% |
| Service user/patient was uncomfortable with the technology | 2% |
| Appointment took longer | 2% |
| Other** | 9% |
* example 'other' benefits included more rapid assessment of patient, allowing patient to attend while at work and seeing the patient despite adverse weather conditions
** example 'other' disadvantages included minor technical issues connecting and assistant needed for the patient using the technology.
3.3 Which clinical conditions and services were [un]suitable for Attend Anywhere?
Conditions and services for which Attend Anywhere worked well
Our interviewees affirmed a consistent finding from previous research - that some but not all conditions are appropriately managed through a remote video consultation. Examples of clinical conditions that seemed well-suited to the remote medium included:
Routine follow-ups of chronic, stable conditions, especially those monitored using evidence-based protocols and biomarkers (blood tests), where the main purpose of the consultation is to confirm that the patient remains asymptomatic and to give and discuss the test results.
"I'd say the majority [of Attend Anywhere for routine follow-up consultations] go well. Patients get told they're responding well to treatment. See you in a month, [they ask] do I have to come to Inverness, [the reply is] no, we can do it via Attend Anywhere, and they're delighted." (#71 Penelope, Macmillan nurse)
"Renal medicine for example. We've always had good remote support from the renal physicians, they were always happy to give advice based on blood results, now they've got one more tool with the video link." (#33 Lynne, GP and physician)
"There's no difference [between face to face and video appointments]. He always asks me the same questions." (#43 Patrick, haematology patient with chronic blood disorder)
"For our service there are a lot of appointments that are routine reviews, prescribing, that don't need that level of intensity, so video works ok for that… New patients we don't do via video, but for return patients you don't have to examine. Say you have to examine lymph nodes, or chest. If you have to do that regularly, then there is no point doing it via video link. But say you have someone with lymphoma, and after one or two courses of treatment, there is nothing left to find." (#58, Richard, consultant haematologist)
Fracture clinic follow-ups, in which the patient is X-rayed locally before a video consultation with orthopaedic specialist who reviews images and can gain a view of the recovering limb via tablet or peripheral camera.
Other surgical follow-ups, in which the review of their recovery or treatment outcomes can be reliably determined by a combination of the patient's accounts and visual assessment that does not require physical contact, such as hand trauma rehabilitation.
"The hand tendons patients work for these [video] follow up appointments because as long as I can see the hand move, I know the tendons are attached. I don't necessarily need to feel it. So I know there has not been a failure of the surgery." (#71, Michelle, physiotherapist)
Some psychology and psychiatry where the main form of management is talking therapy, with or without medication.
"My case load is about 50% personality disorder. Of the rest, 25% are schizophrenia or schizoaffective, and the other 25% are anxiety, depression or OCD [obsessive-compulsive disorder]. Most of these would be eligible [for video consultations]. I wouldn't see new patients but the follow-ups, fine." (#2 Jake, psychiatrist)
Counselling and advice services, involving listening, talking and providing information.
"They can do it from where ever they think is best, they can be in their own home, sitting in a car. It is completely confidential… The whole subject matter comes up quicker and trust is easier to build. And if they feel safe they find it easier to talk." (#68 Esther, Rape Crisis support)
Dietetics e.g. adults with obesity and "fussy eater" children.
Speech and language therapy, including work on breathing and voice control for children and adults with quiet voices
"Some kids who'd been reluctant, but when they could see themselves on the screen, it seemed to empower them." (#39 Louise, speech and language therapist)
Attend Anywhere was also used for more complex telemedicine arrangements, in which a GP with special interest or secondary care clinician (consultant, specialist nurse, physiotherapist) connected with the patient to a tertiary care specialist:
Chronic pain (GP with special interest links to tertiary care pain clinic).
Dermatology (dermatology specialist nurse links to consultant dermatologist).
Pre-operative assessment (specialist nurses examine patients locally, using a peripheral camera to allow an anaesthetist to assess the patient's pharynx via video link).
Respiratory conditions (a generalist nurse examines patients locally, links to a respiratory consultant and specialist respiratory nurse via video, using an electronic stethoscope if needed).
"[We use video for] just about any respiratory condition: bronchiectasis, COPD [chronic obstructive pulmonary disease], asthma, ILD [interstitial lung disease]." (#4 Niamh, specialist respiratory nurse)
"The nurse at the other end examines the patient and does the breath test. And then, I chat to the patient, then I come off the screen to dictate the letter, then Niamh [specialist nurse] stays on the video with the patient to start the self-management education." (#3 Moragh, respiratory consultant)
Cancer care (Macmillan nurses support and examine patients locally, as well as giving and overseeing cancer medication; they sit in on patients' video consultations with oncologists, attend multidisciplinary team meetings by video link; and liaise with other specialist nurses e.g. stoma care).
Interviewer: "Can you give me an example of how cancer care works with Attend Anywhere?"
Respondent: "Sure. Here's a patient, [type of cancer], they'd got progression of disease and a lot of treatments have been problematic, so we needed to discuss their last options. It was a combination of chemo[therapy] and a targeted therapy. So we had a long consultation [via video link with the consultant oncologist] about what's available, weighing up the side effects bearing in mind this patient's history. And it turns out that with this drug, only one in four will benefit. So there was a long discussion with the wife present, and we all had to be realistic - what if you're in the 3 out of 4 who don't benefit? So they said they'd think about it and we fixed up for me to visit them at home 48 hours later. It was a very difficult, emotional consultation. Considering whether to take treatment. That sort of consultation is normal for us on this side of the service." (#26 Leanne, Macmillan nurse)
Palliative care (Macmillan nurses oversee terminally ill patients, linking with palliative care consultants and hospice nurses and pharmacists by video as needed).
'Team around the child' (for children with complex needs, a video consultation can bring together multiple specialists including the GP, paediatrician, educational psychologist, occupational therapist, speech and language therapist). We met one parent who had hosted such a meeting in their home, with four staff attending in person and five linking via Attend Anywhere. A specialist wheelchair service based in Glasgow was also involved in this case:
"We had a new buggy delivered. They [wheelchair service] showed us the same buggy their end, showed us how to take it apart put back together, adjust all the supports. That saved us a trip and saved a long wait for the appointment. It was important because early intervention is recommended for all children with major disability." (#38 Leonie, parent)
Stroke rehabilitation (healthcare support worker with the patient in remote site, linking with neurologist or rehabilitation specialist at specialist centre).
Pulmonary rehabilitation classes (in which a respiratory physiotherapist takes a group of patients through an 8-week course).
"Pulmonary rehab. It's for COPD, any chronic respiratory condition causing breathlessness. It's physio led, physical exercises repeated over 8 weeks, and then you measure how able they are to recover. It won't strengthen their lung function, but it will strengthen their muscles. They will learn that they'll get breathless, but that breathlessness is safe. They learn pacing. We've started doing it by video in a hub and spoke model, class in Fort William of 8 people, using the Near Me screen. We have tried to do it with patients at home, but you get the dog barking and the doorbell ringing in the background! Otherwise if you lose a physio you lose the class." (#4 Niamh, respiratory specialist nurse).
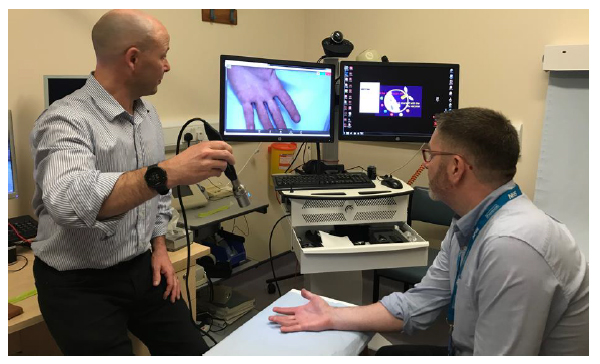
Hand surgery (physiotherapist runs a remote hand clinic, using video link to specialist hand surgeon in tertiary care centre, Figure 4 below.
An important observation on these more complex care arrangements is that the pairings between generalist and specialist appear to be ad hoc and based on strong interpersonal relationships with a high degree of trust and positive regard. The list above should be read as a selection of examples of where enthusiastic clinicians (innovators, champions and change agents) have made the service work, not as a generalisable or exclusive list of where Attend Anywhere will work.
Contra-indications and Cautions
The above examples all feature either conditions for which consultations are highly predictable or ones in which a clinician is present at a remote centre with the patient. Conditions for which our interviewees felt that it would be difficult or impossible to offer the service via Attend Anywhere include the following (note that the quotes are anecdotal and included for illustration only):
Poorly-defined conditions, where each patient is likely to require a different set of investigations and different package of care, and this cannot be predicted in advance.
"We wouldn't do the fibromyalgias by VC as they need working up; they [rheumatologists] want clearly-defined stuff like sacro-ileitis, inflamed joints. […] And the very general stuff - medicine, surgery, paeds - is too broad for remote." (#33 Lynne, GP and physician)
Rare conditions, where the volume of work from the remote site is insufficient to fill even a small clinic.
"We had a couple of teens with eating disorders a few years ago; we thought we might set up a remote clinic, but they've gone now. There's not really anyone with a severe eating disorder locally now." (#33 Lynne, GP and physician)
When essential tests or medication are unavailable locally.
"We're constrained by drug expiry dates. Haematology drugs for example have short expiry times so patients have to go to Inverness." (#24 Ellie, Macmillan nurse, remote site)
Some psychiatric conditions such as paranoia or certain forms of schizophrenia, in which part of the illness is a delusion about the technology (e.g. a belief that one's thoughts might be captured), or those in which the patient's mental state is highly unstable.
"There's safeguarding to think about, say if a patient becomes distressed and you can't de-escalate it, and they start self-harming, what if the tech cuts out. I'll give you two examples: an anxiety attack or the patient becoming hostile." (#2 Jake, psychiatrist)
Not all conditions could be cleanly divided into those for which Attend Anywhere was "suitable" or "unsuitable". In some, there was a trade-off that had to be managed using clinical and wider judgement. Frail elderly patients, for example, were a complex and heterogeneous group, about whom views were divided. On the one hand, clinicians and managers were aware that elderly patients were sometimes reticent to use new technologies and may have conditions (such as cognitive impairment or poor hearing or vision) that would make a remote consultation more difficult. Many also felt that the face-to-face assessment would provide much richer clinical and social information (one geriatrician talked about using his sense of smell as well as hearing and vision). On the other hand, most clinicians also recognised that such patients also found travelling difficult and it was sometimes difficult to coordinate carers to help them attend.
"For some elderly people … there's an NHS bus that runs from [remote setting] to Inverness, but imagine a frail person on that bus - it takes 3 hours and doesn't stop for the toilet." (#50 Pauline, clinician-manager)
"[With video consulting] I'm worried about its impact on frail people. In my experience, for elders it doesn't work, their relative ends up shouting to them. You get the odd one that Skypes their grandchildren. But mostly they've got sensory impairment or cognitive impairment and they need someone else to use the technology. And what you get is, the older person themselves is shut out of the conversation. It can be, it's often more the daughter you're talking to than the patient." (#45 Tom, geriatrician)
Another ambiguous clinical area was sexual health and conditions relating to gender. On the one hand, a remote component to the service provided the opportunity for consulting more anonymously; on the other hand, locally-based staff who knew the patient were sometimes inevitably involved.
"It's a small community. Everyone knows everyone. We've got a sexual health nurse, but we struggle with contact tracing. That's hard to do with a limited service; it could be done via Attend Anywhere. Sexual health is a specialty that's already done a lot with tech, like text messaging results. But gender [reassignment] stuff for example - patients might want to go away for that." (#33 Lynne, GP and physician)
In some specialties, there was perceived to be little need for video consulting. For example, conditions which were highly visual - notably, ophthalmology, dermatology, radiology and some kinds of plastic surgery - were often (though not always - see example below) better suited to asynchronous 'store and send' arrangements rather than real-time video consultations. In this model, photographs could be taken and sent by email to a distant specialist along with a clinical history; a diagnosis and management plan could be returned along with annotations to the image.
Several specialties (e.g. heart failure, diabetes) ran clinical networks in remote settings in which nurses or GPs with special interest worked from a community hospital, advised and supported by a consultant based on the main site. In most such cases, there was little need for video consultations with patients because the nurses had been upskilled to a level that allowed them to practise with a high degree of independence. Liaison with specialists, when needed, occurred by phone. Similarly, a specialist physiotherapist described telephone contact with the tertiary care hub (without the patient present) as "quicker and easier" than arranging a video consultation with the patient present (#34 Christine, specialist physiotherapist). However, see below for examples of the important added opportunities of the video service to support staff training and extended staff roles.
3.4 What were the technological benefits and challenges with Attend Anywhere?
Quality and dependability
Most patients and staff interviewed who had used Attend Anywhere were impressed with its technical performance. They described the technology as very dependable, easy to use and providing excellent visual and sound quality.
"We love it." (#31 Naomi, service manager)
"It worked great. I went to the Near Me suite in [remote] hospital and we had our chat, everything went perfectly. No problems. We could see and hear each other. Everything that we each wanted to say was said. Personal contact was missing but that didn't matter. Someone explained what it [the technology] was going to do, then once the link was established she went away. She would have stayed but I didn't need her." (#47 Hamish, patient, speaking about mental health consultation)
Staff and patients who had used previous teleconferencing software described Attend Anywhere as a "step change" in technical quality.
"In previous years we used video conferencing, Cisco then Jabber. There were big screens, there was lots of support but it really didn't work. [Interviewer: why not?] Technical issues - you'd go into a room and there wasn't a cable; someone had removed it. It was always a wee bit fraught, always a bit of an adventure what you'd find when you went to set up the clinic. You never knew what would happen. We got very good at workarounds. Then with Attend Anywhere it was much more reliable." (#3 Moragh, consultant)
"We had a patient recently, a new diagnosis of [type of] cancer, she'd had a previous video linked with the neurologist, using Jabber, for [neurological condition]. She didn't like it, didn't feel she connected well with consultant. When she was told we were using a video link for her oncologist appointment, she was apprehensive and didn't think she was going to get much out of it. Afterwards, the patient said "it was like she [oncologist] was in the room with me". And it felt the same distance apart as we would have been in the room." (#23 Patricia, Macmillan nurse)
Not all staff held negative views about Jabber (one of the video technologies that had been used before Attend Anywhere). Indeed, one or two interviewees who sang the praises of what they thought was Attend Anywhere were actually using Jabber. For example, a Jabber connection was used to undertake pre-operative assessment of surgical patients on the Western Isles who were booked to have their operation at the Golden Jubilee National Hospital near Glasgow, where some clinical services continue to use Jabber (due to compatibility problems between Attend Anywhere and the firewalls). The nurses' positive experience may be explained by the fact that they never had to set up the technology (they used it in a hospital that had good local IT support and a technical team always set it up and checked it before their clinic). Nevertheless, in most cases those who had gone from Jabber to Attend Anywhere preferred the latter. The few exceptions to this included situations in which the ability to control the camera were considered important for conducting a clinical examination, such as complex neurological examinations involving gait, limbs and eye movements:
"You have control, you can move it around, you can zoom in put right up to the eyes and see the pupils…For Attend Anywhere, if you wanted to move it around, you would need the person to take the camera and move it around." (#65, David, consultant neurologist)
A number of iterative improvements had been made in recent months to the basic Attend Anywhere technology. Staff were particularly pleased with the new screens, better-quality webcams and noise-cancelling microphone provided by NHS Highland, which greatly improved sound quality. The 'screen share' function within Attend Anywhere was also considered useful in consultations that would typically involve the sharing of visual information when conducted face to face. Whilst it was deemed possible to still undertake the consultation in the absence of these visual cues, the ability to retain this aspect of the interaction was considered important for effective dialogue.
"Particularly with IBD [inflammatory bowel disease] patients, I have been able to share the screen with them so we can go through things at the same time. It is particularly good for discussing scan results. Normally I set it up before I start the clinic, get the X-ray software up, results up, so I can flip between the two if required." (#59, Simon, Colorectal Surgeon)
Several interviewees described occasional problems with sound - either one party not hearing the other at all, or very weak sound despite settings on full volume. One of us experienced this latter problem when a patient who had planned to come to the local community hospital for an interview was informed they should not attend (because of an infection outbreak). Whilst the patient was happy to be interviewed via Attend Anywhere, the initial connection resulted in no sound and a re-dial produced only weak sound. Technical troubleshooting from the on-site staff could not resolve this. The patient, who used Attend Anywhere regularly, said this was the first time it had happened to her.
We heard a single account of one occasion when the audio worked but not the video (#38).
Some interviewees had minor complaints which they considered to be technical but which may have been due to how others chose to use the technology.
"That message "you are first in the queue" doesn't mean anything - it might say you're second but then he might suddenly come on." (#44 Victoria, wife of patient)[5]
Several patients and staff pointed out that it was hard to understand - and be understood by - clinicians whose first language was not English. Some tried to lip-read but found they were unable to.
When filling out the online evaluation form for Attend Anywhere, Lachlan (#12, patient) came to the question "could you hear the clinician ok?" He read the question three times and seemed confused. His wife said, "come on Lachlan, you could hear him, couldn't you?". He replied, "Yes, I could hear him perfectly well - but I couldn't follow him." (field notes, remote clinic)
The problem of not following clinicians' accents was the single most common concern raised by patients and healthcare support workers (who often accompanied patients in their video consultations). Some patients were keen to point out that they were not being racist and described the doctor as "nice" but incomprehensible. One patient had seen the same doctor in both a face-to-face appointment and a remote one and commented that they could understand what they said only in the former setting. Some commented that the doctors also had trouble following their strong Scottish accents.
Ease of use (and adjustments needed to use Attend Anywhere effectively)
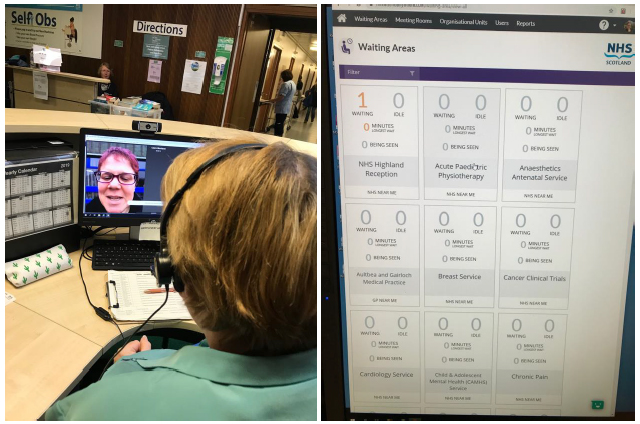
In general, Attend Anywhere was considered very easy and intuitive to use. The ability to connect to the virtual waiting areas via a consistent URL meant that patients were provided with a 'single point of entry' to a clinical department on an appointment letter and/or the Health Board website. Within NHS Highland, this functionality was further simplified for patients through a virtual reception desk. This meant that patients could access clinical services via a single button on the website, which some (but not all) services have implemented. Within NHS Highland, patient entry was managed by a main reception team who welcomed them and directed their video call to the appropriate virtual waiting area (see Figure 5, below).
"It has a single point of entry on the website. Previously [with other products], it was incredibly confusing for patients - there were different links for different specialties. Now they just press start and there's a video call happening. They even see the same receptionist [as they would if attending face to face], the real person comes on screen and chats to them, then moves them into the right virtual waiting room. We've made it easy for patients, we hold all the complexity." (#1 Debbie, clinician-manager)
Integrating the receptionist role in this way requires considerable effort and collaboration with outpatient departments.
face-to-face arrivals and Attend Anywhere video calls [6]
In other Health Boards, patients were either provided with the clinic-specific URL (e.g. in the appointment letter) or could manually select the relevant clinic waiting area on the Health Board website. In some services, the virtual waiting areas were managed by local reception teams, to mirror the workflow and processes of a regular clinic:
"From a patient perspective, if you turn up to the clinic and you check in with the receptionist, they know they are in the right place. If you have sat in the right place, if you have been sitting there for 15 minutes you can eye ball people and say you are still here. If you go on video you have nobody there, you have got a thing saying you are third in the queue but you can't see anybody. You wonder if you are in the right place. So if received by receptionist at least you get that reassurance." (#81, Denise, Project Manager)
Other services relied on the clinician to monitor the waiting areas themselves. Whilst this was mainly considered manageable on a small scale or during the early stages of service development, many believed an administrator or receptionist would need to be involved if the service was to become more routine and scaled up. But how this would be structured and managed would depending on the existing administrative structures, workflows and roles:
"So when the patient arrives in the [virtual] waiting room they pop up on your screen, so you can see them waiting….I would know to expect the patient… If I was doing it on a larger scale, and if you were doing clinics that were both part [face to face] and part Attend Anywhere, having a receptionist checking in the waiting room would be a good idea. The biggest problems would be making sure you had receptionists that were happy to deal with it." (#112, Gemma, consultant dermatologist)
"The clinician would manage the waiting room. And have a list of patients and work through each patient that's waiting….We have included our admin support to do the letter and the appointment. But I think another job they will have to do is actually view the virtual waiting room during the day - just to make sure no one has popped in unexpectedly, or time up at the wrong time. Because patients do that all the time, even if they have the appointment letter. So they could potentially do that in the virtual waiting area as well. So we've got to think about all these things, and try to manage that" (#139, paediatric physiotherapist)
Despite Attend Anywhere being described as "simple" (by the Attend Anywhere CEO), and positive comments by clinical staff on the usability, there was still a learning curve before people became confident using it. Some but perhaps not all of the connectivity problems described above may have been due to lack of familiarity of the users with basic set-up issues such as ensuring that sound and camera are enabled.
"There are often connection issues, generally at start of call. Sometimes it can take 5-10 minutes to do the speaker and mic test, for example when it doesn't recognise the speaker or the mic, it's a faff getting set up. One of my colleagues adds 10 minutes to the appointment time." (#38 Leonie, speech and language therapist)
Clinicians also said they had to get used to consulting in a subtly different way to take account of the physical and symbolic differences in the technology-supported environment.
"I've modified my consultation style because of the lag [in sound transmission]. If you don't do that, there's a moment of over-talking and interruption. So now I give more time [after speaking] to make sure that the patient knows my speech has been completed. We use silence quite a lot in psychiatry anyway. At the beginning of the consultation I do what I call a "technical introduction" - I take 3 or 4 mins to explain to patient the technological process. There's a mini-script you need to go to. For example "if it cuts out, this is what to do"." (#2 Jake, psychiatrist)
Attend Anywhere had functionality to bring in clinicians or relatives from a different site (see example above 'Team around the child'). But this function seemed to be used very rarely. We observed one consultation in which the daughter of a cancer patient wanted to join the consultation (at the patient's invitation), but "these particular doctors won't allow it" (#8 Nicola, healthcare support worker). An elaborate workaround was proposed in which one of the staff tried to link the daughter in via Facetime on an ipad, but in the event, the connection failed. The doctor's reasons for not using the full functionality of Attend Anywhere were not clear, but may have been a combination of limited technical confidence and uneasiness about handling the more complex dynamic of a three-way conversation.
Material infrastructure and IT support needs
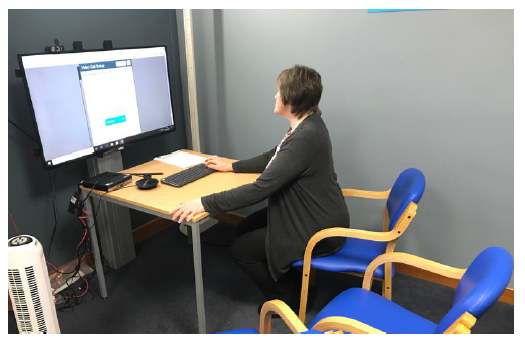
The clinician-manager who had led the introduction of Attend Anywhere to NHS Highland (#1 Debbie) had researched the optimal material surroundings for a high-quality video consultation and encouraged all remote clinics to use a common style. All rooms (or in some cases, the corner of the room that would be in view) were painted grey as this was the optimum for video consultations (for example, it reduced glare and improved the accuracy of skin tone). In addition, Debbie had helped supply all remote clinics in NHS Highland with high-quality peripherals such as the noise-cancelling microphones mentioned above.
"We're fortunate because we've got good stuff [equipment] in here. We got it because of Debbie and Near Me." (#19 Jennifer, nurse)
One or two clinics had been fitted out with highly specialised peripherals such as an advanced camera that produced a very high resolution, magnified image. It had been bought from the USA at a cost of £6000. This "scope" could be used directly (e.g. for skin lesions) or linked to an auroscope (for viewing the ear canal) or a long spatula (for depressing the tongue and getting a view of a patient's airway). The quality of visual images was exceptionally good.
"The Scottish TEC [Technology Enabled Care centre] couldn't find us one, we asked but they weren't set up to find stuff for us, only to help implement if we found it ourselves. I saw it in America when I visited the VA [Veterans' Administration]. The camera is good value because it is used by many specialties - dermatology, pre-op assessment (anaesthetists), rheumatology, hand surgery." (#17 Julian, physiotherapist)
Whilst excellent material infrastructure did indeed improve the technical quality of consultations, it usually meant that Attend Anywhere consultations had to be conducted from one particular room (often the largest and most comfortable consulting room in the building). In some places, this room was in high demand, sometimes for two different virtual clinics running at the same time. Occasionally, there was friction between a healthcare support worker supporting a virtual clinic and a consultant who wanted to use the "nice" room for their own face-to-face clinic.
In some but not all staffed clinics, the video room had been arranged to emulate the physical arrangements of a face-to-face consultation. In one oncology setting, for example, there was a small table between the patient and the screen (Figure 6). The patient would lean on it, rest a bag or notepad on it, and view the doctor on the screen "as if" they were consulting across a desk. This was viewed as a positive but serendipitous arrangement.
"That table was a bit of a mistake. We were told we'd need something to put the two bits of kit [e.g. microphone] on, when it turned up it was twice the size we thought we'd ordered, but it ended up really good. We bring them a cup of tea." (#26 Leanne, Macmillan nurse)
The need for local infrastructure to optimise the call may be one reason why only a small fraction of Attend Anywhere consultations occurred in patients' homes even when this option was available.
"Staffed clinic rooms tend to be used for three reasons: internet connectivity is really poor in many people's homes; the device itself is usually better - we've got the nice screen, the high-quality microphone and so on; and some calls need clinical support. We also have about 15 unstaffed clinic rooms. Hit the button and it turns on, they don't need a staff member - it's locked down, can only get to the NHS Near Me website." (#1 Debbie, clinician-manager)
"I'm not keen on that [patient at home]. It is a bit like a phone consultation. Phone consultations are really bad because the patient is not always somewhere appropriate when you ring the phone… So you don't quite know what you are going to get with the home ones. And lighting, that can be a problem. Depends where they 'park' themselves. You may get kids screaming about. So when they have to go somewhere and present themselves, it is better." (#58, Richard, consultant haematologist)
The material infrastructure in remote sites required (but did not always have adequate) IT support, as we discuss below.
For services running Attend Anywhere appointments with patients at home, it was necessary to ensure patients had access to the appropriate technology and were aware of the requirements for a good quality consultation. This was often achieved through a combination of direct communication and information resources provided to the patient upon booking the appointment.
"When we started, it was quite a bit of work because I would look at the return waiting list Near Me, and the patient would have to be contacted to explain the whole process, and do a line check…. If the patient was not able to use Attend Anywhere, and wanted a phone appointment -there was quite a lot of backwards and forwards. Now, when the person is vetted, they get sent a letter saying you have been vetted for a Near Me, please do a line check. So now, the onus is on the patient to do the line check, and if they don't like it or can't do it, my number is on the letter. And then I can offer the option of the Near Me room". (#61, Beverley, medical secretary).
Another form of support for patients at home was the opportunity to test call and gain some familiarity with the technology. Whilst the Attend Anywhere system allows for users to test the connectivity of the device, some services enrolled staff to allow patients to call them in preparation for their appointment. In NHS Highlands, this was formalised further through the virtual reception desk, in which patients could call the central virtual reception desk at a designated time every Friday.
Local clinical support for Attend Anywhere consultations
Healthcare support workers (sometimes) and Macmillan nurses (almost always) sat in on the consultation with the patient. They always offered to leave the room but were often asked to stay - either for emotional support or to help them understand what the doctor was saying. Sometimes, they were needed to undertake a limited physical examination or adjust equipment under instruction from the doctor by video, after which they usually offered to leave (and were usually asked by the patient to stay).
"Maggie is a healthcare support worker who works with Diane. She's reassuring and down to earth. She's good at supporting people with the tech, she settles them in and talks them through it. She's very enabling". (#33 Lynne, GP and physician)
[Interviewer: What kind of patient would want you sitting in with them?] "Epilepsy for example. They seem to want me in with them, some have LD [learning disability]. Rehab - knees, aches and pains, neuropathies, they sit there, I have to test their reflexes, I get my tendon hammer, and this thing with my finger and their nose [a test for tremor], and watching them walking up and down; these are follow-ups, their first appts would have been face-to-face so we're checking against a baseline. Sleep apnoea, quite a few have to have their machine adjusted, there's a mask, they may need new mask and filters, there's a data card that records everything, I have to send it to Inverness via internal mail". (#42 Oona, healthcare support worker)
"Chemo[therapy] patients when they're on treatment, they're not feeling 100%. We [Macmillan nurses] can explain things they don't understand or pick up. It's a 3-way conversation but we know the main conversation is between consultant and patient, but he looks for information from us as well. The interpretation of a question can be different between patient and oncologist. That's why we attend with them - we're with them throughout their whole journey". (#41 Penelope, Macmillan nurse)
Some patients were opposed to using Attend Anywhere from home because a particular member of healthcare staff (whom they mentioned by name) would then not be available for emotional support or to help explain the specialist's words
In some clinical settings, the support of a health practitioner on the remote end was necessary for conducting physical tests and assisting the specialist with remote examinations. The familiarity and understanding between the clinician and remote practitioner often played an important role in collaborating and coordinating actions effectively for the purposes of the examination.
"Because [the Near Me nurse assistant] just needed a few tips here and there. And by the end of the first consultation, there was, occasionally I would have to say can you do this, can you do that, she would run through the examination part of it. She was good of course and I had already worked out how to ask her to do things in a way that would work. Which also meant I had to modify my neurological examination." (#56, Bebak, consultant in neuro rehabilitation)
Issues with other technical systems
The routine use of Attend Anywhere for remote consulting relies on the configuration of other technical systems. One major challenge has been the integration of video (Attend Anywhere) appointments within the clinical administration systems used across secondary care services. Most, but not all, Boards use TrakCare, but not all are on the same version. Most services seek to incorporate Attend Anywhere appointments within their existing face to face clinic ('mixed' clinics). However, the ability to set up TrakCare to account for the mixed arrangement of appointments was variable across Health Boards, depending which version was being used. With the 2016 version used by some boards, appointment letters can only be generated for one appointment type (i.e. face to face or video). This has meant that some teams have had to develop 'workarounds', either by manually creating appointment letters or by running 'shadow' video clinic schedules alongside the existing face to face clinic schedule; both of which require additional work on the part of administrative and/or clinical staff and increase potential for error (e.g. patient receiving two conflicting letters, double booking):
The dependability of Attend Anywhere has also been affected by hospital network configurations, such as security and internet browser settings. In one Health Board (Golden Jubilee National Hospital), efforts needed to be made by the IT staff and the Attend Anywhere support team to resolve problems routing the video call through the local network. After a lot of diagnosis and work, it was established there was a very unique issue to do with a partially blocking web cookie. In this case, the workaround was to wipe the internet browser cache before loading the application. Whilst this was an effective troubleshoot option, it was not considered to be a scalable way for clinicians to run their video clinics.
As noted above, Attend Anywhere works on internet browsers Google Chrome and Apple Safari, but not on Internet Explorer. As Internet Explorer remained the default internet browser for NHS computers in many boards, varied approaches were taken to enable access to Google Chrome on NHS computers for the purposes of using Attend Anywhere. Up until January 2019, Google Chrome was not recognized as a 'supported' internet browser within the NHS Scotland National Infrastructure Standard, which raised governance and security concerns among some eHealth departments, further holding up implementation efforts.
Although Google Chrome has posed challenges for some services, the national NHS Scotland rollout of Microsoft Office 365 will mean that Microsoft Edge (which Attend Anywhere is compatible with) will soon become the standard NHS internet browser, and so should overcome these issues.
3.5 What value did the Attend Anywhere service bring for patients, staff and the service?
Almost everyone we interviewed who had been personally involved in the Attend Anywhere video consultation service had positive things to say about it. Clinical directors used words like "quality improvement", "convenience" and "choice" to describe what they saw as a significantly improved patient experience. Below, we describe some specific aspects of the added value (both financial and non-financial) of Attend Anywhere, before (in the next section) describing staff and patients' concerns that Attend Anywhere might bring negative value.
Less need to travel
An obvious and frequently-mentioned advantage of video consulting is reduced need for patients to travel. This was linked to lower NHS and patient-borne costs, since some but not all costs of travel for NHS appointments are reimbursed, and (assuming growth of the service) a potentially reduced carbon footprint for the NHS in Scotland. Staff talked of the vast distances that some remote patients needed to travel for what was sometimes a very short and straightforward appointment. Those on islands were dependent on planes and ferries, and parts of the mainland were also many hours' drive (often on poor roads) from their nearest hospital. Older patients in particular were often not physically well enough or strong enough to make the round trip in a day. Some were simply too sick to travel.
"In the winter, there's often fog, the flight might be late, then they miss their appointment, or they might miss the flight home, or it's delayed. I've had people vomiting in plastic bags that they had to buy from WH Smith at the airport with their own money. Not good". (#24 Ellie, Macmillan nurse, Western Isles)
Both cancer and respiratory clinicians described terminally ill patients who had been reluctant to consult by video until they were too sick to make the journey. In both cases, the patient was said to have been very satisfied with the remote consultation and had asked for their next consultation to be by video.
The benefits of less need to travel were confirmed by patients, in terms of satisfaction with the service and living with their condition:
"It was more efficient because I wasn't exhausted from the journey, my mind was fully engaged. The dialogue itself was far more constructive…. So I would say it was actually better than a face to face. Because I was in a better physical and mental condition to describe my symptoms of the preceding six months, since I had last spoken to her." (#83, Oliver, patient, respiratory).
Reduced need to travel was seen as a means to improve equity of service delivery, in which service access may be restricted by travel distance and/or limited mobility.
"For patients that have had repairs to tendons in their hands, we have clear management guidelines where we will put them in splints for five weeks and essentially immobilise their hands…. So it means that they can't drive, they can do basic movements, but it immobilises them quite a lot and impacts their independence. So if have a patient that lives three hours away and they can't drive, it is very difficult for us to see them. We also say as part of the guidelines that we want to see them once a week to make sure their tendon repair is still functioning... But that then becomes very problematic because they need to get some form of transport to see us for an appointment…. Patient benefit has always been the driver. It was more about us being able to provide equitable care. We really felt if Jo Bloggs who lived round the corner can be seen as often as we like -- but there was doubt about asking people to drive in." [#71 Michelle, physiotherapist]
Faster and more direct access to specialists
Before the introduction of a video consultation option, patients in remote areas faced a long wait until a specialist visited their local clinic (in some cases, such visits occurred only every three months), or a long journey to a specialist tertiary care centre. Video consultations allowed them to get specialist opinions much more promptly, reducing stressful delays in diagnosis.
"I've got a [slow-growing cancer]. I'd lost weight, and gone to Inverness for a CT scan. It was initially diagnosed as [a fast-growing form of] lung cancer. My [specialist respiratory oncologist] is Dr X--- who's based down in [English town]. Normally that would have meant a long wait but my GP arranged a video consultation the same day I got the cancer diagnosis. Dr X--- was able to reassure us that he didn't think it was lung cancer, he said the prognosis is not as bleak as you might think. I had lots of small areas which were thought [by the radiologist who reported the CT scan] to be met[astase]s but they turned out to be inflammation. But on that first day, my GP read the CT report out to me and it was ooh heck. When I spoke to Dr X---, I could see his face, it was very clear, we had no trouble getting through. Even to wait a few days with that sort of diagnosis would have been awful. He arranged a biopsy, I had that within a couple of weeks and it confirmed he was right. That was 18 months ago." (#37 Trudy, cancer patient living in Western Isles)
A Macmillan nurse at one remote clinic, which was based in a community hospital, described how they had wheeled a patient on a bed from the ward to the Attend Anywhere consulting room in outpatients to have a video consultation with their oncologist during an inpatient stay for a complication of chemotherapy.
Some interviewees in remote sites described arranging a prompt video consultation to provide a rapid, one-off specialist consultation to reassure the patient and (in particular) back up a decision made by the local doctor or nurse, perhaps when no active treatment was the recommendation. They saw the video service as helping to avoid situations where patients waited months for a specialist opinion and anticipated an operation, expensive test or cure.
"The other thing is if we send them to Inverness, the patient gets their hopes up." (#45 Tom, geriatrician).
Improved access to urgent specialist opinion was also demonstrated in the Ophthalmology setting, in which A&E consultants and optometrists could establish a live video stream for a second opinion on hospital referrals for eye problems. Instead of (what would typically be) a telephone interaction between clinicians, the ophthalmologist could view the patient's eye via video camera attached to a slit lamp. This new service model was found to provide more timely diagnosis and reduce unnecessary hospital admissions.
"When you see something [via Attend Anywhere] that is instantly recognisable like a contact lens related ulcer or various types of keratitis or marginal keratitis, you know exactly what it is and you know what treatment is going to work for them, and you can start that treatment and say 'I don't need to see them'. A phone call - you might get the description, but you would never commit yourself because the examination skills on the part of the emergency department is so variable". (#91, James, consultant ophthalmologist).
More holistic care, linking with the home and family
Many GPs, and some consultants, spoke of the additional information they gained when video-consulting to patients' homes about how the illness was affecting them and their families. They spoke of gaining insights into family dynamics (for example, seeing interactions with anxious or overbearing relatives) and observing aspects of patients' and families' lifestyle.
"I've done a couple [of video consultations] from patient's home. There was a child, living in [remote part of island]. Good internet at home. The kid was 18 months old. The parents didn't have to take him to a clinic. I just sent them the link to Attend Anywhere. They just clicked on it at the right time. They [parents] were sitting on sofa in living room, very laid back, and when they were talking about things they fed the boy, they could get stuff from kitchen and ask "is this ok to give him?", and the kid was on floor the whole time playing with his own toys. I did another one with another parent who wasn't feeling well, we just shifted it from clinic to home." (#29 Lisa, dietitian)
Clinicians occasionally seized an opportunity to educate family members in caring tasks or emergency management.
"There was a patient with [a degenerative lung disease], and he has anxiety too. He had this breathless attack on the video. You wouldn't have wanted it to happen but we were able to support the daughter to assist him. The relatives being able to be present is a great advantage. And if we do it via VC [video consultation], the relatives are more likely to attend." (#4 Niamh, specialist respiratory nurse)
Overcoming reluctance to see a doctor and visit clinical spaces
We found two examples of patients who had overcome a fear of hospitals or doctors by consulting remotely. In one case, the patient was a teenager who had been referred to a mental health team but had refused to attend. The teen agreed to a remote consultation and felt that it was "a bit like playing a video game in my room"; they subsequently agreed to attend a face-to-face appointment with the same doctor. In the other case, past trauma had made the person extremely reluctant to be physically close to a doctor:
"What I enjoyed about [the video consultation] was I have insecurities from when I was a child. I've overcome that, mostly. But I was nervous about being in a room with a surgeon, him taking my [outer garment] off looking at my [part of body]. I was a victim of [briefly describes past trauma]. Having a smear test is the worst. What this appointment did for me is it helped me overcome some of that. When [my clothing] came off and everything, it was ok. The surgeon and the patient, he's over there [in a different building] and you're in here. And the fact that he was there and I was in here, it was much easier to communicate." (#15 Imogen, surgical patient).
Staff also talked about situations when video helped build rapport with individuals that were anxious about engaging and meeting with others to discuss sensitive issues:
"We went out to see a patient - and his reaction to us was quite upsetting, he could not cope to seeing the physios and was quite distressed… At that same time Attend Anywhere had just come in, and we thought this might be helpful in this particular instance…. So we had a virtual consultation. And he actually looked at the physio - made eye contact - for the first time. And was able to say to her what he was worried about… The plan was to alternate face to face and virtual appointments. He actually decided not to use virtual. But I think that option gave that bridge, breaking the fear he had." (#139, Holly, paediatric physiotherapist)
Financial savings to the service
Although this evaluation does not include an economic evaluation or an exploration of the system-wide financial impact of Attend Anywhere, nevertheless the Scottish Government were also interested in finding out people's views on financial savings and what local assessments of impact had been made. One important saving was more efficient use of staff time. Clinicians and managers gave numerous examples of substantial savings in staff travel time when they provided a video outpatient clinic from a 'hub' hospital instead of traveling to a remote 'spoke' clinic.
The use of video links in emergency situations sometimes saved a costly (and perhaps risky) transfer of a patient for a specialist assessment:
"Let's say the patient presents to [remote rural hospital] in distress, maybe if they're detained under the Mental Health Act, you'd need to take nurses off the ward to accompany them, but by the time they get seen, the crisis has settled. So they get sent back at a waste of 7 hours of ambulance and nurse time." (#2 Jake, psychiatrist, Highlands)
Whilst there were many examples of such savings, some video consultation clinics generated considerable additional work for staff in remote clinics (see quote from Diane below).
Home visits were also raised as potential areas for saving practitioner time and travel, where clinically appropriate. In the following extract, the respiratory physiotherapist was able to see a patient with lung disease for a 20-minute video appointment, when it would typically necessitate a two-hour visit to their home because a phone call would not provide sufficient visual and contextual information:
"The other thing you get with Attend Anywhere, you can see people, you can see how breathless they are, you can see the colour of their skin, you can see how much effort they are putting in their breathing. You can hear someone is breathless on the phone, but if you are really put a lot of effort in your breathing your shoulders will move differently, you might go a bit blue so it is really helpful seeing that…Home visits are very time consuming… to do a home visit you are talking at least two hours, whereas the Attend Anywhere visit would take 15-20 minutes…. I may have been able to do it over a phone call. But probably would have ended up doing it as a home visit". (#66, Natalie, respiratory physiotherapist).
With regard to using Attend Anywhere as an alternative to the patient attending clinic, most staff participants thought that video appointments were of shorter (or about equal) duration than face to face appointments. Shorter durations were attributed to engaging in less 'orientation' and 'social' talk. This time saving was perceived by staff to be beneficial in terms of 'keeping to time' and managing workload (e.g. spending more time with complex patients, completing paper work in allocated clinic time), rather than increasing capacity or volume of activity.
"Both my Near Me appointments and my physical appointments are 15 minutes, same length of time. However, Near Me - as soon as the patient is there it is instantaneous having a conversation. Normally after five or ten minutes of conversation we can conclude it. And that give me five minutes to do dictation, paperwork, complete any referral letter, complete any investigation forms and such like that well within the 15 minutes. It allows me time to look at results before the next patient is there. So it doesn't tend to run on. But in a traditional clinic, you go out and greet the patient in the waiting room, wait for them to come in, take the jacket off, sit down, introduce, shake their hand - it's three minutes gone already. And then examine them if required. So then it is 15 minutes plus. Then I've got to do administrative part of things. So I find physical clinics tend to get crammed and tend to roll on. The time just disappears." (#59, Simon, consultant colorectal surgeon).
Some clinicians also reported that capacity and cost-saving could be made through reductions in DNA (did not attend) rates:
"The number of DNAs in my Near Me clinics is virtually zero. I used to have a large proportion who did not attend. For two reasons; one was they would forget because of cognitive impairment. A second is a large number would be waiting for ambulance and patient transport to pick them up, and they would be one or two hours late and miss their appointment…" (#56, Bebak, consultant in neuro rehabilitation]
Staff convenience, flexible working
Many clinicians pointed out the greater flexibility offered by video consulting. One described being able to continue running some of her clinics from home while off work with a complication of pregnancy. Several consultants lived and worked on the Scottish or English mainland but ran a regular clinic on one of the islands. In some cases, these clinicians had previously lived on the island or travelled there for a face-to-face clinic, but their circumstances had changed so the video option allowed them to continue to see their 'own' patients.
One or two interviewees mentioned staff safety issues with home visits.
"The smoking cessation team, it's a small team and they're pressed. They used to go to [remote setting] but didn't want to go into patients' smoky homes." (#32 Eilidh, service manager)
The uncoupling of clinical delivery from the geographical location of the clinician meant that clinicians could provide input to particular patients when they had a relevant sub-specialist interest. A speech and language therapist with a particular interest in Parkinson's Disease, for example, could be linked via Attend Anywhere to a patient based in another therapist's catchment area.
We heard two examples of consultants who were depicted as offering poor value for money, because they allegedly used a part-time contract for video consulting to increase their personal earnings but were not interested in developing local staff or contributing to improving the local service.
"[Name of] clinic VC Mr [name]. We should be doing it [only] if it's giving us something we haven't got. He's doing it from [country in mainland Europe]. Having him on site is important; when the [name] clinic is going on, we should have a specialist on site. He's using it as an excuse to earn a ton of money and stay in [country]. His family is in [country]. He gets 12 PAs [high salary] a week." (#25 Fiona, clinical service manager)
In addition to the time and financial saving, reduction in travel to the 'spoke' clinics provided greater work satisfaction for the clinicians:
"There is a time saving for me, so I don't have to think I've got to get to this location, I have to potentially be away from home. From a personal satisfaction, I hated driving over to [remote site]. I detested it. It was a long day. I ended up getting a headache. Patients were probably not getting the best of me because it was an early start. So from a personal satisfaction and what the patient gets, I feel better. The patients are getting a better me and better service." (#57, Debra, epilepsy advanced nurse specialist).
Attend Anywhere as an opportunity for radically new service models
The facility for technically high-quality, dependable video consultations through Attend Anywhere offered the opportunity for specialists, generalists and healthcare support workers to collaborate in new ways through extended staff roles and transformed working relationships. In particular, less specialised staff could undertake some specialist functions with remote support (see examples of complex care arrangements above). As noted previously, these novel arrangements appeared to emerge from prior working relationships between particular individuals that were characterised by mutual respect and trust.
In all cases where new models of care were described, the staff who had developed them were extremely positive and depicted the new model as having greatly improved the patient and staff experience and (usually) solved a specific problem that had existed before, such as a gap in provision or a safety risk.
One major benefit of such arrangements was training and professional development of the remote staff member. In all the quotes below, the less specialised staff members gain bespoke training from a specialist clinician, allowing them to undertake aspects of an extended role under that supervision, thereby feeling valued and gaining professional fulfilment.
"I'm learning lots, can do the hand exams myself now. I know what he's going to say." (#17 Jonathan, physiotherapist who runs a hand clinic linking remotely to a specialist hand surgeon)
"It's [the shift from a visiting dermatologist to a remote service] been a huge change for me. My day to day has gone from following his instructions every couple of months on very minor things to diagnosing, carrying out biopsies, and managing the service. My learning curve has been huge. […] The first remote consultant was not very experienced in teledermatology, but the next one was. I've learnt how to take better images with her instruction. I'd never used a gel coating under a dermatoscope. She knew it enhances the image. You're learning all the time.. […] We've been able to feed back to GPs, I'm taking images to forward to someone else, they send them back highlighting things, we then feed them back to the GPs. I'm one module away from a PG (Post-Graduate) Diploma through [distance learning provider], all online. It was as we were developing the new system, I thought "I'm going to be expected to do much more at a much higher level". I've got a regrading going through. .... So it upskills locally. You have the support via technology to do new things." (#21 Barbara, specialist dermatology nurse)
"I've used it [Attend Anywhere] to give Makaton training. I'd seen [Makaton] used in a nursery setting a while back. [Interviewer: you mean for kids with learning difficulty like Down's?] It is used for that, but you can also use Makaton for normal kids who have delayed language. I gave them [nursery staff in remote site] a link to my Attend Anywhere room, they can come directly into my room [using the 'meeting' function], so that avoids using the virtual waiting room. Nursery staff in [remote site] all sat round the table with a laptop. I shared my screen, showed them stuff, then I set them some activities and watched what they did with their hands. They could ask me questions, stop me if they needed. It worked well." (#39 Louise, speech and language therapist)
[Interviewer: Do you go on a course to learn to do physical examinations?] "I've got courses coming out my ears, but it's mostly the consultants who teach me, it's the best teaching ever. I was taught spirometry by a professor, the loveliest doctor ever. Professor N---. He's so high up, his wife is also a doctor. He works at the [specialist London hospital]; he flies to [Arab country] to give second opinions to Sheikhs. He's an absolute sweetheart, nobody could have taught me better. You get to know the way they like to do it, it can be very unique." [#42 Oona, healthcare support worker)
"Orthopaedics for example. With Near Me [video connection to Inverness], we're not just a backwater hospital seeing sprained ankles, we're seeing complex cases via VC." (#25 Fiona, clinical service manager)
Staff who had benefited from the extended role opportunities (or who had seen others benefit) spoke very positively about the importance of local upskilling, which resonated well with the collaborative and non-hierarchical ethos of many remote clinics (in which everyone "mucked in" rather than keeping strictly to formal job descriptions). These staff depicted traditional 'visiting consultant' service models as (often but perhaps not always) old-fashioned and overly hierarchical, especially when the consultant failed to appreciate the skills and experience of local staff.
"It [face to face clinic once a month with visiting surgeon] had been a terrible service! The surgeon was charming to the patients but treated us as slaves and serfs. He's like Teflon, pings it back, you've not done the full work-up of [pre-investigation tests]." (local doctor, code omitted to protect source)
"[On setting up the new video service] we quickly realised that because we weren't being dictated to by a consultant it would actually be stronger. The old guy was very traditional, very old school, everything had to be laid out just right. I was handmaiden, and wrong. He used to shake the Dictaphone at me and say "darling, make it work". Most of my job was appeasing patients after they'd seen him. The new system is supported by the way we are here, we're not hierarchical. He came in with his "I am the big I am", it didn't go down well." (local nurse, code omitted to protect source)
"[When I visit remote island hospital] I have five nurses swarming about me for one clinic, lovely day out, nice cakes, good craic all along." (mainland-based consultant who is opposed to the video consultation service, code omitted to protect source)
We cautiously conclude that there are situations in which video consulting may not add value if roles and relationships are unchanged, but it can add considerable value if staff are able and willing to transform their relationships to create a new service.
3.6 What concerns were raised about Attend anywhere by patients or staff?
Whilst many staff and patients were keen to describe the added value of Attend Anywhere services, we also spoke to those who were concerned that value was being (or would be) lost. In the sections below, we consider clinical inappropriateness (and clinical risk), time and hassle, lack of 'presence' compared to face-to-face encounters, and the risk of loss of services.
Video consulting is [considered to be] clinically inappropriate in some conditions
As noted in the 'Contra-indications and cautions' section, we were given many examples of clinical conditions and services for which video consultations were considered to be less suitable than a standard face-to-face consultation, though most clinicians acknowledged that in some cases a trade-off needed to be made.
It is worth commenting that clinicians who used Attend Anywhere had a more flexible and accommodating view of what was clinically appropriate, and tended to make judgements on a case by case basis. Those who had never or rarely used the service tended to hold more rigid views, to take a hierarchical rather than collaborative view of the care they provided, to have 'red lines' (situations, such as breaking bad news, where they considered a contact should never be made remotely) and be more likely to depict the remote service as unprofessional or unsafe.
"I can't stand video consultations. First of all, I'm a doctor. I'm owning my patient. A doctor wants to have direct contact with patients. I want to be able to examine them even if I hadn't planned it. There's a lot of bad news in oncology. I make a follow up appointment for 3-6 months. Can I know if they're going to be fine in 3-6 months? No! I can't. If I'd made a VC appt, and then if the scan showed something, I would have to cancel Near Me and book face to face. I can't give bad news when a patient is at home and unsupported. At the very least there'd need to be a professional - a GP or a Macmillan nurse - at the other end." (#46 Veronica, oncologist)
It is noteworthy that the successful video-consultation service operated by Veronica's colleagues operated with precisely the local support that she felt was needed (see quotes from Macmillan nurses and cancer patient). Clinicians who lived and worked in remote areas had little sympathy for such absolute views.
"The Inverness consultants don't see how difficult it is to get to Inverness. They need to get over themselves." (#45 Tom, geriatrician)
Video consulting is [perceived as] inconvenient and time-consuming
Some staff unfamiliar with the Attend Anywhere technology considered it more time-consuming than a face-to-face consultation because of set-up issues (see quote above). Those who used Attend Anywhere regularly rarely commented on these issues, which may become less significant with familiarity of use, though some clinicians said they needed to take some time at the beginning of a remote consultation to explain the different ground rules (see quote above). Our own research has shown that, like for like, remote consultations are actually significantly shorter than face to face ones [7].
Some GP practices in remote areas had installed an Attend Anywhere screen for patients to use for consultant appointments, but had not made (any or much) use of the technology to connect with their own patients at home, mainly because the advantages of video consulting for GP appointments were seen as marginal and had to be weighed against the disadvantages (including clinical risks) and hassles (such as technical connectivity). In the context of a population that was not especially digitally literate, a traditional general practice model (with branch surgeries in remote areas and GPs still undertaking home visits where needed) was seen as offering more benefits than a technological solution.
Extra logistical and administrative work
The physical absence of the patient at the clinic created demand for additional work and resource in settings that involved the sharing of materials (e.g. prescriptions, information sheets) and undertaking of medical tests (e.g. blood tests) as part of the patient assessment care pathway. For example, prescriptions would usually be provided to the patient during the consultation so that they could take this directly to the pharmacy and collect the medication. But following a video appointment, the clinicians and pharmacists needed to conduct additional administrative and coordination work in order for the patient to receive the medication:
"So patients needing something prescribed, the patient would normally receive the prescription in the room, take it to the pharmacy and go home. Now [with Attend Anywhere] we have to send the prescription to pharmacy, specifying where it needs to go, and the pharmacy needs to put in the extra effort to try and get it delivered. And that means we have to schedule appointments slightly differently so that the time-lag of delivery is accounted for […] And so savings on travel should be going into pharmacy, who would be hit…. They probably have the main hit. They have had to adapt to some extent." (#58, Richard, consultant haematologist).
Similarly, clinicians and administrators needed to coordinate with relevant services to ensure patients undertook relevant tests.
"If they are here [in face to face consultation] and you need to take blood samples, you do it in that room, at that moment. But with these [video] ones there is so much admin - getting them to see their GPs, make an appointment, get a sample, and so on… If they were here, everything would be done in one moment. We often takes the blood samples ourselves, and they sign the consent form. So it is little things." (#63, Katrina, genetics counsellor)
The remote environment has less 'presence'
The minority of clinicians who were opposed "on principle" to video consulting, most of whom had had limited actual experience with it, believed that something was inevitably lost by not being in the room with the patient even when no physical examination was needed. One specialist, whose relative had apparently had a bad experience with a remote consultation, talked about the impossibility of making proper eye contact (because the webcam catches the eyes at a slight angle). She also felt that really getting to know one's patients as people was impossible unless one met them face to face:
"They're trying to push us into having one [video consultation service for cancer] and not having the face to face visits from us. But the patients are really island people, I want to know what my patient's dog is called, what their daughter is doing, I can't be a good oncologist if I don't know these things." (#46 Veronica, consultant oncologist)
This comment contrasts markedly with those of clinicians above, who saw the Attend Anywhere service as superior to a clinic visit for getting to know the patient's lifeworld (the patient's dog and daughter, for example, might even be in the frame).
Another doctor, who uses Attend Anywhere for meetings but not clinical consultations, wondered about subtle cues and emotional 'presence'.
"Would the dynamics of the consultation be changed in that rapport is more difficult or challenging over VC, would it be more time efficient, less emotionally engaged? The limits of a consultation are more tightly structured within a CDM [chronic disease management] review, so would other things that the patient brings to the table get less attention? Is there something about emotional transference? You can clock that someone is anxious about something, something that's bugging them. Are they worried about it? When you pick up on subtle cues, you open up a dialogue, is that less in evidence in a VC? Unless you know someone really well, perhaps, in which case you already pick up on cues?" (#22 Emma, GP)
Whilst this GP is speaking entirely speculatively (she has never consulted using Attend Anywhere, though she has used it for meetings), we observed one instance of 'red flag' symptoms (a possible early indication of cancer in a patient with a strong family history) that appeared to be overlooked by a consultant who was seeing a patient remotely. In this case, there was no suggestion that the consultant acted in a clinically dangerous or improper way, since he advised the patient to see his GP. However, the dynamic in the consultation was such that the uneasiness of the patient and his wife were very apparent to a doctor (researcher) who was co-located with them but appeared to go unnoticed by the doctor who was consulting remotely. Clearly, it is impossible to generalise from a single case but the example is instructive and the possibility of missing subtle cues may merit further exploration.
'Losing' a face-to-face service
A small number of interviewees viewed the Attend Anywhere service as either actually or potentially reducing provision in their remote area. Such views tended to be held by clinicians who had professional concerns about the remote service and/or reluctance to use the technology, hence they did not view the remote service as an adequate substitute.
"Attend Anywhere in the Western Isles, they've only ever used it to withdraw a service. With Near Me [Attend Anywhere in Highland], sometimes we get an additional service." (#40 Nick, GP on Western Isles, not a regular user of Attend Anywhere)
In the above quote, Nick contrasts "withdrawn" services (by which he means replacement of a monthly or three-monthly face-to-face visit from a consultant based in Stornoway with a regular video clinic) with "additional" services (by which he means a new opportunity for patients to be seen by consultants in Inverness, Glasgow or Aberdeen using the video link).
A colleague of Nick's, who is more directly involved in running the Attend Anywhere clinics, also spoke in terms of "losing" a service, but felt that the quality of the video service was no worse.
"The Anywheres* are OK but we seem to be losing services, they [staff] used to come down. It probably hasn't reduced the quality of the service." (#35 Diane, community hospital nurse)
(* The term "the Anywheres" means Attend Anywhere appointments on the Western Isles, because unlike in NHS Highland, these are not branded as NHS Near Me. Diane also spoke of "the Near Mes" by which she meant Attend Anywhere appointments to Inverness.)
3.7 Organisational issues in implementing and scaling up the service
Preconditions for success: leadership, resources, champions, data
As noted in the 'Brief history' section, the strategic drivers for introducing Attend Anywhere included a strong national policy push for technology-enabled care; a system-wide quality improvement initiative (a major element of which was to reduce the human, financial and environmental burden of travel); the emergence of a new generation of high-quality, affordable technology; and positive feedback from patients. But these drivers did not play out evenly in all settings, since some organisations were inherently more innovative and had a more conducive set of preconditions.
Research suggests that organisational characteristics associated with successful introduction of innovations include a receptive context for change (history of successful innovation; strong, visionary leaders; a clear, positive narrative about the technology; good data systems that can monitor the effects of the change in a timely way), slack resources (people or money that could be channelled into the change effort), and a predominance of supporters over opponents. For clinical innovation, senior clinician buy-in is crucial. Our findings in this study affirmed these general principles.
We met a number of very able and charismatic leaders and managers (both clinical and non-clinical) who took a systems and human-centred approach to change, sharing power and using their personal qualities and skills to engage, mobilise and support others. We also heard some stories of efforts to introduce the remote service that had stalled because of staff shortages (especially when senior clinicians were replaced by a series of short-term locums) or general lack of resource.
"Attend Anywhere? I don't use it for consultations. [Interviewer: Why not?] Probably because the practice that I have joined has had a major staffing issue. My assumption is that they're continually firefighting. You do need to dedicate a bit of time and resource initially even if it saves time in the long run." (#22 Emma, GP who uses Attend Anywhere for meetings)
In one or two cases, a promising remote service failed completely when a key clinician moved on. This was particularly the case with the kind of highly bespoke, transformed service models described above.
"We did stuff around endoscopy. There was a speech therapist here, who was qualified to put the tube down, and a consultant on the other end. But it was awkward cos they didn't have [the patient's] medical records. And then the consultant retired so it folded. It was person-dependent." (#18 Keith, IT manager)
An important precondition for Attend Anywhere was reliable broadband. Whilst this was generally available, we learnt of one or two remote GP practices which still did not have wifi connection, and other sites where the broadband connection "dropped" so frequently that Attend Anywhere was used for professional meetings but not considered safe enough to support patient care.
A striking feature of the most successful Attend Anywhere services was that their introduction had been data-driven and strategic rather than simply following the clinical interest of a single enthusiast (though the latter was important too). The data-driven approach was sometimes led by service managers and sometimes by clinicians. Often, it occurred as a result of a trigger such as a change in financial flow (as in the first example below), rising workload, a significant event (such as an elderly or sick patient experiencing a dreadful journey) or the retirement of a key specialist (as in the second example below).
"We were starting to look at what it was costing for patient travel but we didn't [initially] have the data. We set up a patient travel database. To travel for an appointment, they need what's called a warrant (permission to travel and approval of the cost of travel). We book the flight. £3.5 million per year for a population of 26,000. We would send everyone, then bill the government at end of year. Then government devolved the budget [which had been set historically]. We needed to now work out who were these patients, where were they going, what for? So we linked in with clinical systems using the patient's CHI number [Community Health Index, the unique patient identifier] and their UCPN [unique care pathway number]. Plug that into a real time dashboard and you can see what patient travel costs are. Having got us a patient travel database, we could then use it [for strategic planning]. We found that the Scottish Government statistics were wrong. For example, oncology would show up 6 appointments in Raigmore [Inverness] per course of treatment but the patient was actually having their treatment here. We were aware of Attend Anywhere; we knew who was travelling; we wanted to get the top ten heavy hitters and ask "is this condition suitable for Attend Anywhere?". The first one was haematology. We could immediately forecast some savings. It all needs to be data driven. Understand patient flows, validate that what that data is implying to you is correct". (#18 Keith, IT manager)
"The resident dermatologist retired so we had to rethink how we did the clinic. Jonathan [service manager #6] and I audited what we had been doing to see what was needed in a new service. We were surprised how few people needed consultant input. Dr [name] would visit 2 days every other month, nobody was vetting the clinics, he'd see anyone from a rash to an outbreak. We have referral guidelines but … They [patients] don't always need to be seen by someone at consultant level." (#21 Barbara, specialist dermatology nurse)
The efforts of IT and service managers like Keith to set up remote services and embed them in business as usual was dependent on clinicians like Barbara who were willing to join the change effort, use the technology and consider working in a different way (see also quote above). Such individuals were relatively rare (described by one interviewee as "the one or two keenies"). In the absence of such individuals, no progress could be made.
"Breast surgeons haven't bought into Attend Anywhere." (#23 Patricia, Macmillan nurse)
"I'm not opposed to it; I'm quite in favour, but there's not a lot of buy-in. Nobody's really shouting "let's do this right now". I don't think there's going to be an explosion any time soon." (#49 Ed, GP, remote island practice)
Ed felt that in the current climate, policy solutions tended to be seen in overly technical terms, whereas many of the problems he faced as a remote GP were not the kind that would be solved by technology ("It's not clinically driven. That's the big thing that's stopping buy-in. The tech folk will come to us with a solution for a problem we don't have"). Whilst he described various challenges in his practice, he did not view the introduction of Attend Anywhere as solving any of these.
Variation in preconditions and the presence or absence of innovators (people who were keen on new products and new ways of working), champions (people who believed in an innovation and sought to persuade others of its benefits) and change agents (people who had the skills, time and personal qualities to drive through the change and recruit others to help) explained why different specialties and remote sites came on board with Attend Anywhere at different rates.
One important aspect of the mobilization effort for clinicians was developing guidance and ensuring that quality and safety were assured (for example, by defining what kinds of patients should and should not be seen by video consultation in each specialty). In some cases, professions in a particular specialty across the country worked together to produce national guidance. For example, national guidance has been developed for telepsychiatry, with recommendations for safe and transferable standards on establishing and delivering video consultations across Scotland (e.g. staff training, contingency planning, ethical and legal considerations).
Embedding and maintaining the change
The research literature on embedding and mainstreaming change identified four key success factors: a socio-technical approach (continually adjusting the technology and work processes to become better aligned); sense-making (what Carl May calls "cognitive participation" in which staff share a vision and feel part of a positive change effort); training and support (including, for IT, a responsive helpdesk); and monitoring (via timely data on what is working well and what needs changing) [1,7-11]. All these were evident in our dataset.
Having seen the examples of up-and-running video consulting services in the USA, Debbie was keen to ensure that the model became business-as-usual and not restricted to a handful of isolated demonstration projects.
"Prior to 2018 we had a few clinical services who were using video conferencing software. It wasn't integrated with our systems. If you had a very good secretary you could make it work but it wasn't going to scale like that. I had to take a system approach. My vision was all services offering VC in a consistent way. We needed to get to the stage where everyone who's moving around the hospital knows it's business as usual - for example, if a nurse or administrator moved departments, they'd meet the same systems and services for VC." (#1 Debbie, clinician-manager)
As they moved to the scale-up phase, various difficulties with the technology and associated work routines (see below) emerged. Because Debbie and her team understood the need for socio-technical design, such problems were taken seriously and systematically addressed.
'Early adopter' specialties were usually characterised by a willingness to share responsibility for an early phase in which things are likely to go wrong, and to work with the service managers to help embed the technology in systems and processes, and then test the service with carefully selected patients.
"Admin put their hands up and said they weren't going ahead with it. Initially we didn't have a virtual receptionist. It was chaotic, as a clinician you desperately want it to be good for the patient, I think that's why people are reluctant to do it. But things did get better. Debbie was amazing. It was her project management that helped it to fly. We had it sorted, we said let's make it fly, she said I'm troubleshooting tell me what needs improving and how. So we sent her 3-page emails with long lists of things to change, and she kept improving things. And in early 2018 we ran a small pilot to test the acceptability within our patient group. 18 patients had been invited to consult via VC [video consultation], 16 accepted, 14 attended and all of those said it was as good as face to face." (#2 Jake, psychiatrist)
Debbie described how, during the set-up phase, the quality improvement team welcomed negative feedback as an opportunity to improve. Responding to the complaints from highly sceptical clinicians in particular, and entering into dialogue with them, produced some converts.
"[Specialty X] is interesting - it's our most problematic service and our best service. When they started the consultant [name] was so negative it was quite funny. He's very critical of everything that goes wrong. But we fed all his complaints into the QI cycle. He's been great, the sound quality wasn't good enough for him, the picture wasn't good enough. The more feedback I get the better it gets. And then he phoned me, "I've got a patient whose son is abroad, wants to phone in". I told him you said you'd never do that, he said I know but it's necessary." (#1 Debbie, clinician-manager)
"It is not only someone who is helpful when asking questions, but also always keen to get feedback on how it could change. For any change like this you need someone who is going to drive it forward. Who is passionate about it." (#60, Brenda, administration manager).
Importantly, patients were included in the effort to embed and scale-up the service (see below and quote from Pauline above).
"Patients came up with good ideas. They came up with the name 'NHS Near Me' which we used to brand the service. And they said it [video consulting] is scary. They asked, "could you do open sessions so I can try it out without having to have a consultation?". We now do that on Friday afternoons." (#1 Debbie, clinician-manager)
As noted earlier, whilst Attend Anywhere is a web platform that was extremely dependable, the material infrastructure to support its use needed setting up and regular maintenance. Staff in one busy remote community hospital described a skills gap in this regard, and felt that the absence of on-site IT support was more of a problem than the lack of on-site specialist doctors. Whereas clinical consultations could usually be conducted to a high standard remotely, remote IT support was perceived as awkward and inadequate.
"We have no IT [support]; they give a virtual service. I need to raise a ticket. It works for someone who is office-based, but I'm basically on my feet all day seeing to the patients. They say "we need to take over your computer" but I'm not at my desk. They want to talk me through something I can do remotely. It's no good. We need IT on site. IT support people could come once a week or once a month. Installing stuff. I have to put the disc in, but it's always I'm not free or he's [remote IT support person] not free." (#35 Diane, community hospital nurse)
In that site, there were several pieces of expensive and sophisticated equipment that could not be used because local staff were not confident to set them up.
"We've got the same camera that they have in Y--- [regional hospital]. But we've never used it because of the lack of IT [support]. It isn't set up right; the colour balance isn't right. I'm sure if Jonathan (#6, IT-savvy service manager at Y---) came down here he'd fix it in a jiffy. That fancy camera would be great for assessing people's airways pre-op." (#33 Lynne, GP and physician)
The importance of routines
A routine has been defined as "a repetitive pattern of interdependent action involving multiple actors" [12]. Organisational work is structured around routines - for example, booking appointments, arranging prior tests, processing patients to and through an outpatient clinic, and following up (e.g. arranging a repeat appointment, sending a letter to the GP). Routines tend to be interdependent with other routines, and if one routine changes it can generate additional work in other routines and processes. As anticipated, we identified some issues (positive and negative) with organisational routines in this study.
The Attend Anywhere technology was developed to address a problem identified with previous software (which had been designed for a different purpose - conference calls). Even when previous products were technically high quality (and hence supported the actual consultation routine well), they aligned poorly with the appointment-booking routine, the 'arrival' routine and the 'following up' routine. Attend Anywhere was designed to emulate the physical arrival of the patient at the hospital desk, followed by a spell in the waiting room, before being shown into the consulting room. After some initial teething problems, this became embedded in the base hospital in Inverness (see picture above), thereby overcoming a major block to embedding and scale-up.
Emulating the outpatient clinic in this way facilitates scale-up because it maintains continuity and enables a degree of flexibility needed for a complex outpatient environment:
"It works because of the way it is set up - to work exactly how the usually outpatient system works, right down to the paperwork... So if I have a Near Me clinic, and I have a patient that needs to come in for injections, I will put them into that slot. More recently. I had a full Near Me clinic starting at 9am and finishing at 1pm and my second patient actually had something on here for a procedure. So they were here, so nipped over to my secretary and said we are here, so can we just see him face to face, so I could." (#56, Bebak, consultant in neuro rehabilitation)
However, because the Scottish model as implemented when the evaluation was undertaken predominantly involved remote NHS sites rather than connection direct to patients' homes, all the routines associated with the consultation (booking it, doing the actual consultation, following up) needed to be coordinated across two separate NHS sites. Because of different processes and patient management systems, a manual 'fix' had to be implemented to keep the show on the road. A senior manager from one of the island hospitals explains the problem.
The use of video consultations between the island and mainland boards presented challenges for the alignment of different administrative routines. In particular, the islands-based teams needed to manage the spoke locations for patients once they had been identified by the mainland hub service as suitable for a video appointment.
"Our systems have some routines, Highland has theirs. A patient will get referred, someone has to assess whether they're suitable for VC, and communicate that back to us, we then make a slot. Diedre [#5, nurse] makes that happen manually. […]. We're displacing outpatient activity from Raigmore to us. We need to be knowingly double-counting - we need a room each end. For a typical clinic, we also need to provide two nurses and a HSW." (#18 Keith, IT manager)
Several of our interviewees indicated that aligning the routines for booking appointments required communication (typically by phone or email) between administrators at both sites, both to make the original appointment and to alter it if needed.
"Technologically we don't have many issues, the issues are around the scheduling of appointments. [When things go wrong we find that] there's not been much communication among teams. […]. We have different PAS [patient administration systems] - they use TRAK we use Topaz. The problem with letters is they don't have the ability to change the location easily." (#31 Naomi, service manager)
The last sentence in the above quote referred to a patient who had been told the wrong remote clinic to attend, resulting in a great deal of work to reschedule the appointment at the clinic nearest to his home. All this had to be done manually.
Whilst our own fieldwork seemed to suggest that the Inverness team were well-organised and had an efficient system for booking appointments, staff at one remote site (in a different board) described the administration in Raigmore as "disorganised", because of a perceived inflexibility in amending bookings when asked. This (alleged) lack of flexibility, and particularly the apparent inability of a booking clerk to make a real-time adjustment when contacted by a remote site, is important since it could generate considerable additional work elsewhere in the system.
"They can't fix things when you speak to them. An overnight receptionist books appointments, but she doesn't really know the system. [Patient] had been booked into Raigmore; he'd been sent 6 different letters. Ellie, his Macmillan nurse (#24 Ellie, Macmillan nurse, remote site), contacted the clinical team directly and sorted it out. The girls in Highland can't change a room, they have to escalate it [to someone more senior]. They're busy. We want to share our room booking tool with Highland. We could put it on the web. Clinics get cancelled then someone moves a room around. I tend to pick up the phone because emails can be misinterpreted. The Near Me team in Highland is only two people. But this is a massive piece of work." (#32 Eilidh, service manager)
The same manager contrasted this situation with one in a different hospital (in Grampian), in which the booking clerk did have the ability to make a crucial change:
"He [patient] had the letter from Grampian. We didn't have the link to the [virtual] waiting room, we don't generally send to Grampian. I found the woman [clinic administrator] on Twitter. She made the link work for her, she put me in touch with their VC helpdesk. They fixed it within minutes. They made me feel like I was the most important person in the world." (#32 Eilidh, service manager)
We identified various relatively minor but irritating glitches in clinic bookings. One healthcare support worker at a busy staffed NHS Near Me 'spoke' site, for example, regularly coordinated patients who were each attending different clinics by video link. Whilst she was sent a list of these patients, it did not include which clinic the patient needed to link to.
"At the end of the day, on [date], I had 6 patients and I did not know what they were coming here for, nobody told me, I had to ask the patients who are you here to see, and that's embarrassing. It turned out to be gastro. And one psychiatry." (#42 Oona, healthcare support worker)
We checked Oona's clinic list and found a column called 'Session description' which had various free text entries. Some gave the specialty (e.g. haematology OPD) but others had more generic entries such as 'contact by video link' or 'Raigmore Hospital OPD'.
As with appointment booking, there needed to be a sense of mutual awareness in the actual video clinics. To ensure smooth running of the clinic at the remote site, for example, staff in the 'hub' site needed to gain a sense of the realities and pressures there and accommodate to those. When a patient appeared in the virtual waiting room, this indicated that he or she was sitting in the room at the remote 'spoke' site with a nurse or healthcare support worker, and that no other patient was therefore able to connect from that site. For that reason, most specialties tried to see patients from the virtual waiting room promptly and keep to time (usually by running a dedicated virtual clinic separate from the face-to-face list). The one exception was haematology, where waits of up to two hours (but more typically 45 minutes) were commonplace. In this clinic, virtual patients were slotted in with the general queue of patients attending face-to-face (whose appointments ran equally late). The clinic staff in Inverness were depicted as either not knowing about the knock-on impact on remote sites or not caring about it.
"We have very limited clinical rooms. We use the Near Me room for other things too. We might be trying to slot in that one appointment in with a [face-to-face local] clinic, so there's massive implications for that clinic if the patient is just sitting there. Haematology, there's someone up there and someone down here, and if I'm in with a casualty the clinic can't run. It's massively labour- and facility-intensive. Dietetics [via Attend Anywhere] is much easier, it runs the same for them. If you look at resources there would be a room in use up there and a room in use down here. We're not in for the whole consultation but we're around to take them in, weigh them, the dietitian would call them in themselves. If I'm not there to show the patient in, the clinic grinds to a halt. Some clinics I'll have a HSW with me, but it doesn't always work like that.... It's an extra person." (#35 Diane, community hospital nurse)
But for the haematology team based at the hub, this delay is a consequence of the necessary 'rotational' system, in which the next available consultant takes on the next patient in the queue; considered necessary to manage volume and the possibility for particularly long consultations. This has meant that they have had to book out the remote clinic room for the duration of the outpatient clinic, rather than specific time slots:
"When the [physical] waiting area is busy, people appreciate it is busy and that they will be waiting a long time. But what they don't appreciate is if half the consultations are done by video link, then the waiting room seems empty. And they think, 'Oh its quiet here, why am I waiting?'. And the same the other end [NHS Near Me spokes]," (#58, Richard, consultant haematologist)
Diane's role in the remote community hospital involved a lot of clinical and administrative multi-tasking. While recording a 45-minute interview with her, we were interrupted six times, during which she excused herself to a) take blood from a patient, b) organise an x-ray, c) see a child with an acute injury in casualty, d) get the doctor to sign a form, e) deal with a patient who knocked on the door asking for directions, and f) deal with a patient's relative asking for reassurance. Even though the research interview had been booked out in advance, Diane was the only person on duty for all the above tasks. Whilst the hospital was remote and small, it was also extremely busy and staff resented the 'hidden work' that was generated when haematology did not keep to time.
Another example of unacknowledged transfer of work to remote sites was pre-operative assessments. The pre-operative nurses in Stornoway, Western Isles, said that assessing patients remotely worked well (though, note, the technology used was Jabber not Attend Anywhere). Diane had a different view:
"All pre-op patients need height, weight, blood pressure, sats [blood oxygen saturation], and an airway check [the Mattipatti score], and lots need spiro[metry], ECG, bloods, urine and swabs. The pre-op nurses have 45-90 minutes for that, but they can't do any of the extra checks. All that is done by us. They're in a room up there, we're in a room down here, we do all the actual things, they just ask the questions. If we do all that work, we need to staff accordingly. Management needs to do the sums. It's double resourced and double roomed to do via video link. Maybe they should train someone down here to do the pre-ops. But I can't do a pre-op clinic and run the A&E. They're not looking at the full picture." (#35 Diane, community hospital nurse)
The challenges with aligning two sets of hospital routines begs the question of whether more appointments could be run from patients' homes - a topic we consider in the next section.
Challenges in setting up Attend Anywhere in patients' homes
The main reason why patients came to NHS sites (or, occasionally, other sites like nursing homes) to have a video consultation was either no internet connection at home or lack of confidence in using technology. The few patients we interviewed who were having regular Attend Anywhere consultations from home had better than average network connections and IT skills.
"How could we improve it? Nothing really. I'm tech savvy, we've got BT fibre right to the house now." (#37 Trudy, patient)
The two senior IT staff we interviewed were reticent about extending Attend Anywhere to patients' homes.
"As for patients wanting to do things from home - I'd be uneasy about getting involved with people's own wifi at home. I'd want to avoid the NHS getting dragged into having responsibility for what's running or not running in their home." (#18 Keith, IT manager)
"You've absolutely got to have good IT support." (#30 Bill, IT manager)
The question of what kind of support patients would receive to ensure that they were set up to consult remotely from home, and by whom such support would be provided, did not have an easy answer. We heard some anecdotal accounts of clinicians providing such support on an ad hoc basis:
"I'd seen an adult client in [very remote site] when working off island, I saw her several times [meaning, the patient travelled to the mainland]. She had internet, but was technophobic, didn't have an email address or anything. It was important to make sure she was confident and comfortable with it [Attend Anywhere at home], so I sent another [speech and language] therapist to get her set up for her first appointment, showed her how to use her computer. I made a document with screen shots. She managed to log on twice after that." [#39 Louise, speech and language therapist]
In addition to ensuring patients were technically set up, there have also been challenges of ensuring patients prepare and base themselves in a location and environment that is suitable for a good quality consultation:
"Some of the challenges we have is around the physical setup of the appointment. Because I am so used to seeing the person's whole body and assessing how they move all together. And we have had really basic challenges about making sure somebody is sat with a desk in front of them so I can see the hands and that they are in the right position. So we have had some really unusual complications that we were not anticipating…. So I've had patients who I have had to review while they were sitting in the passenger seat of a car. We've had patients who are evidently at work and are a little bit embarrassed because someone is asking them to do things with their hands. We haven't developed anything formal, but our requests to the patients are very different now - 'So this is still a clinical appointment, and I need you to give it the same level of respect that you would give an appointment here. So, you need to find a space with a table in front of you, with nobody to distract you…'" (#71, Michelle, physiotherapist)
"I think a lot of them are too relaxed. I had a few women do it [appointment over video] so they did not have to find childcare. But then, it becomes quite disruptive because you are trying to speak with them about something that is potentially important and the kids are running round and they are saying 'one minute' ". [#64, Thelma, genetics counsellor].
The value of a 'quality improvement' mindset
Available resource to release staff and form dedicated roles to address technical and operational issues (e.g. assess technical readiness, install cameras, redesign workflows, explain and demonstrate the technology) were key enablers to implementation. TEC funding allowed health boards to recruit or provide backfill for staff to support rollout, including project management and operational support. But the success of these roles was also underpinned by a recognition of the need to proactively and strategically drive organisational change, rather than simply focusing on the technical aspects of implementation.
"It is about cultural change and behaviour change… Because it is not a technology solution. It is much bigger than that. And we see people put their hand up for a waiting area, and it gets created. But then they never use it. And they're probably afraid to use it, in case it breaks or it cuts out during a consultation. So they will need a lot of hand-holding. And it is about how to help clinicians, how to implement this into practice... I do think it is a broader understanding of behaviour change and engaging at multiple levels. It is not just, on the ground clinicians, but also the more strategic levels as well." [#74, Susan, project manager]
Following the quality improvement mindset, efforts to embed and scale-up the use of video consultations have been easier when local programme leads had operational support from staff that already had good knowledge of the organisation; usually internally recruited onto the project from outpatient roles (e.g. care-coordinators). These staff members brought 'tacit knowledge' (know how) of the complex interrelations between systems and workflows, as well as existing personal relationships and understanding of other key organisational stakeholders. For example, some operational staff described how they drew on their knowledge and experience from working in the outpatients department to help clinic teams incorporate the 'single point of entry' (the single URL into the virtual waiting area) into their particular clinic workflows and administrative processes:
"For example, the single point of entry that we are trying to get to. So we have obviously been trying to promote that from the very beginning and had had resistance from outpatient management. So having that background and knowing how clinics are booked, the types of appointments, how patients attend clinics - knowing all of that, and that background. But then also knowing how Near Me works we were able to layout the options for outpatients." (#80, Lucy, project facilitator).
"You have to bear in mind every speciality runs their service completely differently. There is no uniformity. So how neurology deals with their patient and how they vet their patients will be done completely differently to how dermatology does theirs or how vascular does theirs. And that is how knowledge comes in handy". (#82, Bianca, project facilitator and trainer].
3.8 What wider (contextual) issues have influenced Attend Anywhere in Scotland?
National policies and priorities
As described in the Background section, strategic drivers for the scaling up of remote video consultations in Scotland have included a strong national policy push for technology-enabled care. The 2019-2020 Programme for Government specifically commits to the scaling up of Attend Anywhere within healthcare with reference to cost-effectiveness, reduced travel and people's access to services [13]. This work also aligns with a number of national policy priorities, including the waiting times improvement plan [14], realistic medicine [15], the Access Collaborative emphasis on avoiding travel [16], the 2019 National Islands Plan to improve quality of life of Island communities [17] and the impact of health on 'inclusive' economic growth [18].
Strong policy support for Attend Anywhere has helped address regulatory and operational challenges over the course of the programme (e.g. including Chrome as a supported internet browser within the NHS Scotland National Infrastructure Standard), and plans to expand its use are now included in the Digital Health and Care Local Implementation guidance, which is used to align the health board operational plans with government policies.
However, this still presents challenges, as national priorities do not play out evenly across organisations, and there can be different understandings and definitions of scale-up and 'success' across multiple stakeholders.
"Although Near Me is a national initiative and is being pushed, there are other things that are being pushed nationally, like clinical referral triage, which will help tackle demand and will contribute to reducing workload….There are lots of things around modernising patient pathways. And that ties in with Near Me. But on its own there are other things that will give them more direct results… so it is difficult getting clinicians' time". [#81, Denise, Project Manager]
"Whilst we might present something that we understand to be successful to one director, it may not necessarily be perceived as success for another director, particularly in terms of whether it is directly contributing to whatever is under that director's remit….For example, some may be very interested in all the target aspects of the healthcare services - if it is contributing to reducing waiting times, if it is contributing to preventing people coming into A&E, so the hard metrics of the NHS….Whereas if you speak to someone else, like the chief medical officers, they will have a clear focus on realistic medicine and getting an approach that allows the patient themselves to feel in more control." [# 109, Brian, VC programme board).
General context for NHS services in Scotland
Staff and patients in all the sites we visited were proud of their NHS, which they saw as reflecting deeply-held and widely-shared core values including high-quality universal healthcare provision and equity of access. In this context, the Attend Anywhere video service was generally (but not universally) seen as enhancing the existing service rather than replacing or threatening it.
"I'm very impressed with this service. Can't praise the NHS enough. The media's full of criticism but my experience has been brilliant. Everyone's been very kind." (#43 Patrick, patient)
"I don't know if I'm allowed to be political here? [Interviewer: Sure] OK, the politics of healthcare in Scotland I think may facilitate that [introduction of Attend Anywhere]. All boards work in standardised format, very much an NHS Scotland branding. There's no purchaser-provider split. We work across boards in a collegiate manner; we're a social democratic, socialisty country. Making money out of health and education is not in our national ethos." (#22 Emma, GP)
We found what one interviewee called a "Russian doll" effect, in which a remote site might be a 'spoke' for some services (connecting, say, to Inverness for several secondary care services not available locally) but also serve as a 'hub' to provide some specialist input to even more remote sites (for example via a geriatrician, generalist physician or GP with special interest). Inverness connected to Glasgow for some specialist tertiary care services. Because many generalists in Scotland had developed one or two specialist interests, and because (unlike in England) there was no purchaser-provider split, Attend Anywhere links sometimes occurred horizontally rather than vertically and in a reciprocal and collegiate way.
Connectivity and digital literacy
It is important to acknowledge a fairly rapid pace of progress which has probably not yet had full impact. On the Western Isles, for example, high-quality broadband is now widely (though not universally) available but there is not yet a culture of using it.
"A typical thing is an old person gets given a laptop by their family then left on the island [without support to use it]. 4G became a thing here only 2 years ago. There's not a culture of people owning phones or wireless devices, they used to only turn it [phone] on once a week when they went to town." (#28 Teresa, service manager, Western Isles)
The 'Reaching 100%' (R100) infrastructure initiative was established in May 2016 to deliver superfast broadband to 100% of homes and businesses in Scotland by the end of 2021 [19]. At the time of writing this report, it is estimated that superfast broadband coverage has reached 92% of Scotland premises [20]. The Scottish Government's 4G Infill programme, which began in May 2018, also aims to improve mobile coverage in the Highlands, Islands and other 'black spot' rural areas.
An important initiative in remote parts of Scotland is mPower (https://mpowerhealth.eu), an EU-funded project to help older people with long-term conditions to live independently. Community navigators visit people and put together a wellbeing plan that takes account of family support and local community resources as well as relevant online resources. As appropriate, the individual is supplied with a smartphone or tablet and shown how to use it for keeping in touch with their family, doing online shopping and so on.
"M-power is to support people at home using technology. They get a visit, someone makes recommendations. You get a badge to say you're all right. Maybe they'll do it through a local housing association who assess people for telecare; people doing the visit are already trusted vetted and trained to go into an old person's house." (#18 Keith, IT manager)
This scheme was beginning to explore linking with Attend Anywhere.
"Once we're assured that the person is comfortable and confident to do a VC, we will then annotate that patient's record. And the clinician will see that the patient is able to have a VC. It's done via SCI Gateway,[8] there could be an automatic referral system; it would pick up the demographics, the CHI number." (#28 Teresa, service manager)
National TEC Programme: supporting inter-organisational learning and collaboration
The TEC VC work stream has provided funding through the 'scale-up challenge' (up to £150K) to each participating health board to purchase equipment and recruit and/or buy out staff time to support implementation activities, which further formalised local roll out efforts:
"It made it a formal project, putting rigour and focus and to deliver actions. It helped get all of the stakeholders together at the right time. We would not have been able to do it otherwise, we would have never stood a chance getting it done otherwise, before the funding came in." [#93, Larry, project manager in eHealth)
The TEC VC workstream team have also been forming routes for inter-organisational learning and collaboration through monthly calls/meetings, open webinars sessions and an online discussion forum using 'Basecamp' (online project management and document sharing application). During the time of writing this report, the Basecamp Attend Anywhere forum had nearly 100 users (local programme leads, project managers, operational support and clinical champions and representatives from Attend Anywhere) and has been extensively used by members to raise issues, publicise and share documentation (e.g. guidance, standard operating procedures, public facing resources).
Some perceived a need to build on and enhance these opportunities for shared learning, particularly with regard to reaching frontline staff 'on the ground', linking organisational counterparts and effective signposting to problems and requests:
"I find in the discussion you start picking up on issues that a board are having that other boards have overcome, so at moment I am trying to connect the boards together to share issues. I feel we could do more in that space. Monthly meetings are not the answer. We have got Basecamp but there are not too many people using it broadly." [#74, Susan, project manager]
The national VC Support team (hosted at NHS Grampian) has also played a key role, providing remote support to health boards through helpdesk assistance, operational support and training. Additionally, they help configure and manage administrative settings on users' Attend Anywhere accounts. These roles have recently extended to supporting NHS England trusts adopt Attend Anywhere, as part of the NHS England pilot.
As the national VC Support team interacts with multiple user groups across different organisations on a day to day basis, they are well placed to interface with the Attend Anywhere team (in Australia) to request additional technical support and design requirements.
"Thankfully there is not much that goes wrong with Attend Anywhere. But if there are, we can act as a point to escalate that to the people in Australia, saying there might be a problem with this functionality because x number of people have reported it." [#84 Dee, VC Support Manager)
Contact
Email: socialresearch@gov.scot
There is a problem
Thanks for your feedback